
Abstract
Aims:
Glucagon-like peptide-1 (GLP-1) receptor agonists are increasingly utilised for metabolic optimisation in surgical patients. Their effect on postoperative patient-reported outcomes (PROMs) and satisfaction following primary total hip arthroplasty (THA) has not been well established. This study aimed to describe the association between GLP-1 prescription history and: (1) 1-year postoperative PROMs; (2) 1-year patient satisfaction; and (3) complication rates.
Methods:
This is a retrospective study of 12,749 patients who underwent primary unliteral THA at a tertiary medical centre from January 2016 to December 2022. GLP-1 agonist use was defined as a documented prescription history of a GLP-1 agonist within 1-year prior to surgery (n = 145). Multivariable logistic regression was used to evaluate GLP-1 use and 1-year PROMs [Hip disability and Osteoarthritis Outcome Score (HOOS) Pain, Physical function Shortform (PS), and Joint Replacement (JR)]. Clinical improvements were determined by the patient acceptable symptom state (PASS) and minimal clinically importance difference (MCID) thresholds. We also used multivariable logistic regression to assess the independent association between GLP-1 use and postoperative complications.
Results:
No significant difference was observed between patients with a prescription history for a GLP-1 agonist and failure to achieve PASS, MCID, or satisfaction at 1-year (odds ratio [OR] 0.99, 95% confidence interval [CI], 0.51–1.9; p = 0.98). However, there was reduced odds of 90-day readmission in patients with a prescription history for a GLP-1 agonist (OR = 0.47, p = 0.043) and an increased rate of 90-day medical complications (9.66% vs. 6.01%, p = 0.001). No significant differences were found for length-of-stay, 90-day emergency visits, or 2-year implant complication rates.
Conclusions:
This observational study found that patients with GLP-1 agonist prescription history experienced an increased rate of medical complications but a reduced rate of 90-day hospital readmission. Conversely, the negative findings of the study should be interpreted cautiously as the small, exposed cohort limits statistical power.
Introduction
Total hip arthroplasty (THA) remains 1 of the most effective interventions for alleviating pain and restoring function in patients with hip osteoarthritis.1,2 With increasing procedural volume driven by an ageing population and expanding indications, the focus in arthroplasty has shifted toward maximising value by optimising outcomes while minimising complications and healthcare utilisation. 3 Patient-reported outcome measures (PROMs), such as the Hip disability and Osteoarthritis Outcome Score (HOOS), are now integral to assessing surgical success from the patient’s perspective and are used to define clinical benchmarks like the minimal clinically important difference (MCID) and patient acceptable symptom state (PASS).4 –7 In parallel, enhanced recovery protocols and perioperative risk stratification strategies are being adopted widely to support improved recovery and satisfaction after joint replacement. 8
Glucagon-like peptide-1 (GLP-1) receptor agonists, initially developed for the treatment of type 2 diabetes mellitus, have gained attention for their pleiotropic effects, including significant weight loss, reduced systemic inflammation, and cardiometabolic protection.9,10 These effects are particularly relevant in the arthroplasty population, where obesity, diabetes, and elevated inflammatory burden are well-established risk factors for poor outcomes.11,12 As a result, primary care physicians and orthopaedic surgeons are increasingly encountering patients who are prescribed GLP-1 agents as part of preoperative metabolic optimisation. 13 Despite this trend, there remains a paucity of orthopaedic literature examining the impact of GLP-1 agonist use on THA-specific patient satisfaction and outcomes.
To the best of our knowledge, no studies have used single institutional data to comprehensively evaluate whether GLP-1 agonists influence postoperative PROMs, implant-related complications, or early medical events following THA. Given the physiologic mechanisms through which GLP-1 agents exert their effects, including modulation of glucose homeostasis, appetite suppression, and potential protective effects on vascular endothelium, their role in shaping both subjective recovery metrics and objective surgical outcomes warrants investigation.14,15 Specifically, it is unclear whether GLP-1 use is associated with improved achievement of PROM thresholds such as HOOS-Pain, HOOS-Physical Function Shortform (PS), and HOOS-Joint Replacement (JR), or if it modifies the risk profile for common postoperative implant complications such as infections and aseptic loosening.
