
Abstract
Introduction:
The progressive nature of multiple sclerosis (MS) may adversely affect outcomes following total hip arthroplasty (THA). As patient-reported outcome measures (PROMs) in this specific group are not well defined, this study aimed to compare the clinical outcomes and the rates of achieving the minimal clinically important difference for improvement (MCID-I) and worsening (MCID-W) between patients with MS and those without MS undergoing THA.
Methods:
We conducted a retrospective analysis of 375 THAs, including 75 MS patients and 300 propensity-matched non-MS patients (4:1), performed between 2016 and 2022. Collected PROMs included Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health Mental and Physical, PROMIS Physical Function short form 10-a (PF-10a), and Hip disability and Osteoarthritis Outcome Score-Physical Function Short-form (HOOS-PS). Preoperative and postoperative PROMs and MCID-I/MCID-W rates were compared.
Results:
A total of 375 THAs, including 75 MS and 300 matched non-MS patients, were analysed. MS patients had higher 90-day postoperative complication rates (9.3% vs. 2.3%, p = 0.012) and infection rates (4.0% vs. 0.3%, p = 0.006). The rates of achieving MCID-I and MCID-W were similar for PROMIS Global Mental, PROMIS Global Physical, and HOOS-PS, but MS patients had a higher rate of experiencing MCID-W for PROMIS PF-10a compared to non-MS patients (16.7% vs. 6.5%, p = 0.022). Additionally, MS patients had a longer mean hospital stay (2.4 vs. 1.9 days, p = 0.005) and lower rates of being discharged home (82.7% vs. 94.3%, p < 0.001).
Conclusions:
The present study found that MS patients experience similar rates of MCID-I and MCID-W in most PROMs but have a higher rate of MCID-W for PROMIS PF-10a and increased postoperative complications. These findings highlight the need for careful consideration of postoperative risks despite potential improvements. Further research is needed to explore the impact of MS progression on PROMs and perioperative outcomes.
Introduction
Total hip arthroplasty (THA) is known to enhance comfort and functionality in individuals with hip osteoarthritis (OA). 1 However, outcomes following THA can vary significantly based on patient comorbidities. 2 A comorbidity that warrants further investigation for its impact on THA outcomes is multiple sclerosis (MS). 3 MS is a chronic neurological disorder characterised by autoimmune demyelination of the central nervous system, 4 leading to various neurological symptoms such as paresthesia, diplopia, dysphagia, and urinary and bowel dysfunctions.4,5
Particularly relevant to orthopaedic practitioners, MS patients may also exhibit muscle spasms, weakness, contractures, paresis, unstable gaits, and reduced mobility, which could influence post-THA recovery and function. 6 Additionally, MS patients are at higher risk of falls and fractures, with a prevalence of arthritic conditions ranging from 16% to 26%.7,8 With advancements in MS treatments, more MS patients are ageing into the demographic associated with advanced OA and potential THA indications. 9 While existing literature has explored how MS might predispose to certain conditions or affect outcomes across various orthopaedic specialties,10–12 its specific impact on THA outcomes remains underexplored.
The existing research literature on MS and THA is largely limited to objective outcomes like complication rates or hospital stay.3,13 Few studies have explored the impact of MS on patient-reported outcome measures (PROMs) in THA.14,15 PROMs offer a patient-centred evaluation of surgical success and can be further interpreted using the minimal clinically important difference for improvement (MCID-I) and worsening (MCID-W).16,17 MCID-I represents the meaningful improvement from preoperative to postoperative PROM scores, while MCID-W signifies the significant worsening.
Given the limitations of the current literature, orthopaedic clinicians can benefit from a study that thoroughly investigates how MS may impact both complication rates and PROMs following THA. Therefore, the aims of this study are to: (1) investigate the postoperative complication rates in MS patients undergoing THA compared to a matched control cohort; and (2) evaluate the rate of achieving MCID-I or MCID-W between these 2 cohorts. By investigating both subjective and objective outcomes in conjunction, while also utilising newer PROM methodology such as MCID-I and MCID-W, our study aims to provide a more well-rounded view of the experiences and outcomes of MS patients following THA.
Methods
Patients who underwent THA between 2016 and 2022 were initially identified from a multi-institutional arthroplasty registry using Current Procedural Terminology (CPT) code 27130 following approval from the institutional review board. Inclusion criteria comprised individuals aged 18 years or older whose index arthroplasty was performed within our hospital network. An electronic chart query was conducted using the International Classification of Diseases, Tenth Revision (ICD-10) code for multiple sclerosis (G35), and each patient’s diagnosis of MS was manually confirmed through chart review.
