
Abstract
Introduction:
Hip resurfacing remains a valid option in young male patients. The creation of the optimum cement mantle aids fixation of the femoral component. If the cement mantle is too thick the prosthesis can remain proud leading to early failure or if it penetrates too far into the femoral head, it may cause osteonecrosis.
Method:
18 of 96 femoral heads collected from patients undergoing total hip arthroplasty were matched for their surface porosity. They were randomly allocated into 2 different cementing groups. Group 1 had the traditional bolus of cement technique, while group 2 had a modified cementing technique (swirl) where the inside of the femoral component was lined with an even layer of low viscosity cement.
Results:
The traditional bolus technique had significantly greater cement mantle thickness in 3 of 4 zones of penetration (p = 0.002), greater and larger air bubble formation (6 of 9 in bolus technique vs. 1 in 9 in swirl technique, p = 0.05) and more incomplete cement mantles compared with the swirl technique. There was no relationship to femoral head porosity.
Conclusion:
The swirl technique should be used to cement the femoral component in hip resurfacing. Long-term clinical studies would conform if this translates into increased survivorship of the femoral component.
Introduction
Modern hip resurfacing (HR) is less popular now than in the early 2000s but remains an option in younger male patients engaged in heavy manual work or high impact sport. Cement forms an integral part in the fixation of the femoral component in the majority of designs and Campbell et al. 1 in 2006 proposed that a cement mantle of 2–4 mm is sufficient for fixation and >5 mm is probably excessive and can lead to femoral head osteonecrosis.
Studies of conventional total hip arthroplasty (THA) have shown that thicker cement mantles have reduced stress, strain and de-bonding of the bone-cement interface with retrieval studies of THA showing an increased incidence of cracks in thin cement mantles.2–8 However, applying information from conventional cemented THA to cemented HR is limited as the forces through each prosthesis are different.
Despite 7 investigations into the cementing technique of SRA there remains no consensus on the optimum cementing technique.9–15 Retrieval studies point to failures from excessive cement mantle thicknesses and femoral heads filled with cement. 16 The bolus technique leaves thick cement mantles with poor penetration and low viscosity cement fills the femoral head with cement.1,3,15,16
2 main cementing techniques exist in HR. These are the manual application of cement directly to the femoral head or filling of an upturned femoral component. Our aim was to analyse the cement mantle created using 2 differing upturned techniques.
Materials and methods
This study was approved by our local ethics committee and all patients gave their consent to enter the study.
Specimens
25 femoral heads were chosen from 96 femoral heads harvested from patients undergoing total hip arthroplasty at our institution. These 96 femoral heads have been previously studied. 17 In short, femoral heads were harvested after a standard osteotomy for THA, frozen at −80°C and defrosted at room temperature overnight before the experiments. Femoral heads were reamed to accept a size 50 Adept hip resurfacing. Once reamed, the exposed cancellous bone was cleaned by pulsatile lavage (Interpulse, Stryker). The porosity of each femoral head was then measured using the technique previously published. 18
25 femoral heads from the 96 perfectly accepted a size 50 mm Adept hip resurfacing. After visual inspection of the cut surfaces of the femoral heads, 18 remained which had no defect in their surfaces for instance from subchondral cysts. These 18 femoral heads were then matched for their surface porosity, making 9 pairs; each pair was then assigned to a cementing group by random coin toss. The mean porosity in group 1 (bolus) was 0.63 (range 0.4368–0.8482) and the mean porosity in group 2 (swirl) was 0.65 (range 0.5208–0.8463). There was no significant difference in porosity between groups p = 0.8).
Cementing techniques
Low viscosity cement (Palacos, Hereaus) was used in all experiments. The cement was prepared as per the manufacturer’s instructions. 10 g of cement was used in each group, by filling into an upturned femoral component which was measured after placing the femoral component and zeroed on weighing scales.