The primary aim of this study was to assess whether GLP-1 agonist prescription history is associated with a change in 1-year PROMs and patient satisfaction following THA. A secondary aim was to evaluate its association with early postoperative outcomes, including 90-day medical complications, emergency department visits, readmission rates, and implant complication.
Methods
Study design and data source
This was a retrospective study of elective primary THA patients from 9 sites within a single tertiary academic medical centre. All patients between January 2016 and December 2022 were screened for inclusion (n = 14,548 patients). Data were extracted from the Orthopedic Minimal Data Set Episode of Care (OME), a prospectively maintained institutional registry, which captures patient demographics, comorbidities, medication history, and longitudinal patient-reported outcome measures (PROMs).16 –18 GLP-1 agonist users were identified using the OME and electronic health system. GLP-1 agonist exposure was defined as documented prescription history of any GLP-1 receptor agonist within one year prior to the index arthroplasty. This reflects prescription history and does not confirm perioperative use, adherence, dose, or duration. Patients without documented GLP-1 prescription in the year prior to surgery were classified as non-users. The median duration of GLP-1 prescription among exposed patients was 188 days (interquartile range 48–917).
Study population
Of the patients screened for inclusion, patients were ineligible if they underwent staged or simultaneous bilateral THA. A total of 12,749 patients undergoing unilateral elective THA were eligible for inclusion. Of those, 145 patients were classified as GLP-1 users (Figure 1(a)). Patients were excluded from analysis of 1-year PROM outcomes if preoperative and postoperative PROMs were not complete. A total of 8827 patients completed preoperative and 1-year PROMs, of which 93 were GLP-1 users (Figure 1(b)).
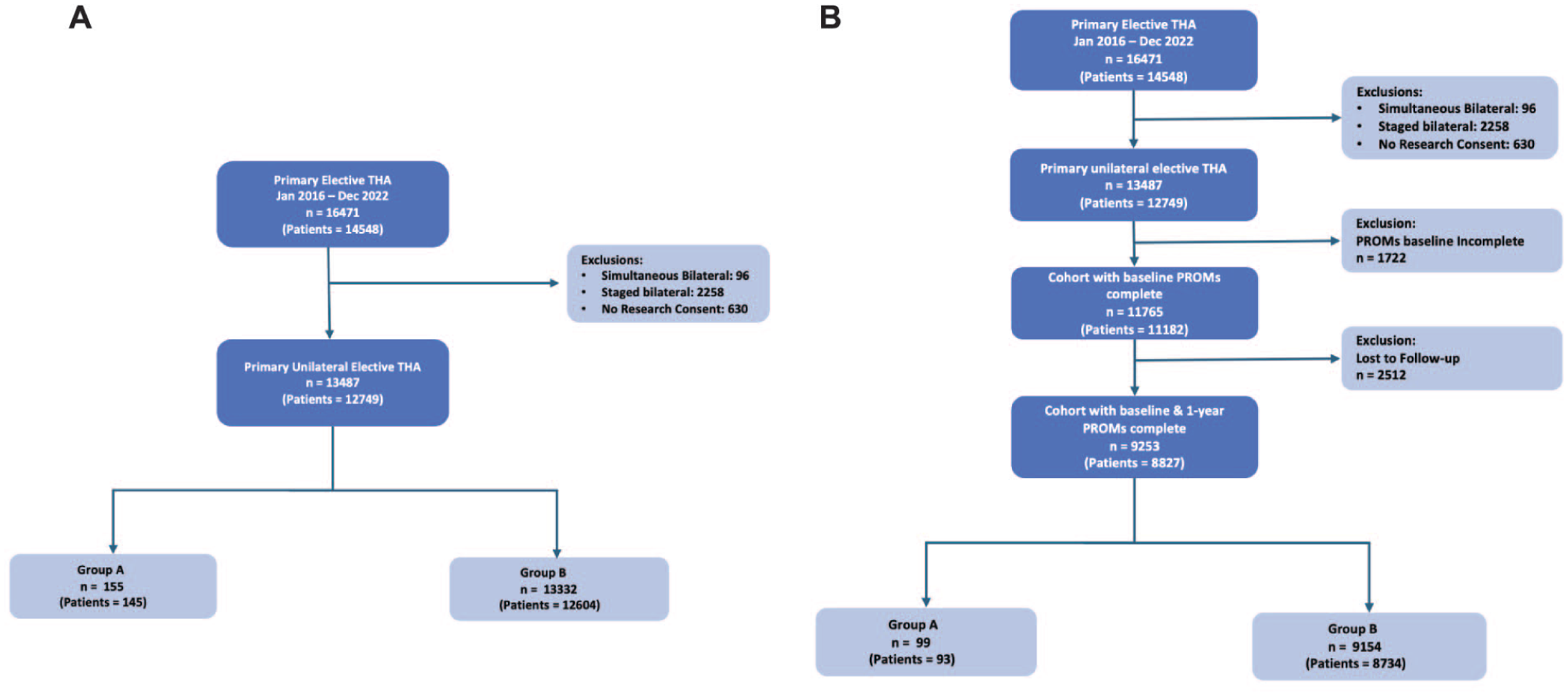
Strengthening the Reporting of Observational studies in Epidemiology (STROBE) diagram for: (a) overall cohort; and (b) patient-reported outcome measurement (PROM) cohort; THA: total hip arthroplasty.
