
Abstract
Purpose:
To define the anatomical relationship of the major neurovascular structures to the standard endoscopic portals used in endoscopic hamstring repair. A secondary outcome was to determine the safest angle of insertion from each standard portal.
Methods:
Endoscopic portals were established in the 3 standard locations (lateral, medial, and inferior) and Steinmann pins inserted at various angles. Each hip was dissected and the distance between the pins and the pertinent anatomy measured.
Results:
The lateral portal placed the sciatic and posterior femoral cutaneous (PFC) nerves at greatest risk: direct injury to the sciatic nerve was seen in 11/30 (37%) of the lateral portals sited. A lateral portal with an approach at 60° was the most dangerous orientation with a mean distance of 0.36 ± 0.49 mm and 4.30 ± 2.69 mm from the sciatic and PFC nerves, respectively (p < 0.001). The 60° medial portal was the safest of all portals measured, at a mean distance of 67.37 ± 11.06mm (range, 47–78 mm) from the sciatic nerve and 58.90 ± 10.57 mm (range 40–70 mm) from the PFC nerve.
Conclusions:
While currently described techniques recommend establishing the standard lateral portal first, this study shows that it carries the highest risk of injury if used blind. We recommend that the standard medial endoscopic portal is established first to identify the neurovascular structures and minimise iatrogenic neurovascular injury. The inferior and lateral portals can then be established created under direct vision. The lateral portal should be inserted in a more horizontal orientation to decrease the risk of nerve injury.
Introduction
The hamstrings are among the most commonly injured muscles in athletes.1,2 They consist of the biceps femoris (long and short heads), semitendinosus, and semimembranosus muscles. With the exception of the short head of the biceps femoris, the hamstring complex takes origin from the ischial tuberosity and inserts onto the proximal tibia, thereby crossing both the hip and knee joints. Muscles that cross 2 joints, such as the hamstrings, are rarely stretched during daily activities but are vulnerable to eccentric loading, leading to injury. There is a broad range of hamstring injuries, ranging from strains and partial tears to complete avulsion injuries. 3 The vast majority are muscle strains at the myotendinous junction which typically respond well to nonoperative treatment including active rest, oral nonsteroidal anti-inflammatory medication, and physiotherapy.4,5 However, roughly 12% involve the proximal hamstring origin, and the treatment of these remains controversial. 5 Indications for surgery have been proposed including bony avulsion with 2 cm of displacement, complete tear of at least 2 of 3 tendons with >2 cm of retraction, and partial tears that remain symptomatic despite at least 6 months of non-operative treatment. 6
Several techniques for open surgical repair have been described which typically involve an incision of approximately 8 cm in the gluteal crease, elevation of the gluteus maximus, identification of the sciatic nerve and torn tendons, and fixation of the tendons to the ischial tuberosity using suture anchors.7–9 Problems with open repair include difficulties with visualization of the proximal hamstring origin, particularly in patients with greater gluteal bulk, neurapraxia of the cutaneous nerves of the buttocks (cluneal nerves) from traction of the gluteus maximus, injury to the sciatic nerve and inferior gluteal neurovascular bundle, and infection risk due to proximity to the perineal area.10,11
The endoscopic repair of proximal hamstring injuries was first described by Dierckman and Guanche 12 and with advances in endoscopic techniques and equipment has gained in popularity.12–15 described endoscopic technique involves the establishment of 3 standard portals, lateral, medial, and inferior, through which the proximal hamstrings, ischium, and hamstring footprint can be accessed. 12 The advantages of endoscopic repair include minimal disruption to the local anatomy, decreased blood loss, a lower risk of infection, direct visualization, and potentially decreased neurovascular complications because of improved visualisation.12,13
While the endoscopic approach has its advantages, there are concerns about the technique. These include injury to neurovascular structures during blind portal placement, a steep learning curve, and the technical challenges of passing and shuttling sutures for repair. 13 The 3 main nerves at risk of injury during open surgical hamstring repair are the posterior femoral cutaneous (PFC), inferior gluteal, and sciatic nerves. 16,17 There is, currently only limited data about the incidence of complications and iatrogenic injury to neurovascular structures during endoscopic hamstring repair.
The purpose of this study was to define the anatomical relationship and proximity of the major neurovascular structures to the standard portals used in endoscopic hamstring repair. A secondary outcome was to determine which angle of approach would provide the safest approach for this technique. We hypothesised that the standard lateral portal would place the nervous structures at the highest risk of injury.
