
Abstract
Background:
Greater trochanteric pain syndrome (GTPS) is a common problem with an incidence of 1.8–5.6 per 1000 population. Physiotherapy, anti-inflammatories, corticosteroid injections and surgery have all been described in the management of GTPS, with limited, temporal success. Extracorporeal shockwave therapy (ESWT) has been proposed as a potential non-invasive management option for this difficult presentation.
Method:
We ran a prospective, 2-arm, single-blinded, randomised control trial comparing focused shockwave therapy (f-ESWT) to an ultrasound guided corticosteroid injection. Primary outcome measure was the visual analogue pain score. Secondary outcome measures included the Harris Hip Score (HHS) and Trendelenburg test for function; SF-36 for quality of life (QoL); and a Likert scale question for subjective assessment of symptom improvement.
Results:
104 patients (10 males and 94 females), of mean age 61.5 years were recruited. 53 were randomised to receive ESWT and 51 to receive an image-guided injection. 11 patients were lost to follow-up. There were no significant differences in baseline scores between groups.
At 3 months, pain, function and QoL scores had improved in both groups but were not statistically significant. The Trendelenburg test was significantly improved in the f-ESWT group with 80% patients being negative compared to 20% at baseline (p < 0.001).
At 12 months, across all outcomes, the ESWT group had significantly improved scores compared to the injection group; VAS 37.1 versus 55.0 (p = 0.007, 95% confidence interval [CI], 6.3–30.8), HHS 69.7 versus 57.5 (p = 0.002, 95% CI, −20.0 to −4.6) and SF-36 52.4 versus 47.7 (p = 0.048, 95% CI, −9.31 to −0.04). The improvement in Trendelenburg test was maintained in the ESWT group, but the injection group had reverted to baseline (p < 0.001).
Conclusions:
We have shown f-ESWT is an effective treatment for patients with GTPS. We would advocate f-ESWT as an effective non-invasive treatment modality for this challenging patient population.
Keywords
Introduction
Greater trochanteric pain syndrome (GTPS) is a common problem with an incidence of 1.8–5.6 per 1000 population.1,2 GTPS has become an umbrella term for a range of clinical entities including tendinopathy, partial tears or avulsions of the gluteal tendons, snapping hip syndrome (coxa saltans) or inflammation of the bursae around the lateral aspect of the hip or ilio-tibial tract.1–5 It is more common in women than men with the ratio ranging from 4:1 up to 14:1 and primarily found in 40–60 year olds.3–6 Symptoms are usually unilateral, but can be bilateral. Any condition which causes altered biomechanics around the hip can predispose to the development of GTPS including leg-length discrepancy, osteoarthritis, total hip or knee replacement and obesity.1,3 Athletes can also suffer with GTPS, especially road-runners, with similar difficulties in treatment success. 7
GTPS can have significant impact on the patient’s quality of life. 8 Rest, non-steroidal anti-inflammatories, physiotherapy, corticosteroid injections, platelet rich plasma injections, 9 shock wave therapy, iliotibial band lengthening and surgical debridement (both open and arthroscopic) have all been described in the management with variable results.10–17
Corticosteroid injections are the current standard treatment following a trial of physiotherapy and analgesia, 18 and can be given in a primary or secondary care setting. Studies have shown that both image-guided and ‘blind’ corticosteroid injections give short-term benefits over physiotherapy, but the effects do not last longer than 1–3 months. It remains an invasive procedure with risks of infection, bleeding and tendon rupture.14–16,19–21
The use of Extracorporeal Shockwave Therapy (ESWT) has been described in the treatment of other forms of tendinopathies and enthesopathies such as plantar fasciitis, insertional and non-insertional Achilles tendinopathy and patellar tendonitis, with symptom improvement lasting into the medium term.22–26 There are 2 broad types of ESWT; focused (f-ESWT) and radial (r-ESWT). Focused shockwaves are generated by piezoelectric crystals, electromagnetic or electrohydraulic sources,24,26,27 and converge towards a point at a depth pre-determined by the probe attachment. The shockwaves have both a direct and indirect effect on tissues causing an increase in the release of analgesic substance P, increased neovascularity, inhibition of COX-II (thereby decreasing inflammation) and causing hyperstimulation of nerve fibres and blocking true pain signals through the gate-control theory. 27 Radial shockwaves are produced from compressed air and diverge as they exit the probe. It has been argued that r-ESWT is not true ESWT as the shockwave is not focused on a specific target and that the wave effects are too greatly dispersed in the superficial tisses. 26 Despite this, r-ESWT has been used to treat enthesopathies with good results. There is no evidence in the literature to suggest that f-ESWT offers superior outcomes to r-ESWT on superficial structures such as the patellar tendon although theoretically, f-ESWT is more suited to deeper structures as the depth of convergence can be varied. 28
Unlike in other tendinopathies,24–26 there is limited evidence to support the use of ESWT in GTPS. A systematic review by Barrett et al. 29 in 2016 concluded that there was not enough high-quality research available to draw strong conclusions from and that even the evidence available demonstrated moderate to high levels of bias. To date, 4 randomised controlled trials (RCTs) of ESWT to treat GTPS are reported; 2 using r-ESWT and more recently, 2 using f-ESWT. 14,19,30,31 All have shown significant improvements in pain and function scores compared to other treatment modalities.14,19 In 2011, the National Institute for Health and Care Excellence (NICE) assessed the evidence and issued guidelines on ESWT in the management of GTPS.32–34 They felt the available evidence was limited, and therefore further research studies were recommended with at least 1 year of follow-up.
The aim of this randomised control study is to discover whether f-ESWT is a more effective treatment for GTPS than the current standard treatment of a corticosteroid injection.
