
Abstract
Introduction:
Hip fractures are associated with substantial blood loss occurring both pre- and intraoperatively. While intraoperative bleeding has been extensively studied, less is known about preoperative haemaglobin decline and its determinants. This study aims to identify factors associated with substantial preoperative blood loss in hip fracture patients and assess its clinical implications.
Materials and methods:
We retrospectively analysed 1935 hip fracture patients treated at a single tertiary centre between 2019 and 2024. Haemoglobin (Hb) was measured at Emergency Department admission and before surgery. Preoperative Hb decline (ΔHb), used as a surrogate marker for blood loss, was calculated, and patients were categorised into those with substantial (⩾2 g/dL) versus non-substantial (<2 g/dL) preoperative Hb decline. Multivariate regression identified factors associated with substantial preoperative blood loss. Propensity score matching (1:1) was performed to compare clinical outcomes between groups.
Results:
Substantial preoperative Hb drop occurred in 49.1% of patients. In multivariate analysis, extracapsular fracture type was strongly associated with preoperative blood loss (OR 1.86; 95% CI, 1.54–2.26; p < 0.001), as was advanced age (OR: 1.65 for age >85 vs <65, p = 0.041) and prolonged time to surgery 24-48h (OR: 1.52, 95% CI: 1.06-2.16, p = 0.022). In the propensity-matched cohort (768 patients in each group), substantial preoperative blood loss was associated with higher transfusion rates (17.8% vs 8.1%, p < 0.001) and longer hospital stays (10.8 vs 8.7 days, p < 0.001).
Conclusions:
Extracapsular fracture type, advanced age (>85 years), and prolonged time to surgery (>24 hours) were independently associated with substantial preoperative Hb decline in hip fracture patients. Substantial preoperative Hb decline was associated with increased transfusion requirements and prolonged hospitalisation. These findings may help identify high-risk patients in whom targeted preoperative haemostatic strategies and closer Hb monitoring warrant further investigation.
Keywords
Introduction
Hip fractures are associated with high healthcare costs, 20–30% 1-year mortality, and substantial morbidity. 1 1 such complication is significant blood loss, a critical concern in hip fracture management, with total losses of 500–1500 mL commonly reported. 2
Hip fracture haemorrhage occurs in 2 distinct phases: preoperative (from injury to surgical incision) and intraoperative (during surgical intervention).3,4 While intraoperative blood loss has been extensively studied and addressed with various strategies, 5 such as, tranexamic acid (TXA) administration, 6 permissive hypotension techniques, 7 cell salvage, 8 and electrocautery, 9 preoperative bleeding has received comparatively little attention.
Previous studies have documented clinically significant preoperative Haemoglobin (Hb) drops (often ⩾2 g/dL) in hip fracture patients.3,4 This “hidden” haemorrhage can represent up to 40–50% of the total perioperative blood loss and contributes significantly to overall anaemia and poor outcomes.3,4 However, factors that could predict this preoperative blood loss remain poorly characterised. Understanding these factors is essential for developing targeted preoperative haemostatic interventions that can be specifically tailored to high-risk patients, potentially improving outcomes while optimising resource allocation.
The objective of this study was to identify independent factors associated with substantial preoperative blood loss in hip fracture patients and to assess its relationship with postoperative clinical outcomes. We hypothesised that extracapsular fractures, older age, and higher comorbidity burden would be associated with substantial preoperative Hb drop, and that patients with substantial preoperative blood loss would have worse clinical outcomes than those without.
Materials and methods
Study design and population
This retrospective cohort study analysed hip fracture patients at a single Level I trauma centre from January 2019 to July 2024. The institutional review board approved the study (IRB: TLV-0566-23), conducted by the Declaration of Helsinki principles.
We included patients undergoing surgical treatment for acute hip fractures (cephalo-medullary nailing or hip arthroplasty) with available Hb measurements at emergency department admission and pre-operatively. Exclusions comprised: pathological fractures (n = 12), missing admission Hb (n = 73), missing intraoperative Hb (n = 499), and preoperative transfusions (n = 69). The 69 patients who received preoperative blood transfusions were excluded to avoid confounding in the assessment of preoperative Hb decline, as transfusions would artificially elevate Hb values and preclude accurate quantification of preoperative blood loss. Of 2,588 initially identified patients, 1935 met inclusion criteria (Figure 1).
