
Abstract
Introduction:
This project aims to determine if an addition of a local anaesthetic pain pump for 48 hours postoperatively effects verbal pain scores (VRS), opioid usage and length of stay (LOS) after anterior approach total hip arthroplasty (THA).
Methods:
This was a single-centre, single-surgeon, randomised, parallel-group study with balanced randomisation involving 108 patients. Randomisation and blinding were computer generated into 2 groups: local infiltration anaesthetic (LIA) only (Control Group) and LIA+ continuous postoperative infusion of local anaesthetic for 48 hours via a pain pump (Intervention Group). Postoperatively VRS (first 30 minutes, 1 hour, 2 hours and every 4 hours postoperatively up to 48 hours), opioid consumption, length of hospital admission, antiemetic and laxative usage were recorded. Statistical analysis utilised independent sample t-tests and repeated ANOVA.
Results:
Demographics and duration of surgery were similar across both cohorts. On average, compared to the control group, the intervention group required 2 mg less of opioid consumption over 48 hours (p = 0.41). VRS between the 2 groups showed no statistically significant difference. Scores ranged from 0 to 7, with an average of 1.28 in the intervention group and 1.29 in the control group (p = 0.31). 9 patients in the intervention group and 10 in the control group required antiemetics. There was no difference in the LOS or postoperative constipation. No complications or adverse events occurred.
Conclusions:
Our study has shown the addition of a continuous postoperative infusion of local anaesthetic for 48 hours post an anterior THA had no effect on VRS, opioid consumption, LOS and antiemetic usage.
Keywords
Introduction
Orthopaedic procedures can be associated with significant painful morbidity, with 41% of patients reporting moderate to severe pain within 48 hours of surgery. 1 There are several strategies to decrease opioid post-surgery to prevent chronic pain such as regional anaesthesia, non-opioids with analgesic properties and local infiltration of anaesthesia (LIA).
The majority of studies reporting on LIA in hip arthroplasty, have involved the posterior and direct lateral approaches with minimal studies reporting on the direct anterior approach. Anterior total hip arthroplasty (THA) is becoming increasingly common, with the potential advantage of reduction in muscle damage, post-operative pain scores and hospital stay.2,3
The effect of LIA can potentially be extended with the insertion of catheters into the periarticular space, allowing for a continuous infusion of anaesthetic via portable contained delivery systems. The use of these systems has been shown to be safe and successful in hip arthroplasty utilising the posterior and direct lateral approaches, but the effectiveness is unknown in the direct anterior approach.4 –6
Our study aimed at assessing the efficacy of LIA with continuous infusion of local anaesthetic in hip arthroplasty via the direct anterior approach.
Methods
This was a single-centre, single-surgeon, randomised, parallel-group study with balanced randomisation (1:1) over 12 months. Inclusion criteria for participants enrolled in this study were patients undergoing an elective direct anterior THA for osteoarthritis over 18 years old and who had given verbal informed consent. Exclusion criteria included an allergy or intolerance to ropivicaine, complex regional pain syndrome (CRPS), and preoperative opioid use. All 108 participants received the same uncemented hip prosthesis (Quadra/Versafit, Medacta, Strada Regina, Switzerland).
Ethics approval for this study was obtained from the local institutional ethics board- St Vincent’s Hospital Melbourne Ethics Committee (HREC/17/SVHM/97).
Patients
Patients underwent a central randomisation via an online computer-generation into 1 of 2 groups. Every patient received 0.2% ropivacaine 2 mg/kg and 1:1000 adrenaline LIA. The control group received only LIA without the pain pump. Patients in the intervention arm had a catheter placed underneath the iliotibial band and into the hip joint. The catheter was connected to an elastomeric pain pump (On-Q, Kimberly-Clark) containing 400 ml of 0.2% ropivacaine. All pumps were commenced at a rate of 2 ml/hour and could be titrated up 14 ml/hour, based on the patient’s verbal reported pain. All pumps were removed after 48 hours.
