
Abstract
Introduction:
Osteonecrosis of the femoral head (ONFH) is a progressive disorder characterised by vascular compromise, osteocyte loss, and regional structural deterioration that ultimately leads to femoral head collapse. Because ONFH affects the femoral head heterogeneously, understanding zone-specific structural and mechanical alterations is essential for clarifying mechanisms of structural failure.
Methods:
15 femoral heads obtained during total hip arthroplasty were analyzed using a patient-matched multiscale approach. Trabecular cores from necrotic, sclerotic, and preserved regions within the same femoral heads were evaluated using micro-computed tomography, uniaxial compression testing, nanoindentation, Fourier-transform infrared spectroscopy, x-ray diffraction, and histology to assess microarchitecture, mechanical behaviour, mineral composition, and osteocyte viability.
Results:
Compared with the sclerotic zone, the necrotic zone exhibited pronounced trabecular deterioration, with bone volume fraction (BV/TV) reduced by 55.35% (p < 0.001), apparent elastic modulus reduced by 60.25% (p < 0.001) and mineral/matrix ratio reduced by 51.70% (p < 0.001). In contrast, the sclerotic zone demonstrated increased trabecular density and stiffness but reduced post-yield deformation, indicating a stiff yet brittle mechanical phenotype. These findings reveal a mechanical paradox in which dense sclerotic bone surrounds structurally compromised necrotic tissue.
Conclusions:
This zonal heterogeneity in microarchitecture, composition, and mechanical behavior may generate stiffness gradients within the femoral head and may contribute to localised stress concentration and mechanical imbalance during ONFH progression. These findings provide a mechano-biological framework for understanding femoral head failure and highlight the importance of considering zonal bone quality in evaluating structural collapse.
Introduction
Osteonecrosis of the femoral head (ONFH) is a debilitating disease of the body, in which the blood circulation in the subchondral region is hindered, resulting in the death of osteocytes and bone marrow. This vascular compromise initiates a cascade of pathological events, including trabecular degeneration, subchondral fracture, and eventual collapse of the femoral head articular surface. 1 The non-traumatic ONFH occurs due to complicated factors of systemic impact such as chronic use of corticosteroids, excessive use of alcohol, metabolic disorders, and coagulation disorders. ONFH commonly affects young to middle-aged adults.2,3 Histopathologically, ONFH has a series of stages, the first stage being the necrosis of bone marrow and osteocytes, followed by an insufficient or a defective reparation process. 4 In osteonecrosis, neovascularisation is often observed at the periphery of the necrotic lesion, where reparative processes contribute to the formation of a sclerotic rim. This dense trabecular boundary may act as a structural barrier that limits vascular ingrowth into the necrotic core and partially isolates it metabolically.1,5 The pathophysiology through which infarction causes collapse of the femoral head remains uncertain, but weakening of the mechanical integrity of cancellous bone has been implicated to a large extent.6,7 This biomechanical mismatch at the border of necrotic and sclerotic bone formations may lead to local stress concentrations, especially during normal physiological loading. Several studies with use of finite element analysis and magnetic resonance imaging have found that there is augmented mechanical pressure at the margins of necrotic territories, which is parallel to the locations where micro-fractures generally begin.8–10 There is a redistribution of cellular activity within these zones; osteoclastic bone resorption is enhanced in areas of necrosis as compared to osteoblastic bone formation in areas of sclerosis, and structural heterogeneity is further augmented. 1 Clinically, radiographic and structural manifestations of post-traumatic osteonecrosis of the femoral head are typically observed within 1–3 years following the initial vascular compromise, particularly after femoral neck fracture or hip dislocation.1,5 This temporal delay between vascular compromise and structural collapse suggests that mechanical deterioration and progressive structural imbalance contribute to disease progression following the initial ischaemic event. The delayed clinical manifestation of ONFH suggests that vascular compromise alone may not fully explain disease progression, and that additional biological and mechanical factors, such as reparative responses, lesion size, and mechanical loading, may influence the timing of structural failure. Furthermore, the necrosis in the femoral head is not localised to anatomical areas of known vascularity; biomechanical variables might play an important role in the development and progression of ONFH.11–13 The observations suggest that micro-architectural perturbation and redistribution of mechanical loads may be the main cause of femoral head collapse and not large-scale alteration in bone composition. The changes in its biomechanical features, bone quality determinants, and internal structure organisation are probably major factors in disease process.
A mechanical explanation of ONFH should be zone-based assessment since femoral head is not affected in every part. The necrotic zone is associated with severe trabecular structure osteocytes loss; the sclerotic zone is a dense but may be brittle shell, and an intact subchondral area may be present with these altered tissues. The extent to which these regions vary in structural, compositional, and mechanical scales and impact of such heterogeneity on overall stability of the head is not well defined. In order to fill this gap, we performed a multiscale study of necrotic (NCZ), sclerotic (SCZ), and preserved healthy zones (HZ) of the same osteonecrotic femur heads. The current study provides direct structure-composition-mechanics relationships between zones through the combination of micro-CT architecture, bulk compressive behavior, nano-indentation-based tissue mechanics, FTIR (Fourier-transform infrared spectroscopy) and XRD (x-ray diffraction) mineral composition, and histological evaluation. This approach highlights the mechanical paradox of the sclerotic zone, which is dense and stiff yet brittle, and clarifies how localised heterogeneity in bone quality may contribute to mechanical imbalance and increase susceptibility to failure in ONFH.
Materials and methods
Study participants and sample preparation
Femoral heads were obtained from patients with ONFH undergoing total hip arthroplasty (THA) at Max Superspeciality Hospital, Mohali, India, between January 2023 and June 2025. Inclusion required radiographic confirmation of ONFH based on anteroposterior (AP) and frog-leg lateral hip radiographs according to the modified Ficat-Arlet staging and a clinical indication for THA. 14 Disease stage was determined according to the Ficat-Arlet classification based on preoperative radiographic assessment. Patients with osteoporosis (T-score ⩽ -2.5 according to WHO criteria), diabetes mellitus, chronic liver or renal disease, prior hip fracture, inflammatory arthritis, prolonged immobilisation, or medications affecting bone metabolism (e.g., bisphosphonates, denosumab, teriparatide, antiepileptics) were excluded. Alcohol-associated osteonecrosis was defined as chronic consumption ⩾320 g ethanol/week (⩾45.7 g/day) for ⩾6 months, whereas steroid-induced osteonecrosis was defined by a cumulative prednisone-equivalent dose ⩾2 g within the preceding 12 months. 15 femoral heads fulfilling these criteria were included. The areal bone mineral density (aBMD) and T-scores of the contralateral femoral neck were obtained from preoperative dual-energy x-ray absorptiometry (DXA) scans performed within 3 months before surgery. The study protocol was approved by the Institutional Ethics Committee of Max Superspeciality Hospital, Mohali (Ref. No. BHR/TS/MSSH/HBPL/MOHALI/IEC/GASTRO/23-06), and written informed consent was obtained from all participants. The comprehensive details of the clinical parameters are provided in Table 1. Excised femur heads (Figure 1 (i) (a) and (b)) following THA were put under saline-covered gauze, placed in airtight containers, and kept at −80°C. Specimens were bisected parallel to the head-neck axis using a customised water-cooled bone saw, and cylindrical trabecular cores (~5 mm diameter, 9–10 mm length) were extracted from necrotic (NCZ), sclerotic (SCZ), and preserved healthy zones (HZ) in the coronal plane using a diamond-coated core drill under continuous cooling (Figure 1 (i) (c) and (d)). End surfaces were trimmed to obtain parallel loading faces, and specimen diameter and length were measured using a digital vernier caliper (±0.01 mm). Diameter was recorded at 3 positions along each core and averaged to calculate cross-sectional area for stress normalisation. To ensure anatomical consistency, cores were harvested from comparable depths beneath the subchondral plate within the weight-bearing region, avoiding the subchondral cortical layer; sampling locations were guided by macroscopic inspection and micro-computed tomography (micro-CT) imaging.
Patient-specific clinical data.