Data stratification and outcomes
The primary exposure variable was GLP-1 agonist prescription history, stratified as a binary variable (prescription history vs no prescription history). Outcomes were evaluated across 2 domains: patient-reported outcomes and perioperative events. PROMs were assessed using the Hip disability and Osteoarthritis Outcome Score (HOOS) subscales Pain, Physical Function Shortform (PS), and Joint Replacement (JR), captured both preoperatively and at one year postoperatively. 19 These outcomes were used to determine whether patients achieved clinically meaningful improvements in symptoms, as defined by MCID thresholds, and whether they reached acceptable postoperative states, as defined by PASS thresholds. 20 MCID thresholds were calculated using a distribution-based method that defines clinically meaningful improvement as 1-half standard deviation of the change in PROM scores from baseline to1 year. 21 PASS thresholds were defined using anchor-based methods. 22 In addition to PROM achievement, patient satisfaction at one year was evaluated using a binary satisfaction question embedded within the PROM survey, with dissatisfaction modelled as the event of interest.7,23 Perioperative outcomes included length of stay (LOS), 90-day readmissions, emergency department (ED) visits, and medical complications. 2-year implant-related complications were also analysed.
Statistical analysis
Continuous variables were summarised using medians and interquartile ranges (IQRs), and categorical variables were reported as counts and percentages (Table 1). Between-group comparisons were performed using Wilcoxon rank-sum tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables, as appropriate. Multivariable logistic regression models were constructed to evaluate the independent association of GLP-1 use with failure to achieve PROM thresholds, dissatisfaction, and adverse perioperative outcomes. Models were adjusted for prespecified covariates, including age, sex, race, body mass index (BMI), education level, smoking status, insurance type, Charlson Comorbidity Index (CCI), area deprivation index (ADI), preoperative NARX score, PROM phenotype, baseline PROM score, diabetes status, insulin use, and metformin use. Missing data were addressed using multiple imputation, with models fit across imputed datasets and results pooled for inference. The events-per-variable ratio exceeded conventional thresholds for acceptable model stability. All statistical analyses were conducted using R software (Version 4.2; Vienna, Austria), with a 2-sided significance threshold of 0.05.
Baseline characteristics.
