
Abstract
Background:
Sciatic nerve palsy is a rare but devastating complication following total hip arthroplasty (THA). While the use of the direct anterior approach is increasing, limited data exist regarding sciatic nerve palsy and surgical approach. The purpose of this study was to determine the factors and outcomes associated with sciatic nerve palsy (SNP) after THA.
Methods:
A retrospective analysis was performed at a single institution of 7 SNP that occurred in 4045 THA via direct anterior approach and 10 SNP in 8854 THA via posterior approach, being operated between 01 January 2017 and 12 December 2021. SNP patients were matched 1:5 to patients without SNP. Medical records were reviewed for demographics including age, gender, body mass index (BMI), comorbidities, and preoperative indication. Additional workup of SNP patients including advanced imaging and reoperation were documented. Recovery grades were assigned to all SNP patients at most recent clinical follow-up.
Results:
5 of the SNP were complete and 12 partial. They occurred as frequently with the direct anterior (0.17%) and posterior approach (0.11%, p = 0.5). The presence of femur cables and reoperations were associated with SNP (p = 0.04 and p = 0.002, respecitvely). Age, gender, BMI, comorbidities, and surgical indication had no effect on SNP. 4 of the 17 affected patients had almost complete recovery at latest follow-up.
Conclusions:
The incidence of SNP was similar in direct anterior and posterior approach. Surgeons should counsel patients regarding the risks of SNP regardless of the used approach.
Introduction
Sciatic nerve palsy (SNP) is the most commonly encountered motor nerve injury following total hip arthroplasty (THA) with an incidence of 0.7–1.9%. 1 Although rare, SNP can have devastating clinical consequences for patients and is a frequent cause of medical malpractice litigation following arthroplasty surgery. 2 Known risk factors for SNP after THA include developmental dysplasia of the hip, female sex, and significant limb lengthening. 3 However, nearly 50% have no known aetiology. 4 As the number of arthroplasty surgeries is expected to rise, surgeons seek to provide solutions that best balance risks and benefits to patients. 5
The direct anterior approach (DAA) for THA is rapidly growing in popularity. A 2018 survey of American Association of Hip and Knee Surgeons found that 40% of respondents were using DAA, an increase of 12% compared to 8 years prior. 6 DAA proponents state that the approach might be associated with enhanced recovery after surgery and more accurate component positioning through intraoperative fluoroscopy. 7 Conversely, the DAA might be associated with more complications, like early revision and lateral femoral cutaneous nerve injury. 8 Despite a significant increase it its utilisation, a paucity of data exists regarding the prevalence of SNP after DAA.9,10
The purpose of this study was to answer the following questions: (1) is there a difference incidence of SNP after THA using the DAA or posterior approach (PA); (2) what are the factors associated with a SNP after THA; (3) What is the clinical course and subsequent outcome of patients who develop SNP after THA?
Material and methods
Ethical approval was given from our institutional review board (ethical committee number FWA00009165). 17 SNPs after 12,899 primary THAs (0.13%) in 11,536 patients were reviewed retrospectively. The operations were performed at a single institution between 01 January 2017 and 12 December 2021. Simultaneous bilateral THAs were excluded. No postoperative SNP patient had a history of a SNP preoperatively. Medical records were reviewed for age, gender, laterality, body mass index (BMI), American Society of Anesthesiologists (ASA) score, surgical approach, type of anaesthesia, operative time, and inpatient or outpatient THA.