Group 1 (Bolus technique) had the traditional bolus technique. In this, the femoral component is part filled with 10 g low-viscosity bone cement and the component impacted onto the prepared femoral head after a thickened film of cement has developed on its surface. In group 2 (swirl technique) the inside of the femoral component was part filled with 10 g low viscosity cement. The femoral component was turned slowly in a clockwise direction whilst being tilted, so that an even layer of cement lined the whole interior of the femoral component). In both groups the prostheses were hammered onto the femoral head 2 minutes and 15 seconds after commencement of mixing with any excess cement that escaped from the sides was removed. There was no difference in the weight of the cement between the 2 groups (Student’s t-test, p = 0.538).
Cement mantle analysis
Cement mantles were assessed with CT imaging (Mx8000 Phillips Ct Scanner). In order to allow for computerised tomography (CT) analysis of the cement mantle, the femoral component had to be removed from the femoral head after cementation. To achieve this 1 g of petroleum jelly (Vaseline) was smeared inside the prostheses on all surfaces prior to cementing to allow removal following cement curing. There was no difference in the weight of petroleum jelly between the 2 groups (Student’s t-test, p = 0.538). The femoral component was removed with a retrograde hammer blow to its stem as it protruded from the femoral neck, no cement mantles were damaged during femoral component removal.
CT images were obtained of each specimen. Specimens were mounted on an 8-mm dowel peg protruding from a wooden timber and placed on the CT gurney. Ultra-high-resolution images were obtained scanning in 0.6-mm increments with a slice thickness of 1.3 mm using a Kv 0 120 and a MaS of 100. Axial coronal and sagittal reformatted images were obtained after the initial axial acquisition.
Cement mantle measurements
On the sagittal CT scans, the thickness of the cement mantle was measured in mm using the measurement tool on PACS radiograph viewing platform (GE Medical, USA). Measurements taken were for each slice across the femoral head at the level of the central hole. 4 measurements were recorded - 1 each side of the central hole and 1 at the centre of the chamfer for each side, for every slice available (Figure 1). Labelled as chamfer 1, top 1, top 2 and chamfer 2 as the image is viewed from left to right.
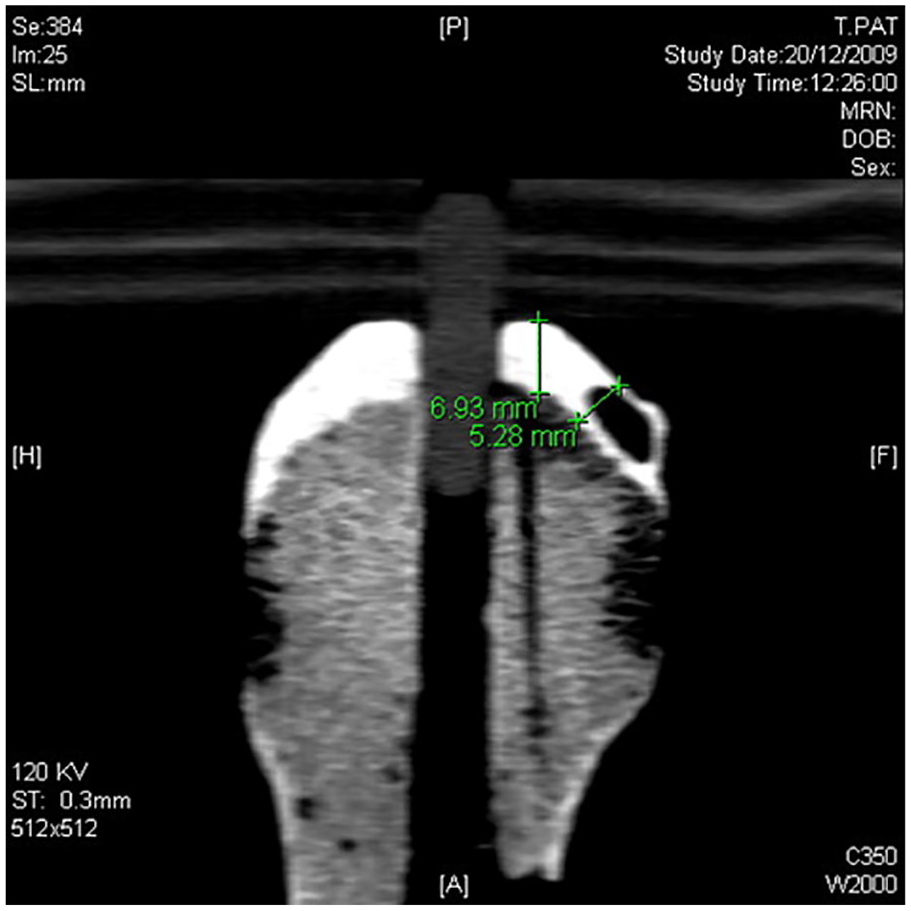
Measurement of cement mantle thickness on 1 side of the central hole.