Demographic variables obtained from the arthroplasty registry included age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), length of stay (LOS), and discharge disposition, categorised as home discharge, skilled nursing facilities (SNF), or inpatient rehabilitation facilities (IRF). Additionally, any MS medication or medication taken for MS-related symptoms was systematically recorded. Perioperative outcomes such as 90-day emergency department visits, 90-day readmissions, postoperative complications, reoperations, and revision surgeries were documented.
Eligibility criteria
The eligibility criteria for the study included: (1) THA performed at 1 of the affiliated institutions; (2) completion of at least 1 preoperative and 1-year postoperative Patient-Reported Outcomes Measurement Information System (PROMIS) survey; and (3) complete information on postoperative complications. The validated PROMs used were PROMIS Global Health Physical, PROMIS Global Health Mental, PROMIS Physical Function Short Form 10a, and Hip disability and Osteoarthritis Outcome Score-Physical Function Short Form (HOOS-PS).18–21
The preoperative period ranged from 0 to 6 months prior to the index surgery, while the 1-year postoperative period extended from 6 months to 2.5 years after the index surgery. This timeframe was selected based on previous research indicating no significant improvements in physical function beyond the 6-month mark and has been widely used in THA research.22–26 For patients who completed multiple preoperative surveys, the score collected closest to the surgery date was selected. Similarly, for postoperative scores, the score closest to the one-year mark was utilised.
Study population
After applying inclusion and exclusion criteria, 75 THAs in 63 unique MS patients were identified. To generate a population of non-MS patients with similar baseline characteristics to minimise confounding, a propensity score match was then conducted using a 4 to 1 nearest neighbour matching without replacement and a caliper fixed at 0.3. The propensity scores were calculated using a logit model that included the following variables: age; sex; BMI; and CCI. The match resulted in a non-MS group of 300 THAs in 297 unique patients.
In our overall cohort of 375 THAs, the average age was 61.1 ± 11.3 years, with the majority being women (69.9%). The mean BMI was 28.1 ± 5.9 kg/m², and the average CCI score was 0.7 ± 1.3 (Table 1).
Demographics of MS patients and 4:1 matched non-MS patients.

BMI, body mass index; CCI, Charlson comorbidity index; IRF, inpatient rehab facility; MS, multiple sclerosis; SNF, skilled nursing facility; THA, total hip arthroplasty.
Matched variables.
Bold values indicate statistical significance (p < 0.05).
Data analysis
Demographic, clinical, and PROMs variables were analysed using descriptive statistics. Differences between groups were assessed using Student’s t-test for continuous variables and the Chi-square test for categorical variables.
To determine if any statistically significant differences in continuous PROM scores were also clinically significant, MCID-I and MCID-W thresholds were also used. 16 The threshold values from Salimy et al. 25 were utilised as the values for achieving MCID-I and MCID-W in this study (Table 2). Preoperative and postoperative PROMs were extracted from the arthroplasty registry and used to calculate the delta scores for each patient. Each patient’s delta PROM score was categorised into 1 of 3 groups: (1) MCID-I, indicating a delta PROM score higher than the MCID-I threshold; (2) MCID-W, indicating a delta PROM score lower than the MCID-W threshold; and (3) no significant change, indicating a delta PROM score between the MCID-I and MCID-W thresholds. Due to some patients completing preoperative, but not postoperative PROMs, or vice versa, MCID-I and MCID-W values were able to be calculated for 42 of the 75 MS patients (58.7%) and 293 of the 300 non-MS patients (97.6%).
Thresholds for minimal clinically important difference for improvement (MCID-I) and worsening (MCID-W) used in this study.

PROMIS, patient-reported outcomes measurement information system; PF10a, physical function short form 10a; HOOS-PS, Hip disability and Osteoarthritis Outcome Score-physical function short form.
All thresholds derived from Salimy et al. 25
A power analysis revealed that with the present patient numbers, an alpha of 0.05, and a power of 80%, a difference of 4.6 in PROMIS scores, 6.9 in HOOS-PS scores and 23.2% in MCID attainment would be detectable between MS and non-MS patients.
Statistical significance was set at p < 0.05. R Studio (version 4.3.1, Vienna, Austria) was used to perform the statistical analyses.
