
Abstract
Background:
Mid-term results (clinical and radiographic) of ultra-short anatomical cementless stem total hip arthroplasty (THA) in patients with osteonecrosis of the femoral head (ONFH) has not often been presented. The aim of this study is to evaluate THA using the Proxima stem in patients with ONFH in the mid-term.
Methods:
The study consists of 73 patients (97 THAs) with a Proxima stem implanted between 2006 and 2015. The mean age of patients was 47.4 years, with a mean follow-up 105.2 months. The clinical results include preoperative and postoperative Harris Hip Scores (HHSs). Radiological follow-up reports on stem migration, bony trabecular development and radiolucent lines. The complications and revisions were registered. Kaplan-Meier survival analysis was performed to determine the implant survival.
Results:
The average HHS improved significantly from 40.3 preoperatively to 98.0 at the final evaluation (p ˂ 0.0001). Stem migration (subsidence and “varisation”) was observed in 11 hips (in 9 of them up to 6th postoperative month without any further progression, in 2 with progressive migration and radiological loosening). Bony trabecular development was detected in modified Gruen zones (1,2,4,6,7 for Proxima stem): in zone 1 (0%), 2 (67.0%), 4 (64.9%), 6 (64.9%), 7 (0%). Radiolucent lines were observed in 1 cup and 6 stems (2 were loose, 4 with fibrous stable fixation). Complications were found in 5 hips (5.1%): squeezing hip once, repeated dislocation in 1, 1 early deep infection, and 2 loose stems. 2 hips (2.1%) were revised (dislocation, infection). The implant survival was 98.9% and 97.9% clinically and radiologically, respectively.
Conclusions:
Observations in the mid-term show that the clinical and radiological results of the Proxima stem in patients with ONFH are promising. The stem design preserves the proximal femoral bone stock. The bony trabecular appearance confirms physiological proximal femoral load transmission.
Keywords
Introduction
Osteonecrosis of the femoral head (ONFH) is a complex clinical, radiographic and pathological syndrome, which leads to hip joint destruction secondary to an impairment of blood supply.1,2 ONFH usually affects patients <60 years, in men 5 times more often than women. 3 The risk factors associated with ONFH are: corticosteroids; chemotherapy and radiotherapy (immunosuppressant agents); and excessive alcohol consumtion.4,5 When the loss of the femoral head sphericity occurs, total hip arthroplasty (THA) for the secondary osteoarthrosis is the recommended treatment option for the maintenance of good hip function and pain reduction. 3 In the past, a few studies about THA (first generation implants) in patients with ONFH presented relatively poor outcomes. 6 Contemporary conventional implants provide good results in patients with ONFH. 7 But there are still described complications of the conventional cementless stems: thigh pain, difficult revision, stress-shielding phenomenon, proximal-distal dimensional mismatch, proximal femoral bone loss.
In an effort to minimise these concerns (preservation of the femoral intramedullary canal and maintenance of femoral elasticity), short and ultra-short uncemented anatomical stems were introduced. 5 The short anatomical stems could be advantageous in younger patients with ONFH, where restoration of normal bone load transmission is crucial for long-term survival of the implant. However, clinical reports on the outcome of these stems in patients with ONFH are scarce. The authors have found only few reported outcomes for the use of the Proxima stem in patients with ONFH.5,8,9 The aim of this study is to assess clinically and radiographically a series of our patients who had undergone primary THA with the Proxima stem for the treatment of ONFH, and who were followed for minimum of 5 years. We hypothesised that ultra-short stem THA would be a promising treatment option for patients with osteonecrosis.
Materials and methods
Patient records were reviewed retrospectively for demographic data, details of the surgery (used implants), x-rays and follow-up results.
The study group consisted of 73 patients with ONHF. All patients were treated with primary THA (using the Proxima stem) between 2006 and 2015 at University Department of Orthopaedic Surgery in Martin, Slovakia.
This study was approved by the Institutional review board. All patients provided informed consent.
Inclusion criteria
Included in this study were patients aged >18 and <65 years with good bone quality (Dorr type A or B), with advanced ONFH: stages III–IV of the Ficat-Arlet classification system and with a minimum follow-up of 5 years.10,11
Exclusion criteria
Previous hip surgery, trauma, inflammatory or oncologic diseases in the area of the affected hip joint, severe osteoporosis, or incomplete follow-up.
1 hip with Proxima stem for ONFH was excluded from the study because of incomplete follow-up.
Surgical procedures
Preoperative planning and templating on radiographs were used to determine the implant sizes. All procedures were performed by 1 of 2 experienced surgeons (LN, MM) in the supine position, via an anterolateral approach. The uncemented Pinnacle cup (DePuy, Warsaw, IN, USA), (range 48–62mm) was implanted with an lateral inclination of 40–45° and 15° of anteversion, using a “press-fit” technique. The ceramic inlay was then inserted. Next, the ultra-short uncemented Proxima stem (DePuy, Leeds, UK) was inserted by the “round the corner” technique. We used a standard stem in 91 cases and high-offset stem in 6 cases; the most frequently used stem sizes were 4 and 5 (Figure 1). The 28- and 36-mm ceramic head was used according to the shell (inlay) diameter.