FN, femoral neck; aBMD, areal bone mineral density; BMI, body mass index.
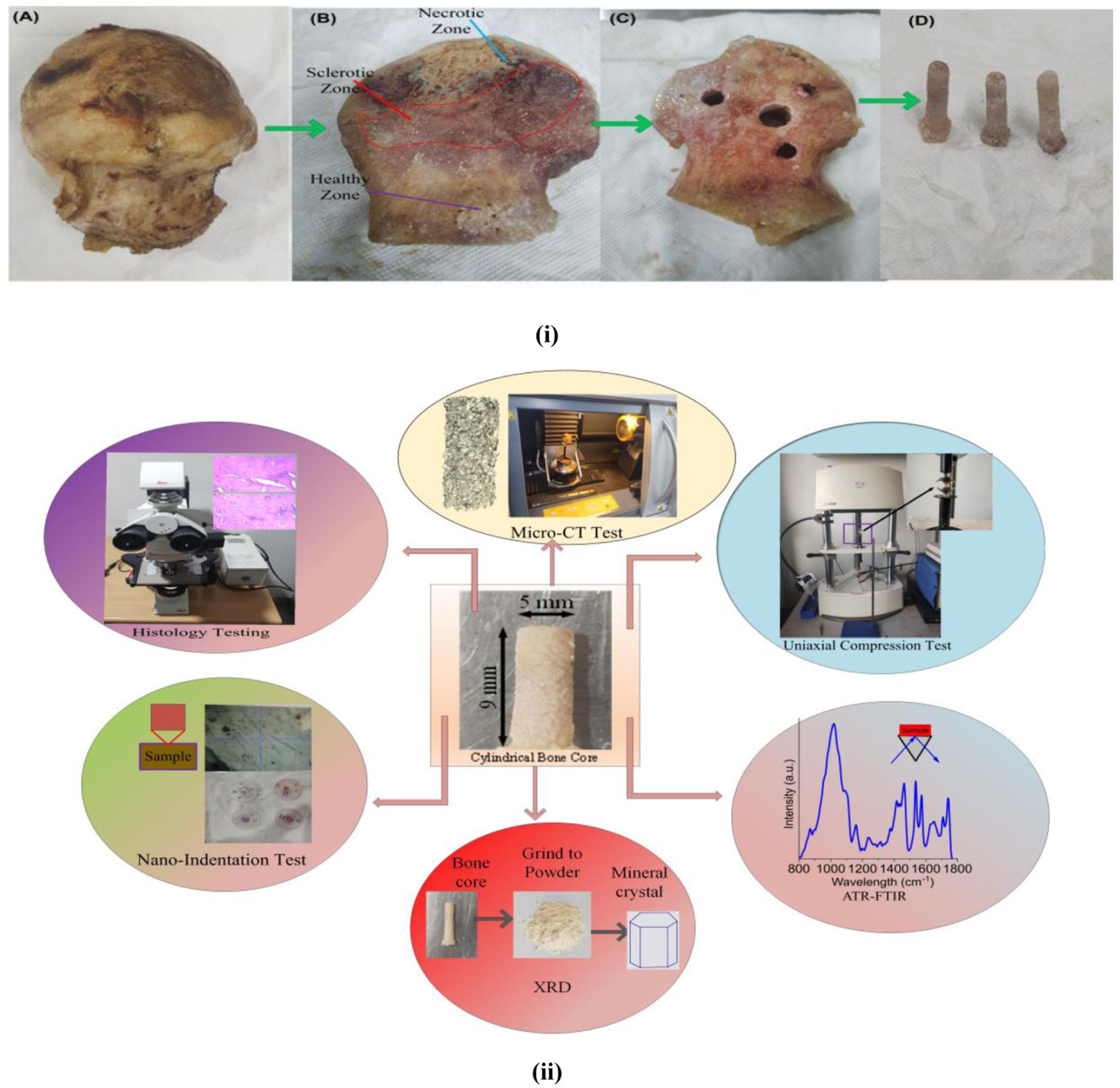
(i) Sequential workflow for core extraction (a) Cleaned femoral head affected by osteonecrosis, (b) orientation along the coronal plane, (c) drilled coronal section showing core trajectory, (d) retrieved cylindrical trabecular core. (ii) Overview of the experimental procedures used for trabecular bone characterisation.
To obtain sufficient material for multimodal analyses, 2–3 cores were harvested from each zone (approximately 6–9 cores per femoral head). However, to avoid pseudo-replication and preserve statistical independence, the femoral head (patient) was treated as the experimental unit; therefore, 1 representative specimen per zone per femoral head was included in quantitative statistical analyses (n = 15 independent observations per zone). Remaining cores were allocated to complementary experimental modalities (e.g., mechanical testing, nano-indentation, compositional analyses, and histology) using distinct specimens while maintaining patient-level independence. Because NCZ, SCZ, and HZ measurements originated from the same femoral head, zone was treated as a within-subject factor in repeated-measures statistical analyses. Zonal identification was determined using preoperative radiographs, intraoperative observations, and characteristic micro-CT and histological features. The classification was independently evaluated by 2 investigators blinded to the mechanical outcomes, and any discrepancies were resolved through consensus. The necrotic zone (NCZ) was defined as the central region of the femoral head lesion characterised by trabecular rarefaction, structural discontinuity, and reduced bone volume fraction on micro-CT, typically located beneath the subchondral plate within the lesion core. The sclerotic zone (SCZ) was identified as the dense trabecular rim surrounding the necrotic region, exhibiting increased trabecular thickness and bone volume fraction on micro-CT and located adjacent to the lesion margin. The preserved healthy zone (HZ) was sampled from morphologically intact trabecular bone distant from the necrotic lesion and outside the sclerotic rim, typically located toward the inferior or peripheral femoral head (Figure 1 (i) (b)). To minimise misclassification, specimens showing mixed structural features or ambiguous boundaries between zones were excluded from sampling (Figure 1 (i) (a)). Prior to testing, specimens were thawed at 4°C for ~12 hours and equilibrated to room temperature in phosphate-buffered saline (PBS) to maintain hydration during preparation and testing.