The 17 patients with SNPs were matched to 85 primary THAs without SNP by age, gender, BMI, surgical approach, and ASA score. Medical records were reviewed for diagnosis, use of intraoperative injectable analgesia, blood loss, haemoglobin drop, blood transfusions, postoperative complications, and preoperative comorbidities. History of alcohol abuse was defined by the National Institute on Alcohol Abuse and Alcoholism. 11 Radiographs were reviewed for intraoperative placement of cables and leg-length discrepancy compared to the preoperative leg length and compared to the contralateral side postoperatively using the criteria described by Clark et al. 12
Additionally, medical records were reviewed for SNP characteristics, including complete or partial, and location of partial SNP. Additional data, such as electromyography and nerve conduction study (EMG/NCS), recovery of SNP, and clinical follow-up, were obtained. All patients received a motor exam immediately postoperatively that was graded on a scale of 0–5 and patients with a SNP received serial motor exams at each follow-up. 13 Complete SNP was defined as 0/5 strength in the extensor hallucis longus (EHL), flexor hallucis longus (FHL), tibialis anterior (TA), and gastrocnemius, with minimal or no sensation in the regions innervated by the superficial peroneal, deep peroneal, and tibial nerves. A partial SNP was defined as having at least 1/5 motor function in the EHL, FHL, TA, and/or gastrocnemius. Sensory exams were graded as sensation intact to light touch (SILT), diminished, no sensation, or paresthesia. All patients without SNP had 5/5 motor and SILT sensory exam in all sciatic nerve distributions postoperatively. The most recent available clinical data was reviewed and categorized into the following outcomes: No recovery, minimal recovery, partial recovery, near complete recovery, or complete recovery.
Demographics
The demographics were similar between patients with SNP and matched controls. Use of spinal anesthesia (p = 1.0), operative time (p = 0.1), and outpatient surgery (p = 1.0) were not risk factors for SNP (Table 1). Mean follow-up of patients who sustained a SNP was 1.5 years, with 9 of the 17 patients having minimum 12-month follow-up and 4 patients having minimum 2-year follow-up.
Patient demographics.
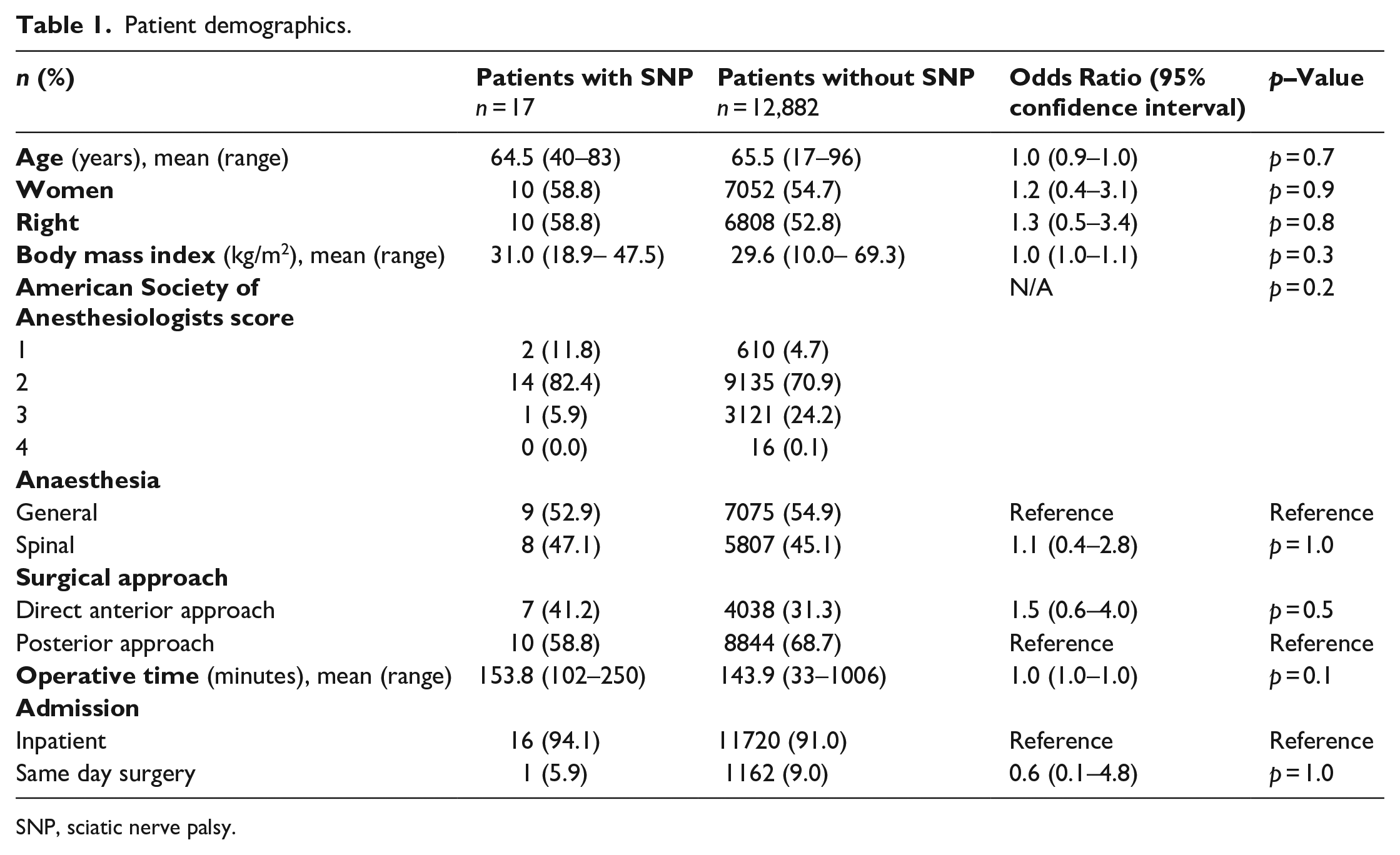
SNP, sciatic nerve palsy.