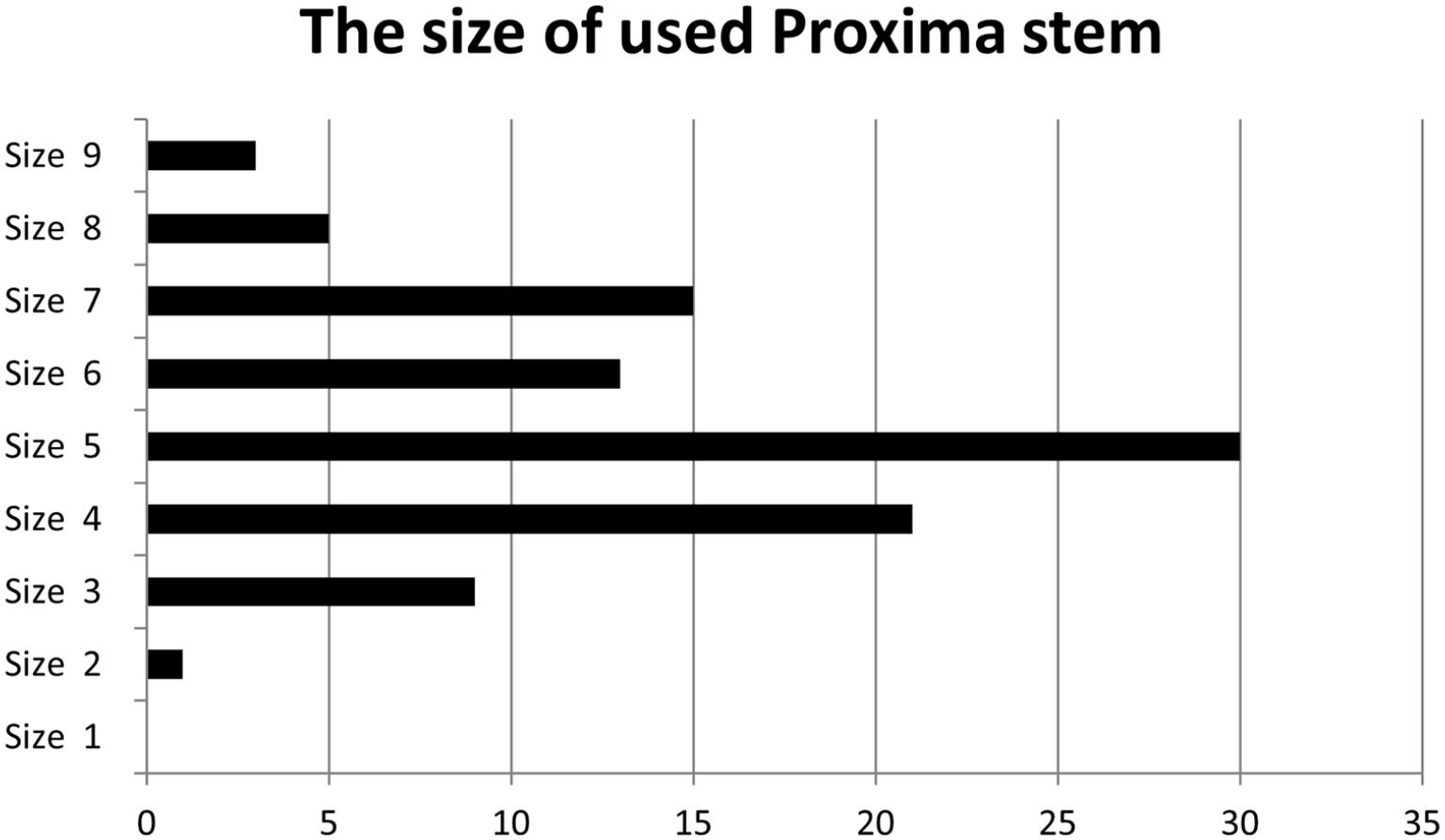
The size of the used Proxima stem.
Postoperative management
Active and passive movements started on the first postoperative day. On the second postoperative day, patients were allowed to stand. Patients were discharged 6 days postoperatively on average (range 4–10 days). Walking, touch-weight-bearing with crutches, was recommended until 6 weeks postoperatively (to prevent early stem migration, rotational stress and loosening), when patients were examined clinically and radiologically. Thereafter, partial weight-bearing was permitted. After the next examination, at the third postoperative month, full weight-bearing was allowed.
All patients were then followed clinically and radiologically at 6 months, 1 year and annually thereafter until the end of follow-up period (during the year 2020).
Clinical outcome measures
Basic demographic data were collected, including age, body mass index (BMI) and osteonecrosis aetiology. The Harris Hip Score (HHS) was assessed preoperatively and at final follow-up. 12 Thigh pain was assessed during physical examination. Any leg-length discrepancy (LLD) was measured radiologically. The early and late complications and any potential need for the revision were recorded.