Patients and methods
Trial design
Participants were randomised into 2 arms: 1 arm received a course of f-ESWT and the other arm, an ultrasound-guided corticosteroid injection. Both groups underwent the same physiotherapist-supervised home exercise programme.
Randomisation was carried out using dedicated computer software (StratOs vs 1.34, Orthopaedic Institute Ltd, Oswestry, UK) and stratified by age, sex, and baseline pain (visual analogue scale [VAS]) and function (Harris Hip Score [HHS]) scores with bias set to 0.7. Concealment was not an issue in this study as a list was not used in randomisation. The trial adhered to the Declaration of Helsinki and gained approval from the West Midlands Ethics and Research Committee (Approval number 15/WM/0170). Trial Registration No. ISRCTN8338223.
Participants
Diagnosis and eligibility of all participants was confirmed prior to entering the study by 1 of 2 blinded consultants (BJB and RDB). Diagnosis of GTPS was made clinically in line with diagnostic criteria set out by Ege Rasmussen and Fano. 21 No participant in this trial had clinical signs to suggest snapping hip syndrome.
Participants were eligible for inclusion if they: (1) were aged 18 years or older; (2) met diagnostic criteria for GTPS; (3) failed conservative management. Exclusion criteria included: (1) presence of ipsilateral hip joint osteoarthritis on a plain radiograph; (2) any intervention targeted at GTPS within last 6 months (injection therapy/bursectomy/iliotibial band lengthening); (3) ipsilateral total hip arthroplasty; (4) contra-indications to ESWT treatment (pregnancy, anticoagulant therapy, advanced peripheral neuropathy, local infection, malignancy, unresolved fractures, a previous history of complications with ESWT); (5) recent history of hip trauma or sciatica; (6) unable to attend/comply with treatment/follow-up; or (7) participation in another clinical trial.
Research consent, baseline and follow-up assessments were performed by the same 2 blinded consultants. Randomisation was performed by another team member to ensure the assessing consultants would be blinded to the treatment received at all stages of the trial.
Interventions
f-ESWT
Participants received a course of f-ESWT by a trained physiotherapist. The patient was in a lateral position and the most clinically tender area identified. Using the Piezowave 2 (Impact Medical Ltd, Liverpool, UK) a F10G6 transducer probe with a 50-mm attachment was used to deliver 2500 shocks. The power level was set between 0.15–0.35mJ/mm2 depending on patient tolerance. This was repeated at weekly intervals for a total of 3 treatments.
Corticosteroid injection
Participants underwent an ultrasound guided corticosteroid injection. All injections were performed by the same consultant hip surgeon (SCL) in a clinic setting. Under aseptic conditions, 80 mg of Depo-Medrone (methylprednisolone) with 3.5 ml 0.5% bupivicaine and 3.5 ml 1% lignocaine were combined in a single syringe and injected using a long 21G (green) needle under ultrasound guidance to target bursae and tendon insertions whilst avoiding wholly intramuscular or intratendonous injections. Patients were monitored for 15 minutes following the procedure.
Physiotherapy
Following the randomised treatment, participants were seen by a single senior physiotherapist, assessed, and given a home exercise programme comprising of progressive slow repetitive exercises. General advice was given on continuation of regular painkillers and cryotherapy, and avoidance of anti-inflammatory medication for 6 weeks post intervention. Continuation of usual activity was allowed but patients were encouraged to refrain from sporting activity for a short period post-treatment.
Patients were reviewed 2 weeks after their initial assessment and then reviewed as necessary if they were having difficulties with the programme. All patients were assessed and followed up by the same physiotherapist to reduce bias. They also had access to an online video of their exercise programme, as well as a paper copy given to them at the start of their treatment. Patients had access to a helpline where they could speak with their physiotherapist should any questions arise.
Outcome measures
The primary outcome measure was the visual analogue pain score (VAS). 35 Secondary outcome measures included the Harris Hip Score (HHS) and Trendelenburg test to assess function, the 36-Item Short-Form Health Survey (SF-36) to assess quality of life and a Likert scale of symptom improvement for a subjective level of change.36–38 The Trendelenburg test has been shown to be highly sensitive and specific for the diagnosis of GTPS in the absence of radiographic features of degenerative hip disease. 37 Performance of the Trendelenburg test was standardised between the 2 consultant examiners (BJB and RDB); the test was performed by standing in front of the patient, hands on hands. The patient was asked to stand on 1 leg for a minimum of 30 seconds. Any increase in pressure, pain or tilt was deemed a positive response.
A patient diary was also issued to document completion of physiotherapy. Patients were reviewed at 3 and 12 months post intervention.
Sample size
A power study was undertaken prior to commencing this study and interim analysis performed to corroborate this. 39 Based on data extracted from Rompe et al., 14 Furia et al. 19 and Mahomed et al., 36 a power level of 80% and assuming a significance level of p = 0.05, a sample size of 101 patients was needed to ensure adequate power. A difference in VAS between the 2 treatments by at least 2 points was considered the minimum clinically important difference (MCID). 40
Blinding
This was a single-blinded study; the Consultants who consented to the trial and assessed the patients throughout the study were blinded to the treatment group.
Statistical analysis
The VAS, HHS and SF-36 scores were analysed using analysis of covariance (ANCOVA). The stratifying variables (age, sex and baseline VAS and HHS) were used as covariates in these analyses. Outcomes of the Trendelenburg test were compared using the chi-squared test. The symptom improvement scores (Likert scale) were analysed using a proportional odds logistic model. To help clinical interpretation we calculated the “effect size” of the difference between the 2 arms for each outcome. 41 An effect size of 0.5 for continuous variables or 0.3 for categorical variables is considered a medium effect size and is the minimum change perceptible by patients with a chronic disease.41,42 R v3.3.3 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses. A 2-tailed p-value of 0.05 or below was assumed to denote statistical significance.
