
Abstract
Background:
Short-stem total hip arthroplasty (THA) aims to preserve proximal femoral bone stock and promote physiological load transfer compared to conventional cementless stems. This design is particularly relevant for younger, active patients, in whom long-term implant survival and bone preservation are critical.
Objective:
To systematically review and meta-analyse the functional and radiological outcomes of short-stem THA in young patients.
Methods:
A systematic search of Medline, Embase, PubMed, and the Cochrane Library was conducted to May 2025 following PRISMA guidelines. Eligible studies included patients with mean age <55 years and ⩾4.5 years mean follow-up. Primary outcome was Harris Hip Score (HHS) or modified Harris Hip score (mHHS); secondary outcomes were complications, survivorship, and radiological findings.
Results:
32 studies involving 4082 hips (mean age 46.7 years, mean follow-up 8.6 years) were included. Mean HHS improved from 45.3 to 93.8. Complications were infrequent, including intraoperative fracture (1.6%), dislocation (0.6%), and infection (0.4%). Radiological changes, including osteolysis (1.3%), heterotopic ossification (1.9%), and stem subsidence ⩾2 mm (0.7%), were uncommon. Stem survivorship free from aseptic loosening was 99.7%. The overall revision rate was 1.6%. Subgroup analyses indicated better outcomes and lower revision rates with posterolateral approaches and ceramic-on-ceramic bearings.
Conclusions:
Short-stem total hip arthroplasty in patients younger than 55 years appears to be associated with excellent mid- to long-term functional outcomes, low complication rates, and high implant survivorship. While these findings suggest that short stems are a safe and durable option for young, active patients, substantial heterogeneity across studies and the limited randomised evidence warrant cautious interpretation. These findings are hypothesis-generating and warrant confirmation in adequately powered prospective studies.
PROSPERO registration:
No: CRD420251046310
Keywords
Introduction
Despite the success of uncemented femoral stems in the younger more active population, potential issues of proximal stress shielding can arise due to alterations in load transfer of the proximal femur. 1 Stress shielding, characterised by the demineralisation of surrounding bone and peri-prosthetic bone loss, can contribute to implant loosening, thigh pain, and an increased risk of peri-prosthetic fracture. Associated bone loss in the context of revision surgery creates further potential challenges.2,3
In their prospective cohort, Liang et al. 4 reported approximately 8% bone mineral density (BMD) loss in Gruen zone 7 for short stems versus 18% for conventional stems. Similarly, in their meta-analysis of 9 randomised controlled trials, Zhang et al. 5 found that short stems demonstrated 10–15% less BMD loss in zones 1 and 7 compared with conventional stems. Moreover, Yan et al. 6 concluded that short stem designs feature a clearly favorable pattern in terms of a lower reduction proximally and improved metaphyseal loading in comparison to the conventional stems. Collectively, these studies confirm that metaphyseal-fitting short stems substantially mitigate proximal stress shielding and preserve femoral bone stock. These properties are particularly advantageous for younger or active patients who may require future revision surgery. However, it remains unclear whether this preservation of proximal bone stock translates into improved outcomes at revision.
Although no exact definition of short stem exists, these prostheses are characterised by their fixation principles and the location of proximal loading. Short stems are broadly characterised by lengths that are shorter than conventional or standard femoral stems (Figures 1 and 2). 7
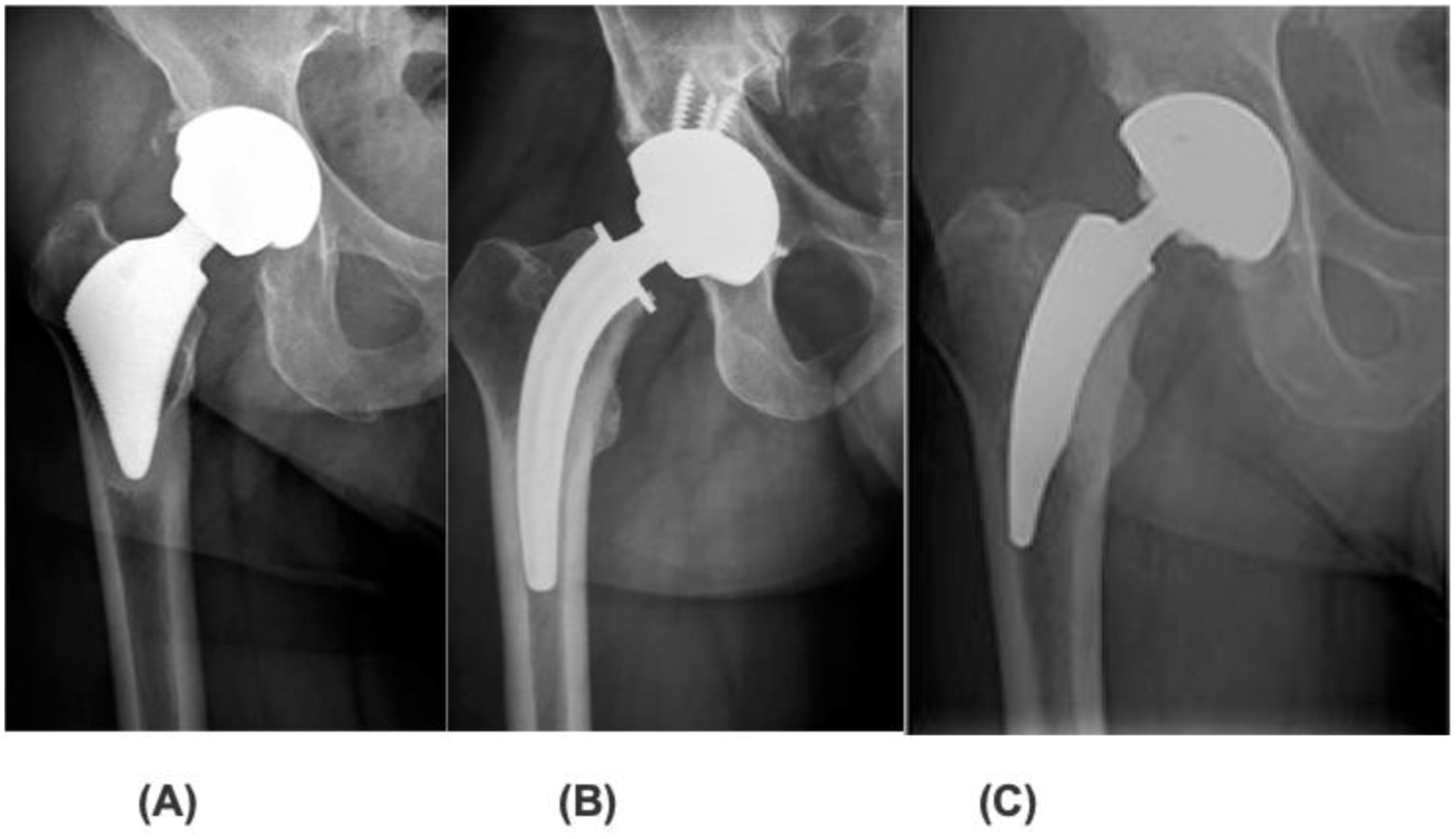
Examples of short stem designs (a) Proxima stem, (b) CFP stem, (c) NANOS stem. Reproduced from Loppini M and Grappiolo G 1 .
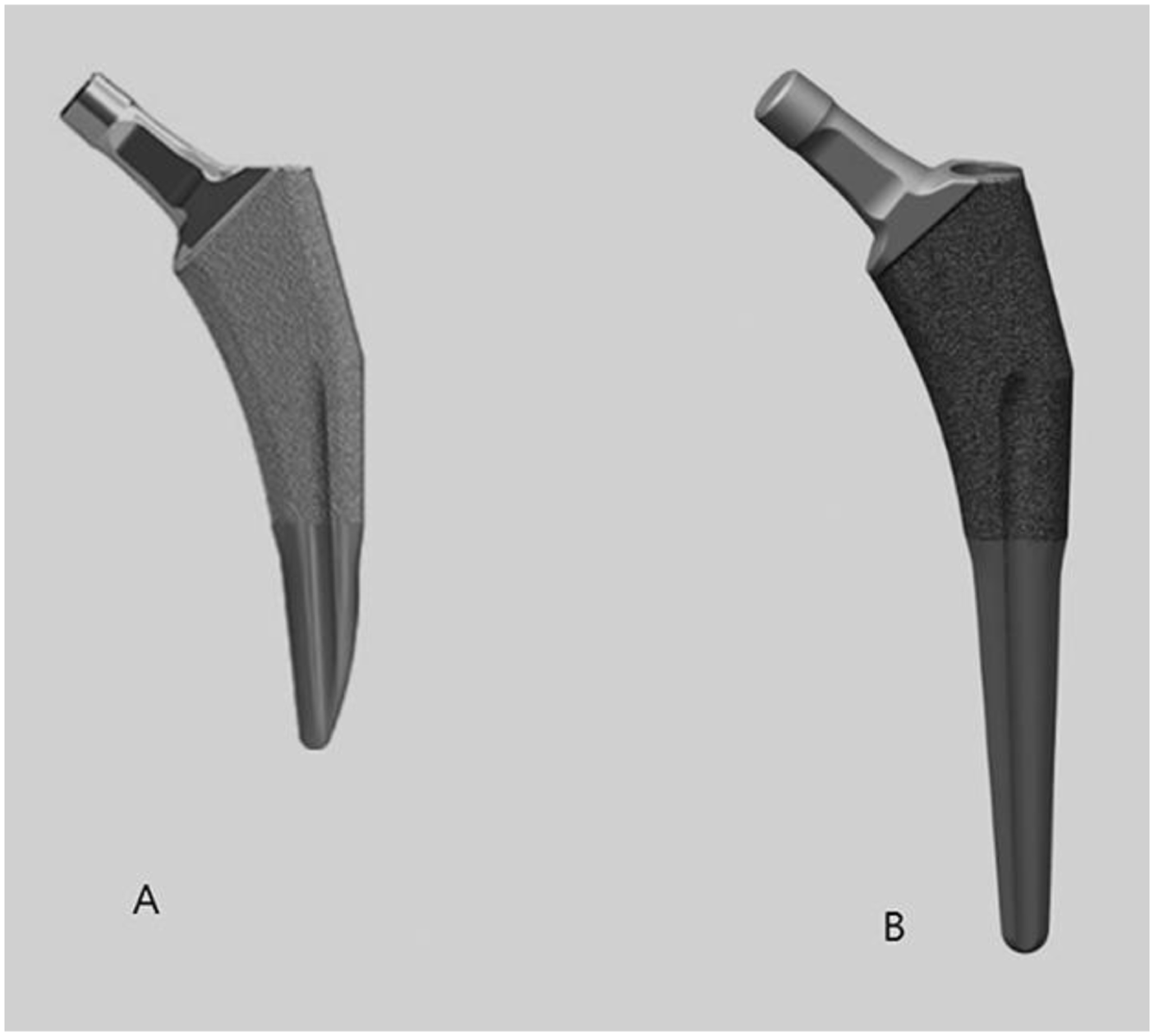
(a) the TaperLoc® Microplasty stem (Zimmer Biomet, Warsaw, IN, USA) and (b) the standard TaperLoc stem. The Microplasty stem is 35 mm shorter than the standard stem. Reproduced from Won et al. 7
While there’s no single strict cut-off, many definitions consider stems less than 120 mm as short. 8 However, some short stem designs reported in the literature exceed 120 mm, reflecting the wide variety of designs.4,9
Gulow et al. 10 divided femoral stems into 4 types according to the different anchoring principles, including resurfacing endoprosthesis anchoring on the epiphysis; collum endoprostheses solely anchoring on the metaphysis; short collum-preserving stems anchoring on the metaphysis with short anchorage on the diaphysis, and conventional stems anchoring in metaphysis and extending deeply into the diaphysis.