The reliability of the cement mantle thickness measurements was confirmed by repeated measurements (Figure 1) on 10 specimens taken a week apart. Good reliability was identified (Pearson’s correlation 0.946 (95% confidence interval [CI] 0.820–0.993), p < 0.001). For each axial slice the completeness of the cement mantle was recorded and graded as complete or incomplete with any breaks in the cement mantle rendering it incomplete. The presence of air bubbles in the cement mantle was also recorded.
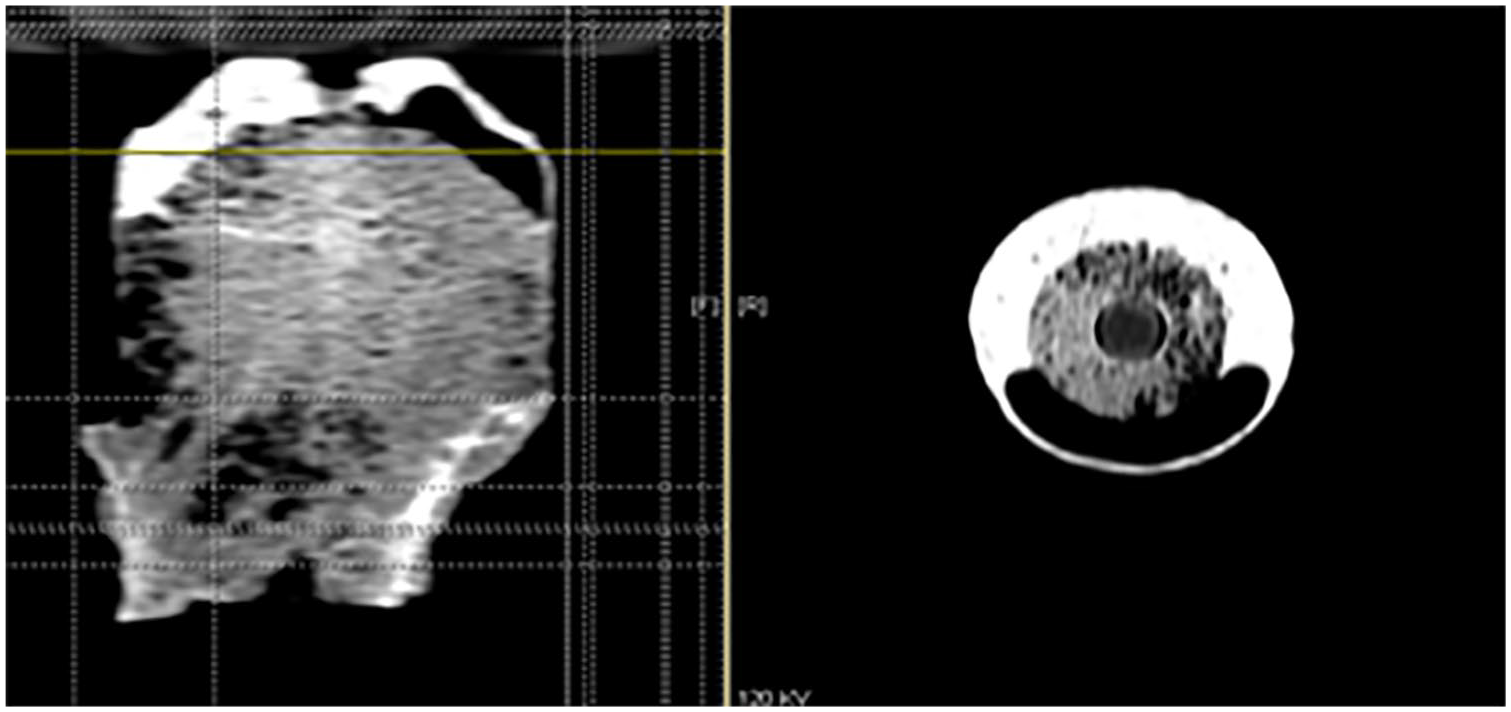
Cement penetration into the cancellous bone was recorded as present or not present for each axial slice scanned (Figure 2).