Radiographic assessment
Preoperative, postoperative and final follow-up radiographs, in both projections (anteroposterior [AP] and lateral), were examined blindly by an experienced orthopaedic radiologist (MH), who was not involved in any of the studied THAs. The stage of ONFH and Dorr type of the femur were evaluated preoperatively. On the postoperative radiographs, the cup position and stem alignment were evaluated. The stem position was assessed according to Gombár et al. 9 on the AP x-ray: as “neutral”, if its deviation from the axis of the femoral shaft was ⩽5°; “varus” or “valgus” with a deviation of 6–10° and “severe varus” or “severe valgus” with greater deviation. Radiological evaluation during the follow-up period was focused on stem migration-malalignment (subsidence, ”varisation”), radiolucent lines, stress-shielding phenomenon and bony trabecular development in modified Gruen zones for the Proxima stem (Figures 2 and 3 (a–e)). 13 Stem migration was evaluated according to Martel et al. 14 Implant stability was assessed based on the radiological features of the bone-implant interface according to Engh et al. 15 Criteria for radiological loosening of the stem were defined as a radiolucent zone >2 mm, or a migration >3 mm with an adjacent radiolucent line surrounding the entire stem on the anteroposterior and lateral radiographs.5,9
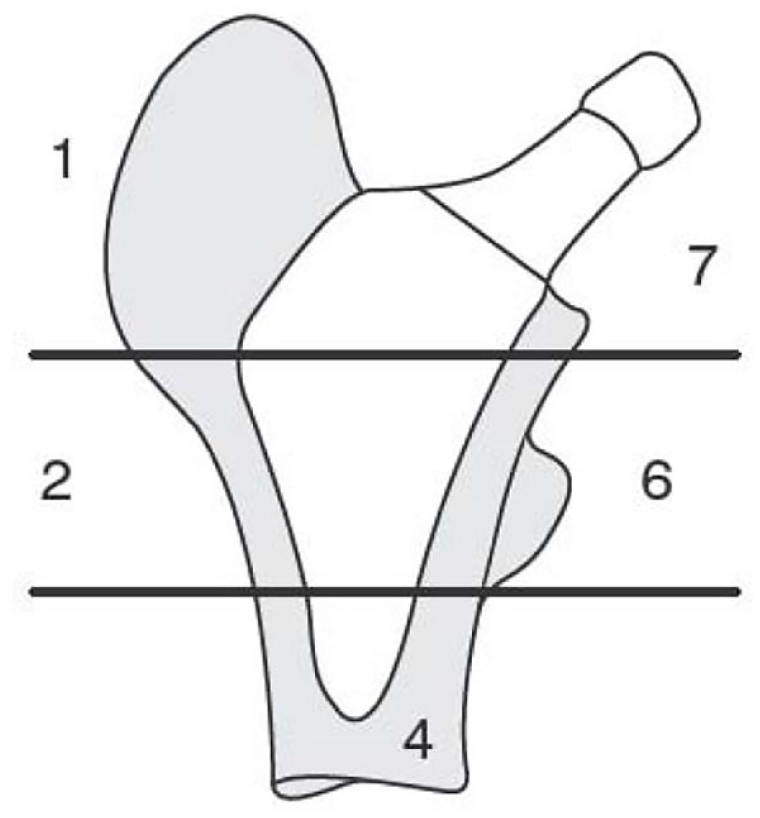
Modified Gruen zones for the uncemented ultra-short anatomical stem Proxima, without “classic zones” 3 and 5.
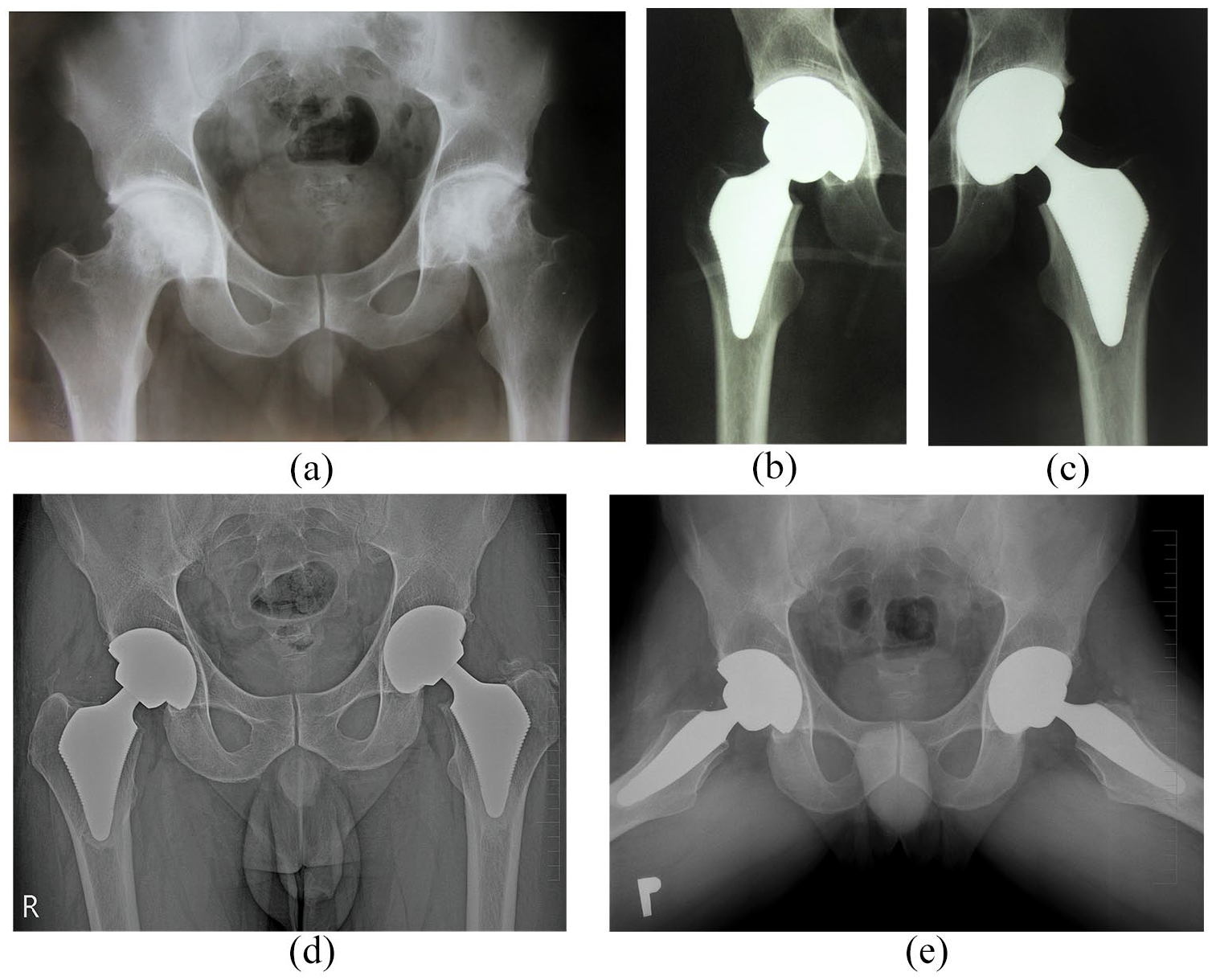
(a) Preoperative anteroposterior radiograph of 27-years old patient with bilateral osteonecrosis of the femoral head (post radiotherapy).