Statistical analyses
Matching was performed for the DAA and PA THAs separately to ensure a 1:5 ratio for both approaches. R was used to calculate propensity scores and perform 1:5 Mahalanobis distance matching by age, gender, BMI, and ASA score. Python was used for the statistical analysis. Cohorts were compared using chi-square and independent-samples t-test. Odds ratios (OR) and 95% confidence Intervals (CIs) were calculated. Firth’s correction in R was used to calculate OR and 95% CI when there were 0 instances of a condition. 14 A Mann-Whitney U-test was used to compare motor exams. An alpha level of 0.05 was used.
Results
Incidence of SNP
7 SNPs occurred in 4045 THA with DAA (0.17%) and 10 in 8854 THA with PA (0.11%), respectively, There was no difference in the incidence between the approaches (p = 0.5, Table 1). 5 patients (29.4%) had complete and 12 patients (70.6%) partial SNPs, all involving only the peroneal fascicle. There was no difference between approach and the development of a complete versus partial SNP (p = 0.1).
Factors associated with SNP
Patients with an diagnosis other than osteoarthritis were more likely to develop a SNP, the difference was not significant (p = 0.06; OR = 4.9; 95% CI, 1.2–20.8). This included 2 hips with osteonecrosis, 1 hip with post-traumatic arthritis, and 1 THA following a hip arthrodesis in the SNP cohort and 4 patients with osteonecrosis and 1 with Legg-Calvé-Perthes disease in the control group. Intraoperative placement of femoral cables was associated with a higher incidence of SNP (p = 0.04; OR = 8.9; 95% CI, 1.4–58.1). Comorbidities, intraoperative injectable analgesia (p = 0.6), increased blood loss (p = 0.3), haemoglobin drop (p = 0.2), and receiving a blood transfusion (p = 0.4) were not associated with SNP. Leg lengthening compared to preoperative radiographs (p = 0.9) or to the contralateral leg postoperatively (p = 0.4) were not associated with developing a SNP (Table 2).
Factors associated with SNP.