Khanuja et al. 11 classified short stems according to fixation principles and location of proximal loading. The authors distinguished 4 categories: femoral neck fixation; calcar loading; lateral flare and calcar loading; and shortened tapered stems. In this classification system, resurfacing was not included. 11
Van Oldenrijk et al. 12 classified short stems into 3 categories: (1) Collum Stems: ultra-short stems, with complete anchorage in the femoral neck with no diaphyseal contact; (2) Partial Collum Stems: curved designs that preserve part of the femoral neck, with some metaphyseal fixation and limited diaphyseal support; and (3) Trochanter-Sparing Stems: trochanter-sparing but not neck-sparing, with a shortened tapered stem (Figure 3).12,13
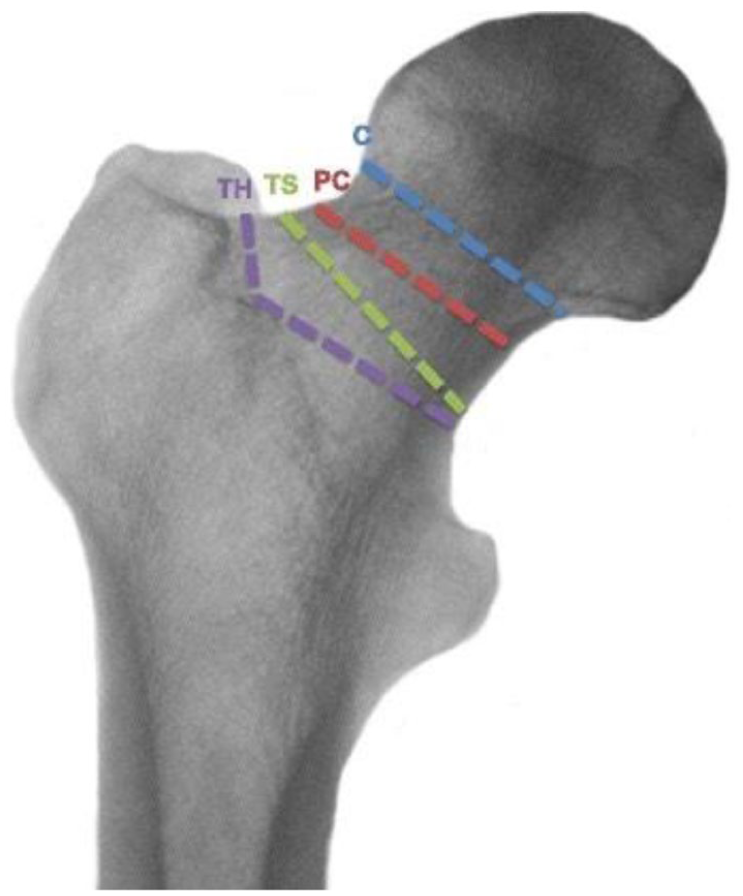
Osteotomy levels of the different stem types (collum (C), partial collum (PC), trochanter sparing (TS), and trochanter harming (TH). Reproduced from Burchard et al. 13
Previous systematic reviews have shown excellent clinical results with short stem total hip arthroplasty, yet the results have been limited by relatively small inclusion numbers, short follow-up and broad inclusion criteria yet show similar survival rates and clinical outcomes.4,8
Aim of the study
The objective of our study is to conduct a systematic review and meta-analysis of the mid- to long-term functional and radiological outcomes of short stem designs in patients younger than 55 years.
Methods
A systematic review following Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines was undertaken. 14 We used the classification system used by van Oldenrijk et al. 12 in their comprehensive review, which classifies the short stem per the level of the neck resection into Collum, Partial Collum and Trochanteric Sparing. Details of the protocol for this systematic review were prospectively registered on PROSPERO (ID: CRD420251046310). 15
Search strategy and data extraction
A systematic literature search was conducted using key words; ‘total hip replacement/arthroplasty’, ‘short stem prosthesis’, ‘functional’, ‘Harris Hip Score/HHS’ in various combinations. The search was limited to English, French, German and Dutch languages. All clinical studies published in Medline, Embase, PubMed and the Cochrane Library Database from inception until May 2025 were included. Results from the database searches were collated and duplicates removed. Papers were screened using study title and abstract and inclusion/exclusion criteria to assess suitable papers for inclusion. Full text papers were reviewed for inclusion and citations screened to identify any additional studies. The data were extracted into the Excel sheet before analysis. To minimise bias, data were blindly extracted by 2 authors (MB and VV) independently using a purpose designed proforma. Disagreements were resolved by discussion with a senior author (TL).
Participants and study criteria
The eligibility criteria to include the studies were: full text clinical trial or case series of primary clinical or radiographic outcomes. short stem THA in patients with average age ⩽ 55 years, minimum average follow-up ⩾ 4.5 years, and reported clinical outcome score (Harris Hip Score [HHS] or modified Harris Hip Score [mHHS]). The studies with custom/Collum/Extramedullary anchorage prosthesis were excluded. We also excluded case reports, biomechanical studies, in vitro studies, and studies failing to specify post-operative clinical or radiographic outcomes. The age threshold (<55 years) was chosen because the majority of the studies evaluating the outcomes of short stem total hip replacements included patients around or less than this age. Also, younger patients represent a distinct demographic with higher activity levels, longer life expectancy, and greater revision risk. Evaluating outcomes in this group provides important insight into implant durability and bone preservation for long-term performance.
Variables
Study characteristics were extracted including: study design, period, country, number of hips and patients, age at operation, gender, diagnosis, surgical approach, stem type, and bearing surface. Study outcomes extracted include mean follow-up with range and standard deviation, mean preoperative HHS with range and standard deviation, HHS at last follow-up with range and standard deviation, radiological evidence of subsidence or loosening, survivorship and reported complications. Any missing standard deviations were calculated using the mean HHS and the range, using the method described by Wan et al. 16
Risk-of-bias assessment and study quality
The studies included in the analysis were assessed for bias within their methodology. Randomised control trials were assessed using the RoB2 tool (Revised Cochrane risk-of-bias tool for randomised trials). Non-randomised trials were assessed using the ROBINS-I tool (Risk of bias in non-randomised studies of interventions).17,18
Statistical methods
All data analysis was conducted using RStudio. Meta-analyses were performed to evaluate pooled Harris Hip Scores across subgroups. The inverse variance method was employed with outcomes expressed as mean differences (MD) and 95% confidence intervals (CI). Standard deviations (SD) were estimated using the method of Wan et al. 16 when not reported. Both common effect and random effects models were fitted. The restricted maximum-likelihood estimator calculated between-study variance (τ²), with confidence intervals derived using the Q-Profile method. The Hartung-Knapp adjustment was applied to random effects models to provide conservative confidence intervals. 19 Heterogeneity was assessed using the Q statistic (significance test), I² statistic (proportion of variation due to heterogeneity), and H statistic. Subgroup analyses compared outcomes between surgical approaches, stem types, and bearing surfaces, with between-group differences tested using the Q statistic. Forest plots visualised individual study effects and pooled estimates. Statistical significance was set at p < 0.05. Given substantial heterogeneity (I² > 90%), random effects model results were prioritised for interpretation as they better account for between-study variability
Results
Study selection
Out of 949 studies, a total of 570 potential studies were identified from the electronic databases after removing duplicates. Further 436 studies were excluded by reviewing their titles and abstracts. We then reviewed the remaining 134 full-text articles of which a further 102 studies were excluded. Finally, 32 studies were deemed suitable for inclusion following screening and assessment against all of our inclusion and exclusion criteria (Figure 4).