Proximal femoral stress-shielding was assessed according to Zicat et al. 16 Heterotopic ossifications were assessed according to Brooker’s classification. 17
Statistical analysis
All statistical analyses were performed using R software version 4.0.2 (R Core Team 2020). Continuous variables were expressed as mean and standard deviation (SD) as well as range. Dichotomous outcomes were expressed as the number of events and percentage. Normality of HHS data were confirmed using the Shapiro-Wilk test (p ˂ 0.05).
2-sided, paired Student’s t-test was used for statistical analysis of the pre- and postoperative HHSs. Statistical differences were considered to be significant when the p-value was <0.05. Relatively large effects (following the guidelines from Cohen, 1988) were reported in the previous studies for HHSs. A power analysis, using the R 3.5.0 (power package), indicated that a total sample of 15 patients-hips would be needed to detect large effects (d = 0.8) with 80% power, using a 2-sided paired t-test between means with alpha at .05. 18 Survivorship analysis was performed with the Kaplan-Meier estimator with end point at almost 10 years (105 months) after surgery (Figure 4).
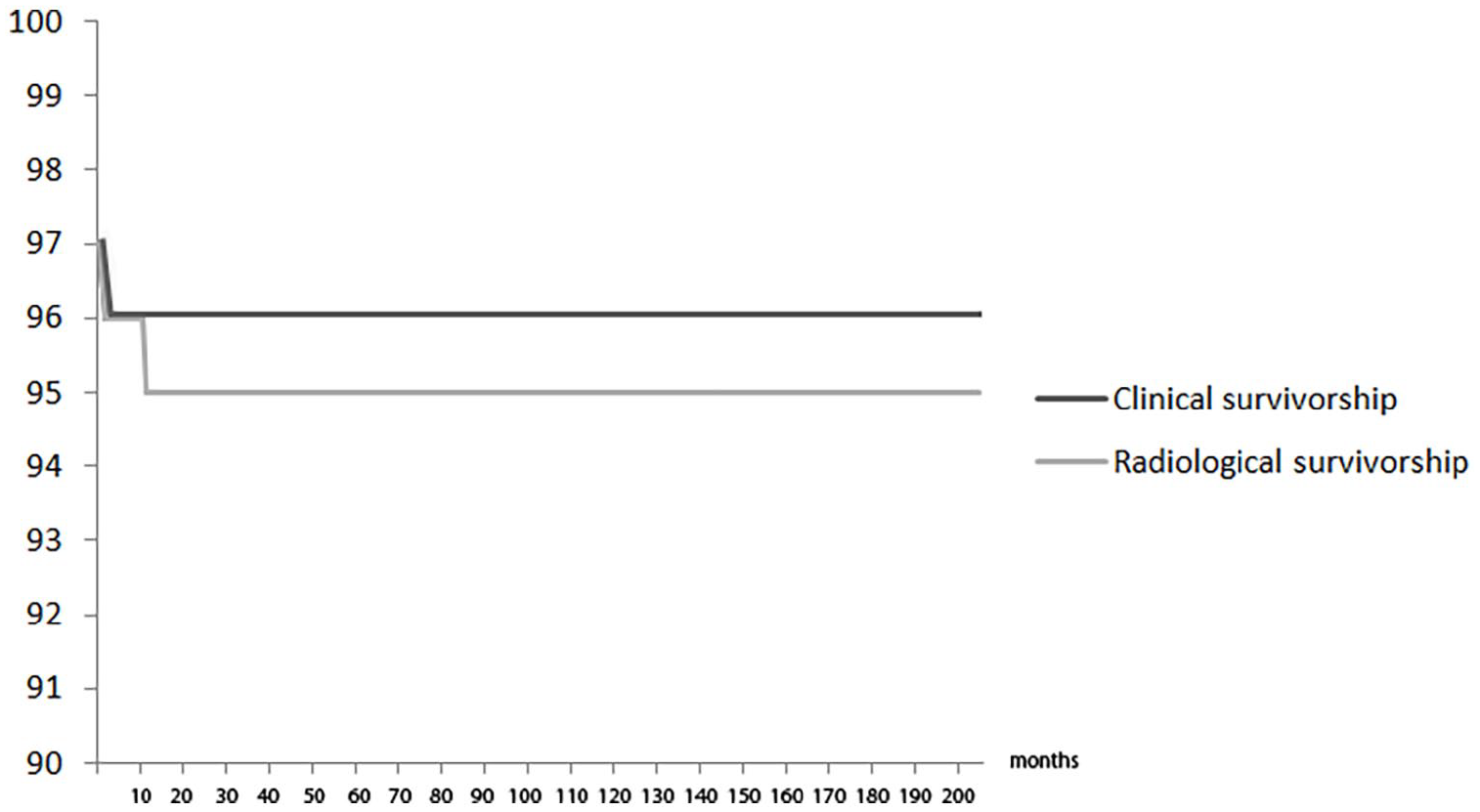
Kaplan-Meier clinical and radiological survival analysis of the Proxima stem.
Results
Clinical analysis
All 73 patients (97 hips) were followed, and the final evaluation was performed at a mean of 105.2 months (62–168 months, standard deviation [SD] 25.6 months).
There were 24 cases with bilateral and 73 hips with unilateral procedures. 64 patients were men and 9 were women. The mean age of the patients was 47.4 years (23–63 years, SD 9.0 years). The mean BMI was 28.4 kg/m2 (16.12–37.00 kg/m2, SD 4.3). The aetiology of ONFH was alcohol-induced in 55 hips (56.7%), corticosteroid-induced in 19 hips (19.6%), others (idiopathic, no underlying conditions) in 18 hips (18.6%) and radiotherapy in 5 hips (5.1%) (Table 1).