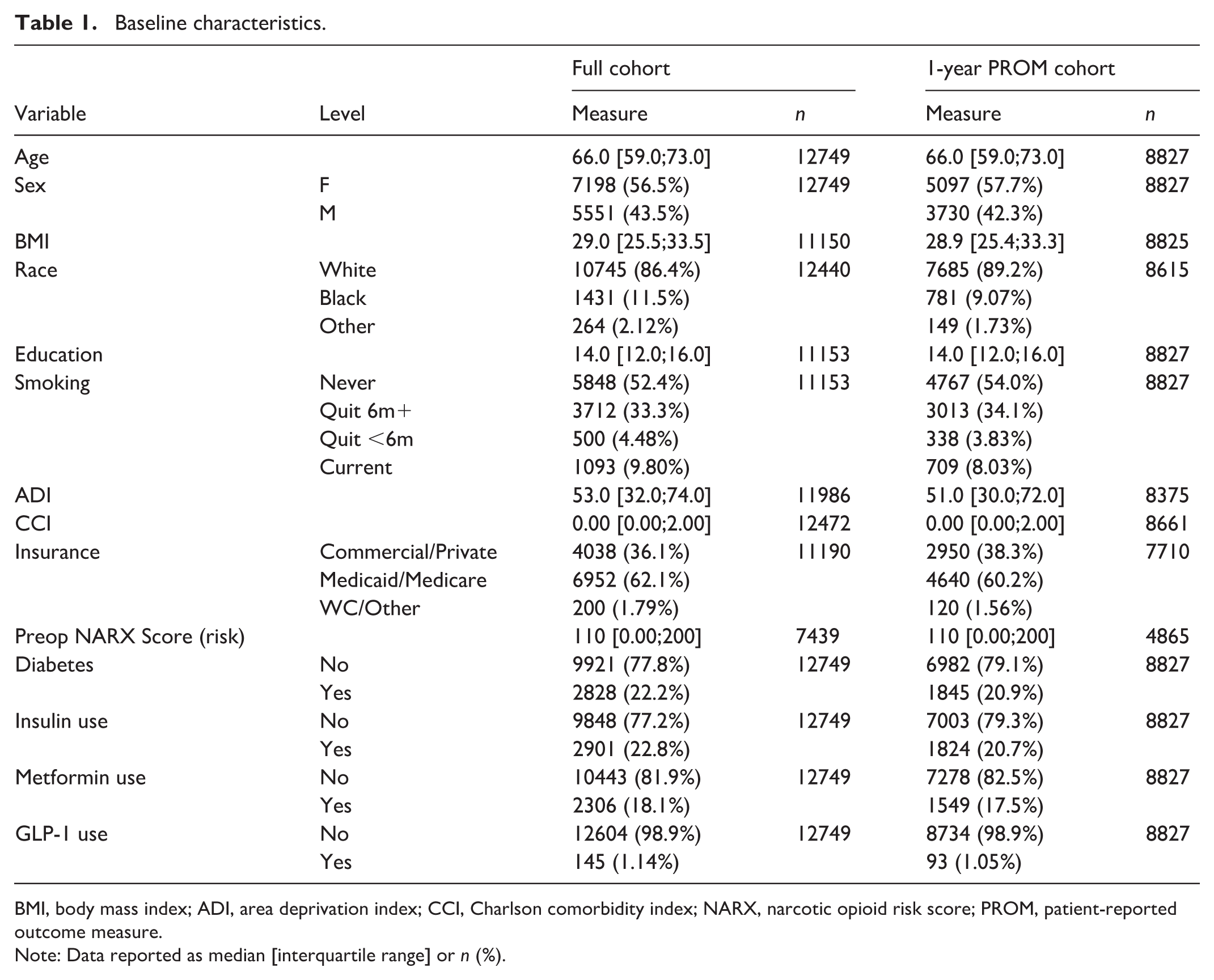
BMI, body mass index; ADI, area deprivation index; CCI, Charlson comorbidity index; NARX, narcotic opioid risk score; PROM, patient-reported outcome measure.
Note: Data reported as median [interquartile range] or n (%).
Ethics approval
Approval was obtained for this study through our institution’s ethical review board.
Results
Early postoperative outcomes
Patients with a prescription history of a GLP-1 agonist were observed to have a reduced rate of 90-day hospital readmission (odds ratio [OR] 0.47; 95% confidence interval [CI], 0.22–0.98; p = 0.043) (Table 2). No significant differences were observed in 90-day emergency department visits (OR 0.62; p = 0.087) or length of stay (OR 1.05; p = 0.83) (Table 2). However, patients with a GLP-1 prescription history experienced a higher rate of 90-day medical complications (9.7% vs. 6.0%, p = 0.001) (Table 3).
Multivariable logistic regression for length of stay (LOS), 90-day ED visits, and 90-day readmissions for GLP-1 agonist users versus non-users.