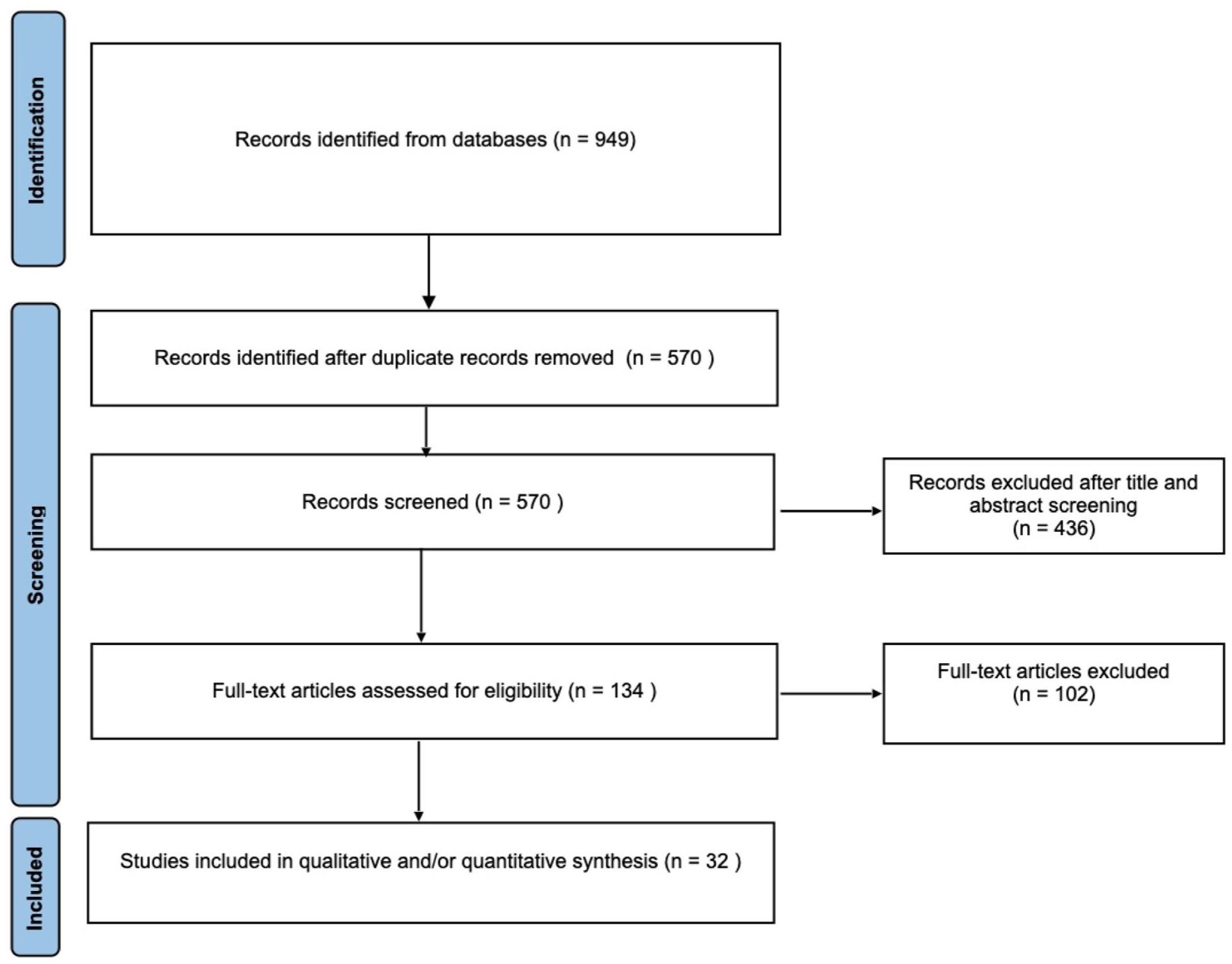
PRISMA flow chart of study selection.
Study and patient characteristics
32 studies (3 randomised controlled trials [RCTs], 29 observational) covering 4082 hips in 3438 patients (mean age 46.7 years) from 14 countries were included. 11 short-stem designs were reported, split equally between trochanteric-sparing and partial-collum approaches. The posterior approach was most common (59.4%), followed by anterolateral (31.3%) and anterior (3.1%). Ceramic-on-ceramic (CoC) was the predominant bearing surface (56.3%), with ceramic-on-polyethylene (CoP) (25.0%), metal-on-polyethylene (MoP) (21.9%), and metal-on-metal (MoM) (3.1%) also used. Study characteristics and primary indications are detailed in Tables 1 and 2.
Characteristics of the included studies including study design, patients’ demographics, stem type and classification, and bearing surfaces.
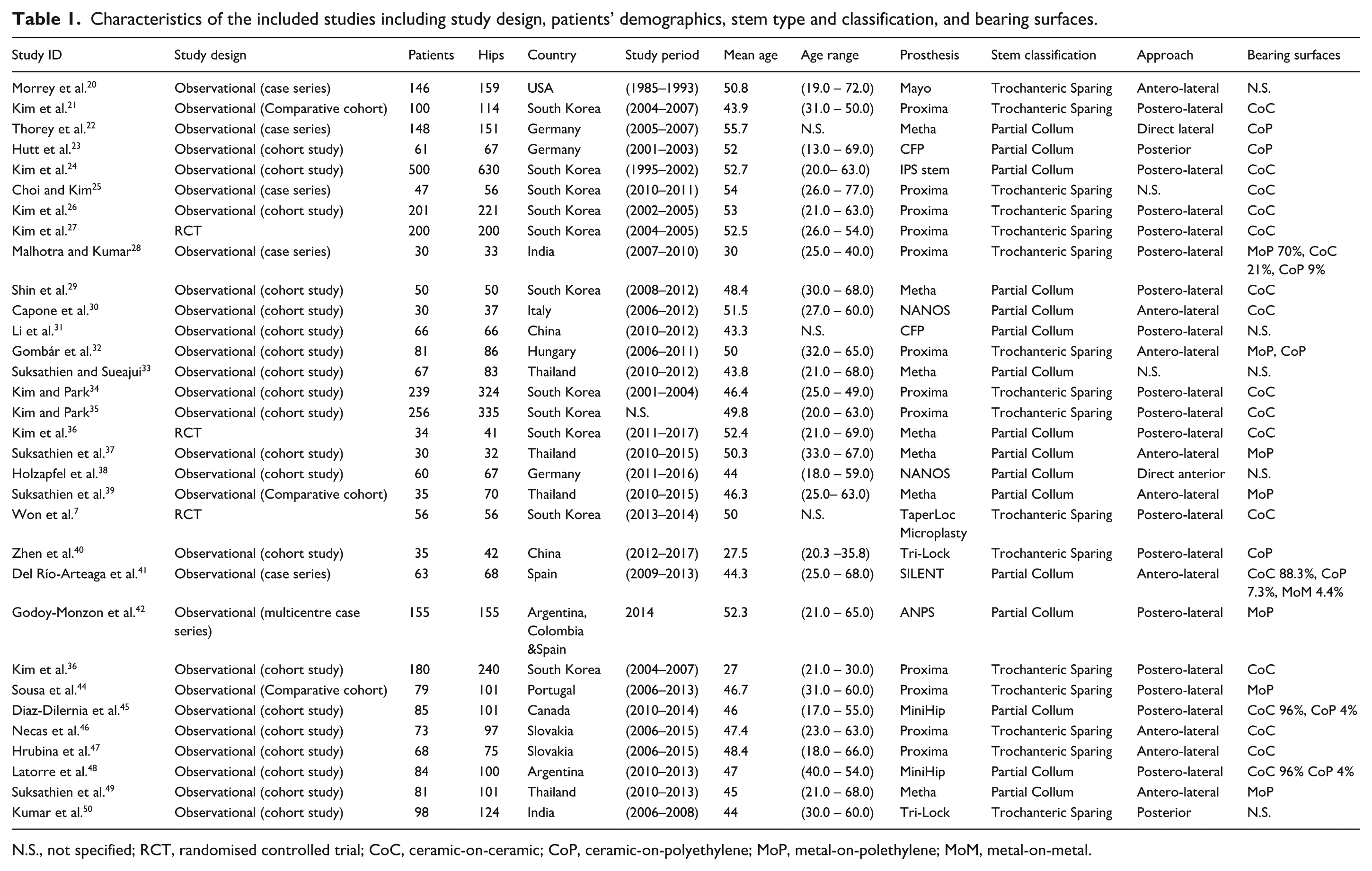
N.S., not specified; RCT, randomised controlled trial; CoC, ceramic-on-ceramic; CoP, ceramic-on-polyethylene; MoP, metal-on-polethylene; MoM, metal-on-metal.
Primary causes leading to hip replacement of the included studies.
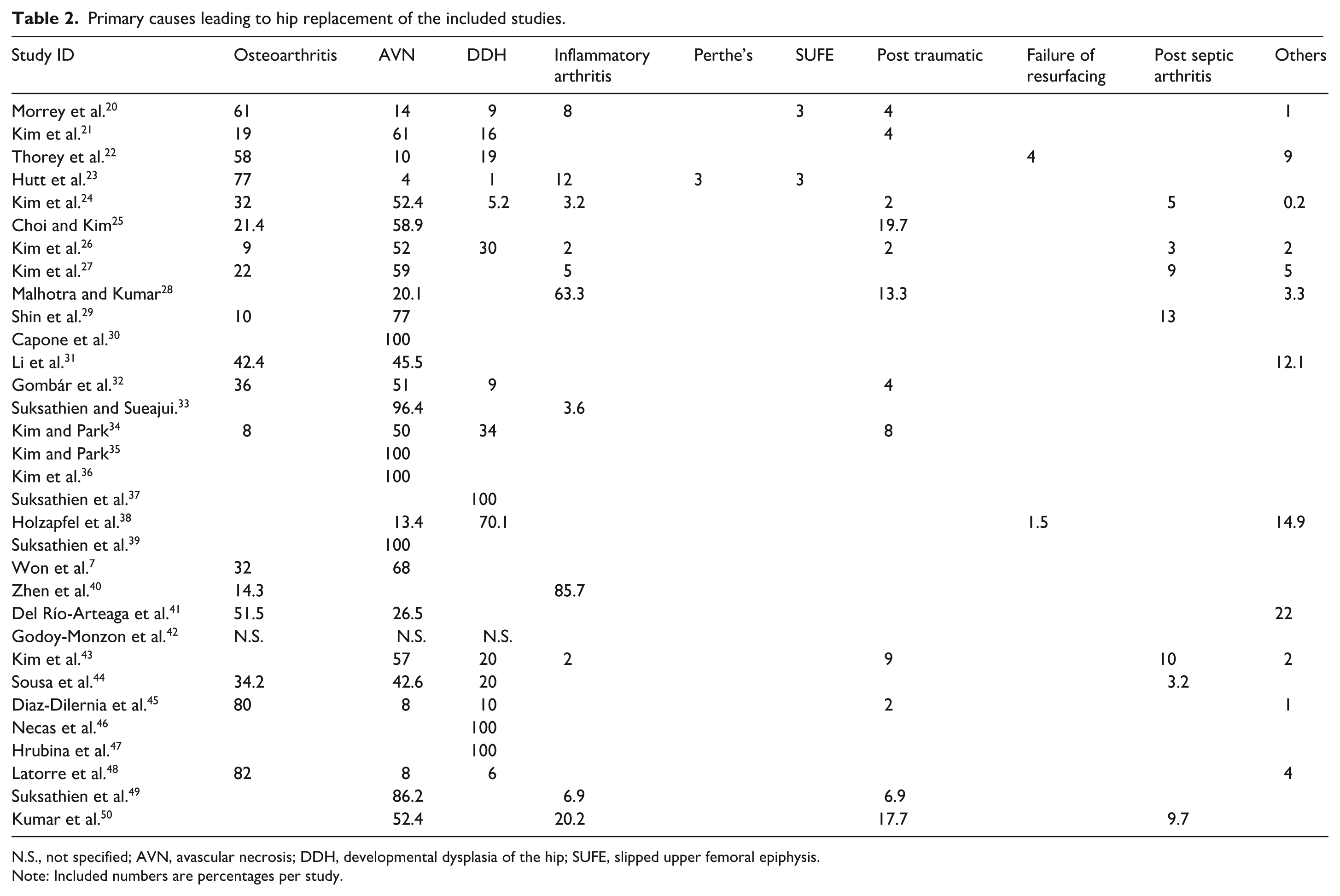
N.S., not specified; AVN, avascular necrosis; DDH, developmental dysplasia of the hip; SUFE, slipped upper femoral epiphysis.