Patients’ demographic and details of the group with the Proxima stem.
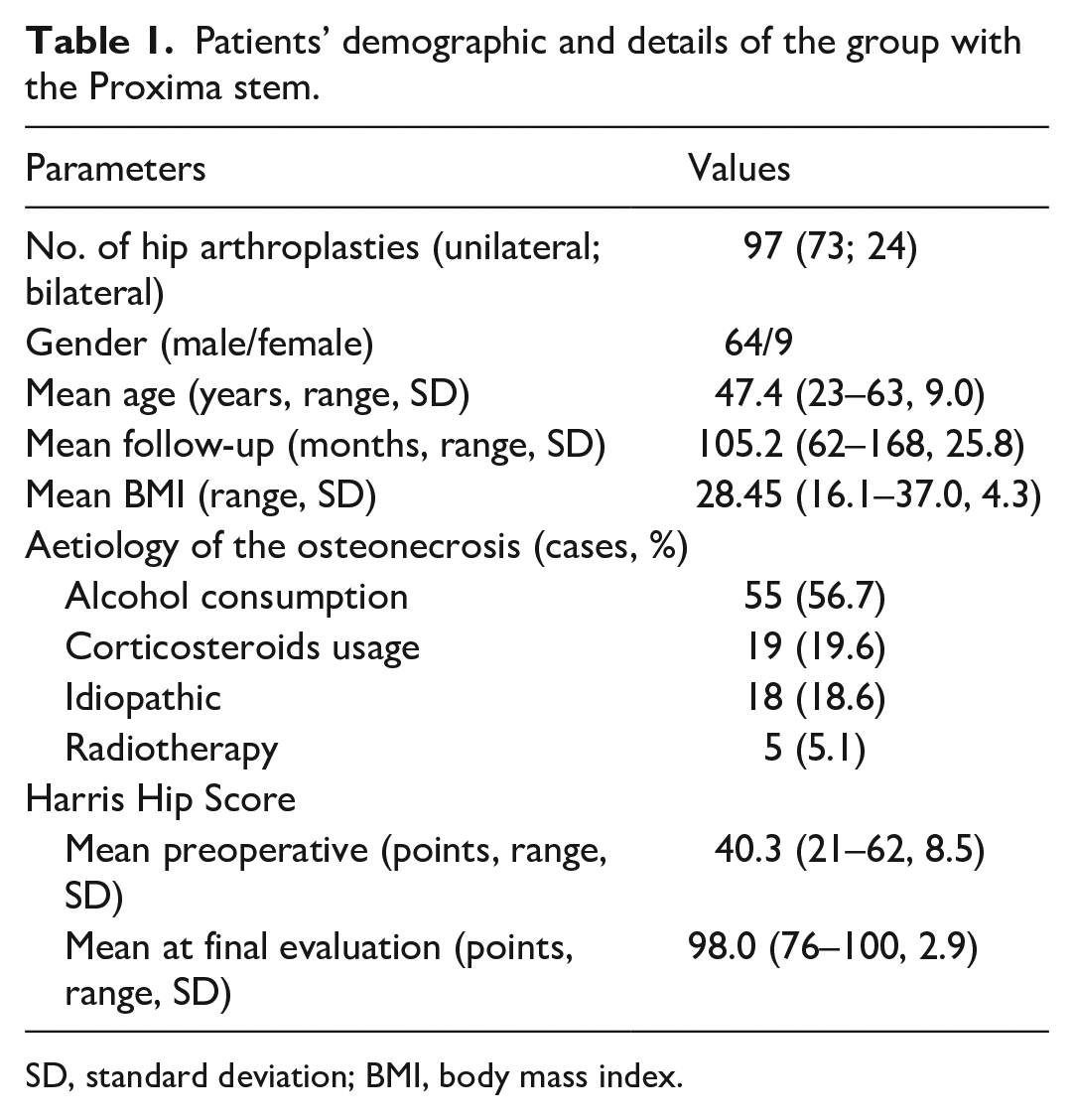
SD, standard deviation; BMI, body mass index.
The mean preoperative HHS improved significantly from 40.3 (21–62, SD 8.5) to 98.0 (76–100, SD 2.9) at final follow-up (p = 0.001). Finally, 56 patients (57.7%) had excellent hip scores (range 90–100 points), 39 patients (40.2%) had good scores (range 80–89 points), 2 patients (2.1%) had fair scores (range 70–79 points) and no patient had a poor score (<70 points).
LLD was 1.5 cm (average shortening) before the operation (range 0.5–2.5 cm, SD 0.8cm) and 0.5 cm (average elongation of the operated extremity) at final follow-up (range 0.5–1.5 cm).
Thigh pain was observed in one patient with a loose stem (1%).
Radiographic analysis
All evaluated hips were ONFN stages III or IV according to Ficat and Arlet. Dorr type A femur was found in 66 hips (68%), Dorr type B was found at 31 hips (32%). No femur type Dorr C was found. The initial cup position (lateral inclination) was on average 44° (range 40–50°) without cup migration during the whole follow-up. We found a radiolucent line of 1mm width in one cup (clinically asymptomatic) in DeLee-Charnley zones I–III. 19 This radiolucent line appeared on x-ray at 3rd postoperative month and was without progression at the last visit (12th postoperative year). The postoperative stem alignment was evaluated as normal in 82 hips (84.5%), and varus (to 10°) in 15 hips (15.5%). Migration (subsidence and varisation) was observed in 11 stems.