Assessment of bone quality indicators
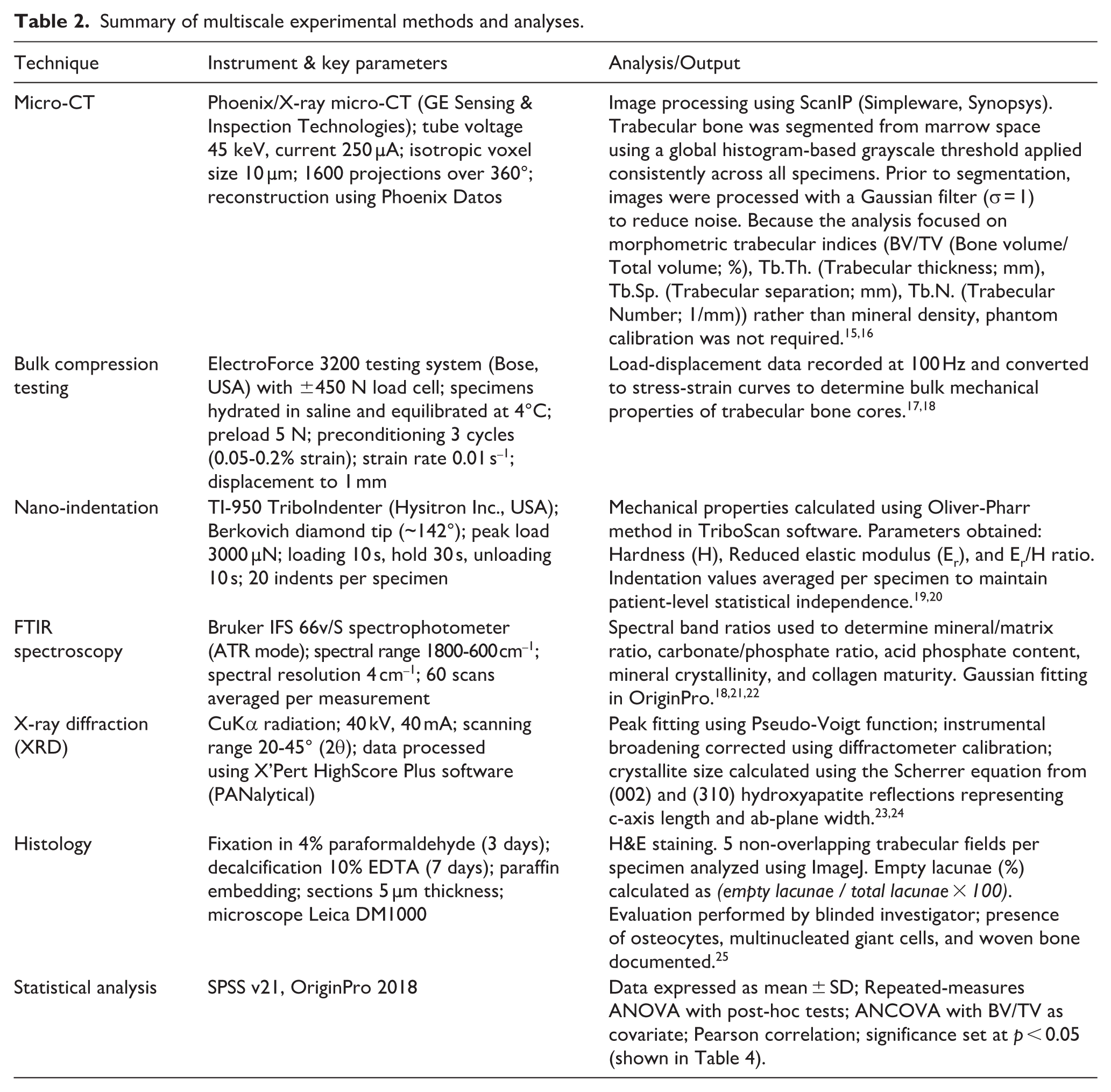
Morphological parameters at the microscopic level were evaluated using micro-CT on trabecular cores extracted from sclerotic, necrotic, and healthy zones. Uniaxial compression testing was used to determine bulk mechanical properties and nano-indentation was used to measure tissue-level mechanical behavior. Fourier-transform infrared spectroscopy (FTIR) was employed to examine mineral and collagen structure and x-ray diffraction (XRD) was used to characterise crystallographic characteristics. Histological examination was subsequently performed to assess morphological and cellular features, followed by statistical analysis of all measured parameters. Detailed experimental conditions, testing parameters, and instrumentation for all analyses are summarised in Table 2.
Summary of multiscale experimental methods and analyses.
Results
Bone microstructure and morphometric data
Representative micro-CT reconstructions of trabecular cores and corresponding coronal sections are shown in Figure 2 (a)–(c) and (d)–(f)), with quantitative morphometric parameters presented in Figure 2 (a)–(d). Compared with the sclerotic zone (SCZ), the necrotic zone (NCZ) exhibited marked architectural deterioration, with BV/TV reduced by 55.35% (p < 0.001) and trabecular thickness (Tb.Th) reduced by 39.28% (p < 0.001). Consistent with this deterioration, NCZ also showed a lower trabecular number (Tb.N: 1.16 ± 0.11 mm–1) compared with SCZ (1.60 ± 0.09 mm–1, p < 0.001) and increased trabecular separation (Tb.Sp: 0.67 ± 0.10 mm) relative to SCZ (0.31 ± 0.04 mm, p < 0.001). When compared with the preserved healthy zone (HZ), NCZ similarly demonstrated reduced microarchitectural integrity, with BV/TV reduced by 18.61% (p < 0.01) and Tb.Th reduced by 14.44% (p < 0.01). In addition, NCZ showed a slightly lower trabecular number (Tb.N: 1.16 ± 0.11 mm–1 vs. 1.25 ± 0.11 mm–1, p < 0.05) and greater trabecular separation (Tb.Sp: 0.67 ± 0.10 mm vs. 0.59 ± 0.05 mm, p < 0.01) compared with HZ.
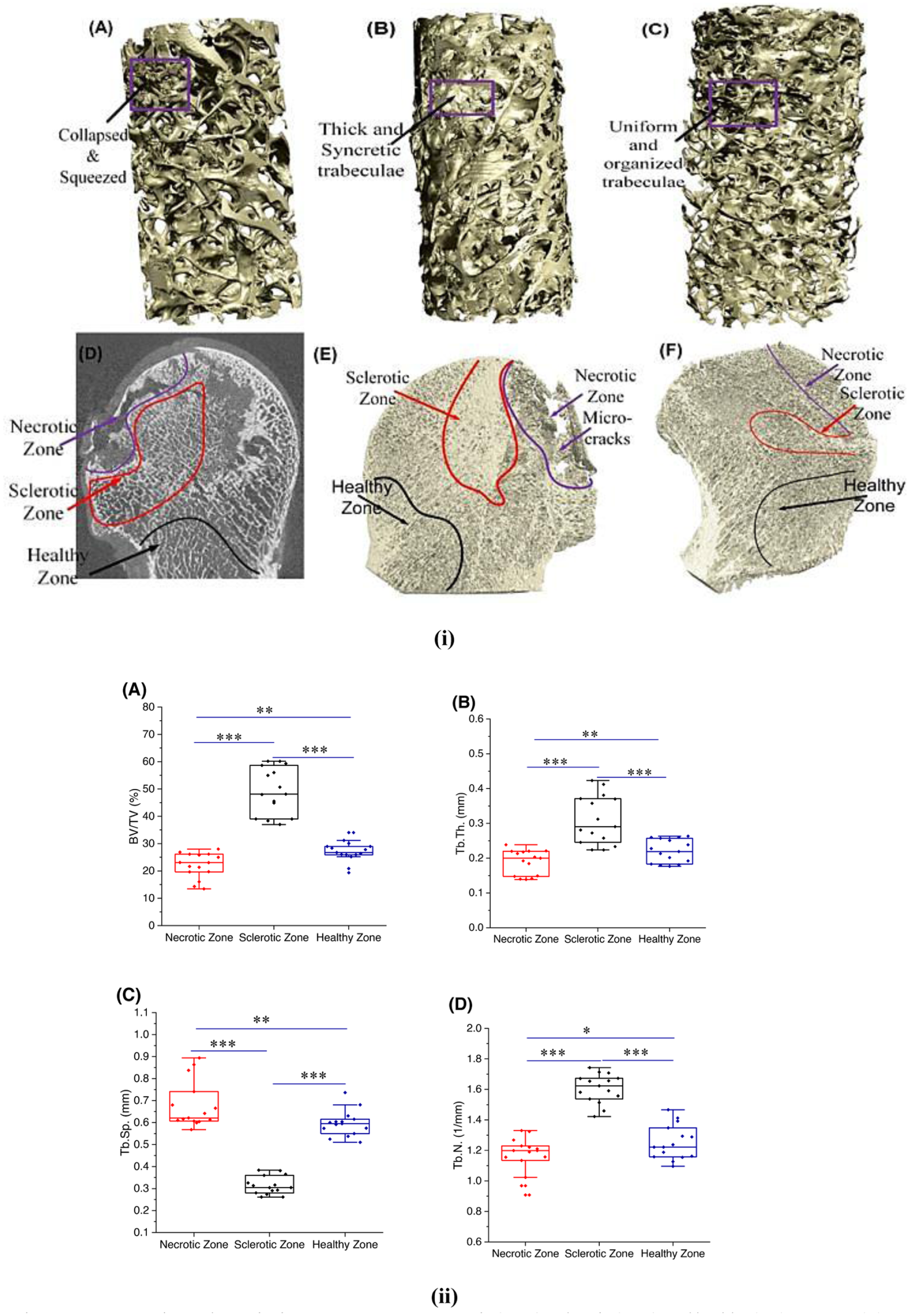
3D micro-CT representation and quantitative parameters across necrotic (NCZ), sclerotic (SCZ), and healthy (HZ) zones. (i) (a) Necrotic region (b) Sclerotic region (c) Healthy region (d) Ficat-Arlet Radiographic segmentation of ONFH (e) Coronal slice of femur head (alcohol induced) (f) Coronal slice of femur head (corticosteroid induced). (ii) (a) BV/TV (Bone volume/Total volume; %), (b) Tb.Th. (Trabecular thickness; mm) (c) Tb.Sp. (Trabecular separation; mm), (d) Tb.N. (Trabecular Number; 1/mm). (The significance was indicated as ***, p ⩽ 0.001; **, p ⩽ 0.01; *, p ⩽ 0.05 between zones).