Results
The trial has been reported in line with the CONSORT guidelines. 43 130 patients were assessed for eligibility (Figure 1). Of the 104 patients who consented to the trial, 53 were randomised to f-ESWT and 51 to the Injection group (Figure 1). Demographics for trial participants are shown in Table 1. Of note, the Trendelenburg test was strongly positive in both groups; 81.2% (f-ESWT) and 78.7% (injection). The follow-up rate at 3 and 12 months was 93% and 90%, respectively.
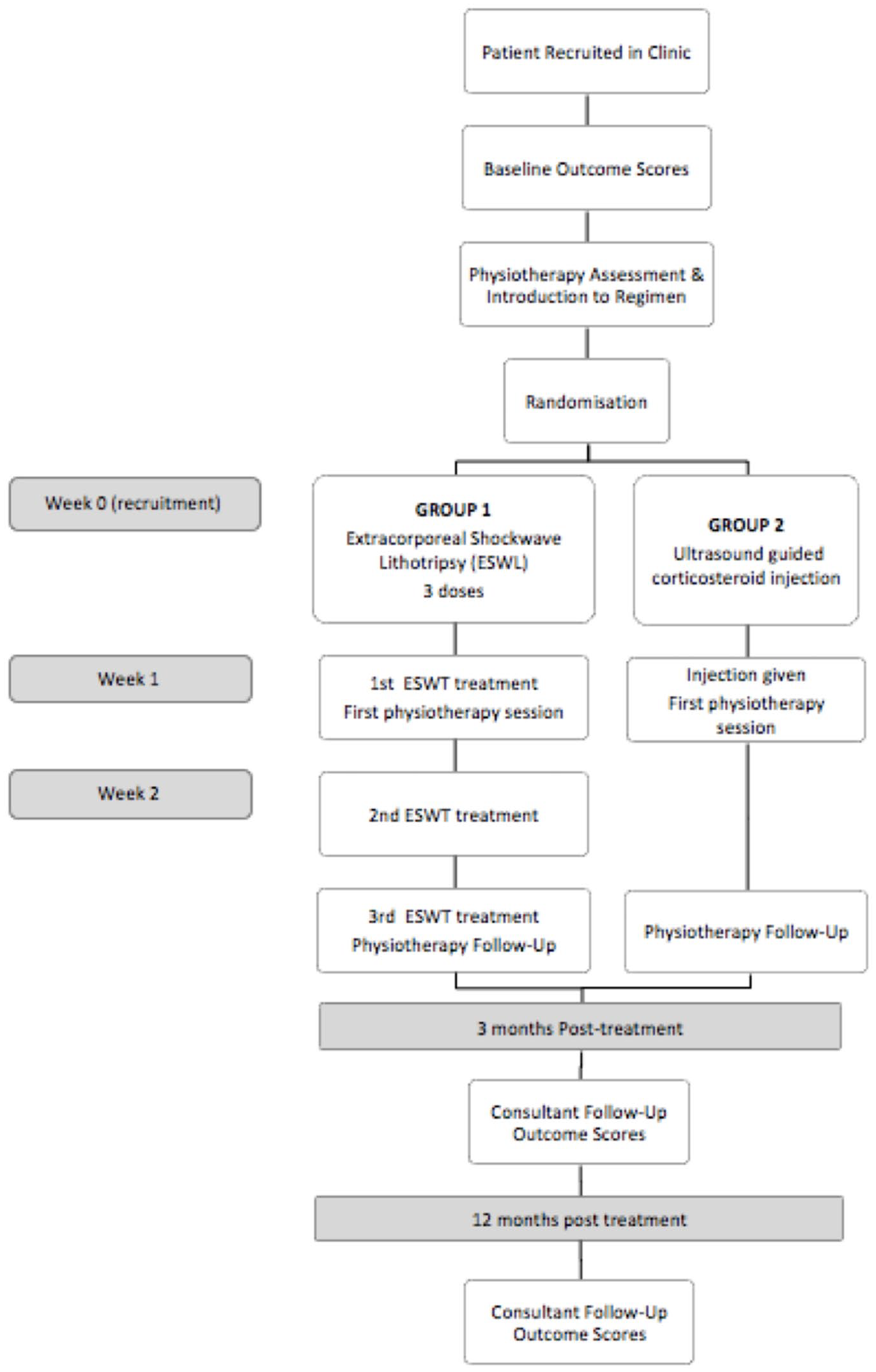
Flowchart showing trial protocol.
Demographics and baseline scores for both treatment groups.
