
Abstract
Introduction:
Iliopsoas tendinitis after total hip arthroplasty (THA) has become more prevalent with the increased use of large-diameter femoral heads impinging on native surrounding tissues. Anatomically contoured heads (ACH) are soft-tissue-friendly femoral heads created to minimise this issue. This retrospective study assesses iliopsoas tendinitis prevalence and re-operations in primary THAs with ACH, while determining the minimal clinically important difference (MCID) achievement and improvement with 5 patient-reported outcome measures (PROMs).
Methods:
We conducted a retrospective analysis of 53 ACHs from January 2020 to July 2023. Patients who completed Hip Injury and Osteoarthritis Outcome Score–Physical Function Short Form (HOOS-PS), Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function Short Form 10a (PF SF-10a), PROMIS Global Health (GH)-Mental, or PROMIS GH-Physical, and pain score questionnaires were identified. PROM scores were collected preoperatively and at 3-month and 1-year postoperative intervals. Comparisons using chi-square and ANOVA tests were applied.
Results:
The rates of achieving MCID and improvement within the first year were (69.2 vs. 76.9%) for PROMIS GH-Physical, (38.5 vs. 46.2%) for PROMIS GH-Mental, (71.4 vs. 92.9%) for HOOS-PS, (80.0 vs. 80.0%) for PROMIS PF SF-10a, and (74.0 vs. 91.7%) for pain scores. PROM scores at 3 months and 1 year significantly varied across all categories, except for PROMIS GH-Mental. No patients had iliopsoas tendinitis, dislocations, or re-operations.
Discussion:
ACH implants may alleviate anterior hip pain, while maintaining comparable strength and bio-compatibility to conventional femoral heads. This study underscores the early safety and potential of ACH implants in reducing iliopsoas tendinitis and impingement.
Keywords
Introduction
Iliopsoas tendinitis after total hip arthroplasty (THA) is a under-recognised cause of groin pain, with recent studies reporting an incidence of up to 5.7% in THA.1–3 However, the diagnosis of iliopsoas tendinitis is challenging due to the limited reliability of imaging modalities and the diverse aetiologies of groin pain that remain poorly understood.4,5 Thus, the diagnosis is often based upon patient history, physical examination, and plain radiographs. 6 Notable findings on physical examination include groin pain with resisted hip flexion, particularly during resisted straight-leg raise, and with stretching of the iliopsoas tendon. 7 Iliopsoas tendinitis can be caused by a prominent or retroverted prosthetic acetabular rim, retained cement, enlarged femoral collar, protruding long screws, or soft tissue impingement with a large-diameter femoral head prosthesis.8–13
Studies have shown that the use of large femoral heads have a greater rate of affecting native soft tissues and impinging on the iliopsoas, causing severe groin pain.14–18 In addition, these patients experienced relief when treated with release of the iliopsoas or downsizing of the femoral head.14–16 The iliopsoas is particularly susceptible to impingement due to its proximity to the hip joint, causing concern for surgeons when performing THAs.
To minimise groin pain with large femoral head implants, an innovative soft-tissue friendly anatomically contoured head (ACH) was developed (Figure 1). The inventive structure of the ACH implant incorporates a 2-prong approach. In the proximal hemispherical portion, the large diameter profile of conventional implants is retained to maximise the articular surface. The distal hemisphere portion integrates a contoured smaller radius to reduce strain on the iliopsoas tendon and reduce material exposed to surrounding soft tissue. A previous study showed that such anatomical contouring of the femoral head does not affect dislocation resistance, wear performance, or the femoroacetabular contact area. 19 In addition to the decreased femoral head volume below the equator, the edge of the implant is rounded.