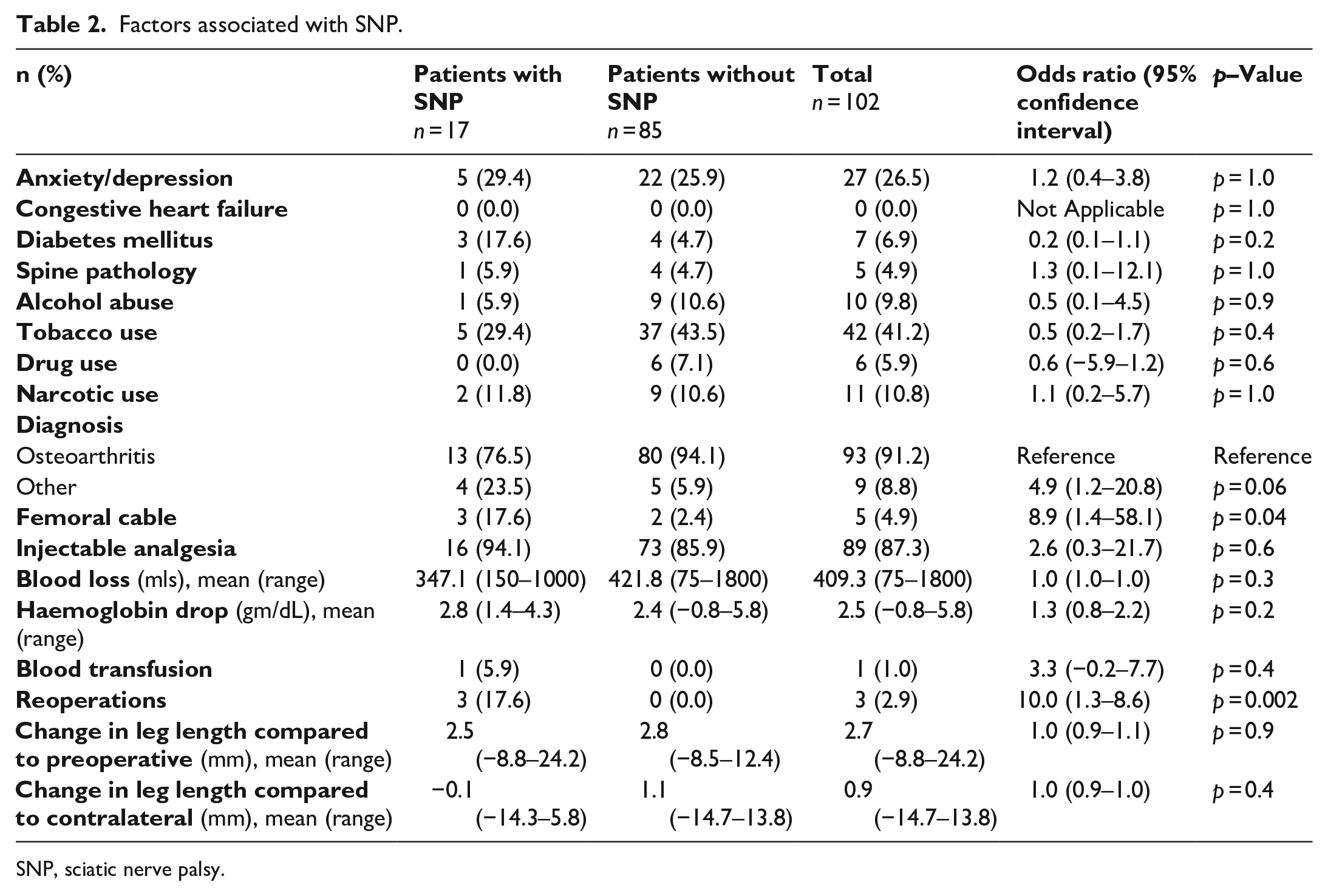
SNP, sciatic nerve palsy.
Management of SNP
SNP was diagnosed in all patients on the first postoperative day. 5 patients (29.4%) had a complete SNP, 12 patients (70.6%) had a partial SNP involving only the peroneal fascicle. All patients had immediate postoperative radiographs per institutional protocol. All radiographs showed evidence of well placed THA.
5 (29.4%) of the 17 SNPs underwent computerised tomography (CT) scan (4 complete and 1 partial), 6 (35.3%) of the 17 SNP underwent a magnetic resonance imaging (MRI) scan (3 complete and 3 partial). Additionally, 11 SNP patients (64.7%) underwent Electromyogram (EMG) test and Nerve Conduction Study (NCS) (3 complete and 8 partial) at a minimum of 27 days after THA.
3 of the 17 SNP patients (17.6%) and none of the control group underwent a reoperation. Indications for reoperation are described in Table 3. No patient had evidence of cable malposition on imaging. All cables were placed intraoperatively due to concern for impending facture in the setting of poor bone quality.
Indications for reoperation.