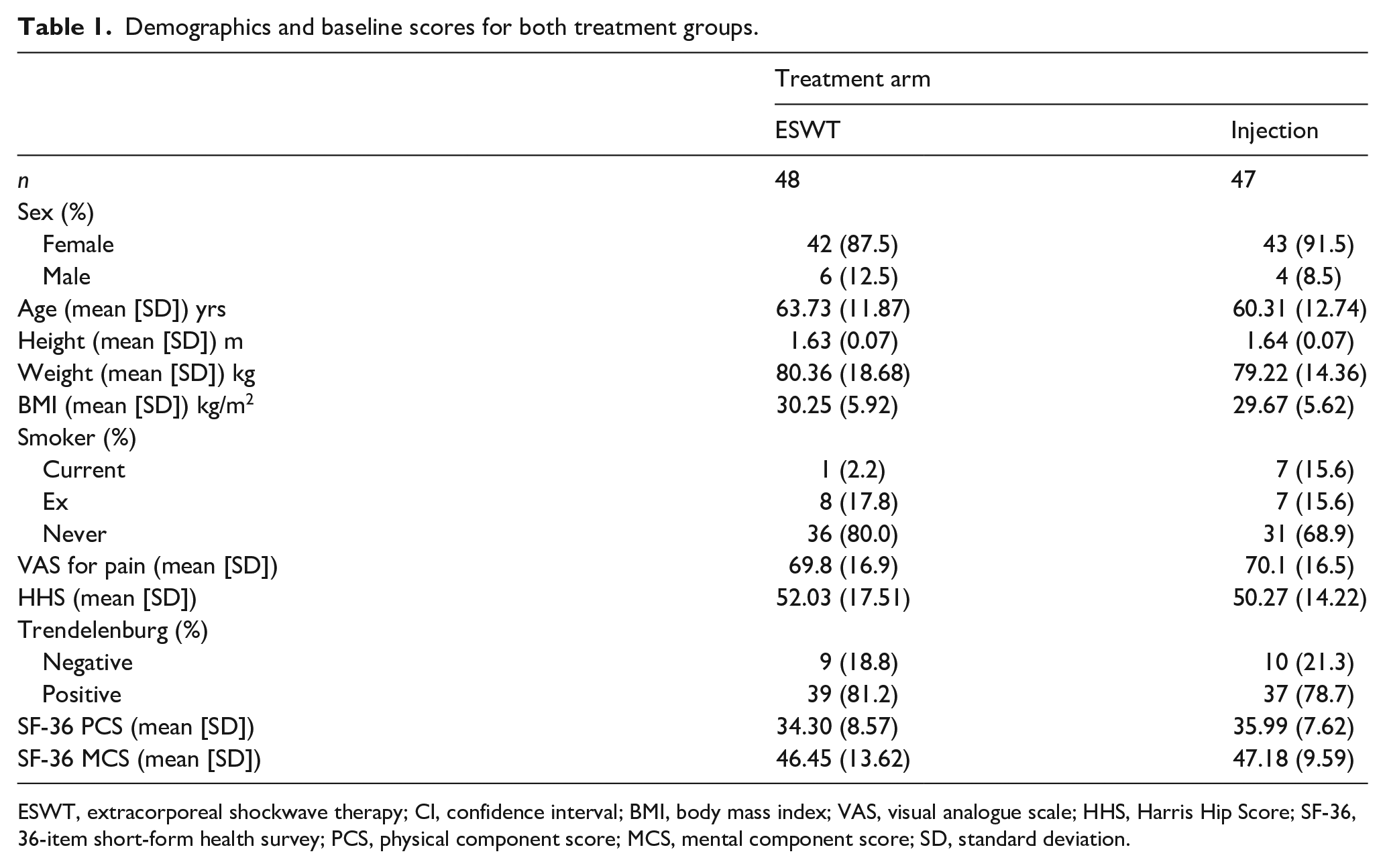
ESWT, extracorporeal shockwave therapy; CI, confidence interval; BMI, body mass index; VAS, visual analogue scale; HHS, Harris Hip Score; SF-36, 36-item short-form health survey; PCS, physical component score; MCS, mental component score; SD, standard deviation.
At 3-month follow-up, 2 f-ESWT and 4 injection patients withdrew from the study (Figure 2). There were improvements in all outcomes in both groups compared to baseline, but this was not statistically significant (Table 2). Both groups showed significant improvement in the Trendelenburg test with 84% of f-ESWT and 40% of Injection patients being Trendelenburg negative (p < 0.001, chi-square test).
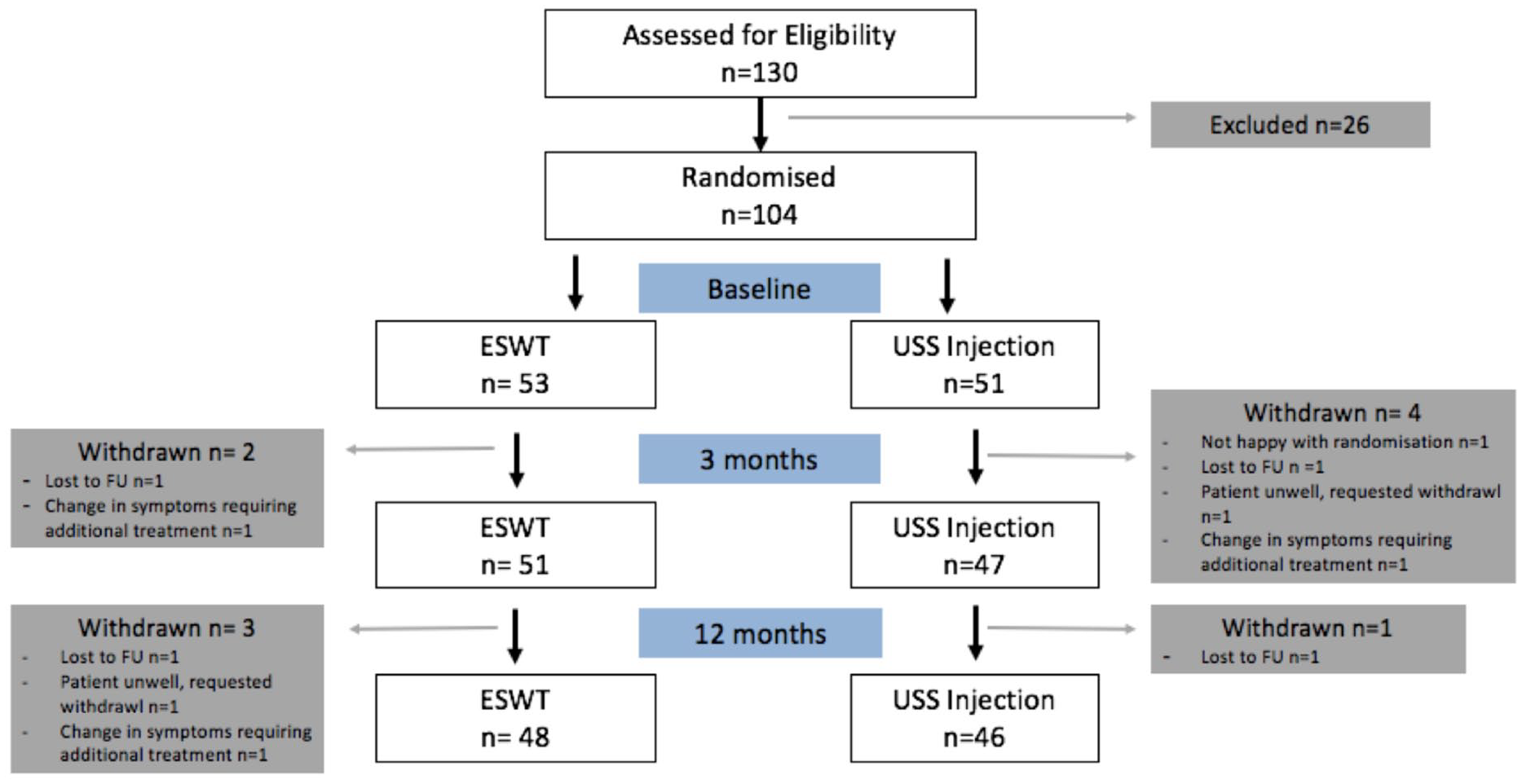
CONSORT diagram for the study.