Mechanical properties
The stress-strain profiles and quantified mechanical properties demonstrated distinct behavioral variations among the 3 bone zones (Figure 3 (i) (a)–(h)). In the necrotic zone (NCZ), a substantial reduction in mechanical strength was observed compared with the sclerotic zone (SCZ) of the same femoral head. Specifically, yield stress, representing the stress at which trabecular bone begins to undergo irreversible deformation and transitions from elastic to plastic behavior, decreased by 54.59% (p < 0.001). Ultimate stress, defined as the maximum stress sustained before structural weakening of the trabecular network, was reduced by 52.10% (p < 0.001). Fracture stress, indicating the stress level at which complete structural failure of the trabecular framework occurs, declined by 31.97% (p = 0.0055). The apparent elastic modulus, calculated from the initial linear region of the stress-strain curve and reflecting the stiffness of the trabecular structure under compressive loading, decreased by 60.25% (p < 0.001). In addition, overall toughness was reduced by 42.06% (p = 0.0439). Toughness was calculated as the area under the stress-strain curve from the onset of loading up to the point of fracture, representing the total energy absorbed by the specimen prior to failure. In comparison with the preserved healthy zone (HZ), NCZ also exhibited significantly reduced mechanical parameters, including a 29.04% decrease in yield stress (p = 0.0188), a 29.19% reduction in ultimate stress (p = 0.0186), a 47.91% decrease in fracture stress (p < 0.001), a 28.80% reduction in elastic modulus (p = 0.0183), and a 62.77% reduction in toughness (p < 0.01).
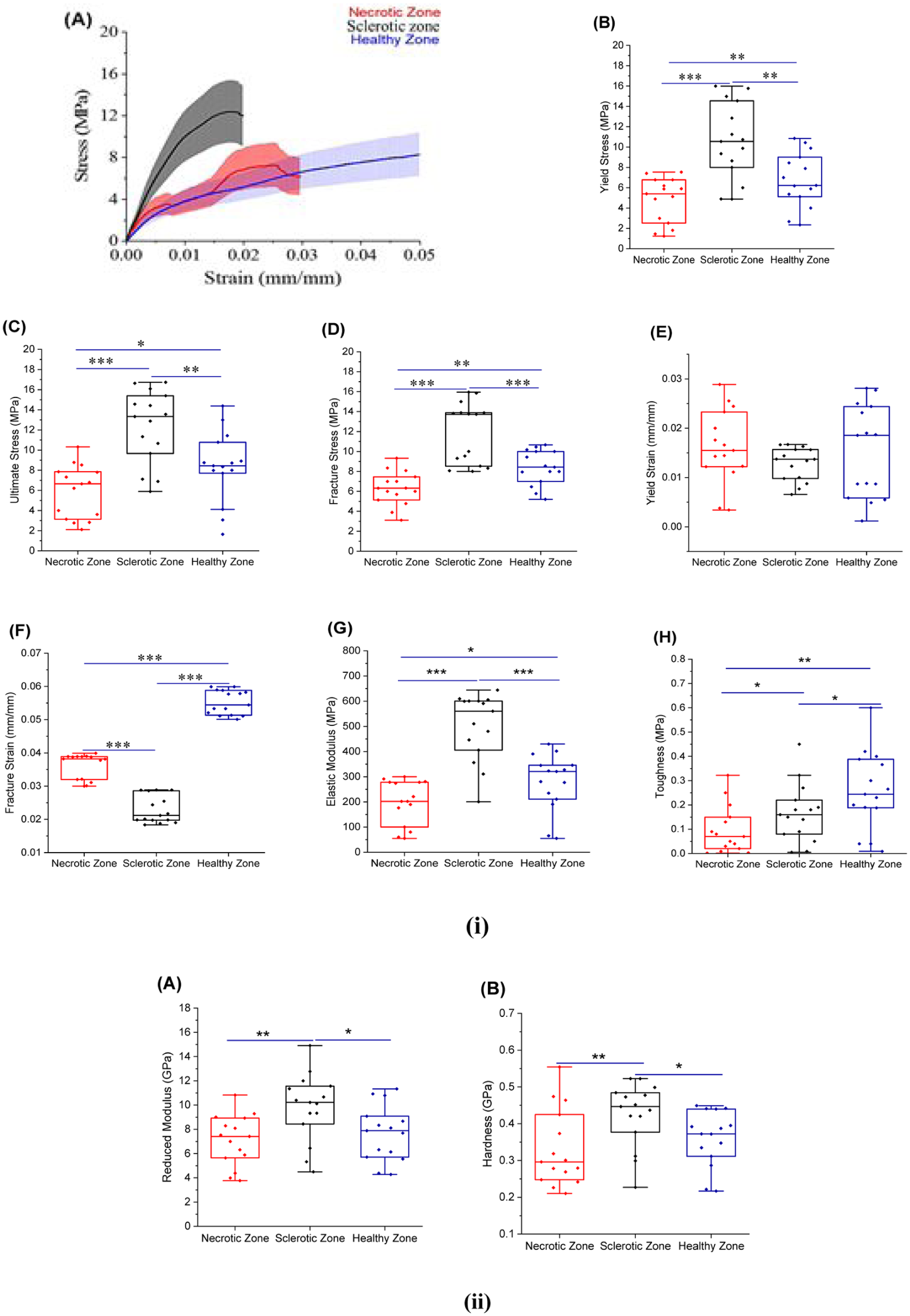
Bulk and tissue level mechanical properties of trabecular bone across necrotic (NCZ), sclerotic (SCZ), and healthy (HZ) zones. (i) (a) Representative stress-strain curves showing mean response with standard deviation as error bars, (b) Yield stress (MPa), (c) Ultimate stress (MPa), (d) Fracture stress (MPa), (e) Yield strain (mm/mm), (f) Fracture strain (mm/mm), (g) Elastic modulus (MPa), (h) Toughness (MPa). (ii) (a) Reduced modulus (GPa) (b) Hardness (GPa) between Sclerotic, Necrotic, and Healthy Zone of ONFH (The significance was indicated as ***, p ⩽ 0.001; **, p ⩽ 0.01; *, p ⩽ 0.05 between zones).
Bone material properties
The average hardness (H) and tissue level reduced modulus (Er) of each region are specified in Figure 3 (ii) (a) and (b). The NCZ showed a major reduction in mechanical properties relative to the SCZ, as Er and H reduced by 27.83 (p < 0.01) and 22.13 (p < 0.01), respectively. On the other hand, mechanical properties within the NCZ were similar to that of the healthy zone and no significant differences were found between the hardness and reduced modulus in the 2 zones.
Mineral and collagen properties
FTIR analysis revealed pronounced compositional heterogeneity across the necrotic, sclerotic, and preserved zones of the osteo-necrotic femoral head (Figure 4 (i) (a)–(f)). The necrotic zone (NCZ) demonstrated significantly elevated carbonate/phosphate ratio (increased by 50.46%, p < 0.01) and acid phosphate content (increased by 47.58%, p < 0.001) compared with the sclerotic zone (SCZ). Additionally, NCZ showed a marked reduction in mineral/matrix ratio (by 51.70%, p < 0.001), mineral crystallinity (by 12.74%, p = 0.02), and collagen maturity (by 28.28%, p = 0.028) relative to SCZ. Compared with the preserved healthy zone (HZ), NCZ similarly exhibited a reduced mineral/matrix ratio (by 34.72%, p = 0.042), together with increased carbonate/phosphate (by 29.93%, p = 0.03) and acid phosphate content (by 24.72%, p = 0.01), whereas differences in mineral crystallinity and collagen maturity between NCZ and HZ were not statistically significant. Collagen-related protein features were characterised using the Amide I and Amide II bands, which arise primarily from C=O stretching vibrations and N–H bending/C–N stretching vibrations of the collagen backbone, respectively. Overall, the normalised peak areas of Amide I and Amide II in NCZ were substantially lower by 43.85% (p < 0.001) and 53.29% (p < 0.001) compared with the healthy zone, indicating deterioration of collagen matrix integrity within the necrotic region. Detailed peak positions and band ratios are summarised in Table 3.