Results
A total of 375 THAs including 75 MS THAs and 300 matched non-MS THAs were analysed (Table 1). In patients with MS undergoing THA, we observed a longer hospital stay (2.4 vs. 1.9 days, p = 0.005) and higher rates of discharge to skilled nursing facilities (SNFs) (10.7 vs. 4.0%, p = 0.022) and inpatient rehabilitation facilities (IRFs) (6.7 vs. 1.0%, p = 0.002). Among these patients, 35 (46.7%) were taking medications for MS symptoms, with 16 on biologic disease-modifying antirheumatic drugs (DMARDs) and the remaining 19 on conventional DMARDs or medications for peripheral MS symptoms. The full list of medications taken by the MS THA cohort are in Table 3.
Medications for MS.

Generic drug (brand drug).
Comparing perioperative outcomes, MS THA patients had a higher 90-day postoperative complication rate than non-MS THA patients (9.3 vs. 2.3%, p = 0.012) (Table 4). Specifically, MS THAs showed higher rates of periprosthetic joint infection (4.0 vs. 0.3%, p = 0.006), wound dehiscence (1.3 vs. 0.0%, p = 0.006), leg swelling (1.3 vs. 0.0%, p = 0.006), fever (1.3 vs. 0.0%, p = 0.006) (Table 5). Furthermore, MS THAs had a higher rate for reoperation for periprosthetic joint infection (4.0 vs. 0.6%, p = 0.024), and reoperation for wound dehiscence (1.3 vs. 0.0%, p = 0.045).
Clinical outcomes of MS patients and 4:1 matched non-MS patients.

ED, Emergency Department; MS, multiple sclerosis; THA, total hip arthroplasty.
Bold values indicate statistical significance (p < 0.05).
Postoperative complications and reoperation indications.

DVT, deep vein thrombosis; MS, multiple sclerosis; PE, pulmonary embolism; THA, total hip arthroplasty; UTI, urinary tract infection.
Of the 5 reoperated for infection, all patients received debridement, antibiotics, and implant retention (DAIR) with liner exchange.
Bold values indicate statistical significance (p < 0.05).
When comparing the PROM scores between the 2 cohorts, we observed significant differences in baseline and postoperative scores (Table 6). MS patients had lower preoperative scores for PROMIS Global Mental (45.8 vs. 49.9, p = 0.013), PROMIS Global Physical (37.0 vs. 40.4, p = 0.007), and PROMIS PF-10a (33.4 vs. 35.8, p = 0.01, p = .007). MS patients also had lower 1-year postoperative PROM scores for PROMIS Global Physical (44.1 vs. 48.9, p = 0.003), PROMIS PF-10a (41.2 vs. 45.9, p = 0.006), and HOOS-PS (76.7 vs. 83.5, p = 0.027). However, the delta scores for all four PROMs were similar between the 2 groups.