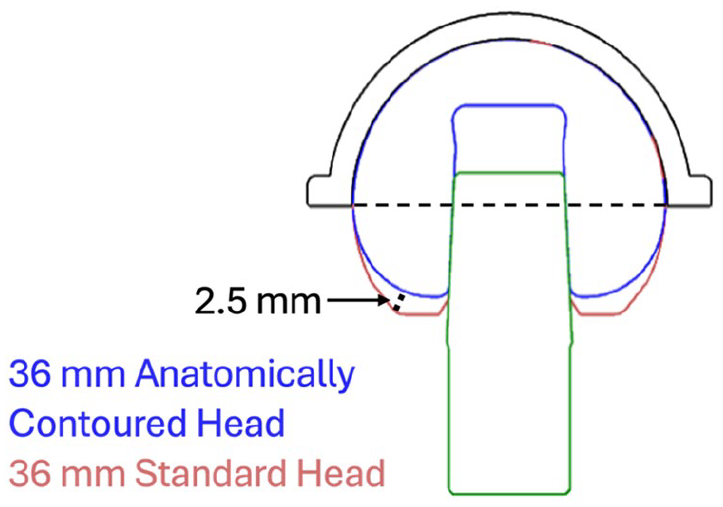
Anatomically contoured femoral head.
Patient-reported outcome measures (PROMs) have been utilised in arthroplasty to incorporate subjective patient assessments of their symptom state in the analysis of outcomes. 20 Various validated PROMs domains such as PROMIS (Patient-Reported Outcomes Measurement Information System) PROMIS Global Health (GH)-Physical, PROMIS GH-Mental, PROMIS Physical Function Short Form 10a (PF SF-10a), pain scores, and Hip Injury and Osteoarthritis Outcome Score–Physical Function Short Form (HOOS-PS) enable the assessment of diverse aspects of patient well-being and the function of the hip joint.21,22 While traditional analysis focused on positive PROM score improvements,23–25 the introduction of the minimal clinically important difference (MCID) addresses discrepancies between objective improvements and patient perceptions.26–28 MCID can be defined as the smallest degree of improvement in PROMs between preoperative and postoperative assessments that patients perceive as beneficial. 28
The present study aimed to evaluate the clinical effectiveness of anatomically contoured heads in primary THA. Our study sought to answer the following questions: (1) What is the prevalence of iliopsoas tendinitis and re-operation in ACH patients? (2) What is the rate of achieving MCID at 3 months and 1 year?
Methods
This retrospective study was conducted with Institutional Review Board approval using data from single institutional database. The database was queried for all BIOLOX CONTOURA Femoral Head (Total Joint Orthopedics, Salt Lake City, Utah, USA) from January 2020 to July 2023. The PROMIS GH-Physical, PROMIS GH-Mental, HOOS-PS, PROMIS PF SF-10a, and pain scores were collected pre-operatively and at 3-month and 1-year postoperative intervals. Only patients with paired PROM assessments (preoperatively and postoperatively) were included in the analysis. In order to maximise the number of patients for analysis and to account for inherent variations in the timing of patient follow-up visits, preoperative scores were defined as those captured within 6 months prior to the index procedure, 3-month postoperative period as those collected between 1.5 and 4.5 months from the index surgery and the 1-year postoperative period as those collected between 0.5 and 1.5 years from the index surgery.
Using this criteria, 53 hips and 44 unique patients were included in the study. Each hip was performed by a fellowship trained arthroplasty surgeon with manual instrumentation. A total of 3 different surgeons performed the surgeries and implanted the ACHs. All surgeries were performed via standard posterior incision, followed by femoral neck osteotomy, acetabular reaming, femoral canal preparation, and component implantation. In our cohort, there were 9 patients during the study period who completed either preoperative PROM questionnaires or postoperative PROM questionnaires, but did not complete the counterpart; thus, we could not include these patients in our analysis. 9 patients received the ACH implant bilaterally, hence, patients were not excluded for a history of THA.