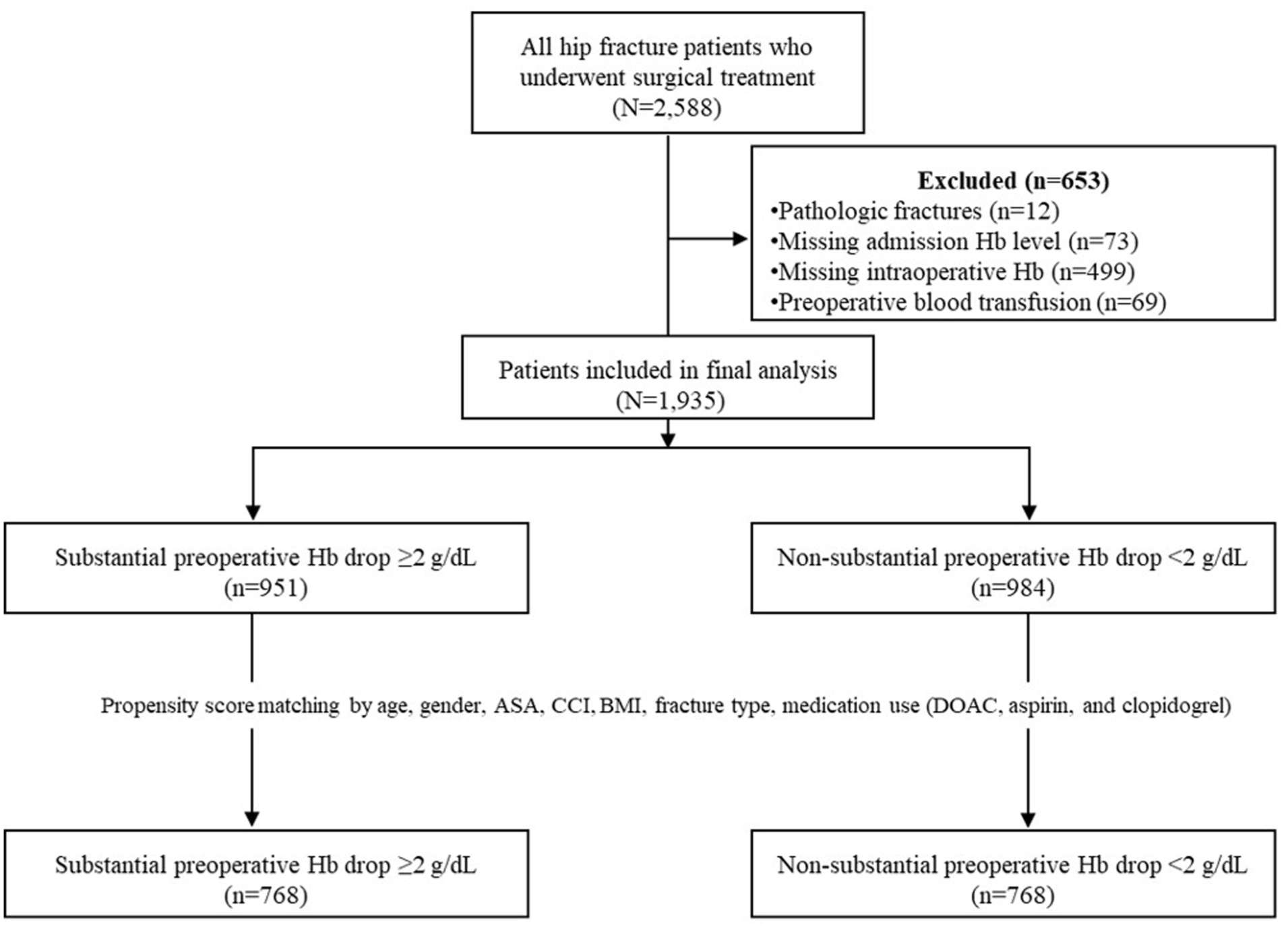
Flow diagram of patient selection and exclusion criteria.
Data collection
Data were extracted from electronic medical records, including patient age, gender, comorbidities (American Society of Anesthesiologists [ASA] classification, Charlson Comorbidity Index [CCI]), chronic medication use with haemodynamic effects (aspirin, clopidogrel, direct oral anticoagulants [DOACs]), time from ED admission to surgery, transfusion requirements, hospital length of stay (LOS), readmission rates, and mortality. Body mass index (BMI) was calculated from height and weight measurements. Fracture type was classified as either intracapsular (femoral neck fractures) or extracapsular (intertrochanteric and subtrochanteric fractures).
Hb was measured at 2 key time points: (1) on admission to the ED (initial lab value upon presentation); and (2) in the operating room (OR) prior to anaesthesia induction. From these values, we calculated the preoperative Hb change (ΔHb). A negative ΔHb indicates a drop in Hb (blood loss). ΔHb was treated as a surrogate marker for preoperative blood loss, although may also be influenced by haemodilution and perioperative fluid shifts.;
Patients were categorised into 2 groups based on the magnitude of preoperative Hb decline: (1) those with substantial preoperative blood loss (defined as ΔHb ⩾2 g/dL); and (2) those with non-substantial blood loss (ΔHb <2 g/dL). This threshold was chosen based on previous literature suggesting that a Hb drop of 2 g/dL or greater represents clinically significant blood loss and has been associated with increased transfusion requirements and complications.10,11
Transfusion decisions followed institutional guidelines consistent with American Association of Blood Banks (AABB) recommendations.12,13 Hb thresholds were <8 g/dL for haemodynamically stable patients and <9 g/dL for patients with cardiovascular comorbidities. Clinical symptoms (tachycardia, hypotension, functional decline) and patient-specific factors were also considered.
Statistical analysis
Descriptive statistics were reported as means and standard deviations (SD) for continuous variables and frequencies and percentages for categorical variables. Between-group comparisons were performed using independent t-tests for continuous variables (with Welch’s correction when variances were unequal) and chi-square tests or Fisher’s exact test for categorical variables.