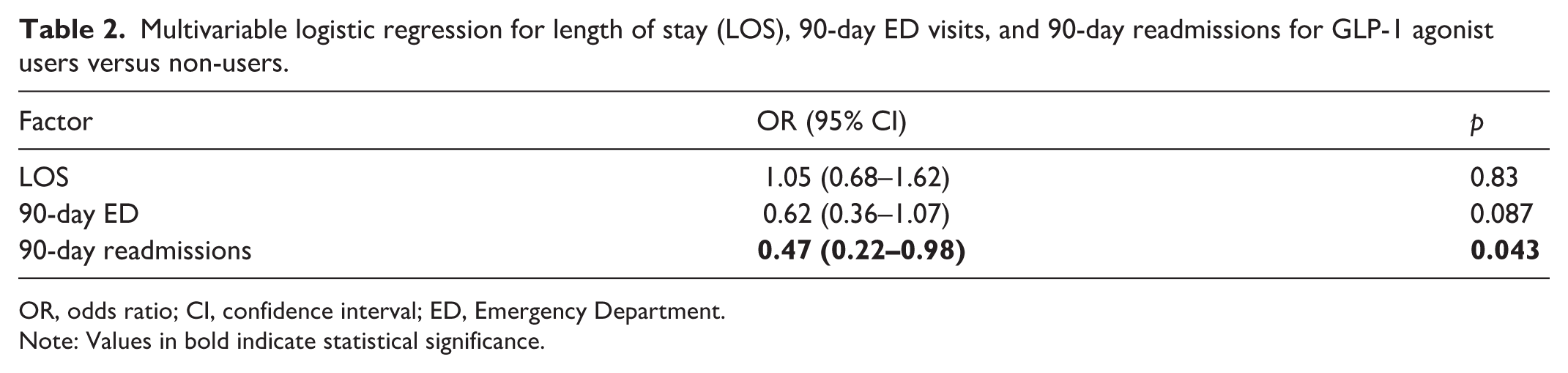
OR, odds ratio; CI, confidence interval; ED, Emergency Department.
Note: Values in bold indicate statistical significance.
Comparison between 90-day medical complication rates.
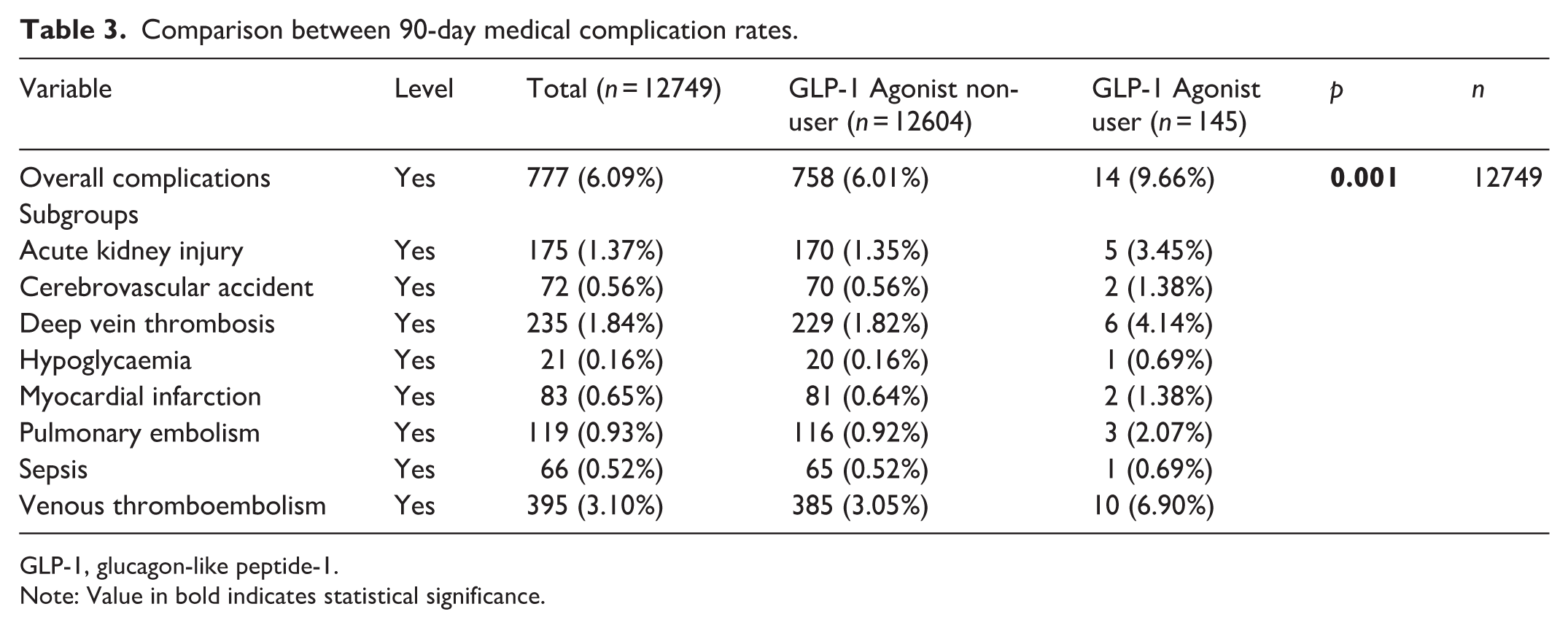
GLP-1, glucagon-like peptide-1.