Stem fixation, using the criteria of Engh et al. 15 was osseously stable in 91 hips (93.8%), fibrous stable in 4 stems (4.1%) and loose in 2 (2.1%).
In those 2 radiologically loose stems (1 of them in a varus position of 10° postoperatively) we observed slowly progressive subsidence (>3 mm) with varisation to 20° and a radiolucent line around the whole stem. The further migration of one loose stem stopped after contact of the stem apex with the lateral femoral cortex 7 years after the surgery at a final follow-up of 132 months, the second stem continued to subside with thigh pain (final follow-up 108 months).
Radiolucent lines were also observed additionally in 4 stems. Patients remained pain-free and these stems exhibited fibrous stability, with the subsidence up to 2 mm and varisation up to 10° until the 6th postoperative month.
Another group of 5 stems show migration up to 2 mm with varisation to 10° during first 6 postoperative months without any other changes – these stems are considered as osseously stable.
Stress-shielding grade I, according to Zicat et al. 16 in modified Gruen zone 7, was found in 91 stems (93.8%); this phenomenon was not found in the loose or fibrous stable stems at the final follow-up.
Heterotopic ossification was diagnosed in 8 hips (8.2%); Brooker type I was found in 6 patients, type II in 1 and type III in 1.
Bony trabecular development was found in all osseously stable stems (Table 2) and their location evaluated in modified Gruen zones: in zone 2 in 65 hips (67.0%), in zone 4 in 63 hips (64.9%), in zone 6 in 63 hips (64.9%).
Bony trabecular development and radiolucent lines around the Proxima stem in modified Gruen zones.