Note: Included numbers are percentages per study.
The mean Harris Hip Score (HHS) improved from 45.3 preoperatively (range 19.7–66.3) to 93.8 postoperatively (range 87.0–99.6). The average follow-up was 8.6 years (range 4.6–15.8 years) (Table 3). Overall complication rates were low. Complication rates were low: intraoperative fractures occurred in 1.62% of hips, clicking in 4.29%, squeaking in 0.49%, dislocation in 0.61%, deep infection in 0.37%, and sciatic neuropraxia in 0.05%. The notable complications identified in relation to the length of follow-up were clicking and dislocation. The occurrence of clicking may reflect underreporting in earlier studies. Dislocation appears to be a plausible finding, potentially attributable to factors such as prosthetic wear or mechanical instability over time (Table 4).
Clinical outcomes and follow-up duration of the included studies.
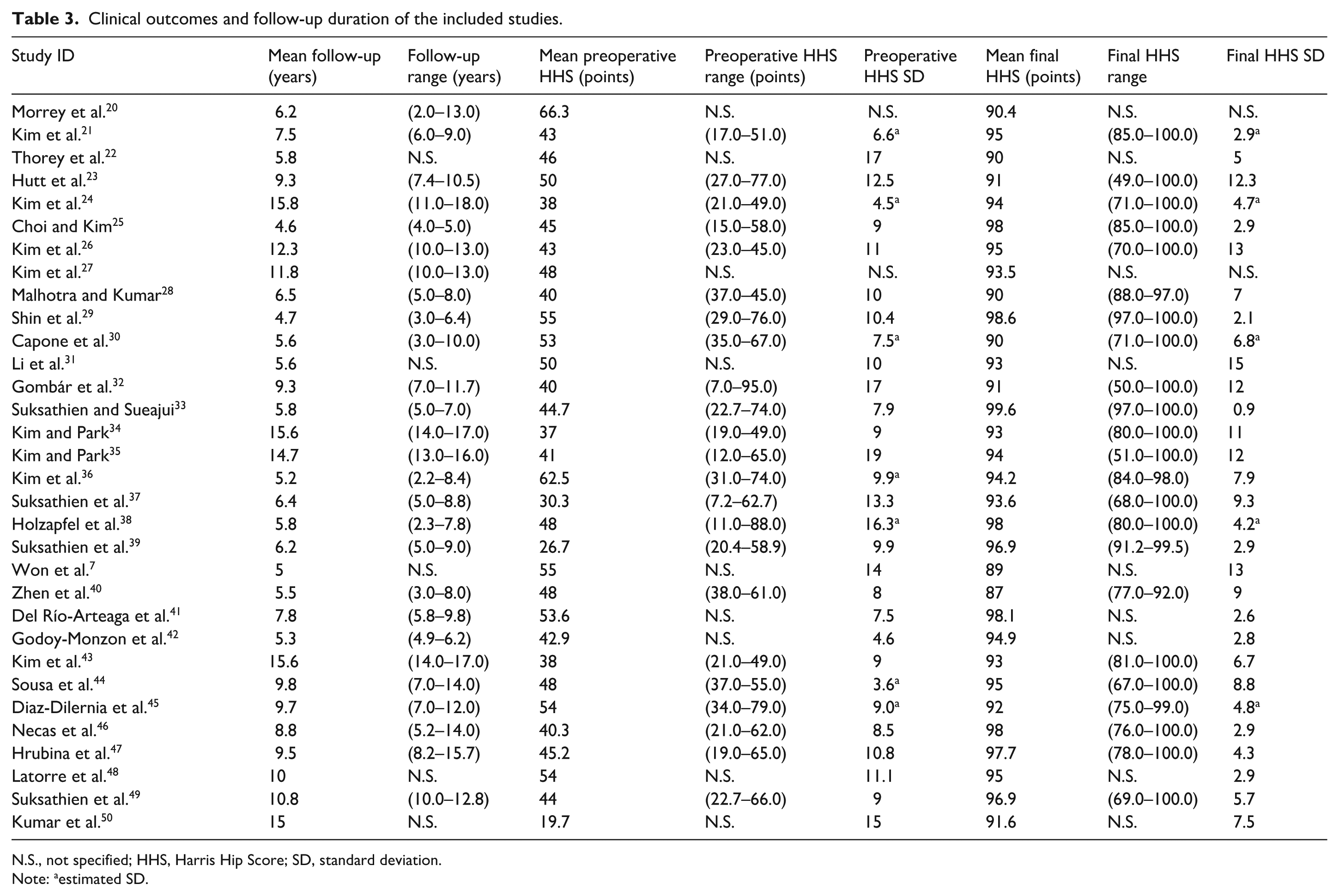
N.S., not specified; HHS, Harris Hip Score; SD, standard deviation.
Note: aestimated SD.
Postoperative complications of the included studies in relation to the length of follow-up.
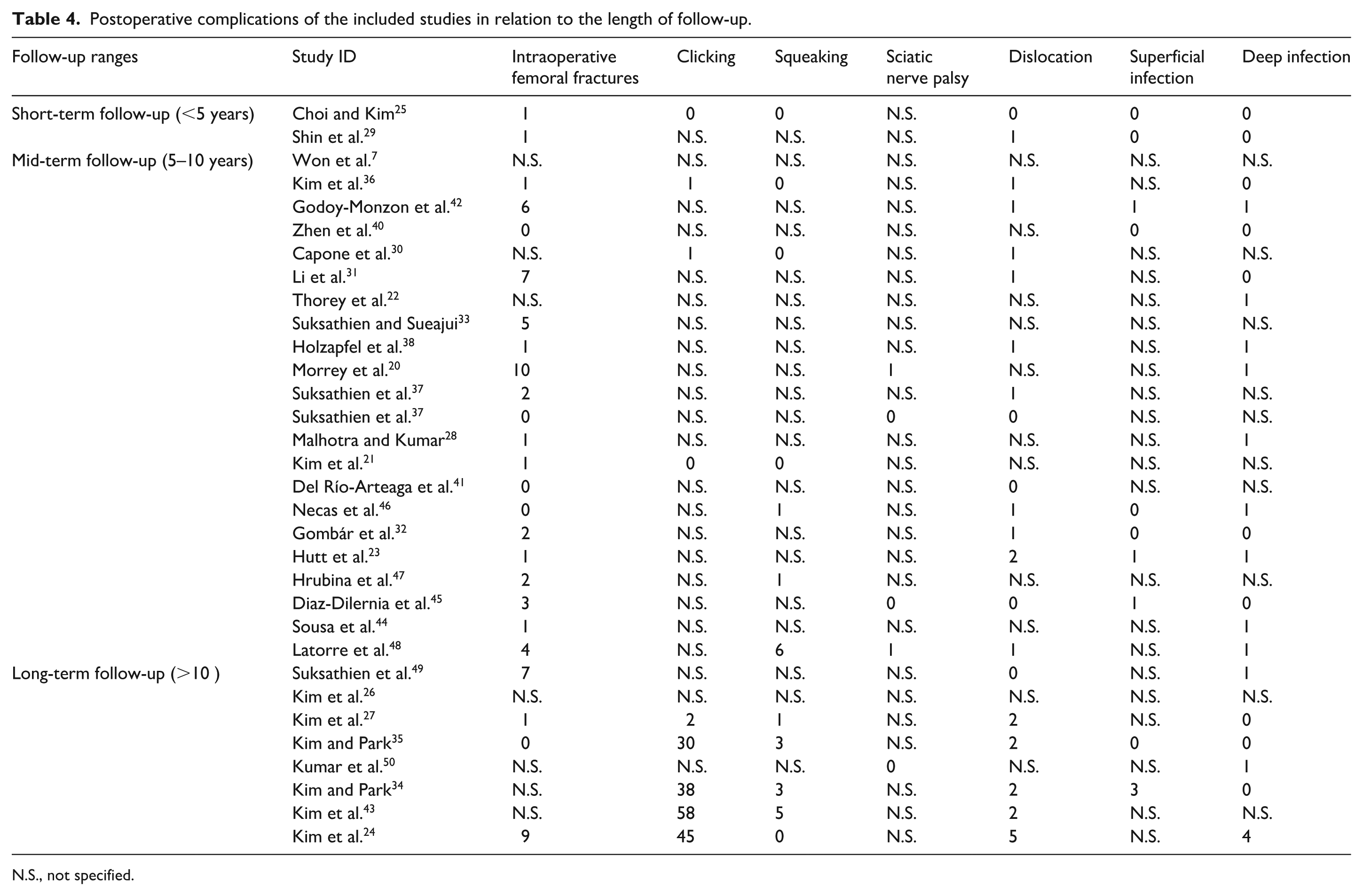
N.S., not specified.