MCID-I and MCID-W subgroup analysis by MS THA and 4:1 matched non-MS THA patients.
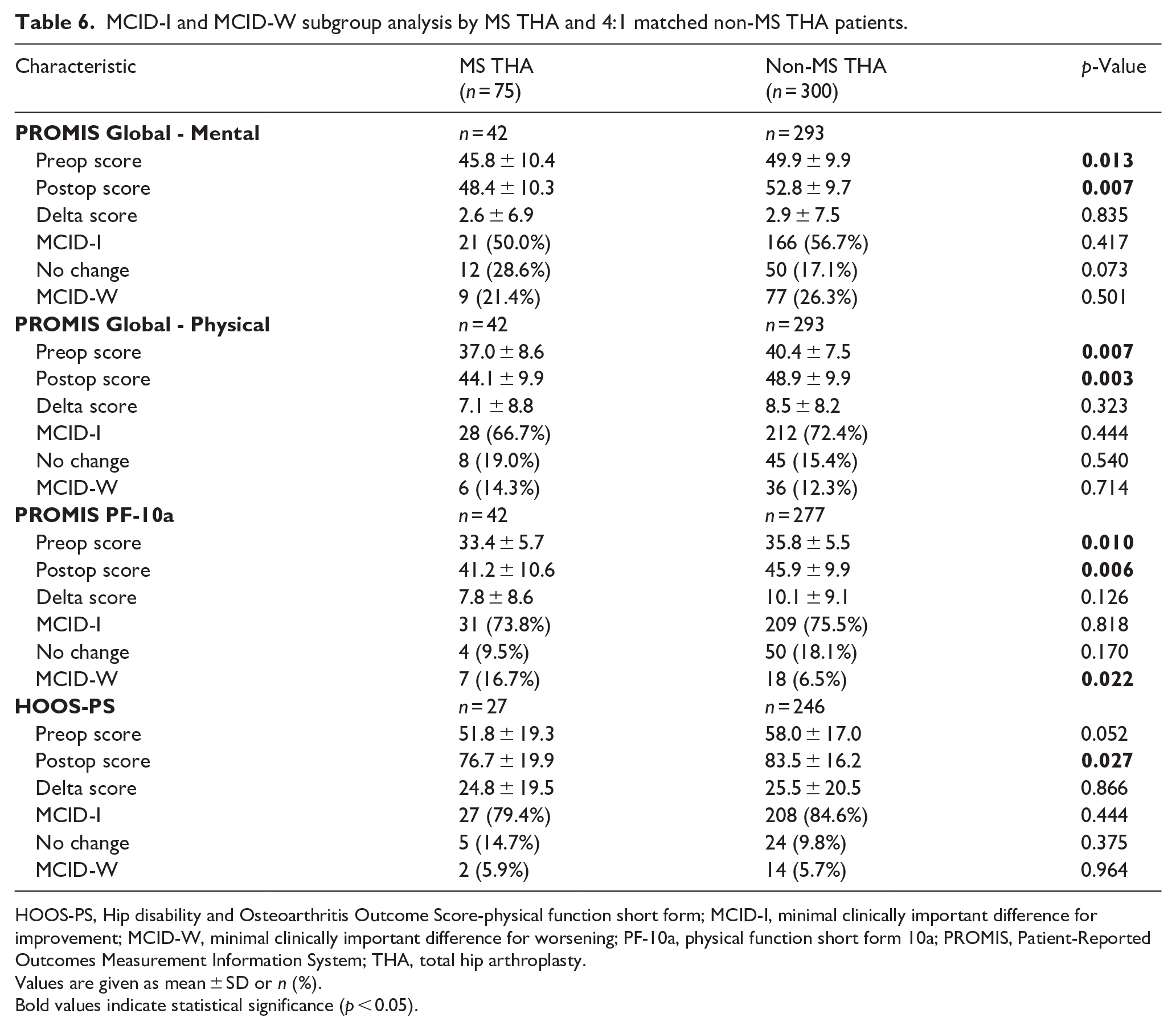
HOOS-PS, Hip disability and Osteoarthritis Outcome Score-physical function short form; MCID-I, minimal clinically important difference for improvement; MCID-W, minimal clinically important difference for worsening; PF-10a, physical function short form 10a; PROMIS, Patient-Reported Outcomes Measurement Information System; THA, total hip arthroplasty.
Values are given as mean ± SD or n (%).
Bold values indicate statistical significance (p < 0.05).
The rate of achieving MCID-I and MCID-W was similar for PROMIS Global Mental, PROMIS Global Physical, and HOOS-PS. Interestingly, MS patients had a higher rate of experiencing MCID-W for PROMIS PF-10a compared to non-MS patients (16.7% vs. 6.5%, p = 0.022), with a similar rate of achieving MCID-I. Sub analysis based on medication use showed similar PROM scores and rates of achieving MCID-I and MCID-W between patients on medications and those not on medications. Further analysis of MS patients based on biologic DMARDs versus non-biologic DMARDs showed no significant differences in PROM scores or rates of achieving MCID-I and MCID-W.
Discussion
Advancements in MS treatments have extended patient lifespans, overlapping with ages prone to advanced hip OA. 9 Hip arthroplasty in MS patients has demonstrated positive outcomes such as pain reduction and improved functional gait. 15 Nevertheless, recent studies have raised concerns about the efficacy of hip arthroplasty in MS patients, highlighting an increased risk of both surgical and medical complications.9,13,27 Notably, there is a paucity of research investigating patient-centred perspectives on how MS affects PROMs in THAs,14,15,28 with no studies comparing MCID-I and MCID-W outcomes. To the best of our knowledge, this study presents the largest series of MS THA cases from a regional health care system to date, encompassing a cohort of 75 THAs. The present study found MS patients have similar rates of achieving MCID-I and MCID-W for PROMIS Global Physical, PROMIS Global Mental, and HOOS-PS. However, MS patients showed a higher MCID-W rate for PROMIS PF-10a. Notably, they also faced higher postoperative complication rates compared to non-MS patients.