Methods
Cadaver data
5 fresh frozen full-body human cadavers (10 paired hips) were procured (United Tissue Network). All 5 were male, with a mean age of 64.2 (range 47–82) years and a body mass index (BMI) of 26.5 kg/m2. No specimen had a history of hip pathology or hip surgery. Institutional review board approval was not required for the completion of this study.
Anatomy
Each specimen was thawed to room temperature and placed prone with the hips in 10° of flexion and neutral rotation. Relevant landmarks were drawn using a skin marker (Figure 1), outlining the ischial tuberosity, and portals were established based on the method described by Dierckman and Guanche. 12 Briefly, lateral and medial portals were marked out 2 cm lateral and medial to the palpable ischial tuberosity and an inferior portal was marked 4 cm distal to the tip of the ischium and equidistant from the medial and lateral portals (Figure 1).
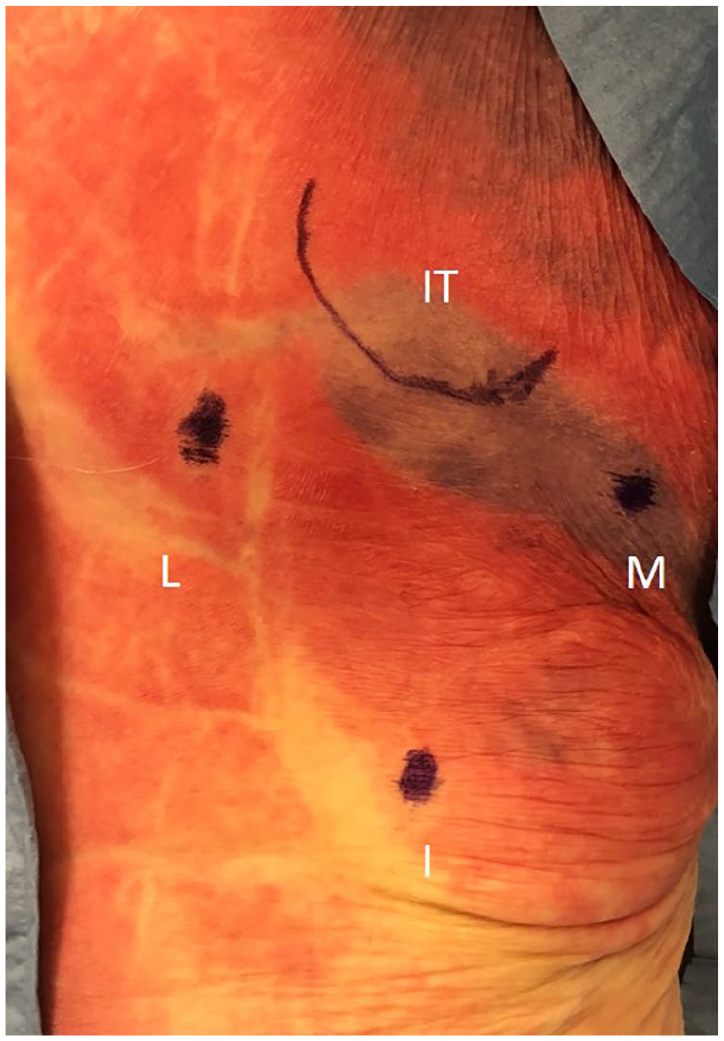
Photograph of cadaver specimen positioned prone with superficial anatomy marked demonstrating the ischial tuberosity (IT), medial portal (M), inferior portal (I), and lateral portal (L).
Descriptions of the surgical technique for endoscopic hamstring repair have clearly outlined the initial positioning of the portal sites; however, the angles at which the initial instruments are introduced have not been described. 12 To assess how differences in the initial insertion angle would affect their proximity to major neurovascular structures, 3/16-inch Steinmann pins were inserted through each entry portal at 3 different angles using a goniometer (Figure 2). Pin insertion was completed by 2 senior orthopaedic residents (CS, ML). For the medial and lateral entry portals, the pins were directed towards the ischial tuberosity at 30°, 45°, and 60° from the horizontal. For the inferior portal, the pins were either aimed directly towards the ischial tuberosity (0°) or at 45° medially or laterally from the tuberosity.