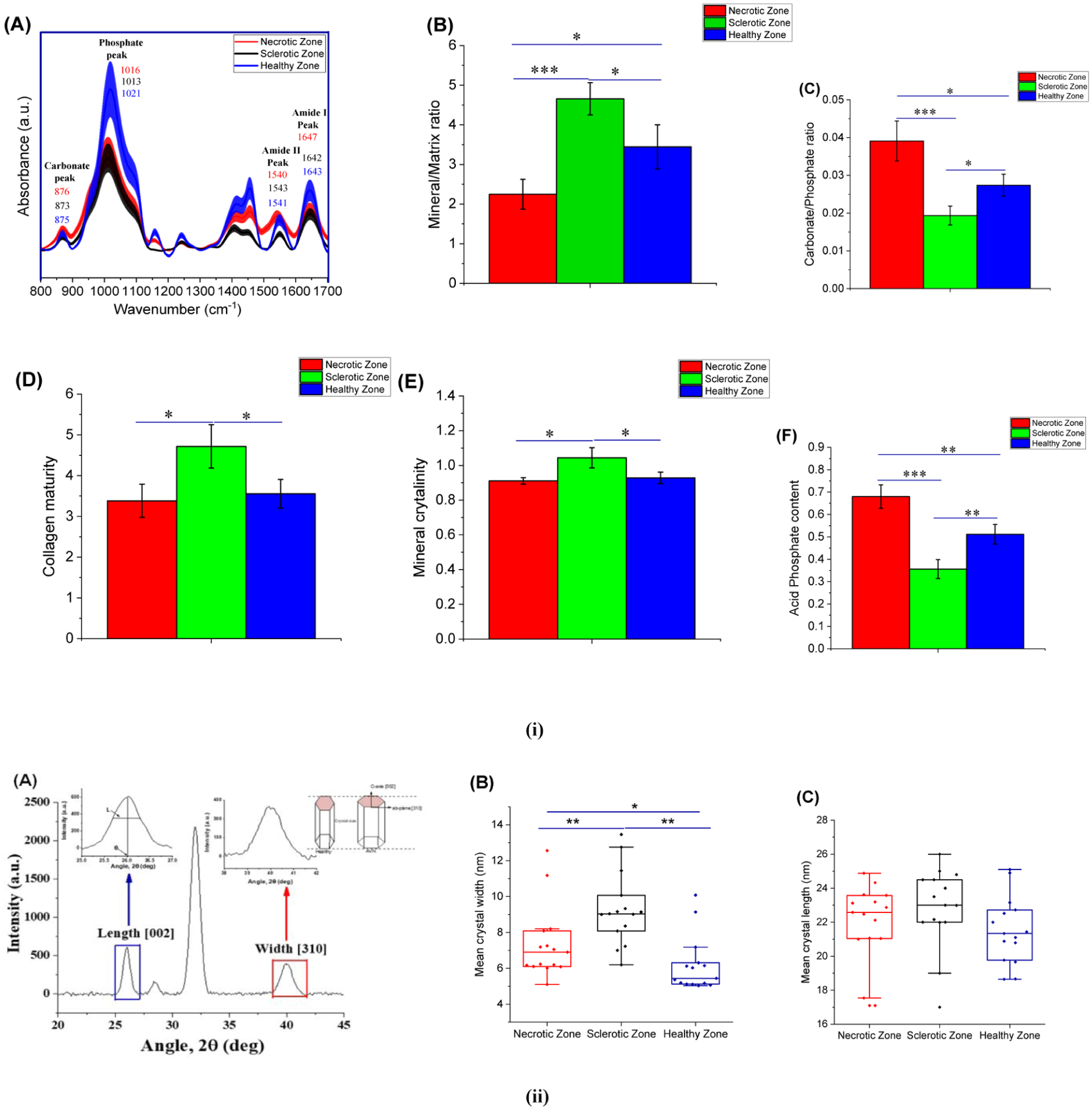
FTIR and XRD analysis of trabecular bone from necrotic (NCZ), sclerotic (SCZ), and healthy (HZ) zones. (i) (a) Representative FTIR spectra showing characteristic mineral and collagen bands, (b) Mineral:Matrix, (c) Carbonate:Phosphate, (d) Collagen maturity, (e) Mineral Crystallinity, (f) Acid-Phosphate content. (The significance was indicated as ***, p ⩽ 0.001; **, p ⩽ 0.01; *, p ⩽ 0.05 between zones). (ii) (a) Representative XRD profile of human trabecular bone (20° < 2θ < 45°). The diffraction peaks near ~26° and ~40° were used to calculate average crystallite length (c-axis) and width (ab-plane), respectively, using the Scherrer relation L = Kλ / (β cosθ), where λ = 1.5406 Å, β = full width at half maximum, and θ = Bragg angle. (b, c) Mean crystallite size plots showing comparable crystal length across groups but a broader crystallite width in the osteonecrotic samples.
FTIR-derived compositional parameters of necrotic (NCZ), sclerotic (SCZ), and preserved healthy zones (HZ) of osteonecrotic femoral heads.
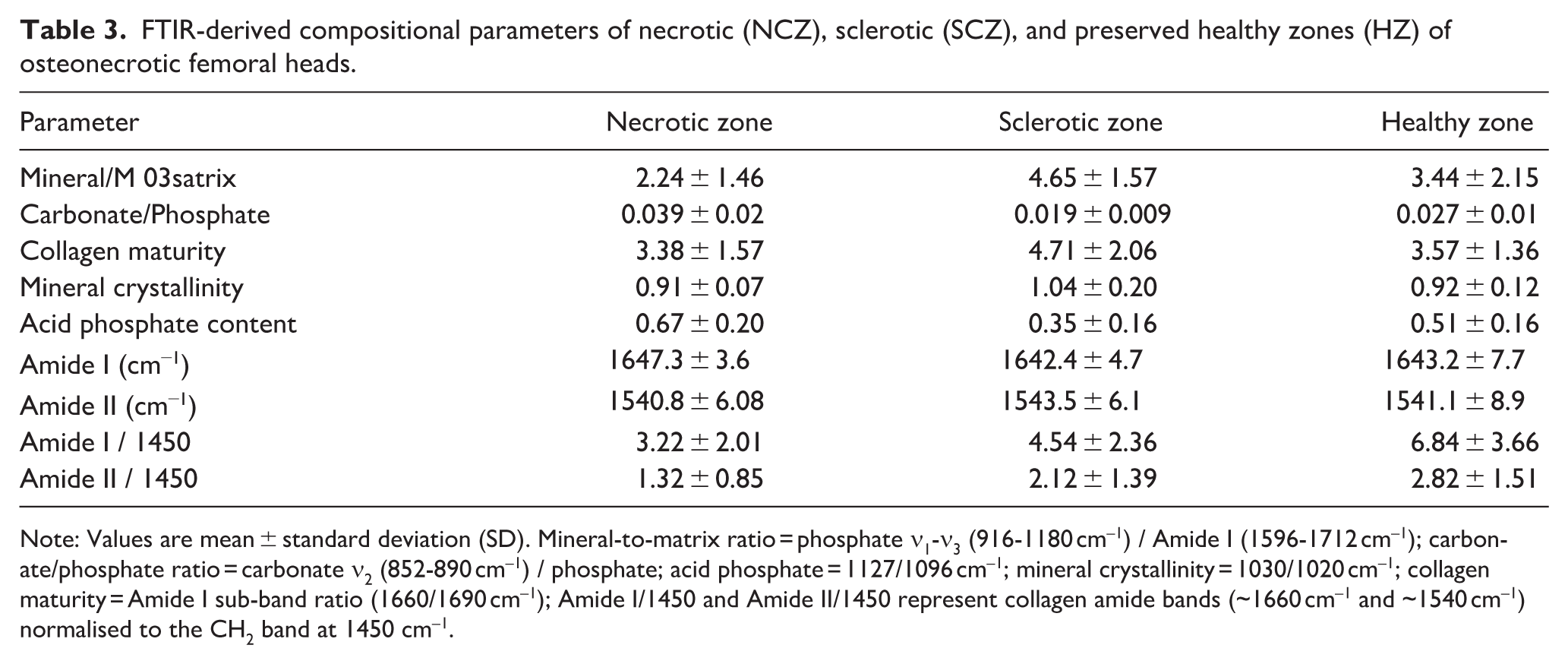
Note: Values are mean ± standard deviation (SD). Mineral-to-matrix ratio = phosphate ν1-ν3 (916-1180 cm–1) / Amide I (1596-1712 cm–1); carbonate/phosphate ratio = carbonate ν2 (852-890 cm–1) / phosphate; acid phosphate = 1127/1096 cm–1; mineral crystallinity = 1030/1020 cm–1; collagen maturity = Amide I sub-band ratio (1660/1690 cm–1); Amide I/1450 and Amide II/1450 represent collagen amide bands (~1660 cm–1 and ~1540 cm–1) normalised to the CH2 band at 1450 cm–1.