For clinically relevant interpretation, age was stratified into 3 categories:14 –16 <65 years; 65–85 years; and >85 years. For analysis of the time to surgery effects, patients with surgery delayed beyond 48 hours were excluded (n = 160, 8.3% of total cohort). At the study institution, surgery within 48 hours represents standard practice for hip fractures, as patients with longer delays are typically non-operable due to severe clinical deterioration. Time from ED admission to surgery was categorised into 3 intervals: <12 hours; 12–24 hours; and 24–48 hours. This exclusion may introduce selection bias by removing patients with the longest preoperative interval, in whom Hb decline is potentially greatest, and the time-to-surgery analysis should be interpreted as applying to surgically eligible hip-fracture patients rather than to the entire admission cohort.
Logistic regression analysis was performed to identify independent risk factors for substantial preoperative Hb drop (⩾2 g/dL). The final model incorporated fracture type (extracapsular vs. intracapsular), age category, gender, ASA score (dichotomised as 1–2 vs. 3–4), CCI, categorised time from admission to surgery, and use of anticoagulant/antiplatelet medications (DOACs, aspirin, clopidogrel). Odds ratios (OR) with 95% confidence intervals (CI) and p-values were calculated. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC).
Due to significant differences in demographic parameters between groups as shown in Table 1, we performed a 1:1 propensity match by age, gender, ASA classification, CCI, BMI, fracture type, and medication use (DOAC, aspirin, and clopidogrel) to account for any potential confounding variables. The propensity score was defined as the conditional probability of belonging to the substantial preoperative Hb-decline group given baseline covariates. The 1:1 match was performed using a balanced, nearest-neighbour propensity score. After confirming balanced cohorts, clinical outcomes were compared between the matched groups using the statistical tests described above.
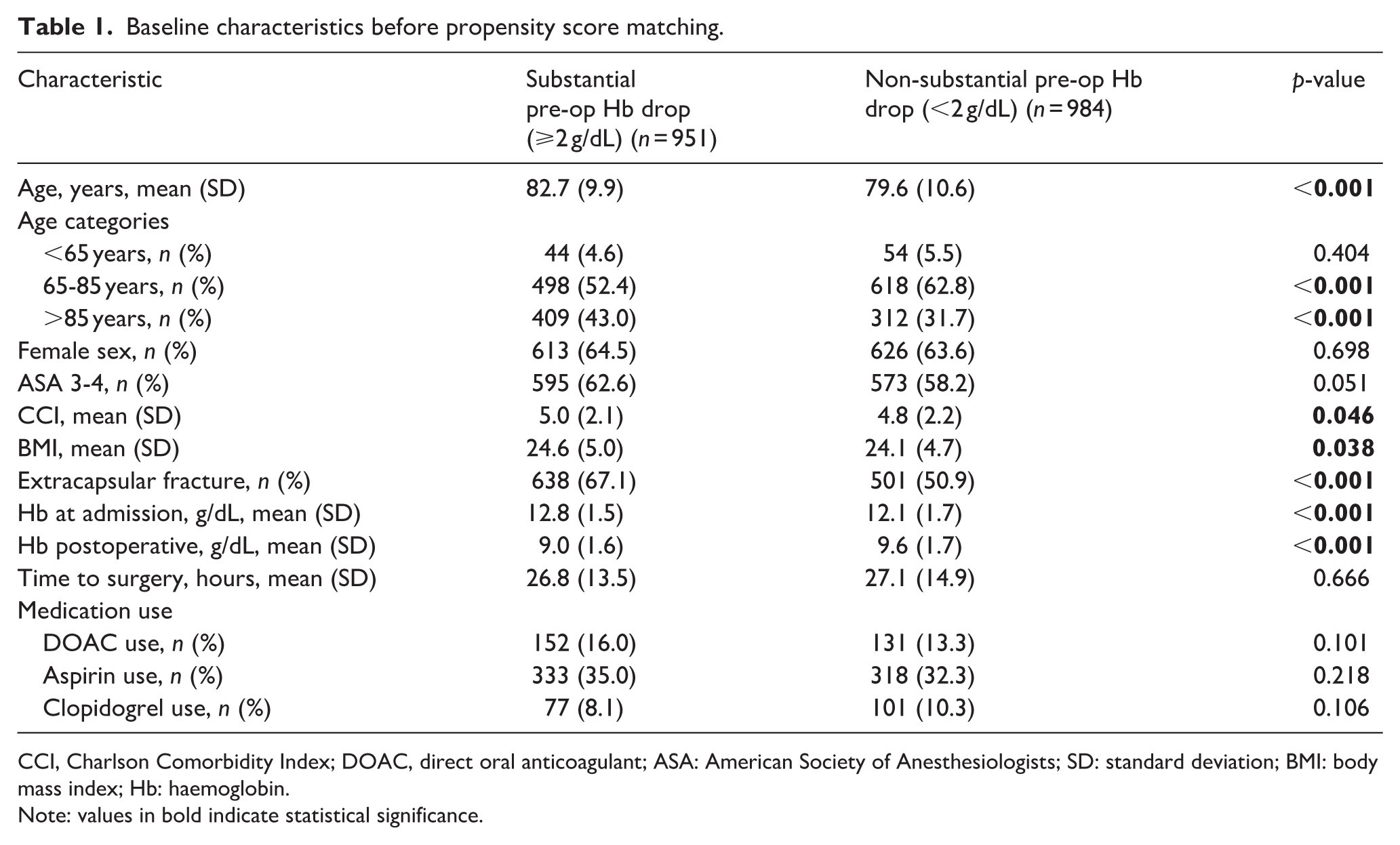
Baseline characteristics before propensity score matching.