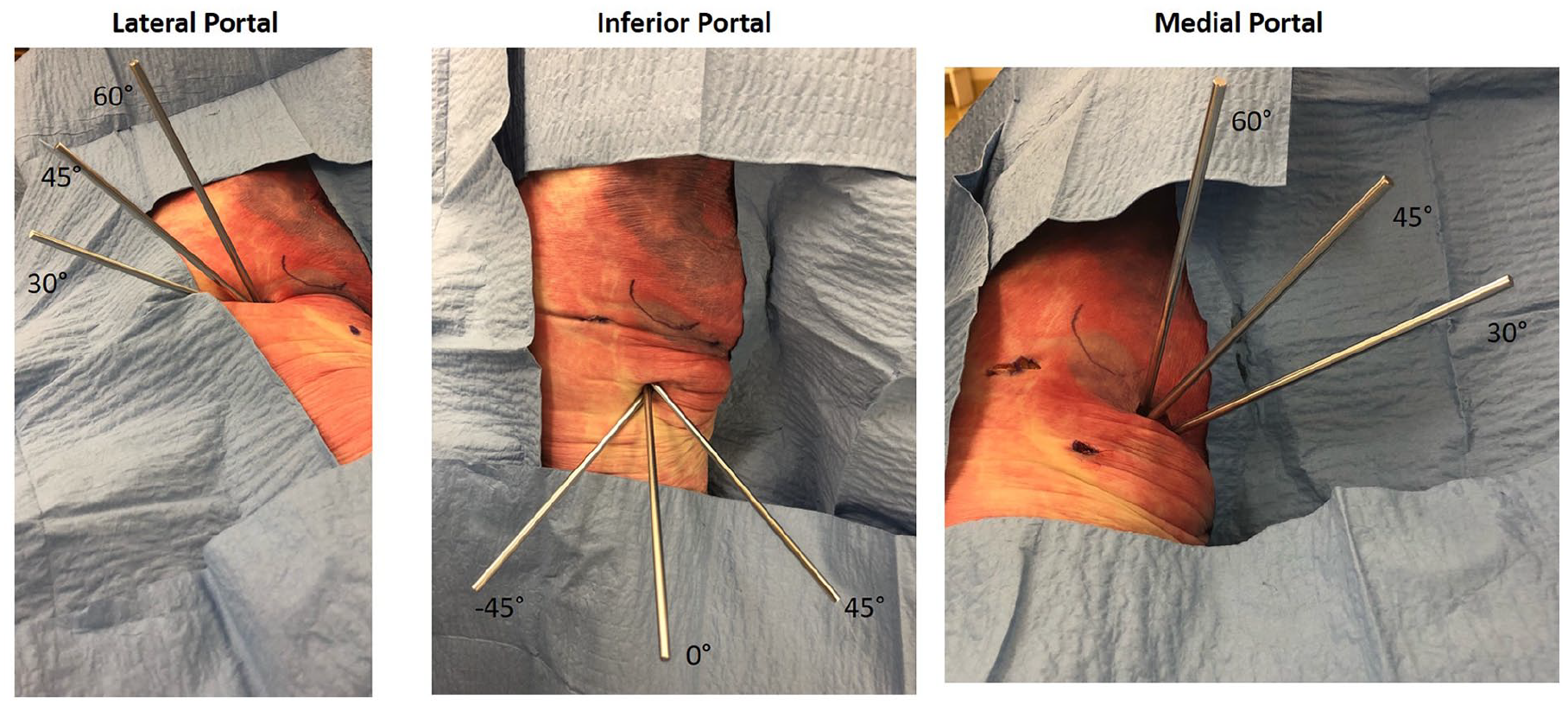
Demonstration of Steinmann pins placed in standard portals at various angles with cadaver specimen positioned prone.
The skin and subcutaneous tissues were then dissected to expose the gluteal and hamstring musculature. Gluteus maximus was reflected and the neurovascular structures of interest were carefully dissected and preserved throughout their course (Figure 3). Measurements were made from the pertinent anatomical structures to the inserted pins using a digital caliper. Dissections and measurements were carried out by 3 authors.