Radiological findings were also positive. Heterotopic ossification was observed in 78 hips (1.91%). Osteolysis or radiolucent lines were noted around 55 stems (1.35%) and 22 cups (0.54%). Stem subsidence was reported in 111 hips (2.72%): 77 hips (1.89%) exhibited <2 mm subsidence, resulting in 4 revisions (0.10%), while 29 hips (0.71%) had ⩾2 mm subsidence, resulting in 6 revisions (0.15%) (Table 5).
Postoperative radiological parameters of the included studies.
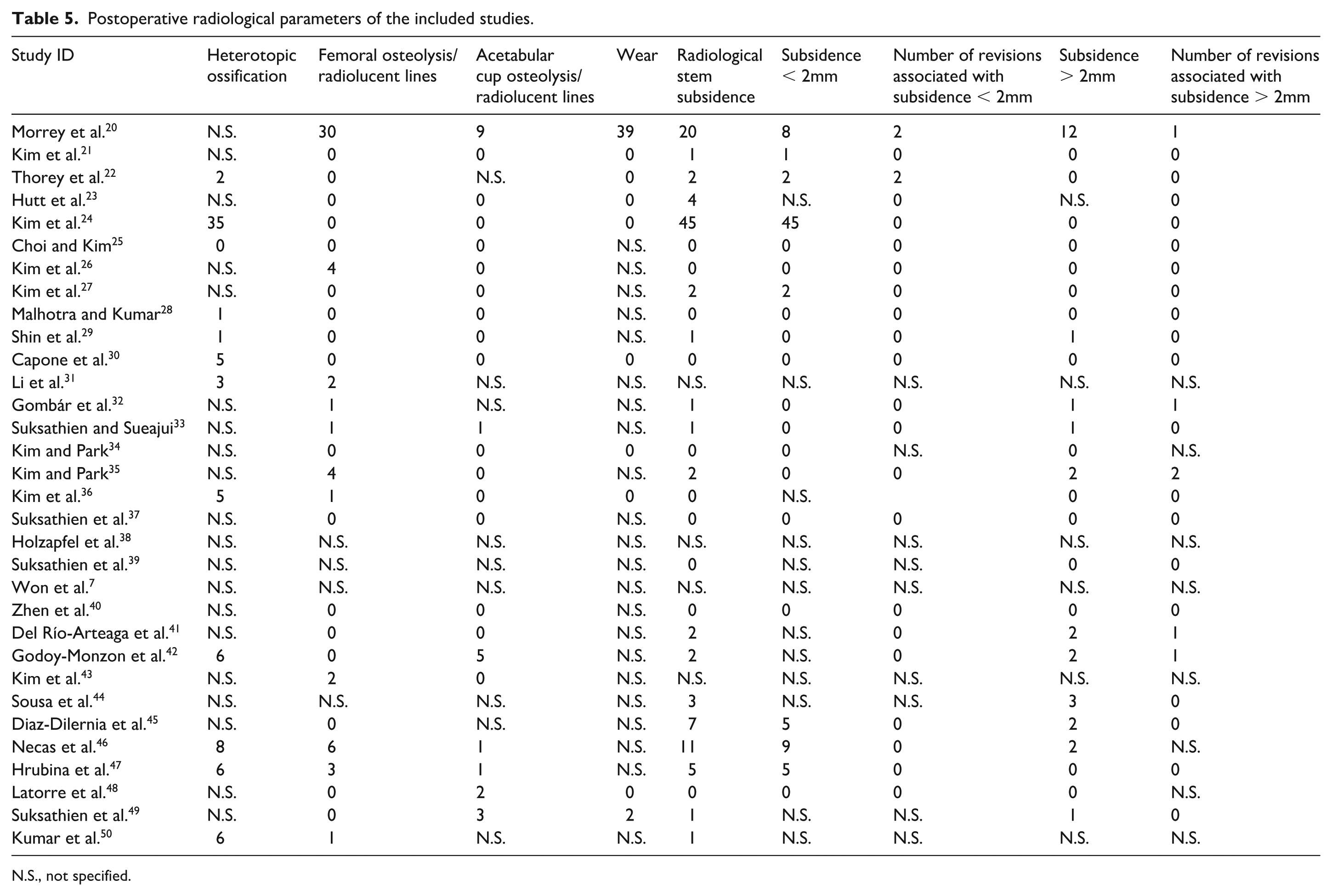
N.S., not specified.
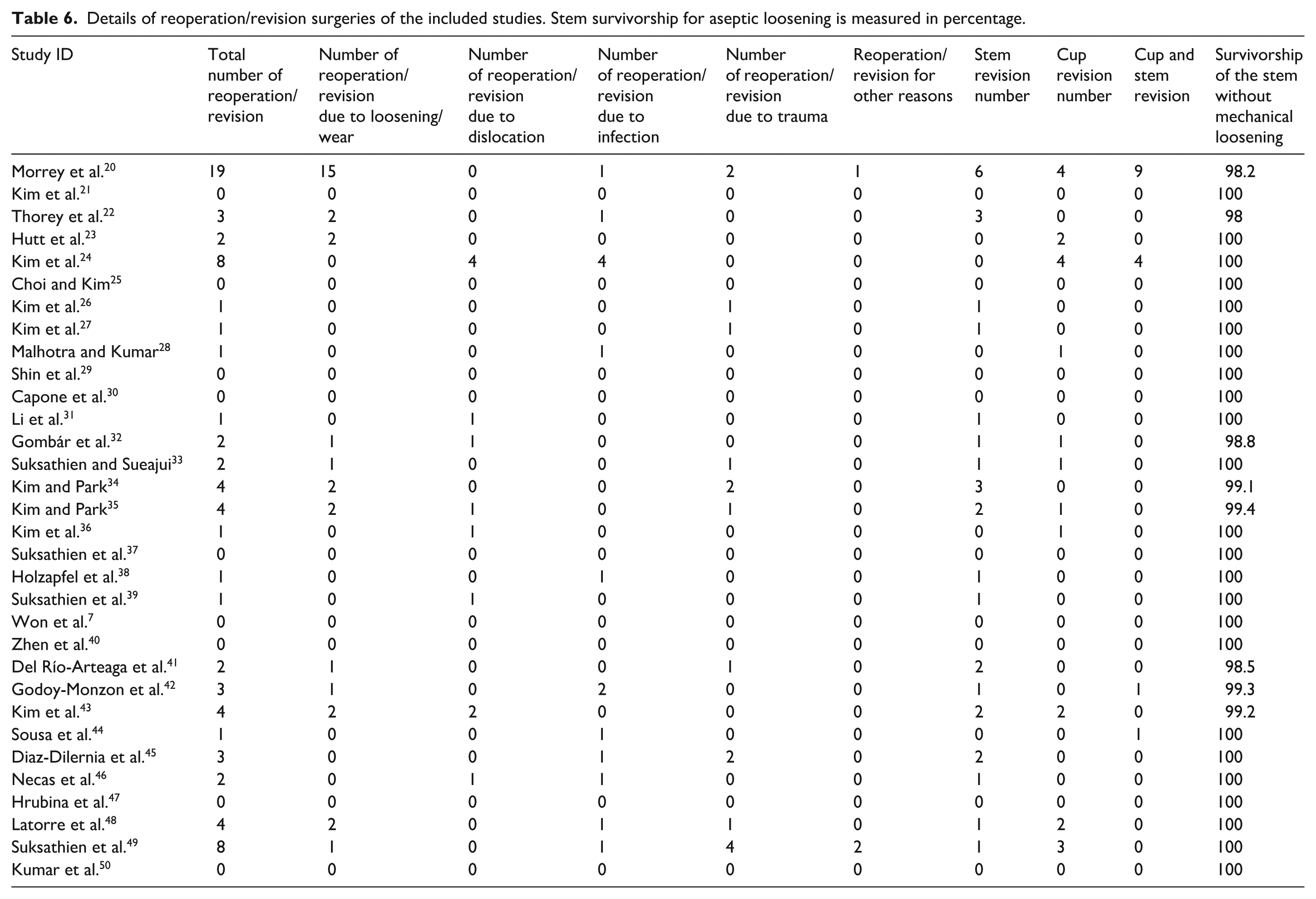
A total of 78 reoperations (1.91%) were recorded. The most common indications were aseptic loosening or wear in 32 hips (0.78%), infection in 15 hips (0.37%), periprosthetic trauma in 16 hips (0.39%), dislocation in 12 hips (0.29%), and other causes in 3 hips (0.07%). In total, 68 components (1.67%) were revised, including 31 stems (0.76%), 22 cups (0.54%), and 15 combined stem-and-cup revisions (0.37%). Stem survivorship free from aseptic loosening was 99.7% (Table 6).
Details of reoperation/revision surgeries of the included studies. Stem survivorship for aseptic loosening is measured in percentage.
Risk of bias and study quality
The included studies were assessed for their quality and risk of bias using the RoB 2 tool (for randomised trials) and the ROBINS-I tool (for non-randomised studies). Assessment demonstrated that none of the studies were judged to be at overall low risk of bias. The majority of studies showed mild or moderate risk of bias across several domains. A serious risk of bias was assessed in 14 studies in relation to confounding, in a single study in relation to missing data, and in 2 studies in relation to measurement of outcomes. In contrast, risks of bias related to selection of participants, classification of interventions, deviations from intended interventions, and selection of the reported results were generally judged to be low. Overall, the evidence base was limited by the presence of moderate to serious risks of bias, which should be taken into account when interpreting the findings of this review (Figure 5).