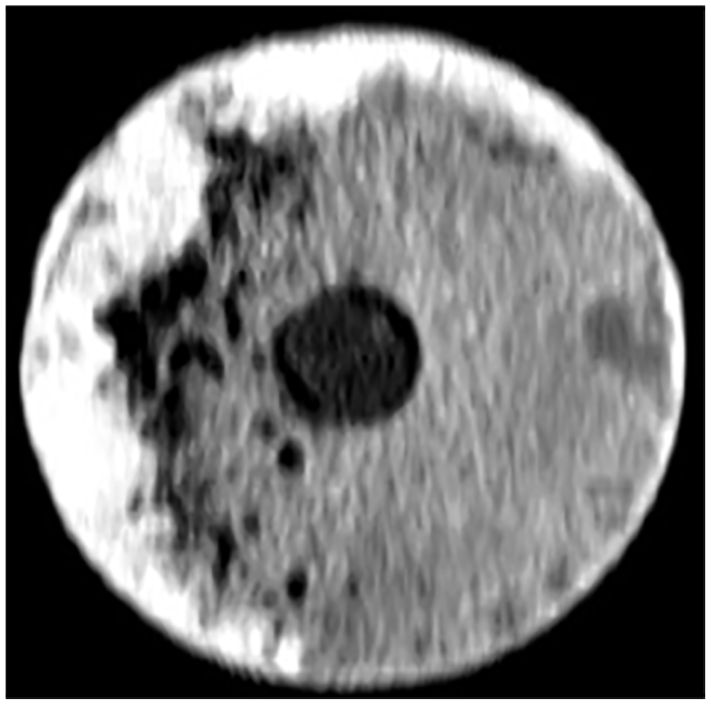
Axial CT slice of femoral head showing cement mantle and cement penetration.
Any breaks in the cement mantle rendered the mantle incomplete. The distance a complete cement mantle extended from the top of the femoral head to its most distant extent was recorded in mm by cross referencing the axial view with the sagittal view.
The presence of air bubbles was recorded on both axial and sagittal slices.
Statistics
Paired Student’s t-test analysis compared parametric data for; weight of petroleum jelly, weight of cement, length of complete cement mantles and cement penetration. Cement mantle thickness was correlated with porosity regardless of technique used and repeatability measurements were tested using Pearson’s correlation co-efficient. Spearman’s rank correlation coefficient compared porosity and penetration. Fisher’s exact test was used to compare bubble formation.
Results
Cement mantle thickness
The mean and maximum thickness of the cement mantle was greater in group 1 than 2 at all sites except at chamfer 1 (Table 1).
CT-derived cement mantle thickness measurements mm (SD).