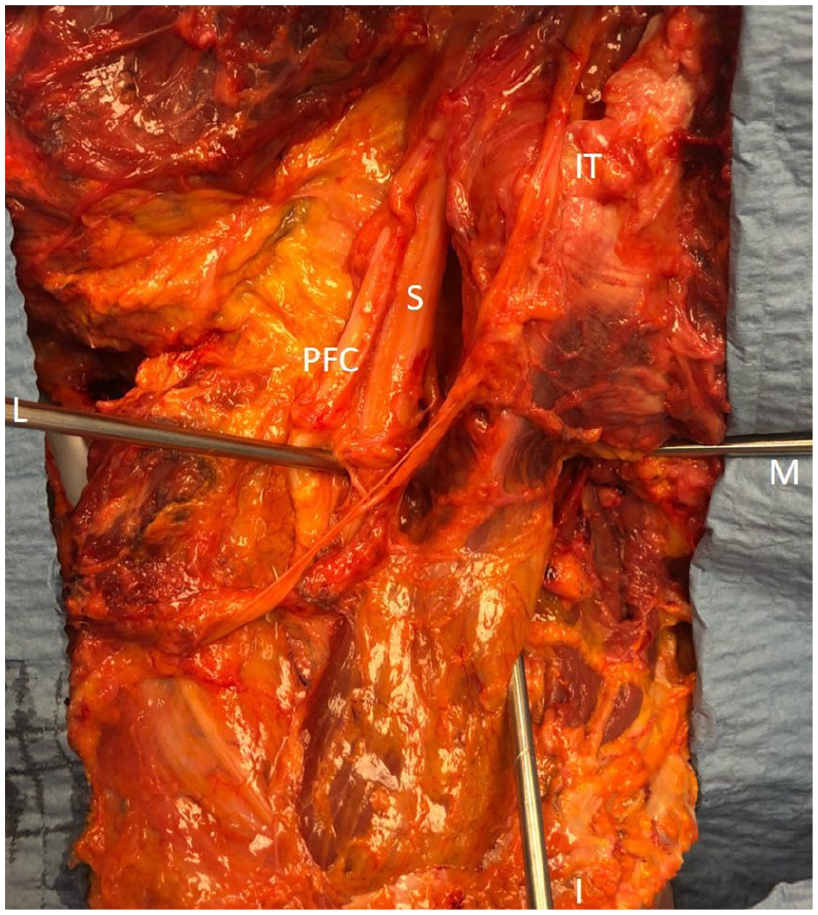
Demonstration of proximity of medial (M), lateral (L) and inferior (I) Steinmann pins to relevant anatomic structures including the ischial tuberosity (IT), sciatic nerve (S), posterior femoral cutaneous (PFC) nerve.
The pudendal nerve and the inferior gluteal nerve and artery were also identified, but these structures were never within 5 cm of the nearest standard portal, so were excluded from analysis as they were determined not to be at risk.
Statistical analysis
Each anatomical measurement was repeated independently by each of the 3 authors and then averaged to provide consistency during measurement. An intraclass correlation coefficient (ICC) was obtained for each of the measurements to validate reliability and was found to be >0.90 for all measurements, indicating excellent reliability. Inter-rater reliability was found to be 0.92. An ANOVA was performed to determine if there was any significant difference among the angles of insertion evaluated. The safest angle of insertion for each portal location was then compared to determine if any of the standard portal placements were more dangerous. All significance values were set at 0.05.
Results
The lateral portal placed the sciatic and PFC nerves at greatest risk when compared to the 2 other standard portals, regardless of the angle of insertion (Table 1). Direct injury to the sciatic nerve was seen in 11/30 (37%) of the lateral portals sited. A lateral portal with pin insertion at 30° (most horizontal) was the safest of the lateral portal orientations for both the sciatic nerve (p < 0.001) and the PFC nerve (p < 0.001) but still injured the sciatic nerve in 2/10 hips (20%). The lateral portal with insertion at 60° (most vertical) was in closest proximity to both the sciatic and PFC nerves, with direct injury to the sciatic nerve in 6/10 (60%) of hips. The 45° lateral portals were at an intermediate distance away from both the sciatic and PFC nerves and were found to directly injure the sciatic nerve in 3/10 (30%) of hips.
Average distance (mm ± standard deviation) from 3 standard arthroscopic portals to major nervous structures.