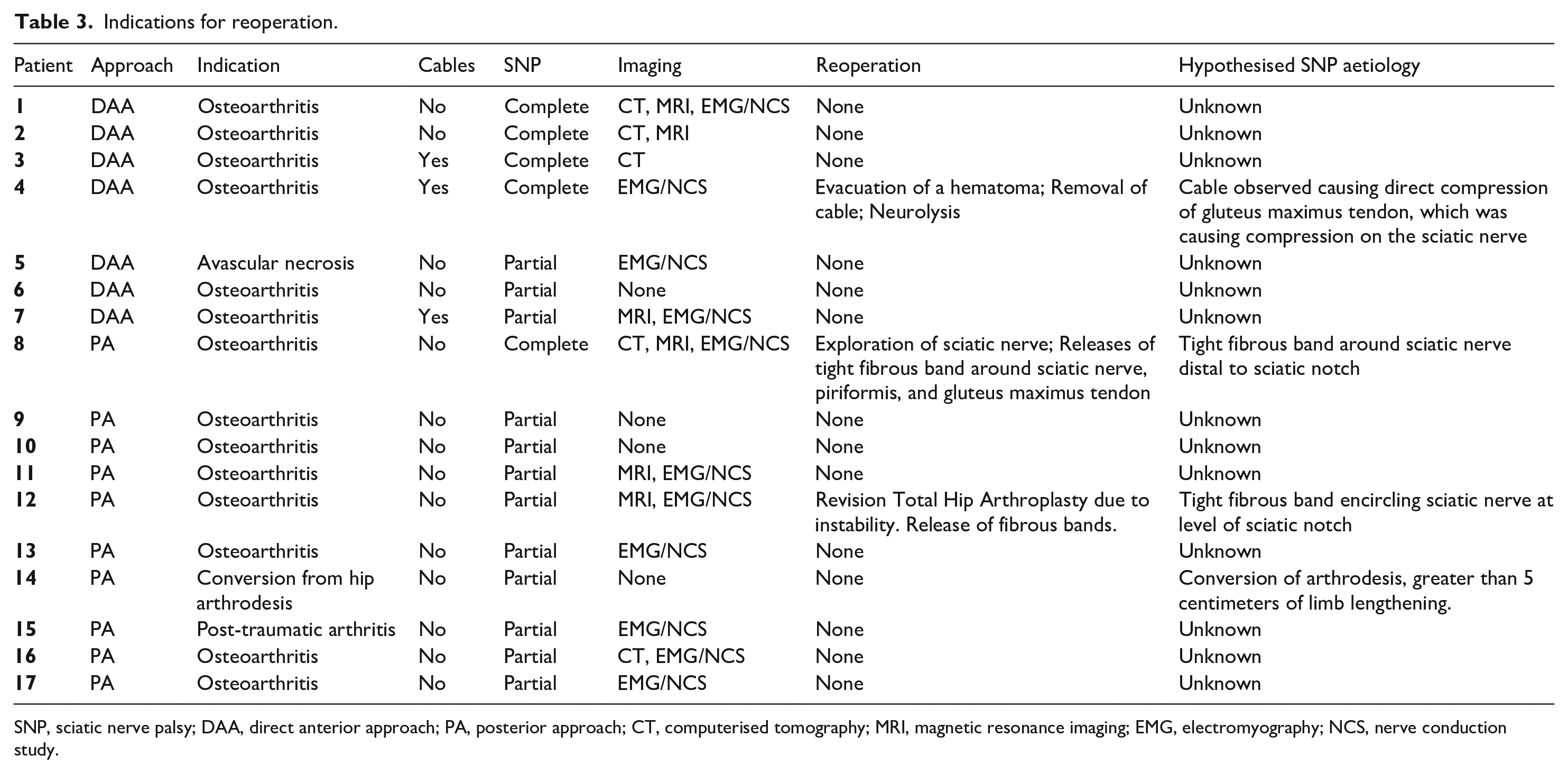
SNP, sciatic nerve palsy; DAA, direct anterior approach; PA, posterior approach; CT, computerised tomography; MRI, magnetic resonance imaging; EMG, electromyography; NCS, nerve conduction study.