Note: Value in bold indicates statistical significance.
Implant-related complications
At 2 years postoperative, no significant difference was observed in the overall implant-related complication rate between patients with and without a GLP-1 prescription history (9.7% vs. 9.0%, p = 0.892) (Table 4). Rates of aseptic loosening, periprosthetic fracture, prosthetic joint infection, and revision surgery were similar across groups.
Comparison between 2-year implant complication rates.
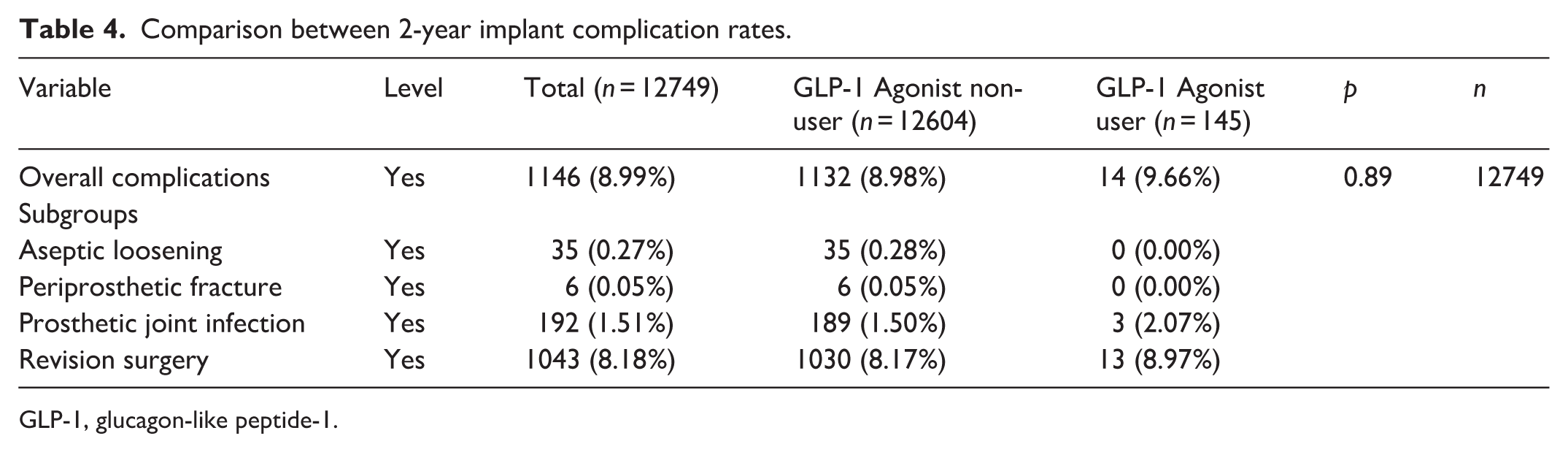
GLP-1, glucagon-like peptide-1.
1-year PROMs and satisfaction
Trends in failure to achieve the minimal clinically important difference (MCID) for HOOS Pain (OR 1.93; p = 0.148), HOOS PS (OR 1.33; p = 0.431), or HOOS JR (OR 1.62; p = 0.259) were mildly greater in patients with a GLP-1 prescription history but these findings did not reach significance (Table 5). Similar trends were observed for the patient acceptable symptom state (PASS) across the subscales: HOOS Pain (OR 1.49; p = 0.086), HOOS PS (OR 1.18; p = 0.493), and HOOS JR (OR 1.35; p = 0.185) (Table 5). No difference in 1-year dissatisfaction was observed (OR 0.99; 95% CI, 0.51–1.9; p = 0.976).