CCI, Charlson Comorbidity Index; DOAC, direct oral anticoagulant; ASA: American Society of Anesthesiologists; SD: standard deviation; BMI: body mass index; Hb: haemoglobin.
Note: values in bold indicate statistical significance.
A 2-tailed p-value <0.05 was considered statistically significant. All analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY) with the PSMatching extension.
Results
Baseline characteristics
Of the 1935 hip fracture patients included in the study, substantial preoperative Hb drop (⩾2 g/dL) occurred in 951 patients (49.1%). As shown in Table 1, patients with substantial preoperative Hb drop were significantly older (mean age 82.7 vs. 79.6 years, p < 0.001) and had slightly higher mean CCI scores (5.0 vs. 4.8, p = 0.046). The proportion of patients with ASA 3–4 classification was higher in the substantial drop group, though this difference was of borderline significance (62.6% vs. 58.2%, p = 0.051). The proportion of extracapsular fractures was substantially higher in the substantial blood loss group (67.1% vs. 50.9%, p < 0.001). Admission Hb was higher in the substantial drop group (12.8 ± 1.5 vs. 12.1 ± 1.7 g/dL, p < 0.001), whilst postoperative Hb was lower (9.0 ± 1.6 vs. 9.6 ± 1.7 g/dL, p < 0.001).
Time from admission to surgery (26.8 vs. 27.1 hours, p = 0.666), as well as medication use including DOAC (16.0% vs. 13.3%, p = 0.101), aspirin (35.0% vs 32.3%, p = 0.218) and clopidogrel (8.1% vs. 10.3%, p = 0.106) were similar between groups.
Independent factors associated with preoperative blood loss
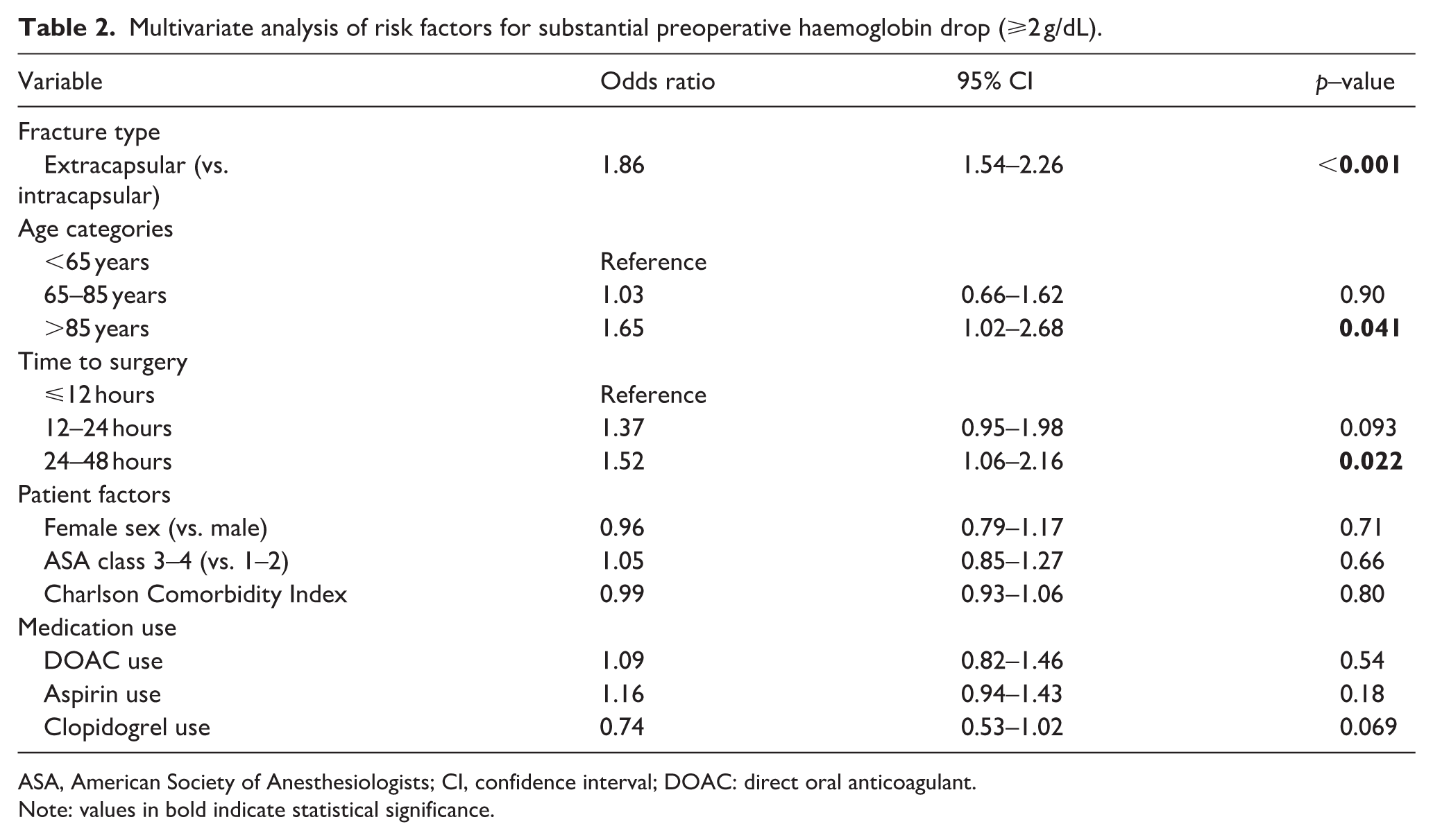