Outcome scores at 3 months follow-up.
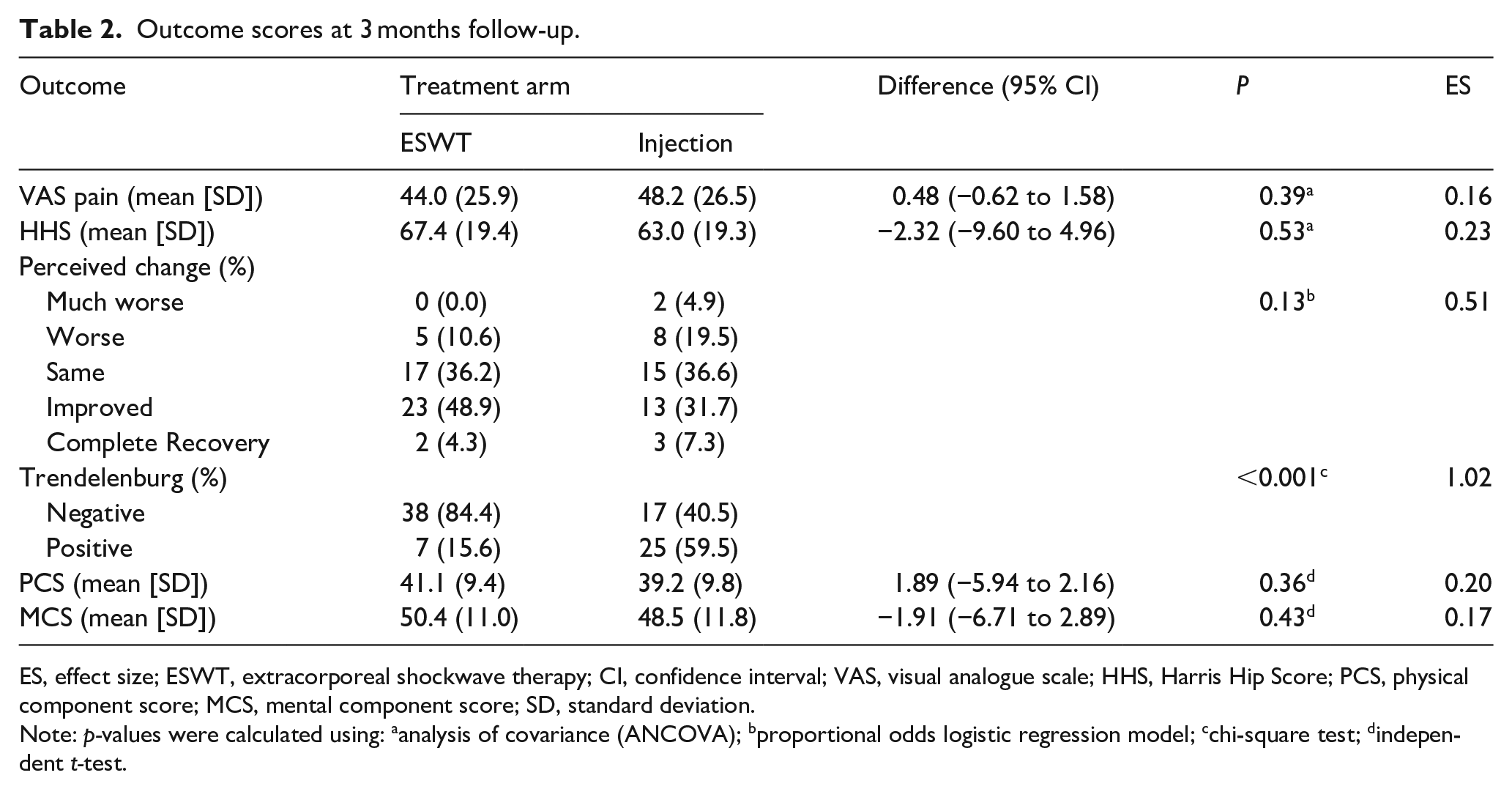
ES, effect size; ESWT, extracorporeal shockwave therapy; CI, confidence interval; VAS, visual analogue scale; HHS, Harris Hip Score; PCS, physical component score; MCS, mental component score; SD, standard deviation.
Note: p-values were calculated using: aanalysis of covariance (ANCOVA); bproportional odds logistic regression model; cchi-square test; dindependent t-test.