The primary outcome was opioid consumption (total morphine equivalent dosage) over 48 hours postoperatively. Secondary outcome measures were the verbal reported pain score (VRS), length of hospital stay, antiemetic and laxative usage. Every patient had regular 1 g paracetamol 4 times a day, whilst opioids were only charted on an ‘as needed’ basis. VRS was taken at the same time points for every patient postoperative–30 minutes, 1 hour, 2 hours, 4 hours and then 4 hourly until 48 hours. Demographic data such as age, gender and duration of surgery was collected.
Statistics
The power calculation was based on previous studies reporting oral morphine equivalent consumption of 0–90 mg (min. 30 mg, standard deviation [SD] 23 mg) during 0–24 hours in patients receiving continuous wound local anaesthetic infiltration.7,8 For a mean difference of 27 mg between groups and SD of 23 mg a need for 49 participants in each group was calculated (alpha of 0.05 and statistical power of 80% [G*Power V3.1, University Kiel, Germany]).
Differences between groups in opioid consumption, pain, length of stay (LOS), antiemetic, and laxatives were analysed using Student’s t-test with a p-value of <0.05 considered to be significant, with intention-to-treat analysis. A repeated ANOVA (2 × 15) was performed to explore differences in pain between groups at the 15 time intervals with Bonferroni as the post hoc analysis.