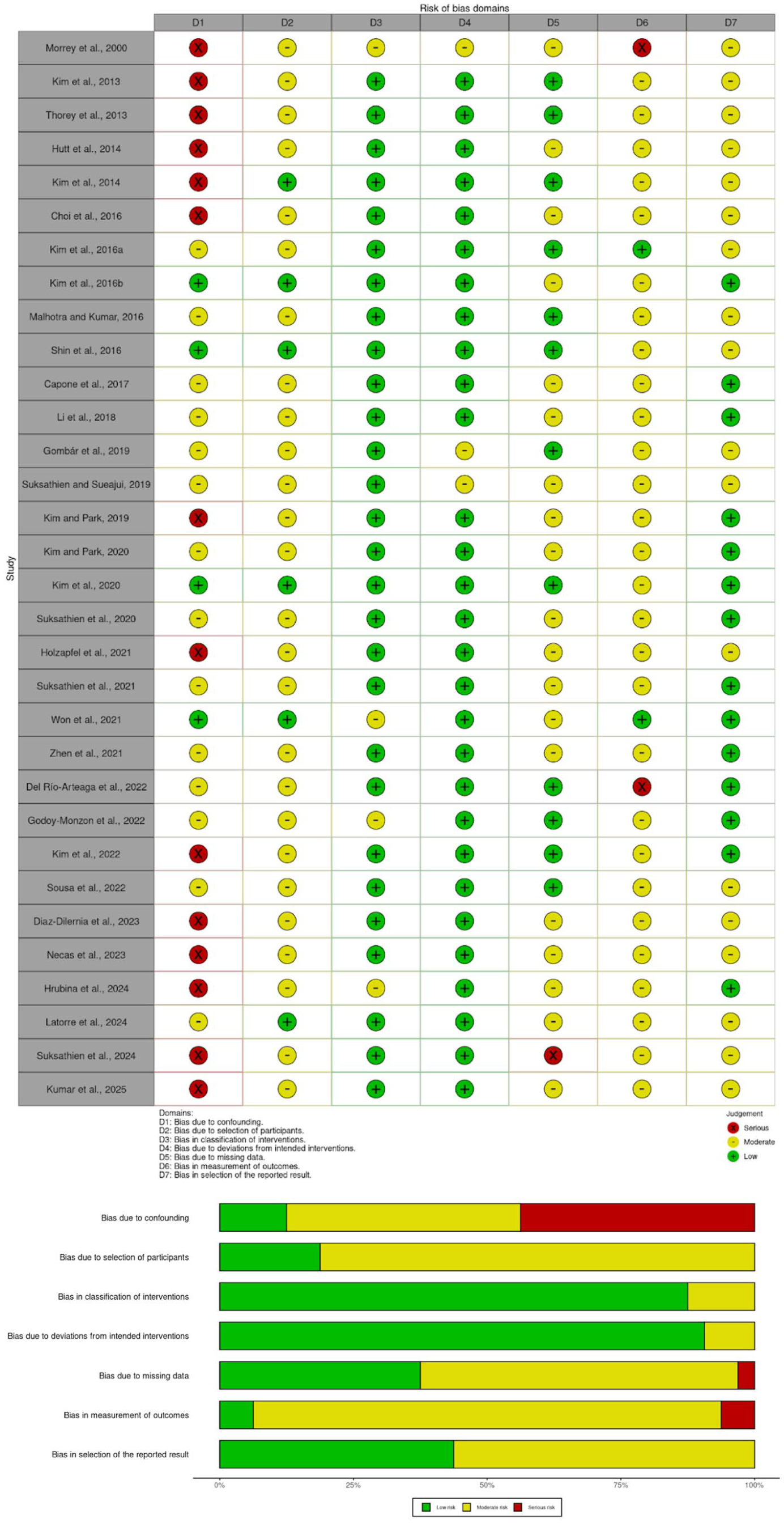
Risk of bias domains.
Surgical approach
26 studies were included in the meta-analysis, comprising 8 studies (30.8%) utilising the antero-lateral approach and 18 studies (69.2%) employing posterior approaches. The overall pooled Harris Hip Score demonstrated excellent clinical outcomes across all approaches (random effects model: 93.9%; 95% CI, 92.7–95.1%). Substantial heterogeneity was observed among studies (I² = 96.0%, 95% CI, 95.0–96.8%; τ² = 7.81, 95% CI, 4.54–16.06; Q = 629.99, p < 0.0001), necessitating the use of a random effects model. Subgroup analysis revealed that studies using the antero-lateral approach achieved marginally higher HHS scores (95.5%; 95% CI, 92.8–98.2%) compared to those using posterior approaches (93.3%; 95% CI, 92.0–94.6%). However, this difference was not statistically significant in the random effects model (Q = 2.81, p = 0.094), with overlapping confidence intervals suggesting that the apparent advantage of the antero-lateral approach may be influenced by study heterogeneity. Both approach groups demonstrated considerable within-group heterogeneity (antero-lateral: I² = 91.8%; posterior: I² = 94.8%), indicating that factors beyond surgical approach likely contribute to variability in clinical outcomes (Figure 6).
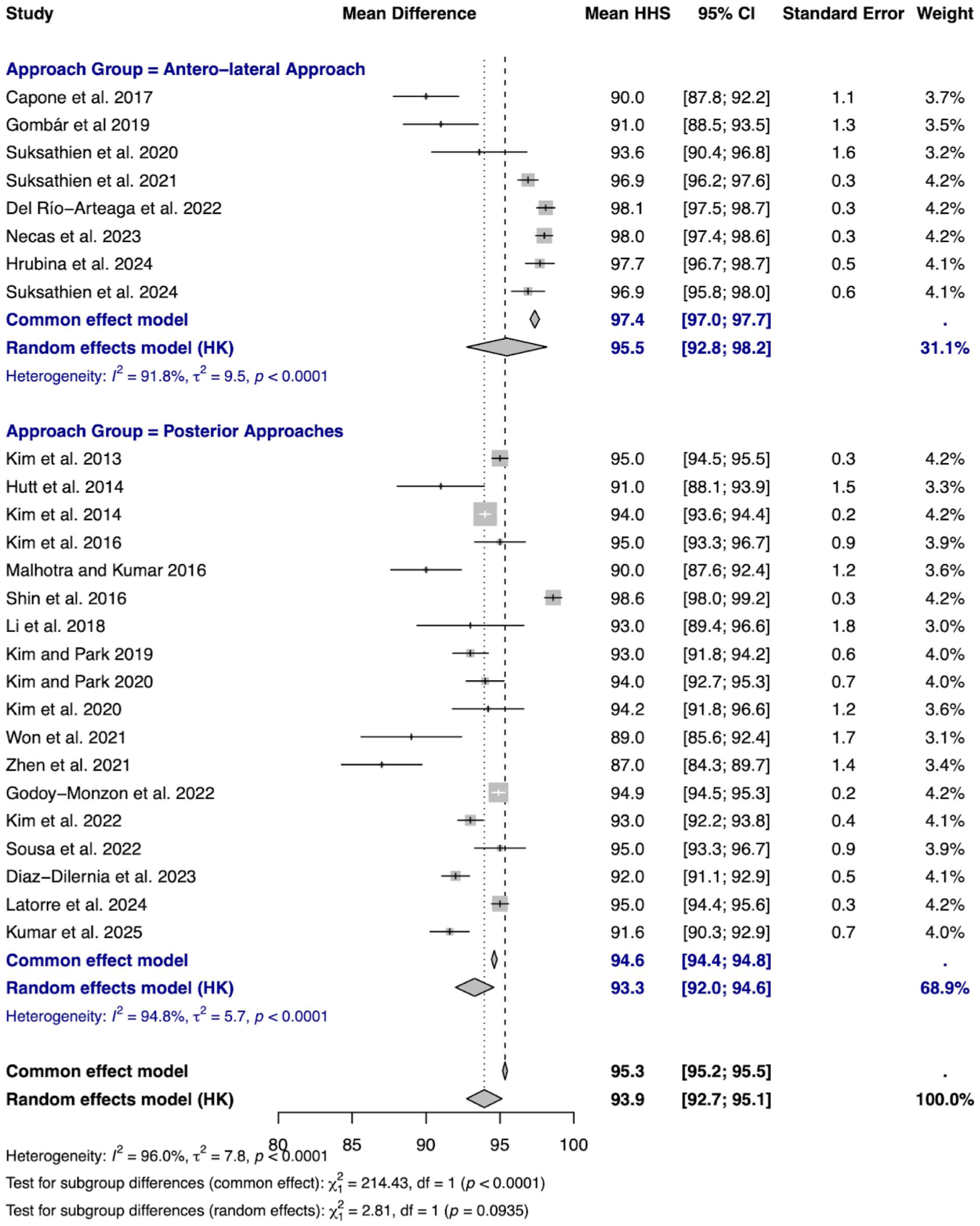
Meta-analysis of the anterolateral and posterior surgical approaches with HHS.
Stem design
30 studies were included in the stem classification meta-analysis, with 14 studies (46.7%) evaluating trochanteric sparing stems and 16 studies (53.3%) examining partial collum stems. The pooled Harris Hip Score across all stem types demonstrated excellent clinical outcomes (random effects model: 94.3%; 95% CI, 93.1–95.5%). Exceptionally high heterogeneity was identified among studies (I² = 98.6%, 95% CI, 98.3–98.8%; τ² = 9.53, 95% CI, 5.82–18.11; Q = 2029.24, p < 0.0001), indicating substantial variability in reported outcomes. Subgroup analysis using the random effects model showed that partial collum stems achieved marginally higher HHS scores (94.9%; 95% CI, 93.2–96.5%) compared to trochanteric sparing stems (93.6%; 95% CI, 91.6–95.5%), although this difference did not reach statistical significance (p = 0.268). Both stem classifications demonstrated extremely high within-group heterogeneity (trochanteric sparing: I² = 95.8%; partial collum: I² = 99.1%), suggesting that factors beyond stem design significantly influence clinical outcomes. The confidence intervals for both stem types overlapped considerably, indicating that the choice between these implant designs may have minimal impact on functional outcomes when accounting for study heterogeneity (Figure 7).