Multivariate logistic regression analysis (Table 2) identified extracapsular fracture type as the strongest independent factor, with 1.86 times higher odds of substantial preoperative blood loss compared to intracapsular fractures (95% CI, 1.54–2.26; p < 0.001). Advanced age demonstrated a significant relationship, but only for the oldest group; patients >85 years had 1.65 times higher odds (95% CI, 1.02–2.68; p = 0.041) compared to those <65 years, while patients aged 65–85 years showed no increased risk (OR 1.03; 95% CI, 0.66–1.62, p = 0.90). Surgery performed 24–48 hours after admission was associated with increased odds of substantial Hb drop compared to surgery within 12 hours (OR 1.52; 95% CI, 1.06–2.16; p = 0.022), while surgery at 12–24 hours showed a non-significant trend (OR 1.37; 95% CI, 0.95–1.98, p = 0.093). Other factors, including gender, CCI, chronic medication use, and ASA classification were not associated with substantial preoperative blood loss.
Multivariate analysis of risk factors for substantial preoperative haemoglobin drop (⩾2 g/dL).
ASA, American Society of Anesthesiologists; CI, confidence interval; DOAC: direct oral anticoagulant.
Note: values in bold indicate statistical significance.
Propensity score matching and clinical outcomes
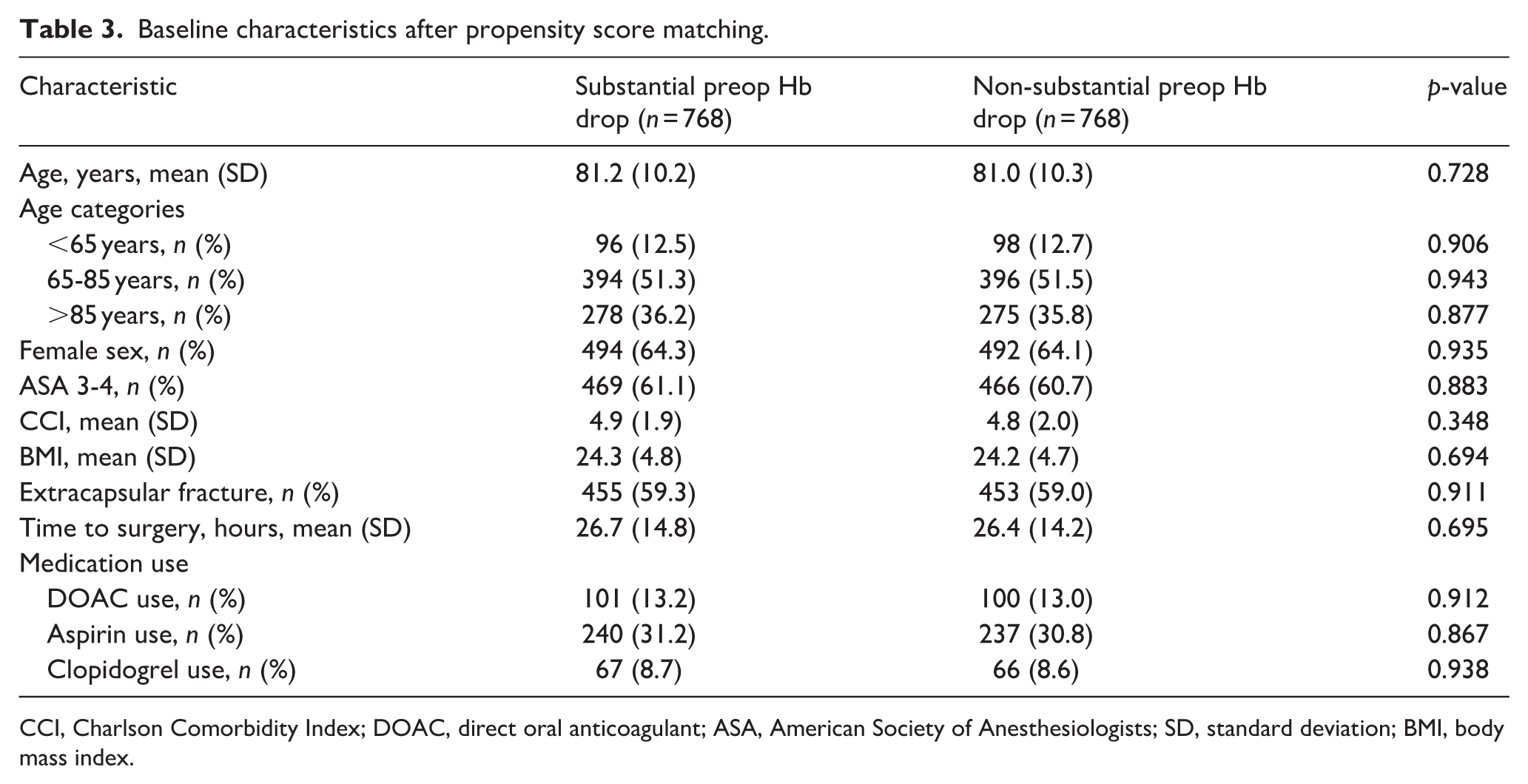
After 1:1 nearest-neighbour matching, we obtained 768 matched pairs (1536 patients total), representing 79.4% of the original cohort. Following propensity matching, there were no significant differences in baseline characteristics between groups (Table 3).