Outcome of SNP
Of 9 SNP patients with minimum 12-month follow-up, 4 (44.4%) had a DAA, and 5 (55.6%) a PA. 2 of these 9 patients had a complete SNP, 1 after a DAA and 1 after a PA, and 7 patients had a partial SNP. 4 patients had minimal recovery. Partial recovery was seen in a single patient), near complete recovery was observed in 4 patients and no patient had a complete recovery (Table 4). Overall, mean improvement for the peroneal fascicle was an increase of 2.0/5. The mean improvement for the tibial fascicle was an increase of 1.1/5. Patients who had a complete SNP had more improvement in the tibial fascicle (TF) (mean = 4.5/5) than in the peroneal fascicle (PF) (mean = 3.5/5). Patients with an isolated peroneal fascicle SNP had minimal change in the tibial fascicle (mean = 0.1/5), but some improvement in the peroneal fascicle (mean = 1.6/5).
Outcome of patients with sciatic nerve palsy with minimum 12-month follow-up.
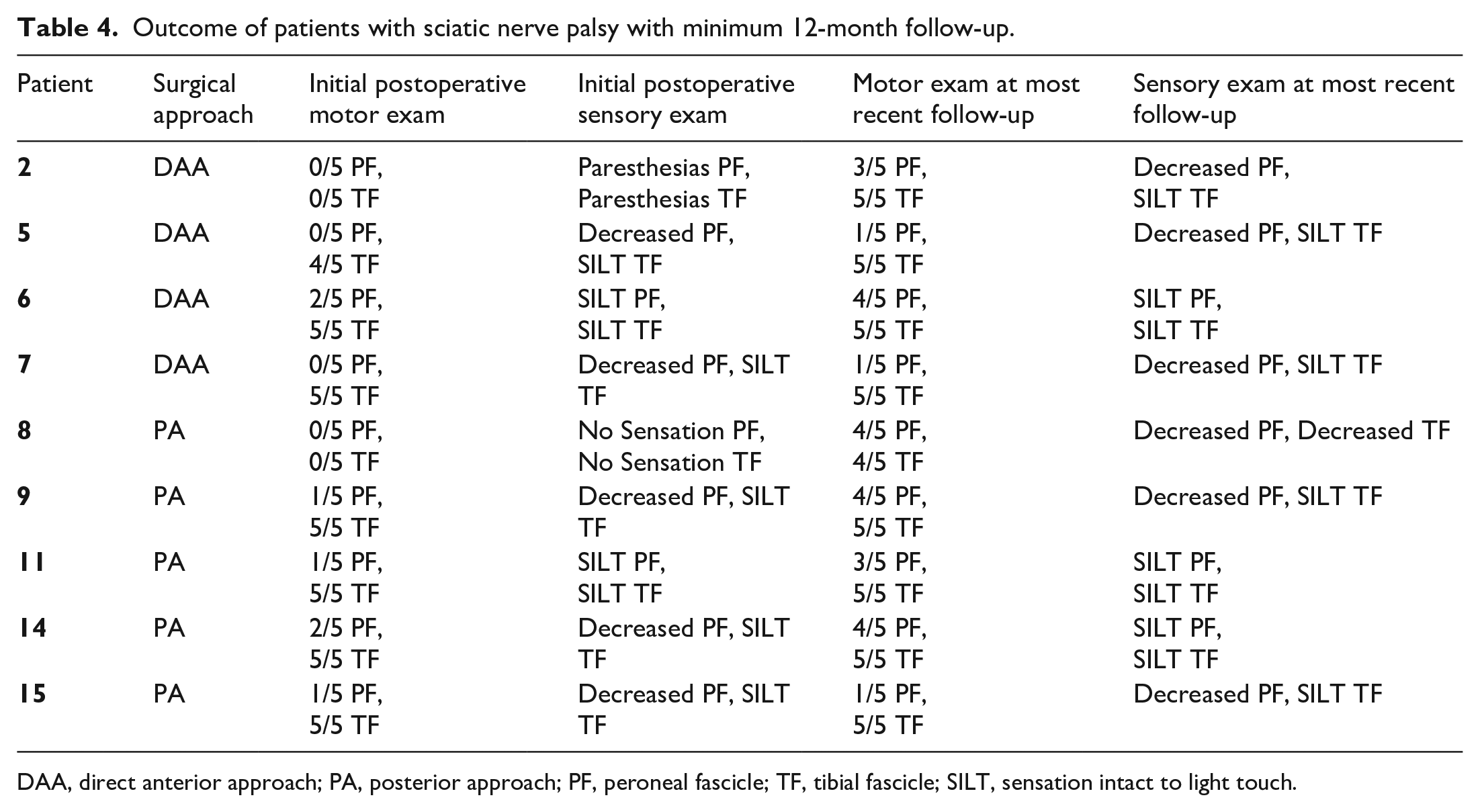
DAA, direct anterior approach; PA, posterior approach; PF, peroneal fascicle; TF, tibial fascicle; SILT, sensation intact to light touch.