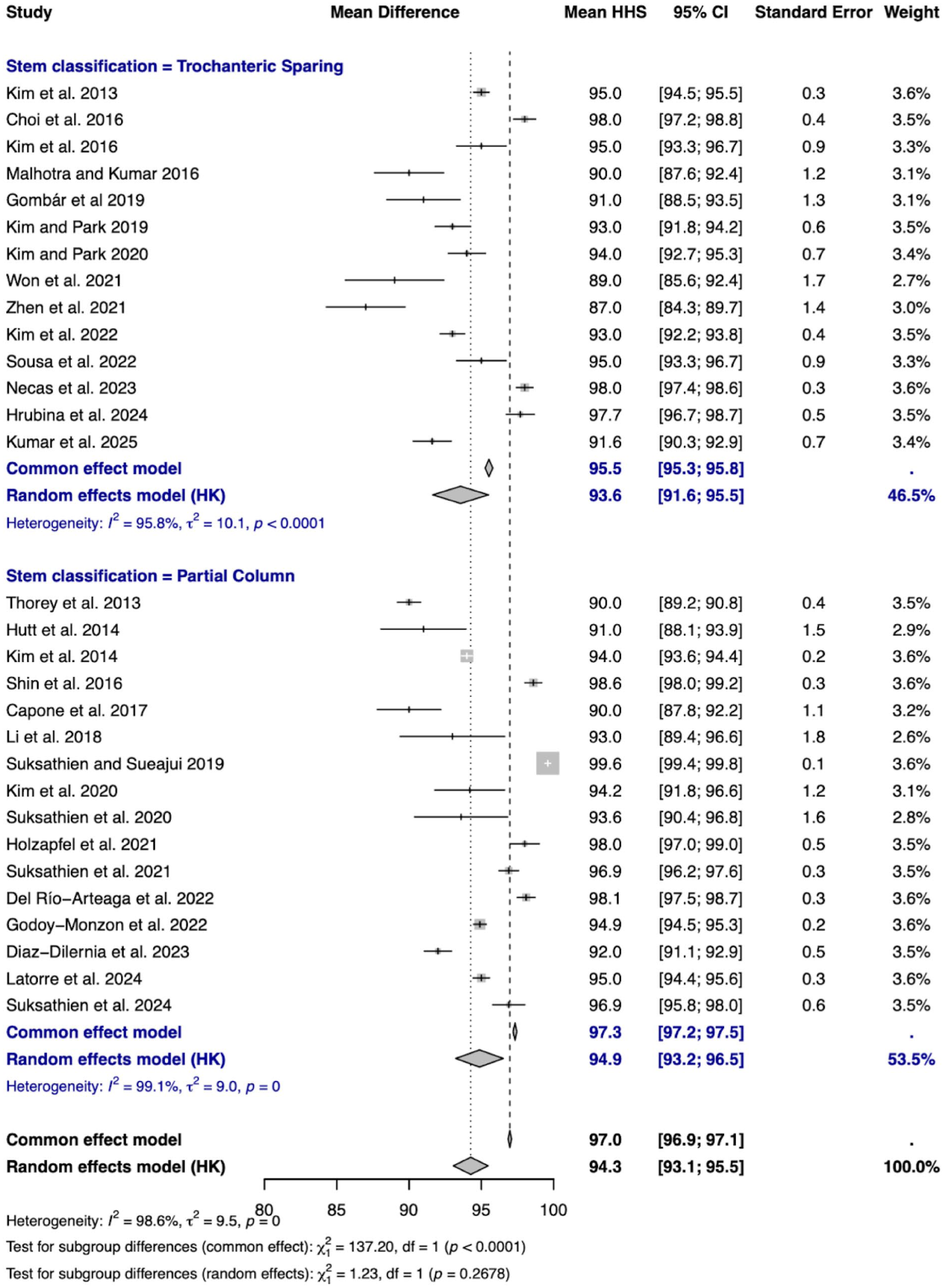
Meta-analysis of the stem classification and HHS.
Bearing surface
19 studies were included in the bearing surface meta-analysis, comprising thirteen studies (68.4%) examining CoC bearings, 1 study (5.3%) evaluating CoP, and 5 studies (26.3%) investigating MoP articulations. The pooled Harris Hip Score across all bearing surfaces demonstrated excellent clinical outcomes (random effects model: 94.7%; 95% CI, 93.4–96.0%). High heterogeneity was observed among studies (I² = 97.1%, 95% CI 96.3–97.7%; τ² = 6.80, 95% CI, 3.69–16.16; Q = 615.03, p < 0.0001). Subgroup analysis revealed statistically significant differences between bearing surfaces in both fixed and random effects models (Q = 77.81, p < 0.0001). MoP bearings achieved the highest scores (95.8%; 95% CI, 94.2–97.3%), followed by CoC bearings (94.8%; 95% CI, 93.0–96.5%), while CoP demonstrated significantly lower outcomes (90.0%; 95% CI, 89.2–90.8%), though this finding was based on a single study. Within-group heterogeneity remained high for both CoC (I² = 97.0%) and MoP (I² = 87.1%) bearings. The substantial and statistically significant differences between bearing surfaces, which persisted in the random effects model, suggest that bearing selection may have a meaningful impact on functional outcomes, although the limited representation of CoP bearings warrants cautious interpretation of its inferior performance (Figure 8).
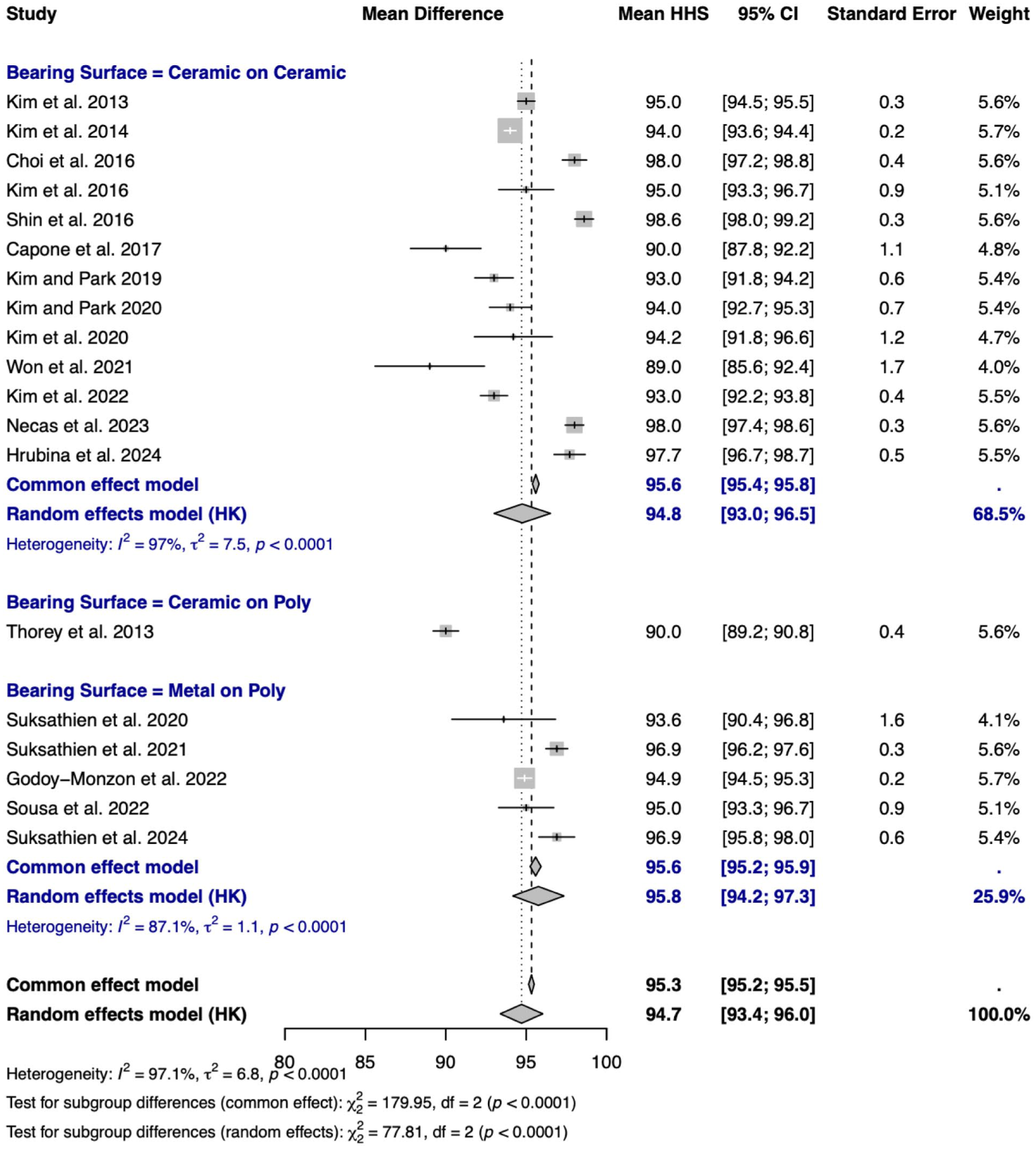
Meta-analysis of bearing surfaces and HHS.
Only 4 studies included the type of poly liner: Suksathien et al.33,37 reported the use of Vitelene, Vit E-Stabilized Highly Cross-linked Polyethylene (B.Braun Aesculap, Tuttlingen, Germany), Godoy-Monzon et al. 42 reported the use of GXL polyethylene liner with a 10° posterior elevated rim, and Suksathien et al. 49 reported the use of conventional ultra-high molecular weight polyethylene liner (Plamacup SC liner, B.Braun Aesculap). We did not directly compare the different types of poly.
Complications
A total of 32 studies including 4082 hips were analysed across surgical approaches, stem classifications, and bearing surfaces to identify complications (Table 7).
Pooled complication rate per category (Surgical approach, stem design, and bearing surface).