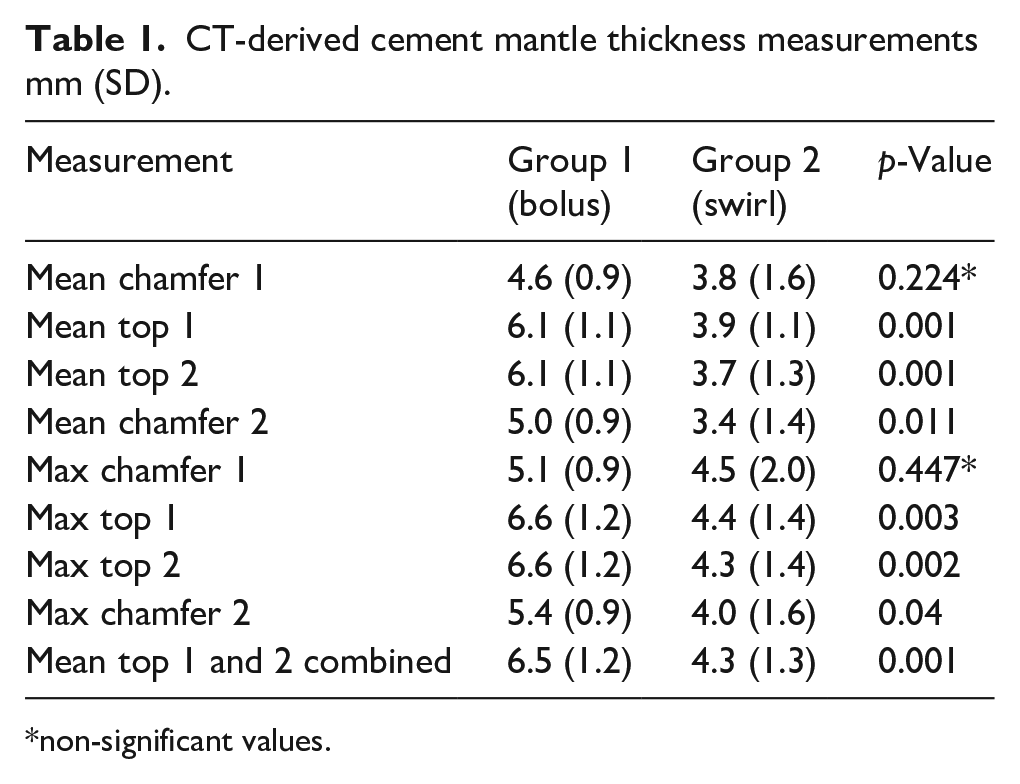
non-significant values.
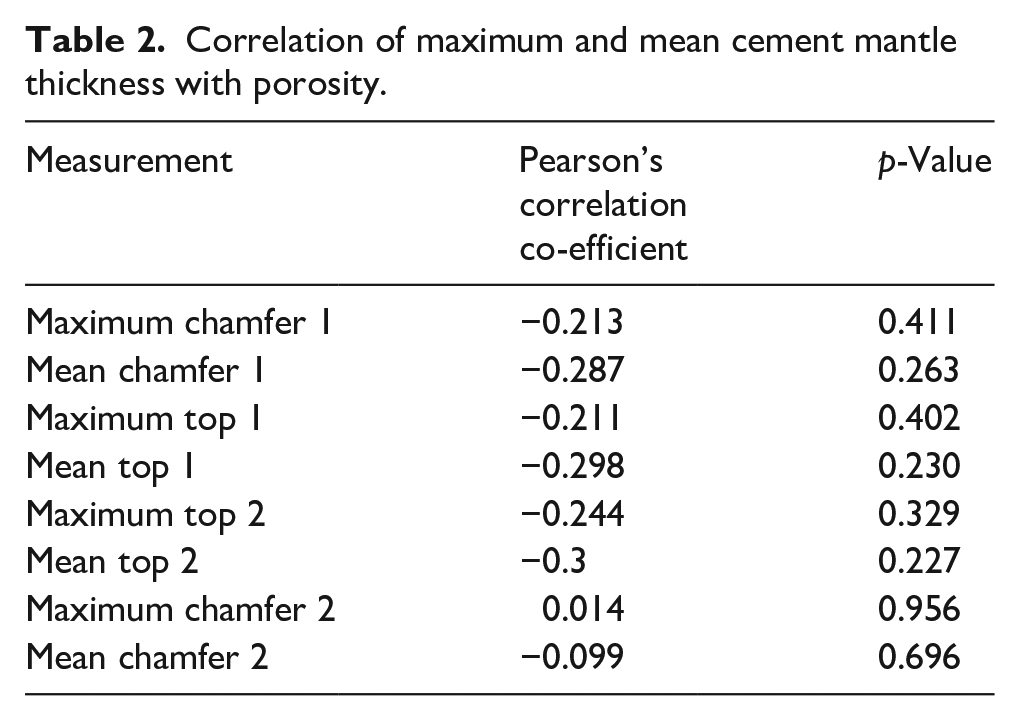
The cement mantle thickness was independent of porosity in both techniques studied (Table 2).