Of that cohort, 35 patients had pairing preoperative and postoperative PROM scores to be included in the analysis. Demographic variables collected for each patient included: age at index surgery, sex, and body mass index (BMI). Each patient was chart reviewed manually for any revision procedures, episodes of iliopsoas tendinitis, injections for iliopsoas tendinitis, and any reason for re-operation. Furthermore, any episodes of anterior groin pain that were recorded were further investigated with radiographic x-rays to exclude any other causes such as acetabular retroversion, hip dysplasia, or bony abnormalities. Lastly, femoral head sizes were identified for each patient. Of the 53 patients, 43 (81%) received 36-mm femoral heads and 10 (19%) received 32-mm femoral heads.
MCID cut-off scores for this cohort were gathered from previous published studies which had utilised the anchor-method. A literature analysis was carried out to review the published literature and gather the reference basis for MCID. 29 The MCID values used in the study were from previous THA articles with over 1000+ patients. The values used were 4.02 for PROMIS GH-Physical, 4.46 for PROMIS GH-Mental, 9.3 for HOOS-PS, and 4.1 for PROMIS PF SF-10a.30,31 Due to the lack of published literature, the pain score value was calculated at 3 months and 1 year using the MCID distribution-method within our own cohort of patients.
Statistical analysis
For categorical variables, a chi-square test of independence was used. For continuous variables, a student’s t-test and ANOVA test were used as appropriate. For each patient, the change from preoperative to postoperative PROM assessments at each time-point was calculated and used to determine whether that patient achieved MCID. The 3 primary outcomes of interest were rate of achieving MCID PROMIS GH-Physical, PROMIS GH-Mental, PROMIS PF SF-10a, HOOS-PS, and pain scores at each time-point. Statistical significance was defined as p < 0.05. R Studio (version 4.3.1, Vienna, Austria) was used to perform the statistical analyses.
Results
The mean age and BMI across the entire patient cohort was 67.7 ± 9.53 years and 28.6 ± 4.22 kg/m2. Of the cohort, 30 of the 44 (68.2%) patients were male (Table 1). The rate of achieving MCID and rate with improvement are reported in (Tables 2 and 3), stratified by the 5 collected PROMs. The MCID rates are stratified by 3 months and 1 year. Thorough chart reviewed showed that zero patients had any revision surgery or returned to the operating room (OR). In addition, zero patients had any incidence of iliopsoas tendinitis or dislocations. Average follow-up for the entire cohort was 2.2 ± 0.61 years.
Patient demographics.
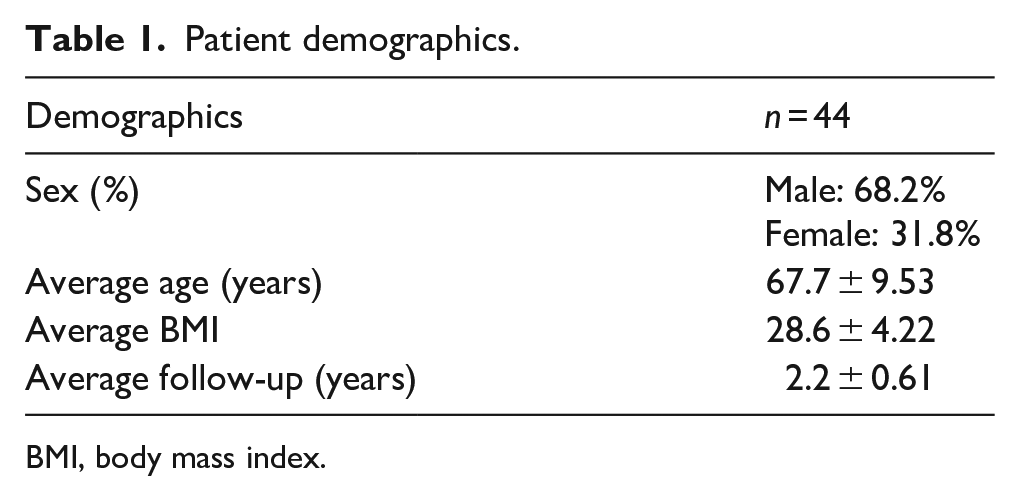
BMI, body mass index.