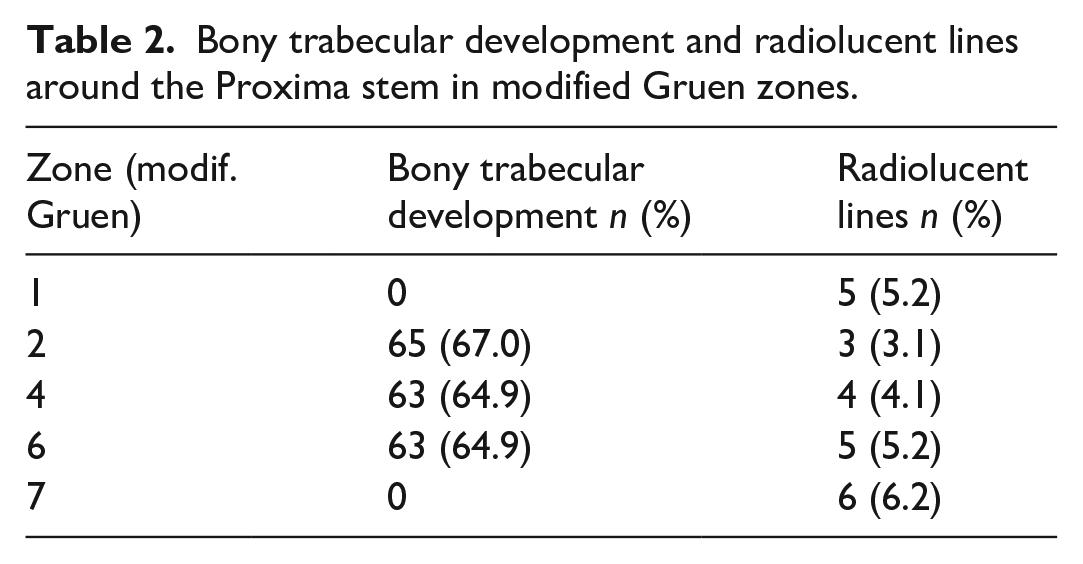
In patients with fibrous stable and loose stems, we did not find development of trabecular bone. In these 6 stems (6.2%) radiolucent lines were diagnosed: in modified Gruen zone 1 in 5 hips (5.2%), in zone 2 in 3 hips (3.1%), in zone 4 in 4 hips (4.1%), in zone 6 in 5 hips (5.2%) and in zone 7 in 6 hips (6.2%).
Complications and revisions
Complications were observed in 5 hips out of 97, with unilateral Proxima stem (5.2%), resulting in 2 revisions (2.1%).
Early infection (Staphylococcus aureus) occurred (2 weeks after the surgery) in 1 case. A successful revision was performed (debridement, implant retention, antibiotics). At the final follow-up (70 months) stable bony ingrowth, with a pain-free Proxima stem was observed.
In a second hip, revision was performed for instability (recurrent dislocation 2 months after the surgery). The stem was removed and a new larger Proxima stem with a high-offset was implanted.
A squeezing phenomenon occurred in 1 case, 3 years after the surgery. The patient was pain-free and clinically satisfied. At the last visit (144 months follow-up) the implant showed no signs of loosening, and the stem was osseously stable.
Both patients with radiologically loose stems were relatively satisfied and declined revision during the last visit.
Kaplan-Meier survival analysis indicated a clinical survival rate of 98.9%, with a radiological survival rate of 97.9% (Figure 4).
The survival for revision for aseptic loosening was 100%.
Discussion
The success of uncemented THA relies on osteointegration of the implants. The short stems have been designed for the use in patients (indicated for the uncemented stems) with the intention to: reduce the stiffness of the proximal femur; better proximal loading; reduce the risk of thigh pain; reduce the periprosthetic bone resorption; the preservation of bone stock early in the evolution of a hip disorder that might require multiple reconstruction surgeries over the course of a lifetime. 5 ONFH obviously affects younger patients, mostly men as also shown in our study. Reports on implant survival in patients with ONFH vary in the current literature. Swarup et al. 4 published outcomes of THA in young patients with ONFH. They assessed 204 hips in 135 patients. The implant survival after 10 and 20 years was 86% and 66%, respectively.
Santori and Santori 20 evaluated the results of 129 custom-made ultra-short cementless stems with a lateral flare without diaphyseal fixation (similar to Proxima stem) with a mean follow-up of 8 years. The mean age of these patients was 51 years. However, only 9 patients in this study were diagnosed with ONFH. In accordance with our results, the final HHS considerably improved with a survivorship of the femoral stem of 100%. The bony trabecular development was visible on the final x-rays in modified Gruen zones 2 and 4.
In a recent study dealing with the Proxima stem, the incidence of ONFH as a diagnosis for primary THA was 26.9% (35/130). The authors reported radiological survival of 98.5% and clinical survival of 100% after an average 10 years in the whole group of patients with a mean age of 45.5 years. The average HHS improved from 42.5 preoperatively to 98.8 at the final evaluation. Similar to our study, the authors reported mild migration and varisation in 23 stems (17.7%), which settled without any further progression by the 6th postoperative month. Radiolucent lines were observed in 5 stems (3.8%). 8
Gombár et al. 9 presented results of 86 hips with the Proxima stem in patients with an average age of 50 years. The incidence of ONFH was 51%. The average HHS improved from 40 to 91 by the final evaluation. In contrast to our study, they reported periprosthetic fractures in 3 hips (3.5%), with the need for revision in 1. Stem malalignment was observed in 10 hips (12%). Stem subsidence with osteolysis was observed in one case with undersizing. The overall stem survival was 97% after 7 years.