Correlation of maximum and mean cement mantle thickness with porosity.
Cement penetration
Cement penetration was present for group 1 in 27% of axial slices verses 65% in group 2. More cement penetration occurred in femoral heads from group 2 (Student’s t-test, p = 0.018). Cement penetration was not associated with porosity (Spearman’s correlation co-efficient 0.023, p = 0.933) (Figure 3).
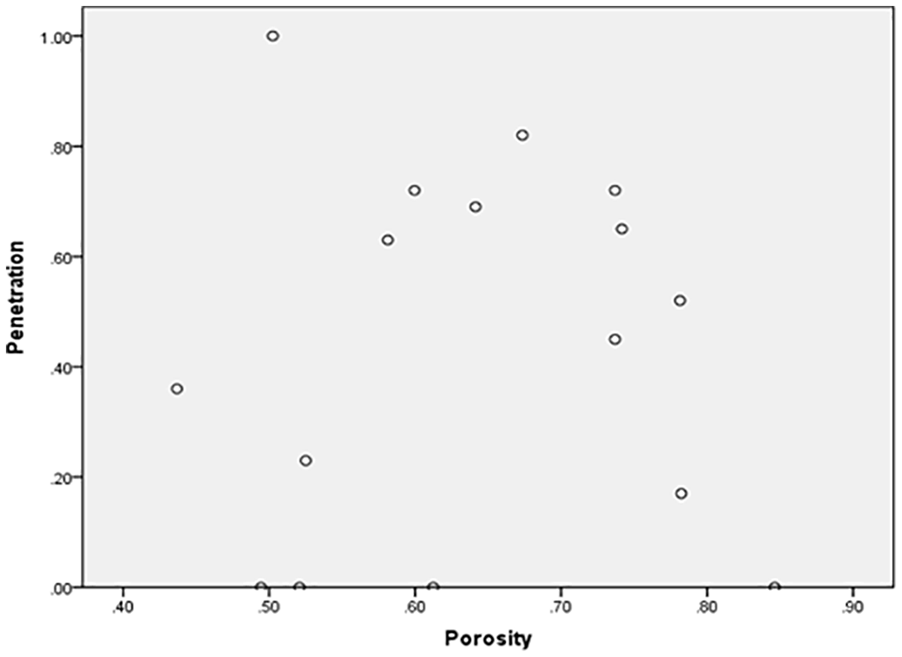
Scatter diagram of porosity against cement penetration.
Complete cement mantles
The cement was complete in its proximal distribution in all cases except 1 (Figure 4). As the mantle proceeded distally, it became incomplete in all cases. Neither technique achieved a complete cement mantle under the femoral prostheses - (a cement mantle of 18 mm in length on all sides of the femoral head). Proximally complete cement mantles extended a mean of 8.8 mm (standard deviation [SD] 1.6 mm) in group 1 and 11.9 mm (SD 1.8 mm) in group 2, before they became incomplete. Cement mantles extended further with the swirl technique (Student’s t-test, p = 0.002).
CT scan image of a large cement defect from air bubble - sagittal view cross-referenced to axial slice.