Summary of PROMs data with minimally clinical important difference (MCID).
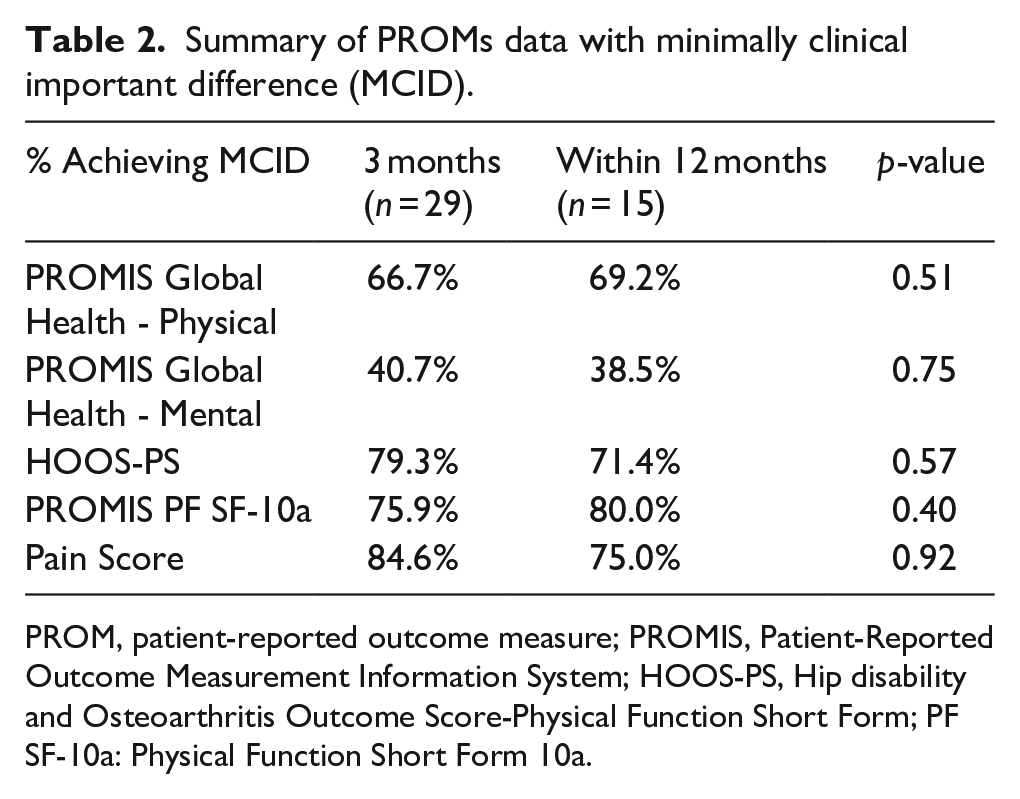
PROM, patient-reported outcome measure; PROMIS, Patient-Reported Outcome Measurement Information System; HOOS-PS, Hip disability and Osteoarthritis Outcome Score-Physical Function Short Form; PF SF-10a: Physical Function Short Form 10a.
Summary of PROMs data with improvement.