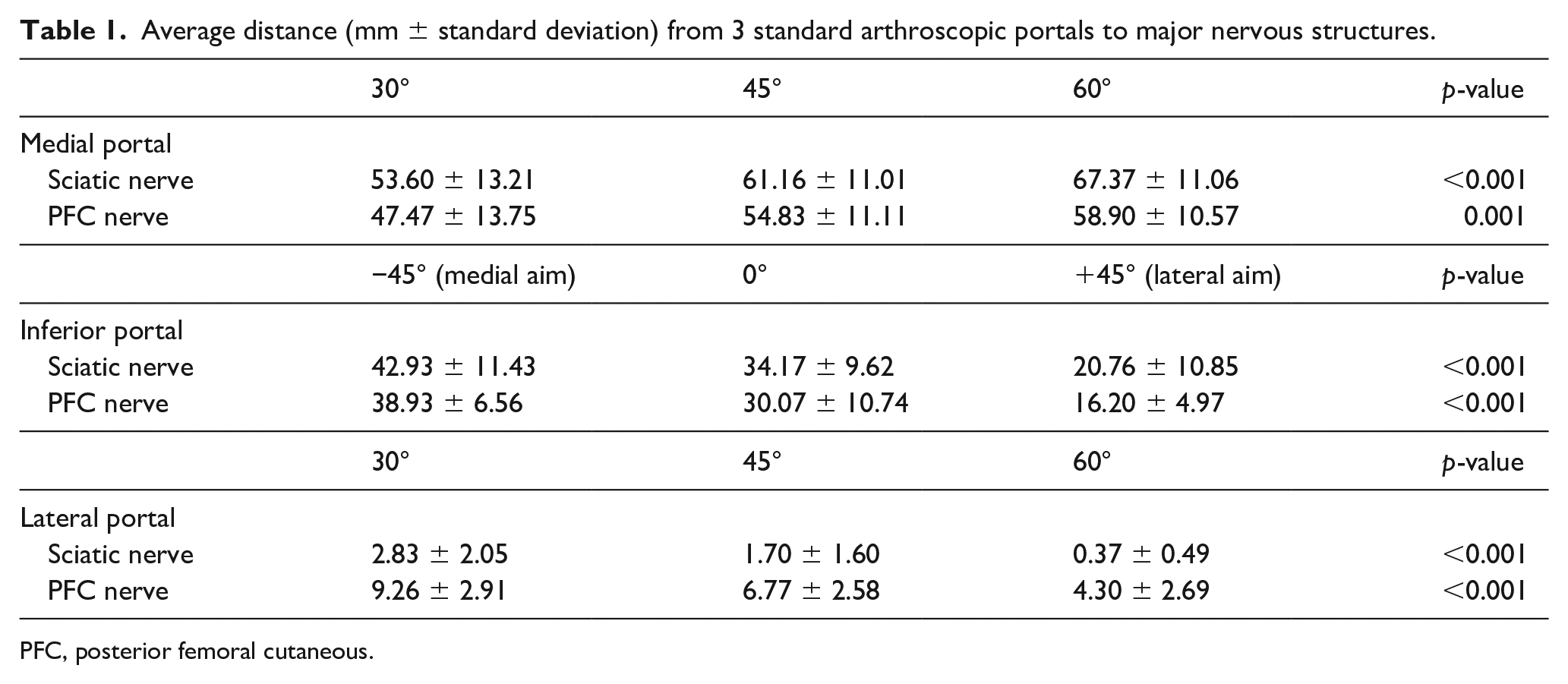
PFC, posterior femoral cutaneous.
Nerves were at significantly less risk with the inferior and medial standard portals (Table 1). For the inferior portal, placement of the pin at 0° or 45° aiming medially was safest for both the sciatic and PFC nerves. A 45° laterally directed inferior portal was the most dangerous of the inferior portals tested. No direct trauma to the sciatic or PFC nerve was seen with any orientation of standard inferior portal placement.
The medial standard portal was the safest of the 3 standard portals with the furthest mean distance between pin and sciatic and PFC nerves. The 60° (most vertical) medial portal was the safest of all standard portals with the furthest distance from both the sciatic nerve (p < 0.001) and the PFC nerve (p = 0.001). No direct trauma to the sciatic or PFC nerve was seen with any orientation of pin through a standard medial portal.
Discussion
Proximal hamstring tendon avulsions are debilitating injuries with a poor capacity for healing. Although open surgical repair has been the standard treatment, improved endoscopic techniques have enabled proximal hamstring fixation without the morbidity of a large incision and the potential for a decreased risk of infection and nerve injury. Moreover, a recent cadaveric study of paired pelvic specimens found no biomechanical difference between open and endoscopically repaired proximal hamstring tendons in terms of ultimate load, strain, or displacement at failure. 18 Our data show that of the 3 standard endoscopic portals, the standard lateral portal is indeed the most dangerous, with direct injury to the sciatic nerve in 37% (11/30). Furthermore, more vertical insertion of a pin through a standard lateral portal placed the sciatic and PFC nerves at greatest risk, with direct injury to the sciatic nerve seen in 60% (6/10) of cases whereas no direct injury to the sciatic or PFC nerves was seen with any orientation of pin through a standard medial or inferior portal. The findings of our study confirm our hypothesis that the standard lateral portal placement puts nerves at the highest risk of injury.