Average mineral crystal dimension
The XRD spectra for trabecular bone samples from different zones are shown in Figure 4 (ii). The calculated crystallite dimensions revealed no significant differences in crystal length among zones. However, crystallite width exhibited clear regional variation. The necrotic zone demonstrated a significantly greater crystal width compared with the preserved healthy region (7.35 ± 2.02 nm vs. 6.16 ± 1.53 nm, p = 0.04), whereas the sclerotic zone showed the highest average crystal width (9.28 ± 2.00 nm).
Histological features
Histological images illustrating mid-coronal slice morphology from each zone are shown in Figure 5 (i) (a)–(c). The necrotic zone (NCZ) exhibited a markedly higher proportion of empty lacunae (64.19 ± 13.22%, p < 0.001; indicated by black arrows) compared with the sclerotic zone (SCZ) (18.89 ± 8.52%). In contrast, the preserved region displayed a greater presence of viable osteocytes (red arrows), resulting in a significantly lower proportion of empty lacunae (41.80 ± 12.33%, p < 0.001) relative to NCZ. Qualitative histological examination further revealed the presence of woven bone (green arrows) within NCZ, suggesting localised reparative responses associated with structural deterioration. In addition, multinucleated giant cells (blue arrows) were more frequently observed in NCZ than in the preserved region, consistent with osteoclast-like resorptive activity involved in the removal of necrotic bone during the remodelling process.
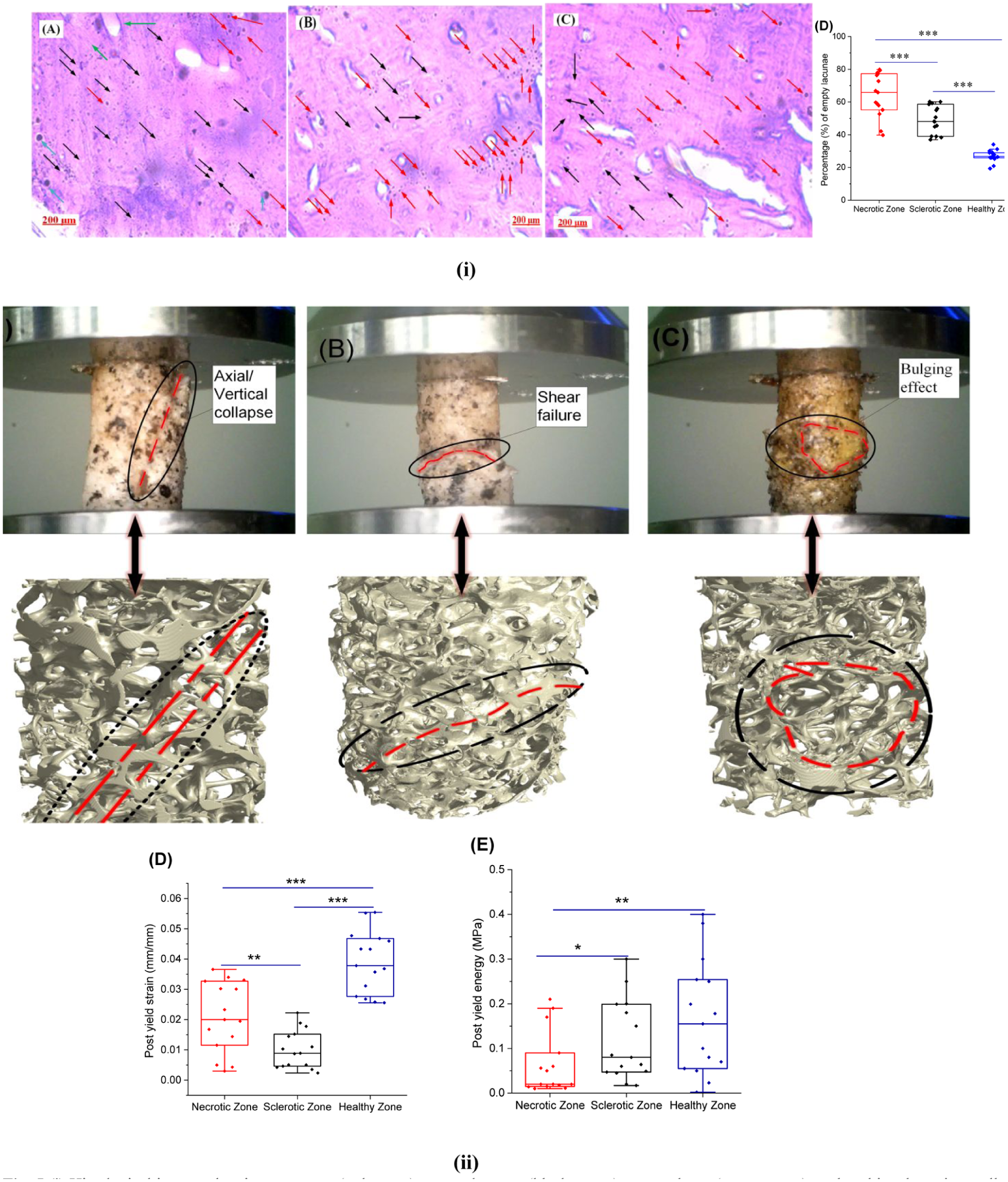
(i) Histological images showing osteocyte (red arrow), empty lacunae (black arrow), woven bone (green arrow), and multinuclear giant cells (blue arrow) in (a) Necrotic zone, (b) Sclerotic zone, (c) Healthy Zone, (d) Percentage (%) of empty lacunae. (ii) Failure patterns of trabecular bone cores obtained from necrotic (NCZ), sclerotic (SCZ), and healthy (HZ) (a) Necrotic zone, (b) Sclerotic zone, (c) Healthy zone, (d) Post-yield strain (mm/mm), (e) Post-yield energy (MPa). (The significance was indicated as ***, p ⩽ 0.001; **, p ⩽ 0.01; *, p ⩽ 0.05 between zones).