Multivariable logistic regression for failure to reach attainment of MCID or PASS for GLP-1 agonist users versus non-users.
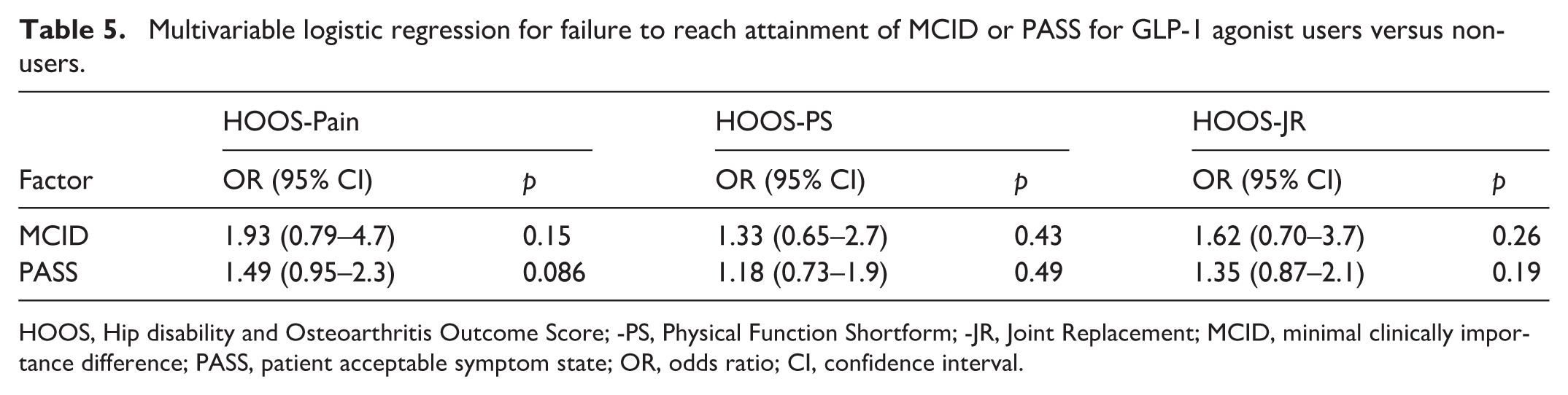
HOOS, Hip disability and Osteoarthritis Outcome Score; -PS, Physical Function Shortform; -JR, Joint Replacement; MCID, minimal clinically importance difference; PASS, patient acceptable symptom state; OR, odds ratio; CI, confidence interval.
Discussion
In this retrospective cohort study of patients undergoing primary THA, patients with a documented GLP-1 prescription history were observed to have borderline reduced rates of 90-day readmission and higher rates of short-term medical complications. No significant differences were observed between documented GLP-1 prescription history and 2-year implant-related complications or one-year PROMs, including MCID, PASS, or overall satisfaction. However, several PROM odds ratios trended toward worse outcomes without reaching significance, and these results should be interpreted cautiously due to the small, exposed cohort.
This study builds on prior literature by providing novel insights in 2 key areas. First, while GLP-1 receptor agonists have been extensively studied in the context of metabolic and cardiovascular outcomes, recent investigations have begun exploring their role in orthopaedic surgical populations.24 –26 Several studies have suggested that GLP-1 use may lead to reduced rates of short-term periprosthetic joint infection control in patients undergoing total joint arthroplasty.27,28 For instance, Kim et al. 29 found that morbidly obese patients on GLP-1 agonists had lower rates of 90-day postoperative infections compared to those not taking GLP-1 agonists (1.6 vs. 3.2%, p = 0.03). Others have reported reduced wound complications and hospital utilisation among GLP-1 users undergoing orthopaedic procedures, though the data remain limited and heterogeneous.24,26 For instance, Heo et al. 30 found that patients not on GLP-1 agonists experienced higher rates of extended hospital stays (OR 1.25, p = 0.01). Our study attempts to complement this growing literature by examining both short-term complications and long-term PROMs following THA, thereby providing a more comprehensive assessment of surgical risk and recovery in this population. Second, while GLP-1 use has been increasingly adopted in preoperative optimisation pathways due to its effects on weight loss and glycaemic control, there has been a lack of data on how these medications influence PROMs, a critical component of contemporary value-based arthroplasty care.