At 12-month follow-up, a further 3 f-ESWT and 1 injection patient withdrew from the trial (Figure 2). Outcome scores for 12 months are shown in Table 3. The f-ESWT group had significant improvement in their VAS and HHS, with an effect size above 0.5 (Table 3). They also perceived the change in their condition compared to baseline as significantly more positive, with 68% of the f-ESWT arm reporting some or complete recovery of symptoms compared to 24% of the injection arm (p < 0.001) and were more likely to have a negative Trendelenburg test (82% vs. 24%, p < 0.001)). The f- ESWT arm reported improvements in their mental outcome score (SF-36 MCS, p = 0.048) but no evidence was found for a difference in physical outcome between the groups (SF-36 PCS). No significant complications were reported in either group. Changes in VAS and HHS from baseline, 3 and 12 months are shown in Figures 3 and 4.
Outcome scores at 12 months follow-up.
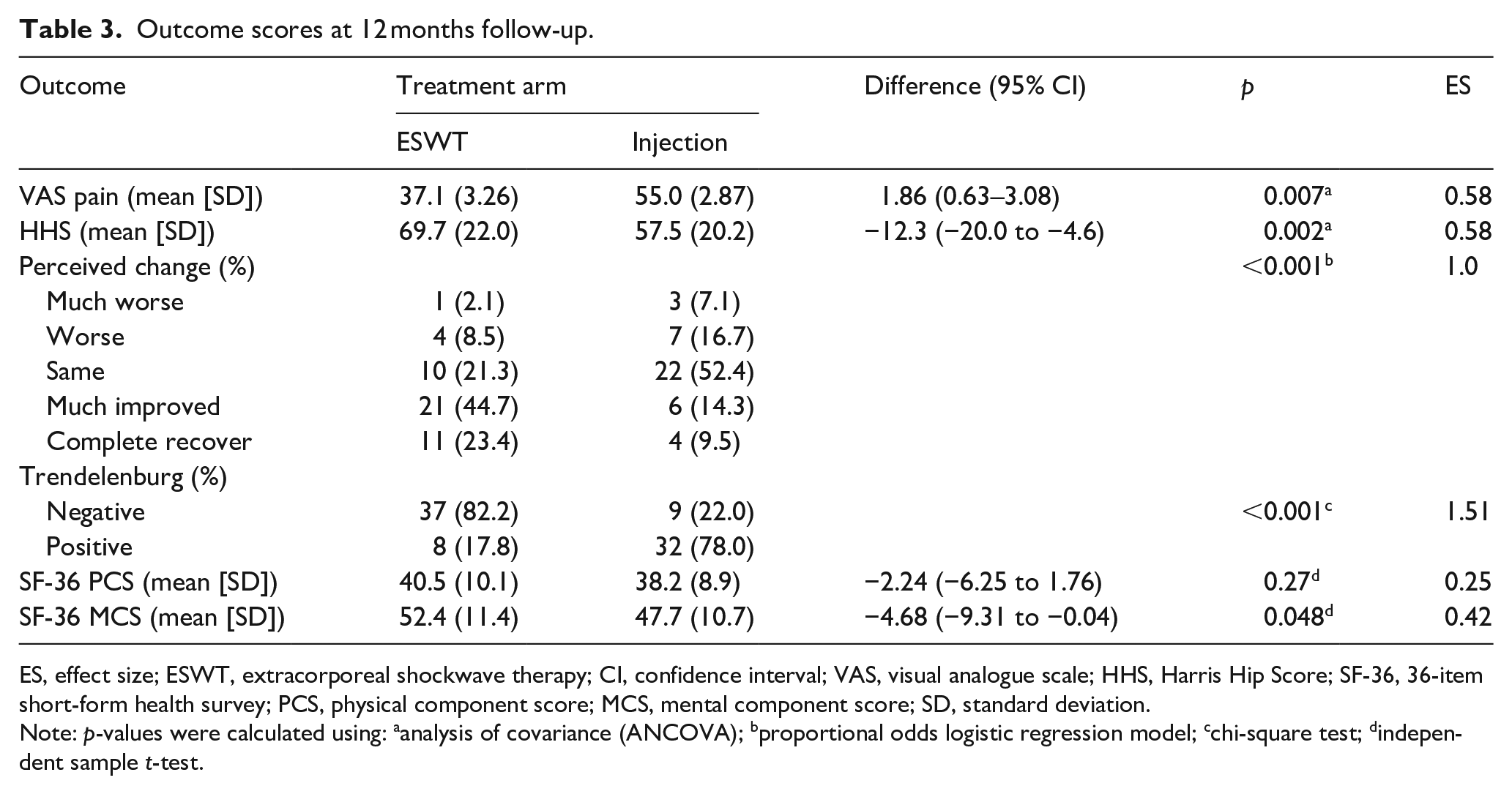
ES, effect size; ESWT, extracorporeal shockwave therapy; CI, confidence interval; VAS, visual analogue scale; HHS, Harris Hip Score; SF-36, 36-item short-form health survey; PCS, physical component score; MCS, mental component score; SD, standard deviation.
Note: p-values were calculated using: aanalysis of covariance (ANCOVA); bproportional odds logistic regression model; cchi-square test; dindependent sample t-test.