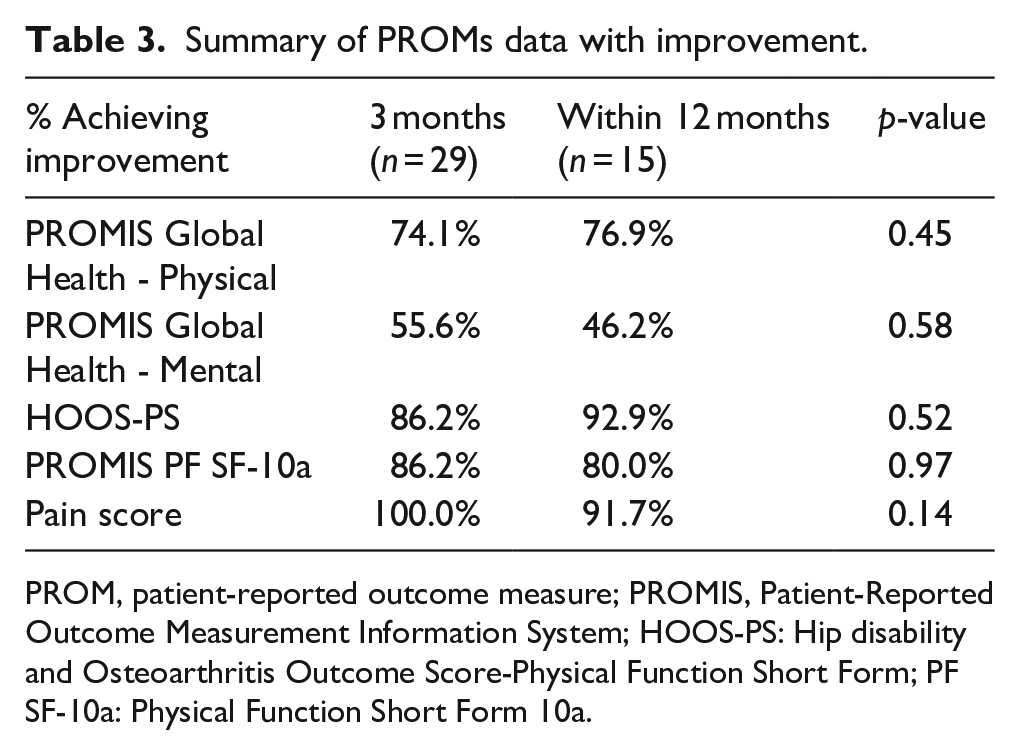
PROM, patient-reported outcome measure; PROMIS, Patient-Reported Outcome Measurement Information System; HOOS-PS: Hip disability and Osteoarthritis Outcome Score-Physical Function Short Form; PF SF-10a: Physical Function Short Form 10a.
Comparing the data for rate of MCID and improvement, majority of the PROMs showed a decrease in the rate from 3 months to 1 year postoperative. For MCID, only PROMIS GH-Physical and PROMIS PF SF-10a showed improvement, whereas all other PROMs displayed a decrease in the rate achieving MCID (Table 2). For rate of improvement, all PROMs showed a decrease in rate between 3 months and 1 year postoperative time points (Table 3). Chi-square analysis between 3 months and 1 year postoperative time points for rate of MCID and improvement showed no significant difference (p > 0.05) (Tables 2 and 3). 13 of the 15 patients in the one-year post-operative cohort also had 3-month PROM data points. The rate of achieving of MCID and improvement within the first year were (69.2 vs. 76.9%) for PROMIS GH-Physical, (38.5 vs. 46.2%) for PROMIS GH-Mental, (71.4 vs. 92.9%) for HOOS-PS, (80.0 vs. 80.0%) for PROMIS PF SF-10a, and (74.0 vs. 91.7%) for pain scores (Tables 2 and 3).
ANOVA analysis of all PROM groups at 3 months and 1 year were statistically significant (p < 0.05), except for PROMIS GH-Mental (Table 4). When further comparing preoperative versus 3-month PROMs and preoperative versus 1-year PROMs, all PROMs were statistically significant (p < 0.05) except PROMIS GH-Mental. T-test analysis between 3-month and 1-year PROMs showed no statistically significant difference between the 2 postoperative time points (p > 0.05) (Figures 2 and 3).
PROMs ANOVA analysis.