The reduction in 90-day readmission among patients with a GLP-1 prescription history is notable and may reflect better metabolic optimisation prior to surgery. Prior studies have shown that patients with improved preoperative glycaemic control and lower BMI are less likely to require early readmission following arthroplasty.31,32 However, the increased rate of early medical complications – particularly thromboembolic events – raises concern and the current literature shows mixed results on this association. For example, our results corroborate those found by Magruder et al., 33 in which GLP-1 agonist users had higher incidence of 90-day postoperative medical complications such as myocardial infarction (1.0 vs. 0.7%, p = 0.03) and acute kidney injury (4.9 vs. 3.9%, p < 0.001). However, Heo et al. 30 found no difference in 90-day postoperative medical complications between GLP-1 agonist users and non-users. 1 potential explanation is that GLP-1 related shifts in volume status, renal perfusion, or metabolic stress may predispose to complications in the immediate postoperative period. Another explanation is that patients with a prescription for GLP-1 agonists are inherently sicker. Nonetheless, these effects need to be further explored.
From a functional perspective, mild differences in MCID and PASS attainment trends across users and non-users were observed but did not reach significance. Given the imprecision of estimates, these findings should be interpreted as preliminary and hypothesis-generating rather than as evidence of equivalence. The absence of statistically significant differences in PROM outcomes does not exclude clinically meaningful differences in a larger exposed cohort.
This study has several limitations. First, its retrospective design is subject to selection bias and unmeasured confounding. Although we adjusted for a wide range of clinical and demographic variables, residual confounding is possible; patients with a GLP-1 prescription history may differ in unmeasured factors such as disease burden, diabetes severity, adherence to medication, and preoperative frailty. Second, the number of patients with GLP-1 prescription history was relatively small, which may have limited statistical power for comparisons; sample size precludes detection of clinically important differences, and non-significant findings should be interpreted cautiously. Third, while PROMs were collected prospectively, patients with incomplete follow-up were excluded from analysis, introducing potential attrition bias. The PROM cohort represents a subset of eligible patients and differential attrition between groups could bias results in either direction. A comparison of patients with and without 1-year PROM follow-up is provided in Supplemental Table 1, demonstrating largely similar baseline characteristics, though this does not eliminate the potential for attrition bias. Lastly, we were unable to evaluate the impact of GLP-1 dosing, compliance, or formulation, which may have heterogeneous effects. Despite these limitations, our study has several strengths. It represents one of the first attempts to rigorously evaluate both clinical and patient-reported outcomes in patients with a GLP-1 prescription history undergoing THA. By examining both short-term complications and long-term PROMs, we provide a more complete picture of the risks and benefits associated with this increasingly common drug class.
Conclusion
History of a GLP-1 receptor agonist prescription was not observed to show a significant difference in 1-year PROMs, achievement of clinical improvement thresholds, or satisfaction following THA. A higher rate of 90-day medical complications was observed among GLP-1 prescription holders, and a mild reduction in readmission warrants cautious interpretation. These preliminary findings are limited by the prescription-based exposure definition, small, exposed cohort, and inherent constraints of a retrospective study. Future prospective studies with confirmed medication use, adherence data, and adequate sample sizes are needed to clarify the relationship between GLP-1 therapy and THA outcomes.
Supplemental Material
sj-docx-1-hpi-10.1177_11207000261450078 – Supplemental material for 1-year patient-reported outcomes in patients with a documented GLP-1 agonist prescription history prior to total hip arthroplasty: a retrospective cohort study
Supplemental material, sj-docx-1-hpi-10.1177_11207000261450078 for 1-year patient-reported outcomes in patients with a documented GLP-1 agonist prescription history prior to total hip arthroplasty: a retrospective cohort study by Brian Benyamini, Shujaa T Khan, Khaled A Elmenawi, Shlok V Patel, Matthew E Deren, Nicolas S Piuzzi, Trevor G Murray, Robert M Molloy, Viktor E Krebs, Nicholas R Scarcella, Michael Erossy, Alexander L Roth, Michael R Bloomfield, Carlos A Higuera, John P McLaughlin and Peter A Surace in HIP International
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NP: provides research support to Osteal Therapeutics, Peptilogics, RegenLab, Signature Orthopaedics, Zimmer.
All other authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.