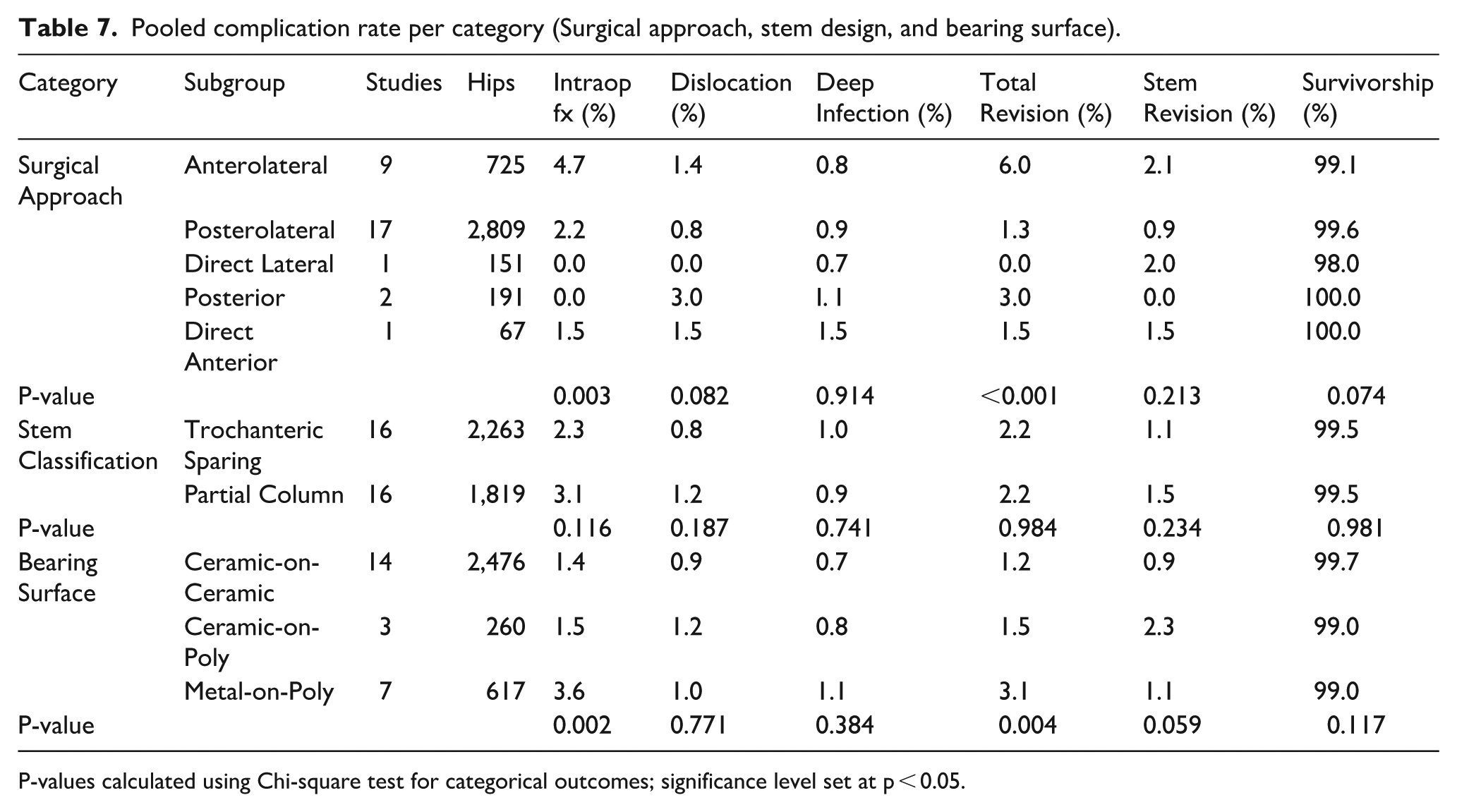
P-values calculated using Chi-square test for categorical outcomes; significance level set at p < 0.05.
Surgical approach demonstrated statistically significant differences in intraoperative fracture rates (p = 0.003) and total revision rates (p < 0.001). The anterolateral approach showed significantly higher total revision rates (6.0%) compared to the posterolateral approach (1.3%), with pairwise comparison yielding p < 0.001. Intraoperative femoral fracture rates were also significantly different across approaches, with anterolateral (4.7%) significantly higher than posterolateral (2.2%, p = 0.001).
Stem classification showed no statistically significant differences for any complication. While partial collum stems had numerically higher intraoperative fracture rates (3.1% vs. 2.3%), this difference did not reach statistical significance (p = 0.116). Total revision rates were identical (2.2%, p = 0.984).
Bearing surface analysis found statistically significant differences in intraoperative fracture rates (p = 0.002) and total revision rates (p = 0.004). Post-hoc analysis showed CoC articulations had significantly lower revision rates compared to MoP (1.2% vs. 3.1%, p = 0.002). The difference in stem revision rates approached but did not reach significance (p = 0.059).
Discussion
Several high-quality studies including large-scale registry analyses (e.g. the Dutch Arthroplasty Register) and randomised or comparative trials have demonstrated that short-stem implants confer survivorship and functional outcomes comparable to those achieved by conventional femoral stems.4,5,7,8,51
In this study of 4082 hips, short-stem total hip replacement (THR) demonstrated a significant improvement in HHS. Implant survivorship was similarly strong, with an overall stem survivorship of 98.9% at 8.6 years and 99.7% of stems remaining free from aseptic loosening. These findings align with work by Lidder et al., 52 who reported survivorship of 98.6% at up to 12.1 years.
Complication rates in this study were low, with dislocation occurring in 0.61% of cases and deep infection in 0.37%. Intraoperative fractures were more frequently associated with an anterolateral compared to posterior approach. This supports Masonis and Bourne 53 and Jolles et al. 54 , who suggest the posterolateral approach provides safer and more technically forgiving access, a particular advantage in short-stem implantation Alecci et al. 55 propose that higher complication rates with the anterolateral approach reflects a steeper learning curve and increased risk of abductor injury, with outcomes improving after a surgeon’s initial 50–100 cases.
Radiographic analysis revealed minimal osteolysis, low stress shielding, and no clinically significant subsidence. Zhang et al. 5 demonstrated that short stems preserve proximal femoral bone mineral density (BMD) more effectively than conventional stems, particularly in Gruen zones 1–7. Similarly, Liang et al. 4 reported superior bone remodelling and reduced stress shielding with short stems. These radiological benefits are particularly relevant in younger patients, where bone stock preservation is critical to mitigate future revision risk.
Meta-analysis of 11 different stem designs, categorised as trochanteric sparing and partial collum, revealed no clinically or statistically significant differences in functional outcomes or complication rates between them. These findings support the interchangeable use of these designs based on patient anatomy and surgeon preference, aligning with Khanuja et al. 11 , Kutzner et al. 56 , and Lidder et al. 52 who emphasised that surgical technique is the primary determinant of success in short-stem THA, rather than subtle differences in stem geometry.
Bearing surface selection significantly influenced both functional and revision outcomes. Ceramic-on-ceramic (CoC) and metal-on-polyethylene (MoP) bearings achieved the highest functional scores (94.8% and 95.8%, respectively), whereas ceramic-on-polyethylene (CoP) scored lower (90.0%), though CoP results were based on a single study and cannot be generalised. Revision rates were lowest for CoC (1.2%) and highest for MoP (3.1%), consistent with the superior wear resistance of ceramic bearings. These findings echo those of Lombardi et al. 57 and D’Antonio et al. 58 who found that CoC bearings offer improved durability and reduced osteolysis in younger patients. While CoC offers superior durability, it is also important to acknowledge the potential for squeaking sounds or ceramic fracture, particularly in younger, highly active patients.
Compared to broader literature, this meta-analysis reaffirms the excellent performance of short stem THR; However, our analysis adds meaningful nuance to the existing evidence by quantifying complication risks.
Clinical relevance
Surgical approach
The posterolateral approach demonstrated the lowest overall revision risk and consistent performance across complications, likely reflecting both its widespread use and inherent stability. Higher complication and revision rates were observed with the anterolateral approach, particularly for intraoperative fractures, suggesting that careful patient selection and surgical expertise are critical. Data for direct anterior approaches remain limited and should be interpreted cautiously.
Bearing surface selection
While all bearing surfaces achieved acceptable outcomes, CoC bearings were associated with superior functional results and the lowest revision risk. Bearing choice should be tailored to patient-specific risk factors and mechanical demands.
Stem design
Both trochanteric-sparing and partial-collum designs produced comparable clinical outcomes. The slightly higher fracture rate reported with partial-collum stems may reflect surgical technique rather than design limitations. Stem selection should therefore be guided primarily by patient anatomy and surgical familiarity rather than anticipated outcome differences.
Strengths and limitations
This systematic review and meta-analysis has several strengths, including a large pooled sample size of over 4000 hips, a young patient population with a mean age of <55 years, and mid- to long-term follow-up averaging nearly 9 years. The inclusion of multiple stem designs and surgical approaches provides a broad overview of contemporary short-stem practice, with consistently high survivorship rates across studies reinforcing the overall safety of this technique.
Nonetheless, several important limitations must be acknowledged. Most analyses demonstrated high statistical heterogeneity (I² > 90%), indicating substantial within-group variability. This suggests that factors beyond implant design, surgical approach, and bearing surface may influence both functional outcomes and complication rates, thereby reducing the interpretability of pooled estimates. Given these limitations in the available literature, our conclusions remain appropriately cautious.
Moreover, HHS was the consistent functional outcome measure across most studies. Whilst HHS includes an assessment of patient function, other patient-reported outcome measures (PROM) such as the HOOS, WOMAC, and EQ-5D would have better captured patients’ satisfaction, quality of life, and functional independence.
We acknowledge that potential selection bias may exist, as many included studies preferentially used short stems in younger, active patients with good bone quality.
The predominance of observational data and the scarcity of randomised controlled trials introduce further bias and residual confounding.
Taken together, these strengths and limitations suggest that while short-stem total hip arthroplasty appears to be a durable and effective option for younger patients, comparative conclusions should be interpreted with appropriate caution.
Future research
Future investigations should focus on generating high-quality evidence through standardised, prospective cohort studies and randomised controlled trials directly comparing short-stem with conventional stems in younger patients. Longer-term follow-up beyond 15 years is essential to determine true implant longevity, particularly with respect to aseptic loosening, late-onset osteolysis, and revision risk.
The influence of the surgical learning curve and technical demands especially for less common approaches such as the anterior approach requires further quantification to clarify their impact on complications and outcomes. Future studies should also incorporate validated patient-reported outcome measures, to better capture patient satisfaction, quality of life, and functional independence.
Finally, comparative analyses of bearing surfaces remain limited. Larger studies directly evaluating CoC, CoP, and MoP bearings in young, active populations are needed to guide optimal bearing selection.
Conclusion
Short-stem total hip arthroplasty in patients younger than 55 years appears to be associated with excellent mid- to long-term functional outcomes, low complication rates, and high implant survivorship. While these findings suggest that short stems are a safe and durable option for young, active patients, substantial heterogeneity across studies and the limited randomised evidence warrant cautious interpretation. These findings are hypothesis-generating and warrant confirmation in adequately powered prospective studies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.