Results
After exclusions, we analysed 108 patients with 54 in each of the control and intervention group (Figure 1). 2 patients did not receive the full 48 hours of continuous local anaesthetic as allocated due to early inadvertent catheter dislodgement.
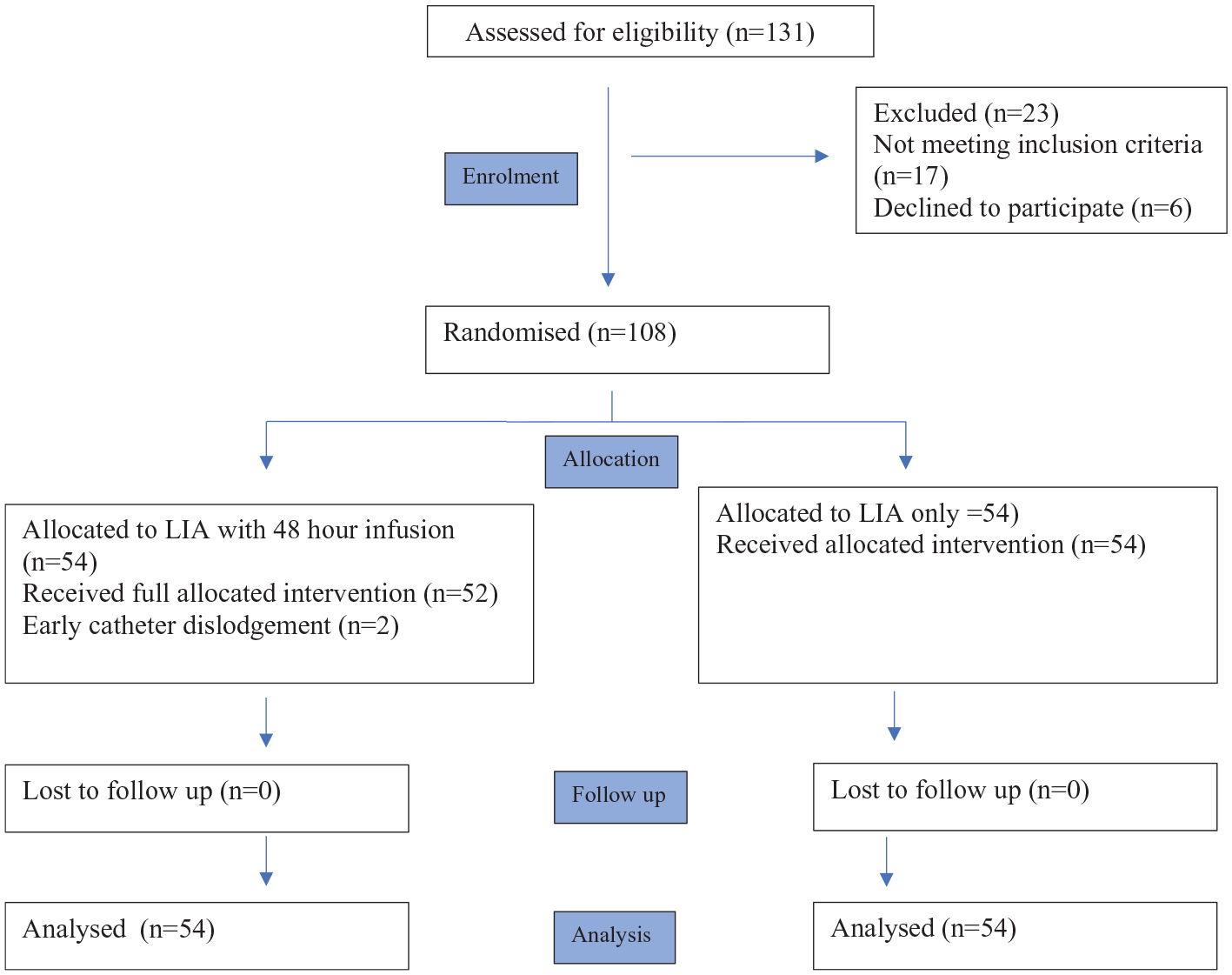
Flow chart of trial recruitment.
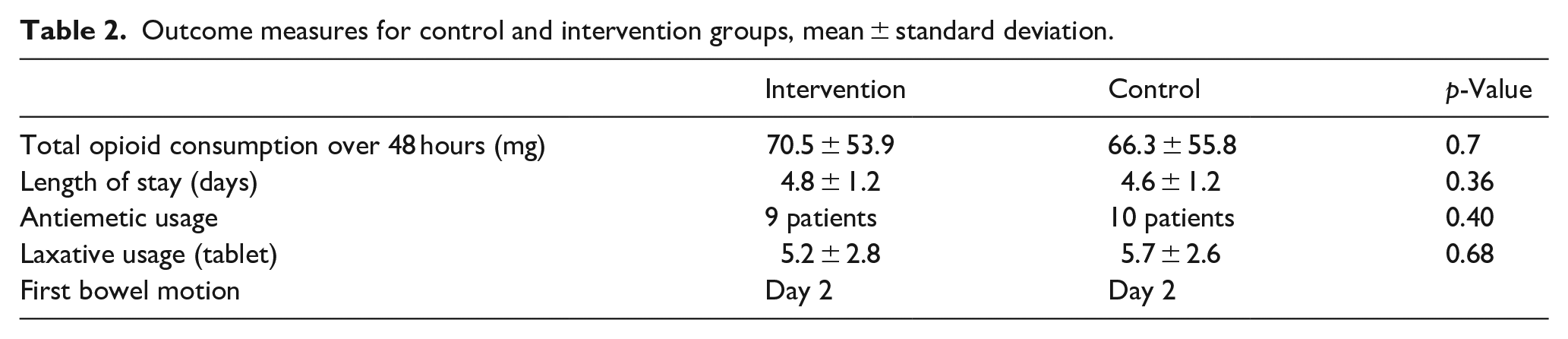
Patient demographics and duration of surgery were similar across both cohorts (Table 1). On average, patients in the intervention group used 179 mL in the pain pump, with a decrease in average opioid consumption by only 2 mg over 48 hours compared to the control group but this was not clinically or statistically significant (p = 0.41). Throughout the 48 hours, verbal reported pain scores were also similar between the 2 cohorts ranging from 0 to 7, with an average of 1.28 in the intervention group and 1.29 in the control group (p = 0.31) (Table 2) (Figure 2).
Demographics for control and intervention groups, means ± standard deviation.

Outcome measures for control and intervention groups, mean ± standard deviation.