Baseline characteristics after propensity score matching.
CCI, Charlson Comorbidity Index; DOAC, direct oral anticoagulant; ASA, American Society of Anesthesiologists; SD, standard deviation; BMI, body mass index.
Comparison of clinical outcomes between the propensity-matched cohorts is shown in Table 4. Transfusion rates were markedly higher in patients with substantial preoperative Hb drop (17.8% vs. 8.1%, p < 0.001), with a relative risk of 2.20 (95% CI, 1.70–2.85). Similarly, hospital LOS was significantly longer in the substantial blood loss group (10.8 vs. 8.7 days, p < 0.001), with a mean difference of 2.1 days (95% CI, 1.4–2.8).
Clinical outcomes in propensity score–matched cohorts (n = 768 per group).
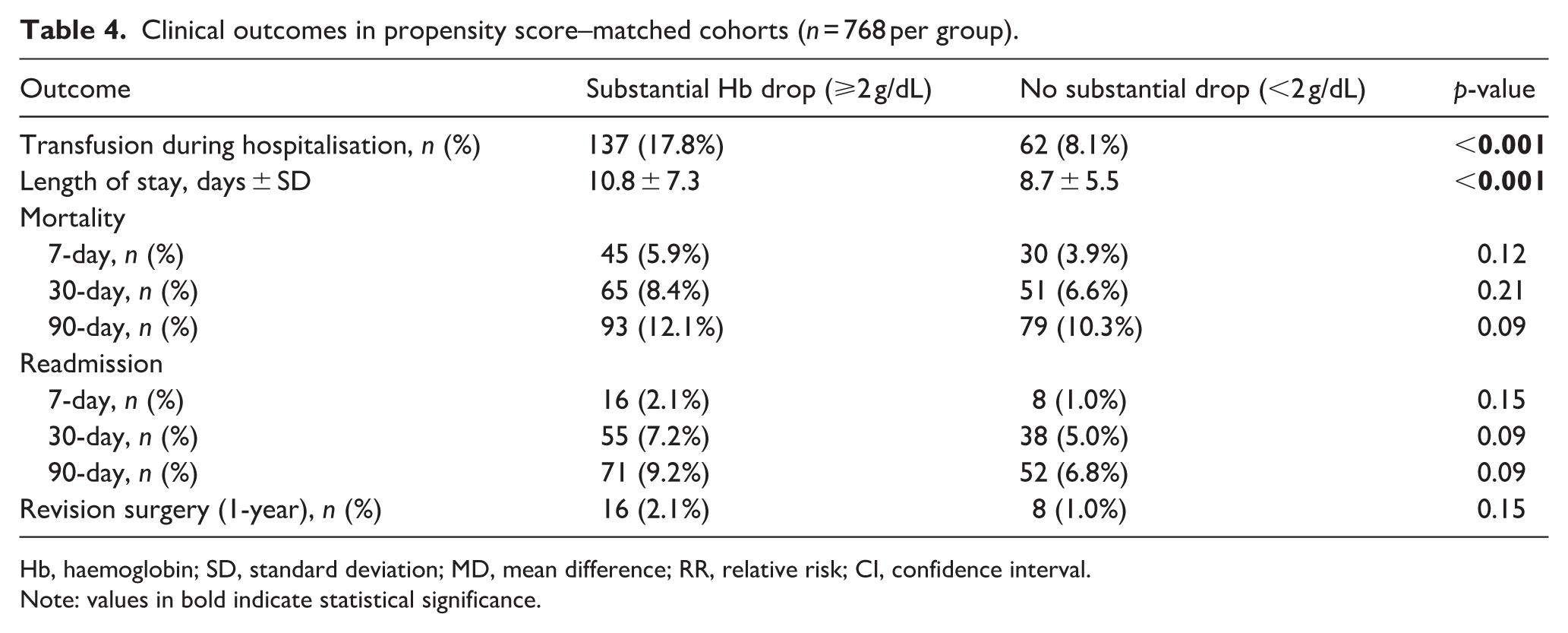
Hb, haemoglobin; SD, standard deviation; MD, mean difference; RR, relative risk; CI, confidence interval.