Air bubbles
Large air bubbles were present in 6 of the femoral heads in group 1 with only 1 air bubble present in group 2 (Fishers exact test, p = 0.05). Worryingly large air bubbles were seen with the bolus technique (Figure 4).
Discussion
2 cementing techniques were compared. The traditional bolus technique had significantly greater cement mantle thickness, greater and larger air bubble formation and incomplete cement mantles compared with the swirl technique. The cement distribution following the bolus technique was largely confined to the top of the femoral head with very little cement below the chamfer of the femoral head.
The swirl technique was not perfect. Cement extended below the chamfer of the femoral head but it was not complete in any experiment. It did, however, extend further than in the bolus technique. Greater cement penetration into the femoral head was observed with the swirl technique possibly because the cement around the sides of the prostheses obstructed its escape from the top.
The thicker cement mantles seen with the bolus technique left the femoral component proud, this has been associated with loosening and clinical failure.1,19
Previous studies have shown that manual application of cement produced the thinnest and most even cement mantles when compared to the bolus technique.9,10,13 6 of 9 experiments in the bolus group had large air voids in the cement mantles; only 1 other investigation into cementing technique identified the occurrence of air voids. 12 Combined filling of the femoral component with cement and manual application of cement to the femoral head had the lowest incidence of air voids. 12 Analysed retrievals have demonstrated air bubbles in cement mantles.9,19
A case in the swirl technique had a large air void. Both bolus and swirl techniques are not perfect. The problem remains, independent of technique, that when the femoral component needs to be impacted onto the femur, it has to be inverted and the cement that has been curing on its inside shifts. In the case of the bolus technique this shift seems to draw air bubbles into the remaining cement. In the case of the swirl technique, the cement has to shift to 1 side of the component, leaving 1 side of the femoral head partially devoid of cement, leaving incomplete cement mantles distally.
Acrylic bone cement is strongest in compression; the presence of air voids in the cement mantle will weaken the strength of the construct as air cannot support a prosthesis. In FEA of conventional THA cement mantles, increased peak stresses were associated with larger cement voids. Poorly supported acrylic cement subjected to increased stresses could fracture leading to loosening and ultimately migration of the prostheses although in practice this is not seen in retrieval of failed SRAs. 20
Several studies have compared high viscosity cement applied manually to low viscosity cement applied as a bolus technique.9,10,12,13 This comparison is difficult as it compares different cements used in differing techniques introducing too many variables into the experimental designs when practically only high viscosity cement can be applied manually in the operative environment.
Beaulé et al. 11 looked at the effect of component design on cement mantles. Comparing the Birmingham Hip Resurfacing (BHR) to 4 other designs with low and high viscosity cements he showed that the BHR regardless of cement type had greater cement penetration into the femoral heads.
There have been 7 studies into the cement mantle and SRA.9–15 5 have used human cadaveric femur,9,11,13–15 none have directly looked at the porosity of bone. Only 1 study controlled for bone density by using DEXA. 11
Baker et al., 16 have shown that increased porosity was associated with radiographic cysts and larger femoral heads. The cement mantle thickness and cement penetration were independent of porosity in both techniques studied. Only 18 cases were studied, but there was sufficient spread of matched porosities (0.43–0.85) to potentially show a difference. This concurs with the observations of other authors who found cementing technique to be independent of pore size and bone density.10,11
Limitations of the study are that there was no control over the force of impaction, but this is unlikely to have an effect, as the prostheses were impacted with moderate hammer blows until no further movement occurred in all cases, replicating the intra-operative environment. Reproducibility of the CT-based cement measurements was good suggesting that the experimental method is robust. However, the method identifies thickness of cement mantle but does not access its strength.
Conclusion
Neither cementing technique studied was perfect. The swirl technique was superior in terms of not leaving the component proud, better distal fixation and superior complete cement mantles.
Further work should focus on defining the optimum cement mantle and then designing the best cementing technique to achieve this. The cementing technique must provide stable fixation of the prostheses, allow its complete seating, avoid air bubble formation (cement voids) and not fill the femoral head with cement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.