Zone-specific failure modes under uniaxial compression
In the necrotic zone (NCZ), a marked reduction in post-yield mechanical capacity was observed compared with the sclerotic zone (SCZ) of the same femoral head (Figure 5 (ii)). Specifically, post-yield energy, representing the energy absorbed by trabecular bone during plastic deformation after the yield point until failure, decreased by 45.36% (p = 0.0411), while post-yield strain, indicating the extent of deformation sustained after yielding before fracture, was reduced by 54.54% (p < 0.01). Relative to the preserved healthy zone, NCZ also demonstrated significantly lower post-yield energy by 61.77% (p < 0.01) and post-yield strain by 37.23% (p < 0.01). Failure morphology further differed among the zones. The criteria used to classify the failure modes observed during uniaxial compression testing. Failure patterns were categorised based on post-test inspection of the fractured specimens together with the corresponding stress-strain responses. The NCZ demonstrated a relative prevalence of axial or vertical collapse patterns, that is, the weakening of the trabeculae structure and the inability to support the loads. On the other hand, a typical shear-type failure with diagonal planes of fracture was observed in the SCZ, which is expected because of the increased stiffness and brittle behaviour. The healthy zone had a bulging deformation pattern before failure, which was more ductile and had a higher ability to absorb energy and redistribute stress.
Discussion
This paper presents a multiscale comparison of trabecular bone in necrotic, sclerotic and preserved areas of osteonecrotic femoral heads and shows severe zone-specific differences in microarchitecture, composition and mechanical behaviour. Specifically, the necrotic zone (NCZ) exhibited substantial reductions in trabecular thickness, mineral/matrix ratio, collagen integrity, and mechanical strength, whereas the sclerotic zone (SCZ) showed increased mineralisation and stiffness but reduced post-yield deformation, indicating a brittle mechanical phenotype. The deterioration of bone quality and mechanical properties can occur as a cumulative effect of interrelated changes taking place at multiple length scales that include altered mineral and collagen integrity at the nanoscale, accumulation of micro-cracks at the microscale, and destabilised trabecular architecture and connectivity at the mesoscale. Thus, the micro and meso-scale disparities observed in this study may be interrelated and collectively contribute to larger structural impairment, providing a more comprehensive understanding of bone fragility and fracture susceptibility in osteonecrosis of the femoral head.
According to the micro-CT, NCZ has the least structural integrity with very low BV/TV, Tb.Th, Tb.N, and the highest Tb.Sp compared to SCZ and healthy parts. Bone microarchitecture changes in both animals and humans have been markedly altered.7,26,27 These structural changes were also directly linked to biomechanical degradation with the necrotic zone having far lesser toughness, post-yield energy, ultimate stress, yield stress, fracture stress and apparent modulus compared to the SCZ and healthy areas. These are the results expected of the past study. 7 The impaired nano-mechanical state of NCZ was also supported by nano-indentation data at tissue level as it had a lower modulus (tissue level) and value of hardness than SCZ, but not significantly different than healthy bone, which provided evidence of heterogeneity at the microscale. This observation suggests that osteonecrosis may primarily disrupt trabecular architecture and microstructural integrity rather than uniformly altering intrinsic material properties of the mineralised matrix. Previous studies have also indicated that structural deterioration at the micro and mesoscale contributes more strongly to mechanical failure than nanoscale changes in tissue material properties. 7 The FTIR analysis showed that the necrotic area had a lower mineral/matrix ratio, less collagen maturity, and reduced mineral crystallinity, and had a larger carbonate to phosphate ratio, and a high acid phosphate level than the sclerotic and healthy bone areas. These results in NCZ indicate not only affected mineralisation, but also collagen and protein misfolding, as the Amide I/II bands were smaller. The sclerotic zone exhibited higher mineral/matrix ratio, higher the collagen maturity, and wider crystal width. The increased average mineral content is an indication of less remodeling activity and longer secondary mineralisation as opposed to active high turnover repair. The prolonged residence of tissues allows further crystal growth and development of fully cross-linked collagen, as is typical of a hypermineralised and structurally aged matrix phenotype, as is available in the literature.28,29 XRD-determined crystal morphology did not show any significant difference in crystal length between zones, but crystal width in both SCZ and NCZ was significantly higher than in the healthy one, suggesting further mineral malformation in NCZ, and thick, potentially fragile, mineral packing in SCZ. Histological analysis (Figure 5 (i)) showed that the percentage of empty lacunae within the necrotic area had high concentration, which suggests that there is high loss of osteocytes and loss of cell viability. This area also exhibited enhanced woven bone remodeling and a reduced multinucleated giant cell, which are considered to be indicative of pathological imbalance of bone turnover that can further weaken the structure, which had been reported before.7,12,28,29 The SCZ exhibited dense osteocyte lacunae within a highly mineralised trabecular framework, consistent with prolonged tissue age and reduced remodelling activity, which may contribute to its increased mechanical strength and stiffness. In contrast, the healthy zone maintained a relatively balanced trabecular morphology with fewer pathological alterations.
Our results, combined, indicate that NCZ is an area of architectural loss, lost tissue mechanics, and severe osteocyte depletion, and SCZ is a highly dense, high-stiffness rim that is a paradoxically brittle shell with minimal post-yield behavior and modified mineral quality. This hard and fragile sclerotic periphery, in contrast to the mechanically compromised necrosis of the core, may generate a localised disparity capable of increasing the stress in the presence of physiological loading. Correlation and regression analysis (Table 4 and Figure 6), and Multimodal analyses, including micro-CT, bulk mechanical testing, nanoindentation, FTIR/XRD, and histology, suggest that the sclerotic region forms a stiff yet structurally vulnerable interface surrounding the necrotic core. Such zonal heterogeneity may promote load redistribution and increase susceptibility to subchondral failure in osteonecrosis of the femoral head.
Pearson correlation coefficients of key variables of the necrotic, sclerotic, and healthy zone.
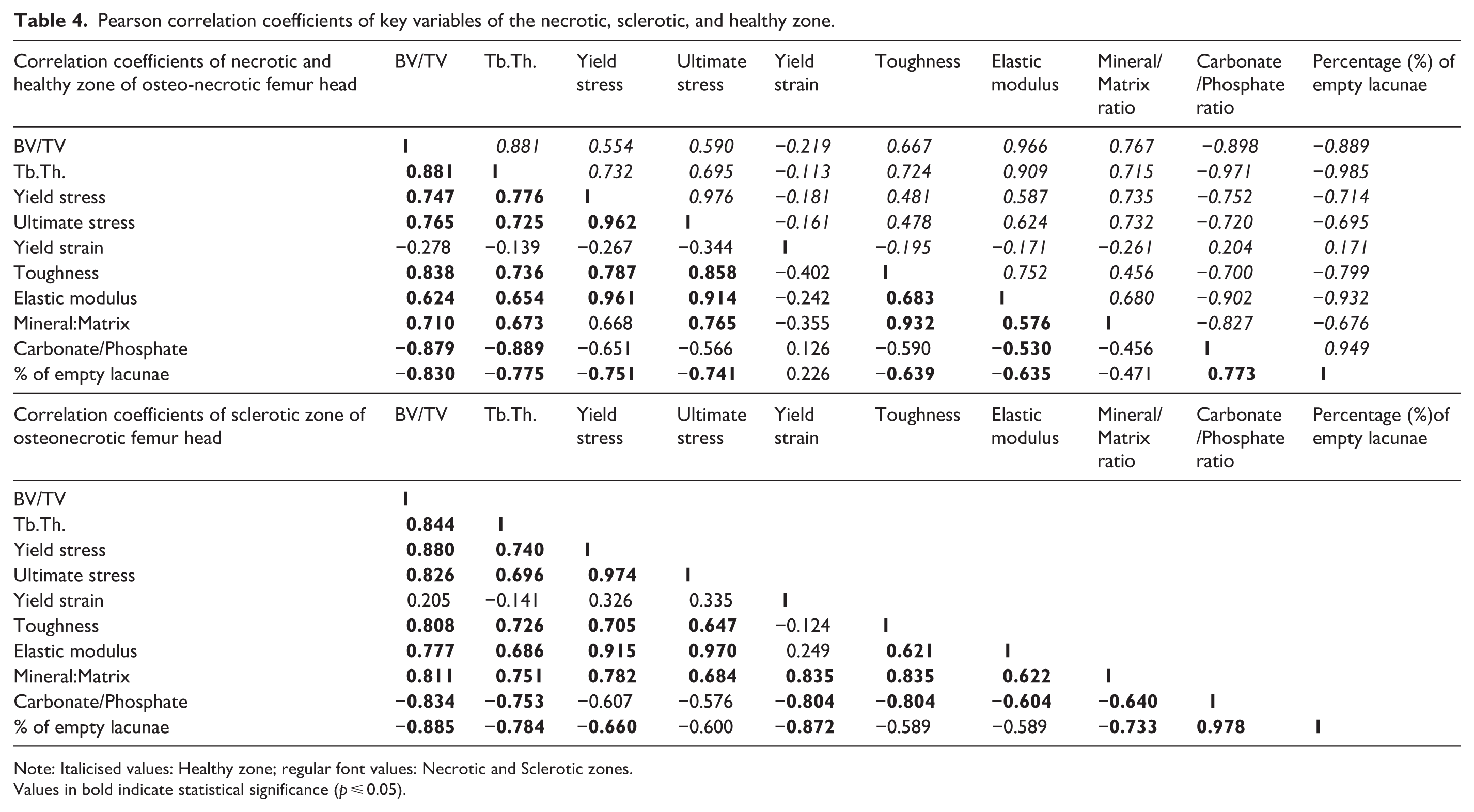
Note: Italicised values: Healthy zone; regular font values: Necrotic and Sclerotic zones.