The technique for endoscopic proximal hamstring repair has been described by several authors.12–14 Interestingly, all recommend establishing the standard lateral portal first, despite the highest risk of injury to the sciatic and PFC nerves. In particular, an anatomical study by Miller et al. 11 found that the sciatic nerve is a mean distance of 1.2 ± 0.2 cm lateral to the ischial tuberosity 10. With the recommended initial lateral portal placement 2 cm lateral to the ischial tuberosity, the sciatic nerve is, therefore, within 1 cm of endoscopic instruments introduced through this portal.
We would instead recommend that the standard medial endoscopic portal is established first to minimise iatrogenic neurovascular injury. This medial portal should then be used as a viewing portal to identify and ensure that the neurovascular structures are adequately safeguarded before creating the inferior and lateral portals under direct vision. Additionally, instruments should be inserted in a more horizontal orientation through the lateral portal to further decrease the risk of nerve injury. We believe that this modified technique would minimise iatrogenic nerve injury and would be a significant improvement on the original technique described by Dierckman and Guanche. 12
Additional studies have found that the inferior gluteal nerve and artery can be found 5.0 ± 0.8 cm from the inferior border of the gluteus maximus at the lateral border of the ischium and that the pudendal nerve is typically found 7.7 ± 1.3 cm from the proximal hamstring centre point.10,19,20 Our dissections confirmed that the inferior gluteal neurovascular bundle and pudendal nerve were not within 5 cm of the nearest endoscopic portal.
A recently published study of endoscopic proximal hamstring repair and portal sites concluded that major neurovascular structures were safely out of the way of all portal site trajectories, with a minimum of 2.4 cm (range 1.3–5.4 cm) to the sciatic nerve and 2.55 cm (range 0.7–6.8 cm) to the posterior femoral cutaneous nerve. 18 The apparent discrepancies with our current study are likely to be related to several factors. Portal marking and placement in our study was performed identically to that originally described and illustrated by Dierckman and Guanche 12 with medial and lateral portals created “2 cm medial and lateral to the palpable ischial tuberosity” and an inferior portal created “4 cm distal to the tip of the ischium and equidistant from the medial and lateral portals”. 12 The study by Ryan et al. 18 instead used four unique portal sites (inferolateral, medial, superolateral, accessory superior) which are different from those used in our study. Secondly, anatomical measurements in their study were made based on the trajectory of each portal site after creating and repairing open and endoscopic proximal hamstring injuries, which we did not perform in our study. Finally, we used whole-body cadavers instead of sacrum-to-proximal femur: full-pelvis specimens may have accounted for some differences. Nonetheless, data from both our studies are in agreement that the laterally based portals place the sciatic and PFC nerves at greatest risk compared to the other endoscopic portals.
Limitations of the current study include those traditionally associated with cadaveric studies including tissue deterioration and differences in tissue mobility compared with those encountered during surgery. Our cadaveric model also does not account for normal physiological responses to hamstring injury including swelling or bleeding that could change the location of nearby structures. Finally, the cadavers were all male and of an older age (mean 64.2 years), which will differ from the demographics of patients who are undergoing proximal hamstring repair. The exact distances identified in our cadaveric model may therefore differ from the anatomy encountered during surgery.
Conclusion
While currently described techniques recommend establishment of the standard lateral portal first, our study shows that this carries the highest risk of injury to the major nerves. We recommend that the standard medial endoscopic portal is established first so that the major neurovascular structures can be identified thereby minimising iatrogenic injury. The inferior and lateral portals can then be established under direct vision. Additionally, instruments should be introduced through the lateral portal in a more horizontal position to decrease risk of nerve injury.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SN: reports non-financial support from Allosource, other from American Journal of Orthopedics, other from American Orthopaedic Society for Sports Medicine, non-financial support from Arthrex, Inc, other from Arthroscopy Association of North America, non-financial support from Athletico, non-financial support from DJ Orthopaedics, non-financial support from Linvatec, non-financial support from Miomed, personal fees from Ossur, non-financial support from Smith & Nephew, personal fees and non-financial support from Springer, non-financial support from Stryker, outside the submitted work.
RCM 3rd: reports personal fees from Stryker Corporation, Consultant and research support Zimmer Biomet, Research support Reflexion Health, Research support, outside the submitted work.
MJS: reports personal fees from Stryker Corporation, outside the submitted work.
All other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.