The 4 patients with minimum 2.5-year follow-up had similar PF (1.25/5) and TF (3.8/5) motor exams immediately postoperatively as the 5 patients with 1 year follow-up (PF = 0.4/5, p = 0.3, TF = 3.8/5, p = 0.9).
Discussion
SNP remains a rare complication of THA and the incidence seems to be independent to the used approach. Macheras found in a retrospective multicentre study 1 single case of SNP after DAA (0.06%). 10 In a case report coagulopathy and haematoma were suggested as cause for SNP after DAA. 9 The historical infrequency of this complication has limited the ability of retrospective reviews to identify nerve palsies after DAA THA. 3 In this study, not only were multiple instances of SNP after DAA THA reported, but there was no difference in the incidence in the rate of SNP after DAA versus PA THA (p = 0.5). In the current study, consistent with previous data, the most common etiology of SNP after THA is unknown. 4 The explanation for this is likely multifactorial, and likely includes surgical technique, and patient anatomy. Therefore, there is no surgical approach that eliminates the risk of SNP following THA.
The relationship between cable placement SNP is unclear. None of the 3 SNP patients (all DAA) with cables had evidence of cable malposition on imaging. 1 of them was reoperated, the cable was compressing the gluteus maximus tendon, which was indirectly causing compression of the sciatic nerve (Table 3). The DAA might be associated with an increased risk for intraoperative fractures of the femur, that can cause the need for cerclages. 15 The authors recommend that femoral cerclages should be placed cautiously, as there seems to be an increased risk for nerval damage in DAA.
The management of SNP after THA remains controversial. There are many low-quality studies on small populations, which have been previously highlighted in a systematic review, unable to give a recommendation. 16 Some data suggest that early intervention and neurolysis may lead to increased partial nerve function. 17 In the current study, 3 SNP patients had a reoperation with outcomes of no recovery, minimal recovery, and near complete recovery. None of the 17 patients had a complete recovery. This is in contrast to Zappe et al., 18 who reported complete recovery in 5 out of 9 sciatic nerve palsies after THA with a median of 13 months. The ideal algorithm for the treatment of SNP remains unknown and is an opportunity for future study.
This study has several limitations. It is a single-institution study, but due to the high number of patients there might be considerable differences in experience of the surgeons and details of the surgical techniques for the 2 approaches. The study was retrospective and exclusively based on medical records, thus partial nerval damages might have been missed and recovery might not have been documented. This might lead to an underestimation of the incidence of SNP and of recovery. The used diagnosis both pre- and postoperatively are subject to errors in coding and documentation. Finally, the lack of institutional protocols prevents a more complete evaluation of a relatively large group of these patients, with both evaluation and treatment being left to the discretion of the individual surgeons. However, the authors believe that the results are representative of current clinical practice in the US and therefore applicable to SNP patients nationwide.
Conclusion
SNP may occur after THA equally frequent with the DAA and PA. The need or use of femoral cerclages seems to be a risk factor for SNP, no other risk factors were found.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Board or Committee member: AAOS, American Association of Hip and Knee Surgeons, Journal of Orthopaedic Experience & Innovation; IP royalties: Conformis; Research Support: Conformis, DePuy, A Johnson & Johnson Company, 3M; Paid consultant: Conformis, DePuy, A Johnson & Johnson Company; Paid presenter or speaker: Pacira; Stock or stock Options: Conformis, ROMTech.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.