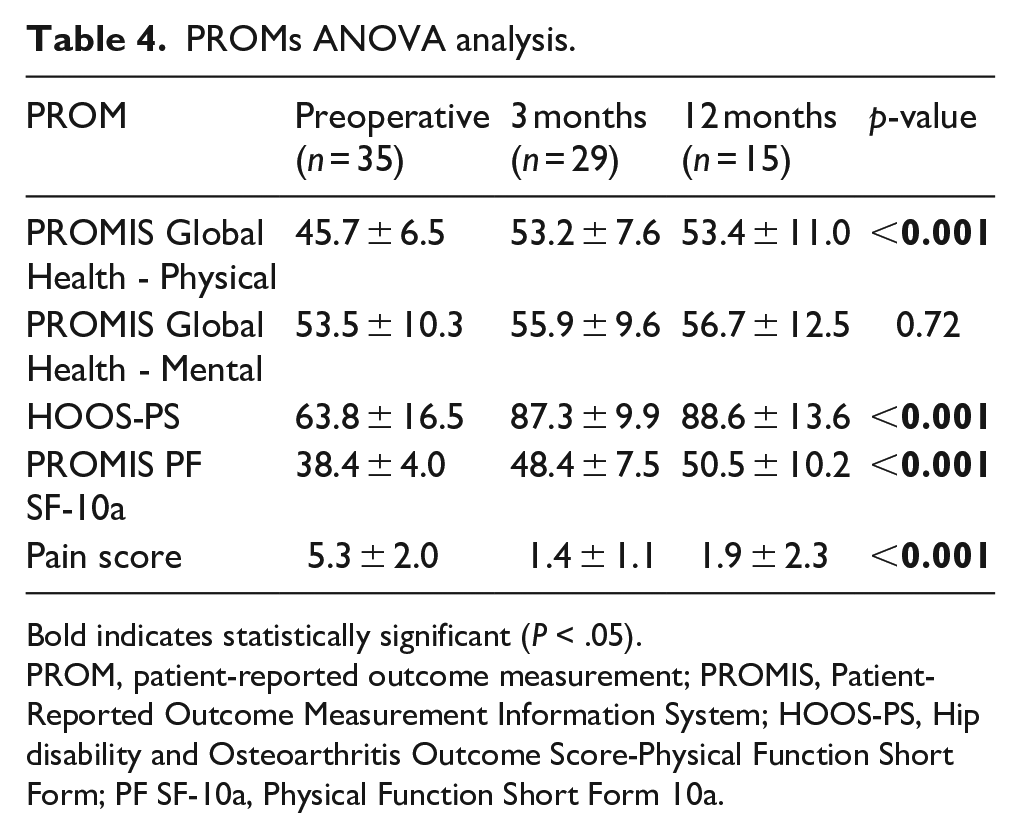
Bold indicates statistically significant (P < .05).
PROM, patient-reported outcome measurement; PROMIS, Patient-Reported Outcome Measurement Information System; HOOS-PS, Hip disability and Osteoarthritis Outcome Score-Physical Function Short Form; PF SF-10a, Physical Function Short Form 10a.
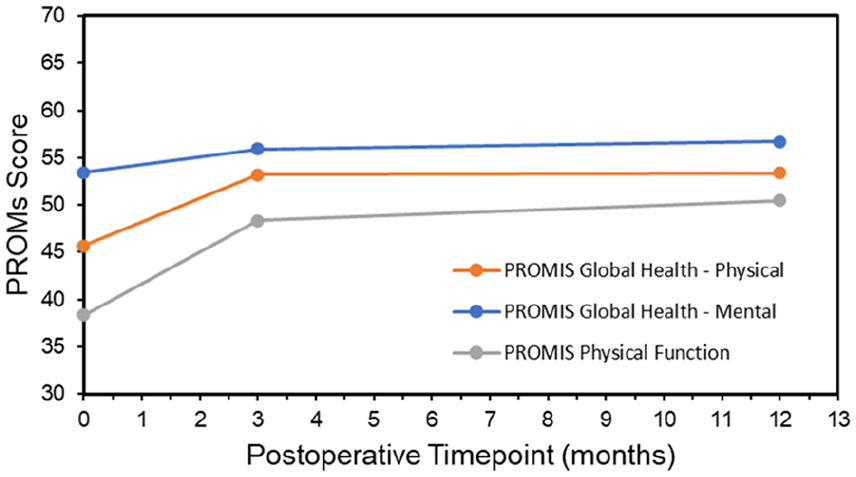
PROMIS Comparison.