Kim and Park 5 published a study of the largest group of young patients with a Proxima stem implanted for idiopathic, or ethanol induced femoral head necrosis. They assessed 256 patients (335 hips) with an average age of 49.8 years. The femoral stem survival was 99% after an average 14.7 years. They reported primary varus position (more than 5°) of the stem in 22 hips (7%), femoral subsidence up to 2 mm in 2 hips and osteolysis leading to revision in 4 stems (1%). The average HHS improved from 41 to 94 at the final follow-up.
Mahmoud et al. 21 have described a stable migration pattern (slight subsidence and malalignment - varisation of the Proxima stem). We have found this phenomenon in 11 stems, 2 of them with progressive varisation and loosening while 9 stems are without clinical problems. The migration ceased progression after the 6th postoperative month.
Proxima stem (based on its design) was not suitable for severe dysplastic hips with Dorr type C femur. 8
Bony trabecular development around the Proxima stem has been rarely described. It occurred around the distal ½ of the stem (modified Gruen zones 2–6) and when this phenomenon occured, the stem was osseously stable.8,21 Our study revealed similar results.
Suksathien and Sueajui 22 described 83 hips with a Metha stem in patients with ONFH. The mean age of patients was 43.8 years, mean follow-up was 69.3 months. The average HHS increased from 44.7 preoperatively to 99.6 at the last follow-up. The Kaplan-Meier stem survivorship was 98.8%. Bony trabecular development was observed in Gruen zone 1 in 65.1%, in Gruen zone 2 in 69.9%, in Gruen zone 3 in 14.4%, in zone 7 in 1.2%, in zone 6 in 97.6% and in zone 7 in 81.9%, but the Metha implant has a different design from the Proxima.
Schnurr et al. 23 reported results of 231 THA using Metha stem with a mean follow-up of 5.3 years. The mean age of the patients was 53 years. The survivorship of the stem was 96.2%. They observed aseptic loosening in 2.3% stems. The incidence of stem revision was 3.8%.
Capone et al. 1 evaluated results of 37 hips with the Nanos stem for ONFH in patients with an average age of 51.5 years. The average HHS improved from 53 preoperatively to 90 at the final follow-up. The follow-up was 5.6 years. They did not observe loosening of the stem or the need for revision. They found stress shielding grade I in the calcar region in 9 hips.
Zeh at al. 24 reported 8-years survival of the Mayo stem in 16 patients with ONFN with mean age of 45 years. No stem subsidence or loosening was detected.
From the above-mentioned studies, it follows that the femoral stem survivorship in patients with ONFH is in the range from 88% to 100% at 10-years follow-up, with the use of different short stems.5,8,20 Our results are at the upper level of this range.
Similar to the published studies, we have observed significantly improved function of the hip, as evaluated using HHS. Bony trabecular development was observed mainly around the distal part of the stem in our study – in modified Gruen zones 2,4 and 6. This indicates the physiological load transfer through the proximal femur, as also shown by bone mineral density analysis in the study of Kim and Park. 5 We have observed stress-shielding phenomenon around osseously stable Proxima stems in zone 7, as was also reported by other authors.5,8,9,25–28 However, it is not clear at this stage, what could happen after 20–30 years if bone resorption in the calcar region (Gruen zone 7) will progress. Such a pattern might lead to short stem varisation, femoral offset increase and possible failure. On the contrary, initial varisation and subsidence, without any progression after the 6th postoperative month had not led to implant loosening at the last visit. When we retrospectively analysed 2 loose stems with progressive migration, we found a few possible factors for stem failure: undersizing (we used sizes 4 and 6, both high-offset), too early full weight-bearing, or low-grade infection. From the other 9 stems with early migration, 7 of them had had a standard stem variant and 2 had a high-offset variant. We did not observe perioperative, or late periprosthetic femoral fracture around Proxima stem in patients with ONFH. 29
The longer-term implications of Proxima stems with adverse radiological findings (if they are symptomatic) might be further migration, proximal femoral bone resorption and possible failure with the need for revision surgery. Further clinical monitoring should be performed to observe these findings.
Our study has some limitations. Firstly, it was retrospective in design, not randomized without a control group, so it is not possible to draw any direct conclusion on the performance of this implant relative to any other. Secondly, this study was not based on dual-energy radiograph absorptiometry, and so we were not able to exactly assess changes in bone density.
However, the study provides a long follow-up, and no patient was lost.
In conclusion, we report that primary THA in patients with ONFN with the use of Proxima stem has promising outcomes in the mid-term. The stem design enables the preservation of the proximal femur. The bony trabecular development confirms physiological force transmission through the proximal femur.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.