Values in bold indicate statistical significance (p ⩽ 0.05).
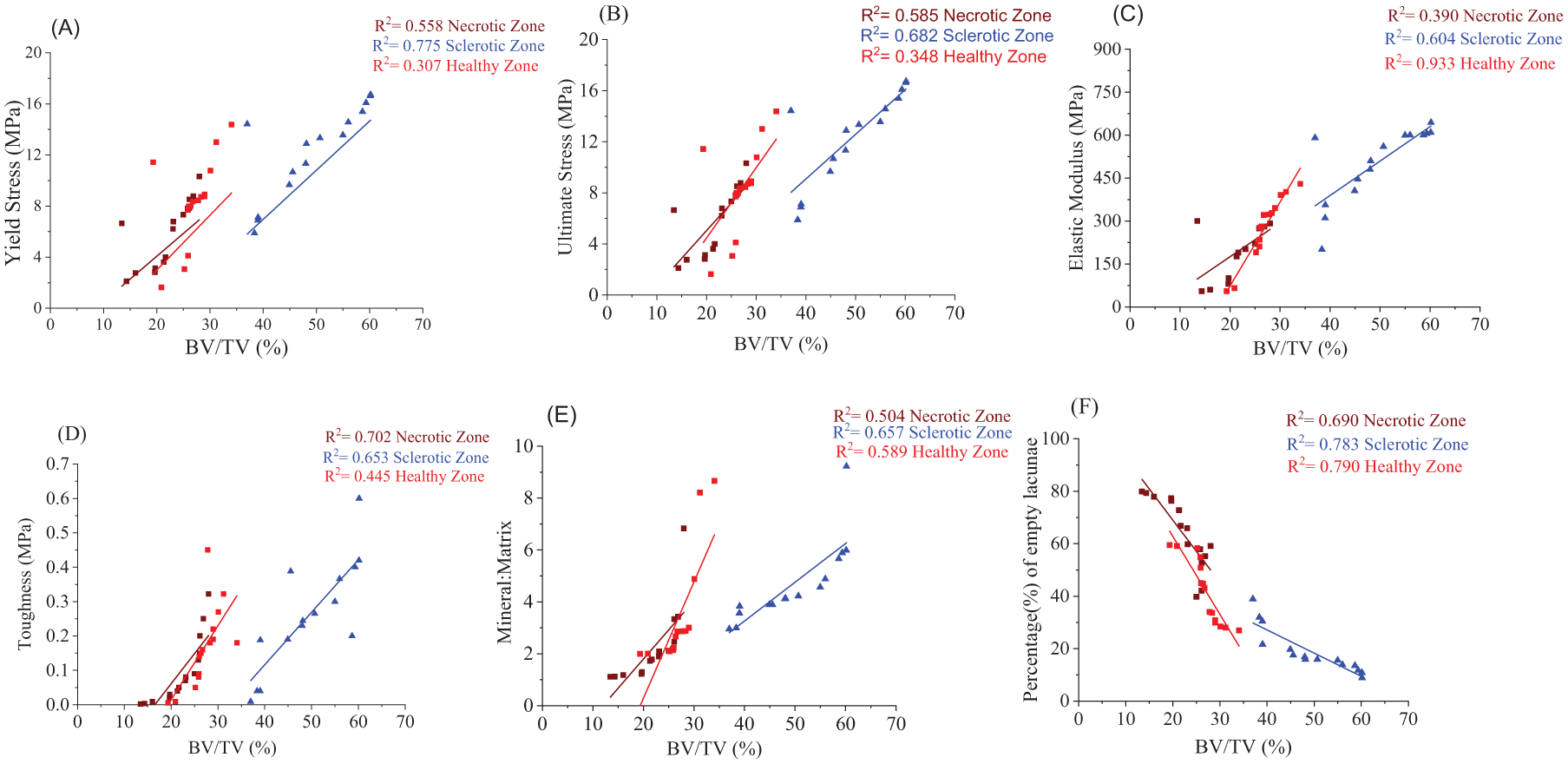
Linear regression analysis showing the relationships between bone volume fraction (BV/TV) and biomechanical and compositional parameters in necrotic, sclerotic, and healthy zones of osteonecrotic femoral heads. (a) Yield stress, (b) Ultimate stress, (c) Elastic modulus, (d) Toughness, (e) Mineral-to-matrix ratio, and (f) Percentage of empty lacunae plotted against BV/TV as a covariate. Regression lines represent zone-specific correlations, with corresponding coefficients of determination (R2) indicated in each panel.
Even though the stress gradients could not be directly measured, the identified structure-composition-mechanics discrepancies may offer mechanistic evidence of the predictions of failure at the necrotic-sclerotic interface using finite elements.8–10 This study demonstrates that multiscale comparison of necrotic, sclerotic, and preserved regions within the same femoral head may provide important insight into how zonal heterogeneity, rather than necrosis alone, influences mechanical stability. The findings suggest that the risk of femoral head collapse may be governed by the mechanical interaction between compliant necrotic tissue and the relatively stiffer surrounding regions, highlighting the potential value of patient-specific surgical planning. Furthermore, recognising the fragile nature of the sclerotic rim and its interaction with the necrotic core may improve prognostic assessment and support more targeted treatment strategies for osteonecrosis of the femoral head.
This study has a number of limitations to be considered. First, the relatively small sample size (n = 15) and the large number of outcome measures can result in a limitation of statistical power despite using statistical correction to control the multiple comparisons. Secondly, since all specimens were collected in patients who underwent THA, the results mainly represent structural and mechanical features of osteonecrosis at an advanced stage and may not accurately represent the earlier stages of the disease. Third, as zonal identification was done through both combined macroscopic examination and micro-CT guidance, regional delineation can still be affected by local heterogeneity in the femoral head. Fourth, since samples across different zones were taken in the same femur head, a repeated-measures statistical system was used to compensate intra-patient dependency. Lastly, although the findings indicate the mechanical heterogeneity among zones, redistribution of stress across the necrotic-sclerotic interface was not directly measured; hence, mechanistic conclusions are inductive.
Conclusion
This study demonstrates pronounced zonal heterogeneity in microarchitecture, composition, and mechanical behavior within osteonecrotic femoral heads. The necrotic zone showed severe structural deterioration, reduced mineralisation, compromised mechanical strength, and extensive osteocyte loss, resulting in diminished load-bearing capacity. In contrast, the sclerotic zone exhibited increased trabecular thickness and stiffness but reduced post-yield deformation, indicating a stiff yet potentially brittle phenotype. This discordance between adjacent regions highlights a mechanical imbalance within the femoral head. Together, these zone-specific alterations provide insight into the structural basis of femoral head failure in osteonecrosis.
Footnotes
Acknowledgements
The authors highly acknowledge IIT Ropar, Max Superspeciality Hospital for providing the necessary infrastructure and facilities used in the current research. The authors would also like to acknowledge Mohd. Waqar Khan and Raja Dewangan for their help in experiments and intellectual discussion during data analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.