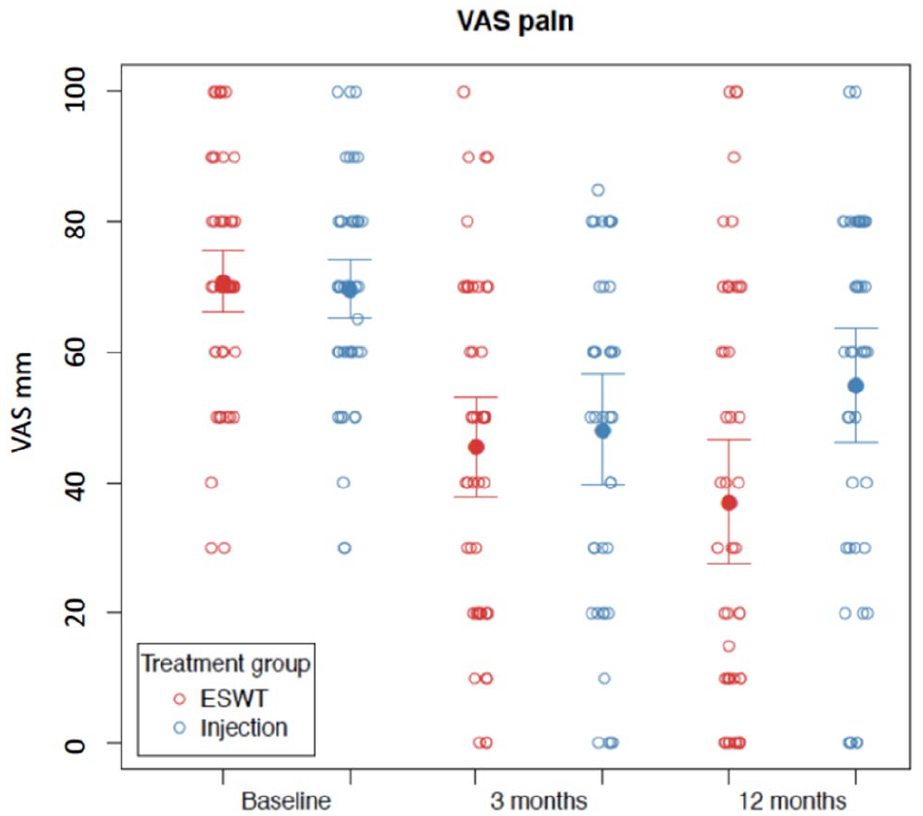
Means and 95% confidence intervals of VAS scores, together with the raw data (open circles), for both treatment groups at baseline, 3 and 12 months post treatment.
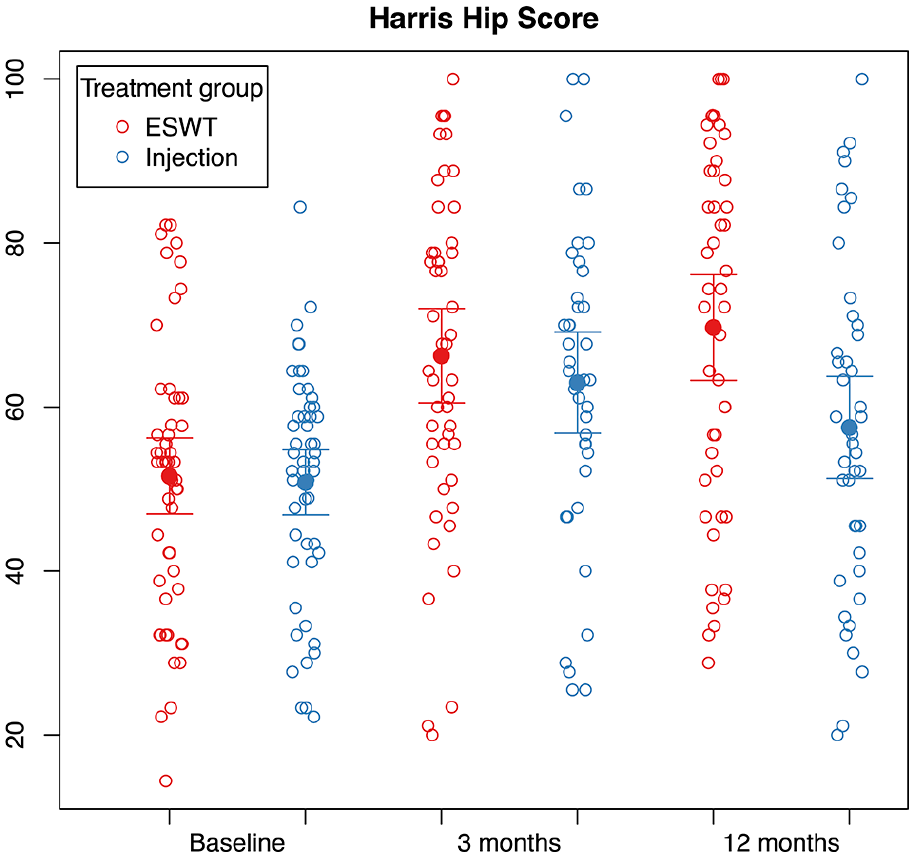
Means and 95% confidence intervals of HHS, together with the raw data (open circles), for both treatment groups at baseline, 3 and 12 months post treatment.
Patient diaries were used to confirm completion of the daily physiotherapy regimen. Of the 53 diaries (51%) returned, an average of 85.5% in the f-ESWT group and 81.7% of the injection group reported completion of physiotherapy exercises in the first 6 weeks following intervention. At 12 weeks, compliance in those who returned their diaries was and 81.7% and 79.8% respectively.
Discussion
This is the first study comparing outcomes of f-ESWT to a guided corticosteroid injection in 2 matched groups. We have shown f-ESWT gives significant improvements in pain, function and health-related quality of life scores at 1 year compared to a guided steroid injection. In all, 68% of participants who received f-ESWT reported complete resolution or much improvement in their symptoms compared to 24% of the injection group.
GTPS presents a difficult condition to treat with patients often having symptoms for months to years. Compared to the current gold standard in treatment, f-ESWT offers an effective non-invasive treatment option. Both treatment arms underwent a course of physiotherapy. Although the physiotherapy might have had a positive effect on the outcome, its effect was likely to be equivalent between the 2 groups and is therefore unlikely to have influenced the difference between the groups. We therefore believe that the difference in outcome scores is a direct effect of the f-ESWT.