Note: values in bold indicate statistical significance.
A trend toward higher mortality rates in the substantial blood loss group was observed at all measured time points, but these differences did not reach statistical significance: 7-day (5.9% vs. 3.9%, p = 0.12), 30-day (8.4% vs. 6.6%, p = 0.21), and 90-day (12.1% vs. 10.3%, p = 0.09). Similarly, readmission rates were higher in the substantial blood loss group at 7 days (2.1% vs. 1.0%, p = 0.15), 30 days (7.2% vs. 5.0%, p = 0.09), and 90 days (9.2% vs. 6.8%, p = 0.09), but these differences did not achieve statistical significance. The rate of revision surgery within 1 year was also higher in the substantial blood loss group, though not significantly (2.1% vs. 1.0%, p = 0.15).
Discussion
This study aimed to identify factors associated with substantial preoperative blood loss in hip fracture patients and to assess its association with postoperative clinical outcomes. The findings identify extracapsular fracture type, advanced age (>85 years), and prolonged time to surgery (>24 hours) as key factors associated with substantial preoperative blood loss in hip fracture patients. Our propensity-matched analysis demonstrates that preoperative blood loss is independently associated with worse clinical outcomes, particularly increased transfusion requirements and longer hospitalisations.
Fracture type emerged as the strongest independent predictor, with extracapsular fractures associated with nearly twice the odds of substantial preoperative blood loss compared to intracapsular fractures. The anatomical basis for this finding likely involves the rich vascularity of the extracapsular region, which receives branches from multiple arterial sources and contains highly vascular cancellous bone. 17 When fractured, this region can bleed substantially into the surrounding tissues before surgical stabilisation. In contrast, intracapsular fractures occur within the joint capsule, where haemorrhage might be contained by capsular tamponade. 18 Our findings align with previous studies which suggest greater preoperative blood loss in extracapsular fractures. Harper et al. 19 found in their analysis of 74 patients that extracapsular fractures had 65% higher hidden blood loss compared to intracapsular fractures. Our larger sample size and use of multivariate analysis provide more robust evidence supporting this association, strengthening its generalisability and clinical relevance.
Advanced age also demonstrated a clear relationship with increased preoperative blood loss, specifically for patients over 85 years. This threshold effect may reflect age-related haemostatic changes that accelerate in elderly patients, including decreased platelet counts (falling by ~20,000 platelets/μL after age 70) 20 and compromised vascular integrity with endothelial dysfunction leading to increased vascular permeability, reduced vascular tone, and altered expression of haemostatic regulators including von Willebrand factor, nitric oxide, and thrombomodulin.21,22 Interestingly, patients aged 65–85 years showed no increased risk compared to younger patients, suggesting that these age-related changes may not be clinically significant until very advanced age, when their cumulative effect becomes more pronounced.
Regarding time to surgery, our analysis revealed a progressive relationship between surgical delay and the risk of preoperative blood loss. While patients undergoing surgery 12–24 hours after admission showed only a trend toward increased bleeding risk, those operated on after 24–48 hours had significantly higher odds of substantial preoperative blood loss compared to those treated within 12 hours. This progressive increase likely reflects ongoing haemorrhage from the fracture site over time. These findings support efforts to minimise time to surgery when feasible, particularly as delays beyond 24 hours appear independently associated with increased bleeding risk.
Anticoagulant and antiplatelet medications were not independently associated with substantial preoperative blood loss in multivariate analysis (Table 2). While patients on these medications might be expected to have increased bleeding, the lack of association may be explained by several factors. First, these medications are often discontinued upon hospital admission, limiting their preoperative effect. Second, the amount of bleeding from the fracture itself may be greater than any additional effect from these medications. Third, the practice of delaying surgery in anticoagulated patients may have allowed medication effects to diminish. Similarly, comorbidity burden (CCI and ASA classification) was not independently associated with preoperative blood loss after controlling for age and fracture type, suggesting that fracture-related factors are more important than patient comorbidities in determining bleeding risk.
Our propensity-matched analysis revealed that substantial preoperative blood loss (ΔHb ⩾2 g/dL) has significant clinical implications. The proportion of patients requiring at least 1 unit of packed red blood cells during hospitalisation was more than twofold higher in patients with substantial preoperative blood loss. While this difference is expected, the findings of this study highlight the clinical significance of increased preoperative bleeding in hip fracture patients, especially considering the vulnerability of this elderly population to transfusion-related complications.13,23 Additionally, the significantly longer hospital stay in patients with substantial preoperative blood loss has important clinical and economic implications. Whilst we cannot exclude the possibility that postoperative complications contributed to this difference, our propensity-matched design accounted for baseline differences, and similar readmission rates between groups suggest comparable major complications. The extended hospitalisation more likely reflects the cumulative effect of preoperative anaemia on recovery. This finding aligns with previous studies demonstrating that perioperative anaemia is associated with prolonged hospitalisation in hip fracture patients.24,25 Furthermore, prolonged hospitalisation has mortality implications, as Haddad et al. 26 demonstrated that longer hospital stay was an independent factor associated with increased 6-months mortality after hip fracture, strengthened by data reported by Nikkel et al., 27 who found that shorter hospital stay was associated with lower mortality rates. Given the substantial economic burden of hip fracture care, 28 this length of stay increase represents significant healthcare expenditure that could potentially be mitigated through targeted preoperative haemostatic interventions in high-risk patients identified by our predictive factors.