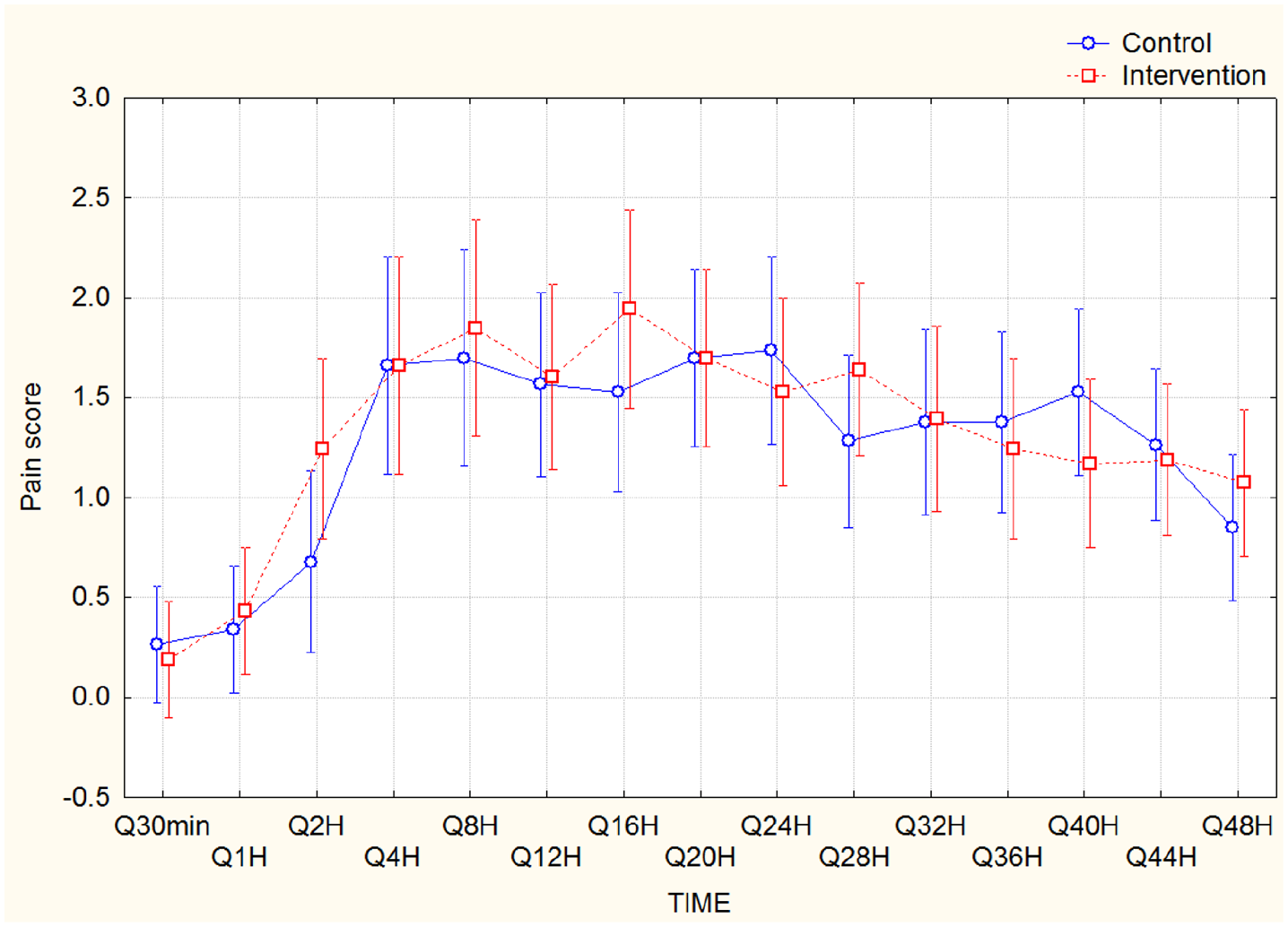
Verbal reported pain scores across 48 hours from 30 minutes to 48 hours postoperative (Q30, Q1, Q2,. . .,Q48H) for control and intervention groups.