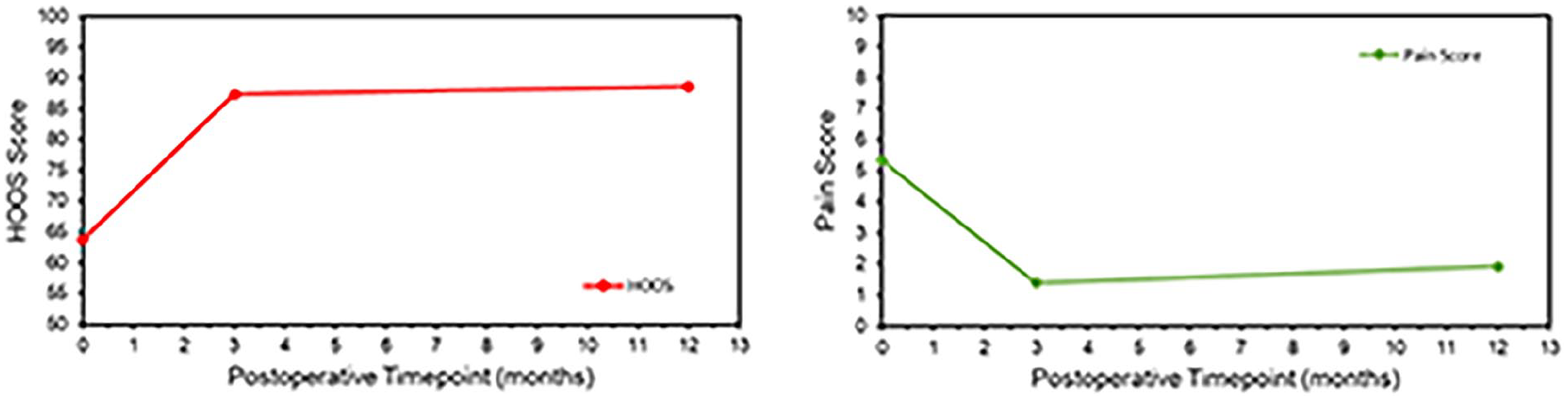
HOOS-PS and pain score.
Discussion
Groin pain after THA is a relatively common occurrence but determining the cause can be difficult. Iliopsoas tendinitis after hip arthroplasty is relatively uncommon but can be disabling. Treatment options for iliopsoas tendinitis after THA such as physical therapy, injection, and arthroscopy are not always effective. As the use of larger diameter femoral heads in THA has increased to mitigate risk of hip dislocation, so has the risk of anterior groin pain due to iliopsoas impingement.14,16 This paper describes the early safety of anatomically contoured femoral head design and its ability to potentially decrease iliopsoas tendinitis and impingement. The present study found that majority of patients with ACH achieved both MCID and improvement at the 3-month and 1-year postoperative mark and no patients reported any groin pain or iliopsoas tendinitis. Using MCID methodology, this study found that the rate of achievement of MCID within the first year for ACH implants was 69.2% for PROMIS GH-Physical, 38.5% for PROMIS GH-Mental, 80.0% for PROMIS PF SF-10a, 74.0% for pain scores, and 71.4% for HOOS-PS. In a systematic review of 15 studies involving 11,140 patients by Czerwonka et al. 32 similar rates of achieving MCID were reported: 59.1% for PROMIS GH-Physical, 26.0% for PROMIS GH-Mental, 52.7% for PROMIS PF SF-10a, and 67.2% for pain interference. Additionally, the proportion of patients achieving MCID for HOOS reported by Lyman et al. 21 aligns closely with our findings, ranging from 67% to 96%. Notably, the similar scores between 3-month and 1-year PROMs raises concerns about the predictive value of early postoperative PROMs for long-term outcomes. In the line with these findings, Canfield et al. 33 noted a plateau in PROMs after the 6-month mark, suggesting that assessments within that time-frame may offer insights into future outcomes.