Nearly half of our cohort (49.1%) experienced substantial preoperative blood loss, highlighting the clinical significance of this often-overlooked issue. Similar frequencies have been reported in previous studies, with Foss and Kehlet 4 documenting significant preoperative Hb drops in 45% of hip fracture patients. This high prevalence, along with the clinical consequences demonstrated in our study and others, highlights the need for greater attention to this phase of blood loss. While intraoperative bleeding in orthopaedic surgery is routinely addressed through established protocols – such as controlled hypotension, intraoperative cell salvage, topical haemostatic agents, and antifibrinolytic medications,5 –8 preoperative blood loss in hip fractures has received comparatively little focus and lacks standardised management strategies. This gap in clinical practice is notable given the substantial contribution of preoperative haemorrhage to overall blood loss reported in several studies,3,4,19 and its potential impact on outcomes. Developing targeted protocols to address preoperative bleeding, particularly in high-risk patients, may represent a valuable opportunity to improve perioperative care and reduce transfusion burden.
Whether earlier administration of TXA in the care pathway might attenuate preoperative Hb decline warrants prospective investigation. TXA administration has become standard practice at many institutions for managing intraoperative bleeding, with well-established efficacy for reducing surgical blood loss.29 –31 However, its application is typically limited to the surgical phase, missing the opportunity to mitigate preoperative blood loss. Based on our findings, a targeted prophylactic approach using TXA for patients at higher risk of substantial preoperative blood loss could be considered. Specifically, elderly patients (>85 years) with extracapsular fractures might benefit from haemostatic interventions earlier in their care pathway.
From a pharmacokinetic perspective, any early TXA administration would need to account for its plasma half-life of approximately 2–3 hours. 32 With typical ED-to-OR times of 24–28 hours in our cohort, a single early dose would not maintain therapeutic levels into the operative period, necessitating a second dose for intraoperative coverage. The principles of early haemostatic intervention are supported by evidence from trauma care.33,34 For example, the CRASH-2 trial demonstrated that early administration of TXA (within 3 hours of injury) in trauma patients significantly reduced mortality from bleeding without increasing the risk of thromboembolic events. 33 While hip fractures represent a different mechanism of injury than major trauma, whether principles of early haemostatic intervention apply to this population warrants further investigation, particularly for fracture types with greater bleeding risk.
This study has several limitations. Initially, its retrospective design introduces potential for selection bias and unmeasured confounders, though our propensity score analysis partially mitigates these concerns. Importantly, we quantified blood loss indirectly using Hb changes (ΔHb), which is a surrogate measure that can be substantially influenced by perioperative fluid administration, haemodilution, and third-space fluid shifts, absolute volumes of blood loss were not directly measured. . Our findings should therefore be interpreted as associations with preoperative Hb decline rather than with directly quantified haemorrhage. Despite this limitation, Hb monitoring remains a widely accepted and practical method for estimating blood loss in clinical settings, offering an accessible and consistently applied tool in both research and practice. Moreover, the lack of data regarding time from injury to ED arrival could influence baseline Hb levels. Due to the retrospective nature of the study and the absence of routinely collected data on this time interval, we were unable to account for this variable. However, our institution is an urban tertiary centre serving a predominantly metropolitan population, where transport times are typically short. Although some patients may have experienced longer delays, we believe this represents a small proportion of the cohort and is unlikely to have significantly affected our findings. Furthermore, this was a single-centre study conducted within a specific institutional context, which may limit the generalisability of our findings. Validation in multicentre studies or diverse healthcare settings would strengthen the external validity of our results. In addition, although our cohort size was substantial, it may still have been underpowered to detect statistically significant differences in less frequent outcomes such as mortality and hospital readmissions. Larger sample sizes or pooled datasets may be necessary to more definitively assess these associations. The 69 patients (2.7% of initially screened) who received preoperative transfusions were excluded to avoid measurement error. These patients had significantly lower admission Hb (9.2 vs. 12.4 g/dL, p < 0.001), higher ASA 3–4 classification (85.5% vs. 60.7%, p < 0.001), and worse outcomes including 1-year mortality of 30.4% vs. 15.4% (p = 0.001), representing a high-risk population and constituting a distinct group from typical hip fracture patients, requiring separate investigation. Finally, whilst we identified factors associated with preoperative blood loss and related clinical outcomes, our study does not evaluate specific interventions to address this bleeding phase. Further research is needed to develop and assess targeted strategies aimed at minimising preoperative blood loss and improving patient outcomes.
Conclusion
In this study, extracapsular fracture type, advanced age (>85 years), and prolonged time to surgery (>24 hours) were associated with substantial preoperative Hb decline in hip fracture patients. Substantial preoperative Hb decline was associated with increased transfusion requirements and prolonged hospitalisation. Whether closer preoperative Hb monitoring or targeted haemostatic strategies improve outcomes in these high-risk subgroups may warrant further investigation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.