Participants will have been aware that f-ESWT was a ‘new’ procedure and may already have tried a steroid injection in primary care. This raises the possibility of the improvement being due to a placebo effect. Whilst we cannot exclude the role of a placebo effect in the improved patient reported outcome data, the significant and sustained improvement in hip abductor muscle function (Trendelenburg test) cannot be wholly explained by this.
A recent systematic review by Schmitz 44 has shown ESWT to be a safe and effective therapy. Evidence for the use of ESWT in managing GTPS is increasing, with a number of studies found in the literature to support its use.
Ramon et al. 30 performed an RCT comparing f-ESWT to sham f-ESWT. Both arms completed a physiotherapy programme. They showed that f-ESWT is a safe and effective treatment with a significant improvement in pain scores at 2 months and improvement in functional and quality of life scores at 6 months.
Carlisi et al. 31 compared f-ESWT to ultrasound treatment and showed improved pain scores at 2 and 6 months but failed to show a significant improvement in functional scores.
Seo et al. 45 retrospectively reviewed the pain and functional outcomes of 18 patients with MRI documented evidence of gluteal tendinopathy who underwent f-ESWT. Both pain and function scores improved in the short and long term, with 55.6% patients reporting good or excellent results at a mean of 27 months post intervention.
A retrospective case series review by Sultan and Lovell 46 showed that 66.7% of patients with refractory GTPS treated with r-ESWT had improvement in their symptoms but noted a variable duration of symptomatic relief.
Furia et al. 19 performed a case-control study comparing r-ESWT to conservative management (33 patients in each arm). Significant improvement was seen in pain and functional scores in the ESWT groups versus the conservative treatment group at 1, 3 and 12 months. Rompe et al. 14 performed an RCT comparing physiotherapy, corticosteroid injection and r-ESWT in a total of 229 patients. At 1 month, pain score was significantly better in patients who had the corticosteroid injection versus r-ESWT or physiotherapy alone. At 4 months, r-ESWT showed significantly better results than corticosteroid injection or physiotherapy and at 12 months, r-ESWT and physiotherapy were better than corticosteroid injection. Our study supports the current findings in in the literature.
The use of corticosteroid injection is well documented for the treatment of GPTS.14–16,20,21 Brinks et al. 15 in 2011 performed an RCT with 120 patients comparing corticosteroid with expectant treatment. There was an early reported improvement in the corticosteroid group with 55% of patients stating they had improved compared to 34% in the expectant care group. However, by 12 months, there was no significant difference between the groups reporting 61% and 60% improvements respectively. The outcomes from the study Rompe et al. 14 also showed that there was early improvement in the corticosteroid group at 1 month compared to physiotherapy and ESWT. This effect however was not sustained. Radial ESWT and physiotherapy had better outcomes at 1 year compared to corticosteroid. Our study also supports this finding. At 3 months, the injection groups reported improvements in pain, function and quality of life scores, but this improvement was not sustained at 1 year follow-up. Cohen et al. 16 in 2009 showed no difference in outcomes whether corticosteroid injection is given “blind” (aiming for the clinical tender spot) or whether the injection is fluoroscopically guided. In our study, we used ultrasound guidance to avoid direct injection into muscle or tendon.
Other invasive treatment modalities have also been described including platelet rich plasma (PRP) injection and surgery. PRP injections are being increasing used in many forms of tendinopathy and enthesopathy with the thought that healing occurs with exposure to an increased concentration of platelet derived growth factors. 47 A recent systematic review by Ali et al. 9 has shown good outcomes at 3 and 12 months following PRP injection but the included studies were small with variable methodology. Although PRP injection is a form of conservative management, it does involve the withdrawal of a reasonably large volume of blood, 25–60 mls reported in the included trials, and so cannot be considered as non-invasive. Open and arthroscopic bursectomy have been described, with or without lengthening of the ilio-tibial band.10–13,48 These studies to date have been small and produced variable results with Govaert et al. 10 reporting recurrence and re-operation in 42% of patients. Slawski and Howard 11 Baker Jr et al., 12 Drummond et al. 13 and Brooker Jr et al. 48 have all shown significant improvement in Harris Hip function scores at 20–25 months post surgery. It should be noted however that surgical invention was performed in recalcitrant cases where conservative management had failed.
1 potential limitation of our study is the absence of a control arm who received no treatment or physiotherapy alone. We felt that our cohort of patients had already self-selected, having failed conservative management for a minimum of 6 months prior to inclusion in our study. Introducing a third arm to our trial would have required a larger sample size and would likely have led to recruitment difficulties with fewer patients per trial arm, potentially resulting in an under-powered study. A recent 3-armed randomised control trial by Mellor et al. 49 compared a wait and see approach to a steroid injection to education and physiotherapy. Although the wait and see approach group did demonstrate improvement throughout the study period, this improvement was not significant compared to the improvements made by the corticosteroid and education/physiotherapy group.
F-ESWT is a well-tolerated, non-invasive treatment which shows good improvement in pain and function scores out to 12 months. This is a treatment which could be repeated at intervals if symptoms recur and which could be administered in the community by a trained physiotherapist or by a local musculoskeletal assessment service, thereby decreasing the need for patients with lateral hip pain being referred to secondary care.
Footnotes
Acknowledgements
We thank the participants who volunteered to participate in the study. We also wish to thank Andrea Bailey, Raj Gilla, Tessa Rowlands and Jean Denton; members of the research physiotherapy team who administered the shockwave therapy; and Lisa Burgess-Collins and Teresa Jones from the research department for assisting with the running of the research clinics and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by orthopaedic institute limited.