The main limitation of this study is that there is no control or matched cohort. We would like to explicitly state that author AF played a role in the design process of the ACH implant. Due to the rarity of iliopsoas tendinitis in this THA, matching our cohort with a control THA group would not have any benefit to the power of the study. All patients included in the study were from 1 hospital, in our analysis, which may limit the generalisability of our findings around hospital setting. In this study, we utilised both the MCID anchor and distribution methods to define our MCID cut-off values. Although both distribution-based and anchor-based methods have their benefits and drawbacks, anchor-based methods are generally considered slightly more robust as they incorporate patient responses from an external questionnaire to which PROM scores are correlated. 34 Due to the lack of literature with pain score PROMs, the distribution method was utilised. In addition, the literature analysis used for the anchor method relies on the secondary literature, which may not be the most representative for our cohort. However, we attempted to mitigate this by verifying values chosen were like previously described calculations.35,36
Another limitation is the relatively small sample size for patients with ACH femoral heads in their THA. Thus, statistical analyses were not adequately powered for PROMs. In addition, the results of percent of patients achieving the MCID may lack the power to detect meaningful differences. Considering the small cohort, a PROMs table was conducted calculating the rate of PROMs that showed improvement. Although MCID has been shown to be more clinically relevant, evaluation with improvement in PROM scores has also been cited as a positive outcome in the literature.23–25 In addition, the period of follow up is another limitation. For several patients, 3-month and 1-year postoperative PROM data were not available. Thus, longer follow-up is needed to truly assess the postoperative outcomes and prevalence of iliopsoas tendinitis and re-operation in these patients compared to those with conventional femoral heads in their THA.
Lastly, 1 assumption we addressed was attributing groin pain to iliopsoas tendinitis. We attempted to narrow down the wide array of complex aetiologies of groin pain by comprehensive exclusion of other potential causes such as acetabular retroversion, hip dysplasia, or bony abnormalities through radiologic imaging. While our study focused on assessing the prevalence of iliopsoas tendinitis and groin pain relief with ACH, we recognise the need for further investigation into the multi-factorial nature of groin pain post-hip replacement and have explicitly included these limitations. Future studies with more rigorous diagnostic criteria and emphasis on imaging modalities can help determine the true clinical effectiveness of ACH implants by differentiating between the various etiologies of groin pain.
Despite these limitations, we believe our research offers valuable insights into the potential benefits of ACH implants in mitigating soft tissue irritation and warrants further exploration in larger samples or registry-studies.
Conclusion
In conclusion, this study showed iliopsoas impingement may be mitigated by contouring the distal profile of the femoral head below the equator as in the ACH implant. Moreover, ACH implants may decrease the risk of anterior hip pain resulting from soft-tissue impingement with large heads while maintaining similar dislocation strength, burst strength, wear rate, and bio-compatibility. The present study offers patient-level insights into the safety of contoured head implants, and future multicentre or registry studies with longer follow-up would allow us to determine the true clinical effectiveness of these implants in preventing groin pain and iliopsoas tendinitis.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AAF: receives stock or stock options from Amplicore, Inc and Orthopaedic Technology Group; is a paid consultant for Canary Medical, Total Joint Orthopedics, and Zimmer Biomet.
HSB: receives royalties from: Exactech, Smith & Nephew, Wolters Kluwer; has stock options in Exactech; is a paid consultant for Exactech and Smith & Nephew; receives research support from Zimmer Biomet.
CML: is a speaker and paid consultant for Smith & Nephew; receives research support from Zimmer Biomet.
All other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.