Groups did not show significant differences between the pain scores throughout the time intervals. Repeated ANOVA analysis, however, showed significant lower pain score for both groups at the time intervals Q30min, Q1H compared to other intervals (p < 0.05) (Figure 2).
Postoperative nausea requiring anti-emetics was recorded in 9 patients in the intervention group and 10 in the control group. This was a once only dosage of intravenous ondansetron with no patient requiring multiple doses for ongoing nausea. There was no difference in the LOS in the acute setting or the number of days it took patients to have a bowel motion postoperatively. All patients were charted the same laxatives from day 1 postoperative of 2 tablets Docusate sodium and senna twice a day, with additional macrogol charted if patients were still constipated for more than 3 days.
There were no complications from the surgery. There were no adverse events or infection caused by the pain pump.
Discussion
Our study demonstrated that in hip arthroplasty via the direct anterior approach, the use of a continuous infiltration of anaesthetic via a pain pump in addition to local infiltration anaesthetic did not significantly reduce opioid consumption, verbal reported pain scores and LOS.
Both cohorts reported pain scores across 48 hours on average below 2. The control group which received LIA only during the surgery, reported consistently low values, and the addition of a continuous infusion of anaesthetic did not lower this further. Opioids were only charted on an as-needed basis, and the opioid usage correlated with the reported pain scores. The total amount of opioid usage in both groups was similar.
The infiltration of large volume local anaesthetic inhibits the conduction of pain at its origin and avoids systemic effects. However, the efficacy of LIA is still to be clearly established, with some studies reporting significant analgesic relief and reduction in the overall opioid postoperative consumption,4,7 –12 whilst other studies comparing LIA to placebo showing no benefit.13 –16 Randomised studies on LIAs have also reported differing effects on LOS and verbal reported pain scores.
Much of the literature reporting on the use of LIA is in total knee arthroplasty, and only a limited number on THA. Studies have demonstrated good results when comparing LIA to a placebo group, patient-controlled analgesia (PCA) and epidural catheters.4,7,12 However, these studies have been largely underpowered with small cohort sizes. Andersen et al. 9 eliminated a major confounder in evaluating the difference in pain scores between the treatment and control group by performing bilateral THA, however, total morphine requirements could not be assessed due to the design of their study.
To our knowledge, only 1 other study in the literature has looked at LIA in anterior THA. 15 Den Hartog et al. 15 compared LIA to a placebo control group and found no statistically significant difference in numeric reported pain score (NRS). Patients were given considerable amounts of multimodal analgesia of celecoxib, gabapentin and tramadol as well as rescue analgesia. Requirement of rescue analgesia was reported, but not total opioid consumption. The NRS reported was 2.9–3.1 and analysis was performed at 4 hours post-op, prior and after mobilisation.
Previous studies assessing the effect of a catheter providing continuous infiltration of anaesthetic to the surgical site have demonstrated little effect. Specht et al. 16 compared a catheter to a placebo and found the consumption of opioids in both groups were equal for up to 7 days, with no statistically significant difference in pain scores. Similarly, Solovyova et al. also found no difference compared to a placebo cohort if a multimodal analgesic regime was used. 6
Our study protocol did not utilise a multimodal analgesic regime, compared to protocols reported in previous studies involving celecoxib, gabapentin and tramadol. Despite this, the patients in our study reported very low VRS and required minimal opioids. This may be secondary to tissue sparing during the anterior approach.
Limitations in this trial include possible leakage from the catheter site which can decrease the amount of LIA infused, however this was documented as being only a small amount by nursing staff. We did not record pain scores related to physiotherapy or mobilisation, however all patients underwent the same post THA rehabilitation protocol.
Conclusion
In patients undergoing hip arthroplasty via the direct anterior approach, the use of a continuous infiltration of anaesthetic via a pain pump did not significantly reduce opioid consumption, verbal reported pain scores and LOS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.