A thorough investigation into clinical outcomes and revision rates following MS THAs is essential. National database studies have consistently shown an elevated risk of surgical and medical complications in MS THA patients, with up to 1.22 times higher rates reported.9,13,27 Additionally, Quinlan et al. 13 reported a notable increase in 30-day hospital readmission rates, 30-day Emergency Department visits, infections, dislocations, and revisions among MS patients, with rates ranging from 1.35 to 2.05 times higher. Our study supports these findings, observing higher rates of 90-day postoperative complications in MS THA patients, particularly with periprosthetic joint infection. The revision rate for MS THA patients has been documented in the literature to range from 4.23% to 7.3%, with periprosthetic joint infection rates surpassing 4.9%.13–15,28 Similarly, in our cohort of 75 MS patients, 3 (4.0%) required revision surgery due to periprosthetic joint infection. While other perioperative outcomes did not show significant differences, the trend towards higher rates in MS THA patients suggests potential challenges in their recovery and postoperative function. 15
In line with previous research, our study confirms that MS patients are more likely to be discharged to post-acute facilities and require a longer LOS compared to non-MS patients. Newman et al. 27 reported a 2.09 times higher likelihood of MS patients being discharged to care facilities based on a large sample of 5899 MS THAs. This discrepancy is attributed to the higher baseline disability and the intricate care associated with managing MS symptoms and complications. Furthermore, our findings are supported by decreased baseline scores in three out of four PROMs, indicating the functional challenges faced by MS patients. Additionally, Newman et al. 27 noted that MS patients had a mean LOS 8.24% longer than their non-MS counterparts and were less frequently discharged on postoperative days 2 and 3 but more often on day 4. These trends underscore the extended recovery period of MS THA patients, highlighting the importance of tailored rehabilitation strategies and postoperative support. 29
Comparing preoperative baseline PROMs, MS THA patients exhibited lower scores in three out of four PROMs. These lower baseline scores can likely be explained by the underlying disability of MS-related symptoms, reduced quality of life, and limited daily activities.30,31 Similarly, MS patients continued to demonstrate lower postoperative scores across all 4 PROMs, likely due to the persistence or worsening of MS symptoms and ongoing disease progression. In line with our findings, several studies have noted that MS patients often require more thorough rehabilitation and a longer time to return to baseline function.28,32,33 Interestingly, we observed similar delta scores across all 4 PROMs, indicating that MS THA patients can achieve comparable improvements to non-MS THAs. These findings suggest that MS patients can experience significant improvements in their physical function following surgery, highlighting the efficacy of this surgical intervention in this patient population.
Lastly, when comparing the rates of achieving MCID-I and MCID-W, MS patients demonstrated similar rates for PROMIS Global Physical, PROMIS Global Mental, and HOOS-PS, but a higher rate of experiencing MCID-W for PROMIS PF-10a. This difference is likely multifactorial and likely arises from the functional debility associated with MS, encompassing symptoms like spasticity, mobility limitations, and muscle weakness.34,35 These factors likely contribute to challenges with physical recovery, potentially influencing the higher rate of experiencing MCID-W for PROMIS PF-10a.
This study was not without limitations. Firstly, its retrospective nature may introduce potential bias. Secondly, due to the limited number of arthroplasties in MS patients, the study may be underpowered to fully evaluate complications. However, the study remains significant as the largest institutional cohort of MS THA cases to date, covering 75 THAs. Thirdly, the findings may not be generalisable to the broader MS population due to the limited sample size, potentially biasing the selection towards more highly functioning individuals for arthroplasty. Additionally, the study’s focus was limited to comparing preoperative and 1-year postoperative PROMs. Future studies are needed with extended follow-up periods to comprehensively evaluate the long-term effectiveness of arthroplasty, especially in managing a progressive disease such as MS. Lastly, the inclusion of patients who underwent bilateral, staged THA could introduce additional confounding factors, given that the questionnaires used assess overall health status rather than being side-specific. Nonetheless, this study is the first, to our knowledge, to report on the achievement of MCID-I and MCID-W in MS patients undergoing THA.
This study revealed that MS patients achieve similar rates of MCID-I and MCID-W in most PROMs but exhibit a higher rate of MCID-W for PROMIS PF-10a, along with increased postoperative complications. The present study offers valuable insights for surgeons and patient education, emphasising the importance of careful consideration regarding postoperative complications despite the potential for substantial improvements. Further studies investigating the progressive nature of MS on PROMs and perioperative outcomes are warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HSB: receives royalties from and is a paid consultant for Exactech and Smith & Nephew; has stock options in DEF Medical and Osteon Holdings; receives research support from Zimmer Biomet; receives royalties from Wolters Kluwer, Smith & Nephew and Exactech.
CMM: is a speaker and paid consultant for Smith & Nephew; receives research support from Zimmer Biomet.
These conflicts of interest are stated here but are unrelated to the present study.
All other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.