
Abstract
Background:
Although a few studies have assessed cosmetic outcomes following total hip arthroplasty (THA), none have investigated their association with hip-specific patient-reported outcome measures (PROMs). This study aimed to investigate the relationship between cosmetic outcomes and PROMs following THA.
Methods:
We included 139 cases of primary THAs for osteoarthritis of the hip with a follow-up period of at least 1 year. Cosmetic outcomes were evaluated using the Patient Scar Assessment Scale (PSAS) from the Patient and Observer Scar Assessment Scale. PROMs were assessed using the Forgotten Joint Score-12 (FJS-12) and Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ). Correlations between cosmetic outcomes and PROMs were analysed.
Results:
The mean follow-up period after THA was 24 months. The PSAS total score was negatively correlated with the FJS-12 total score (r = −0.430, p < 0.001) and JHEQ total score (r = −0.243, p = 0.004). Among the JHEQ subscales, negative correlations were observed with the pain (r = −0.221, p = 0.009) and mental (r = −0.288, p < 0.001) subscales.
Conclusions:
Better cosmetic outcomes were associated with better PROMs after THA. However, the direction and clinical importance of the association remain unclear and warrant further investigation.
Keywords
Introduction
Total hip arthroplasty (THA) is a highly effective surgery performed to relieve joint pain and disability due to degenerative joint diseases and trauma, and the number of THAs has been increasing annually. 1 Various methods are used to assess outcomes after THA; however, patient-reported outcome measures (PROMs) have been increasingly emphasised, and studies using this method are increasing. 2 Various factors are predictors of PROMs after THA.3,4 While 90% of patients are satisfied after THA, 10% remain dissatisfied,5,6 making it crucial to address and improve the factors affecting PROMs in the future.
The surgical wound after THA is a highly visible area for patients and can be easily self-assessed. There are various surgical approaches for THA, and each one has different reported outcomes. While the incision site varies depending on the approach, few studies have detailed the exact location and length of the skin incision.1,7 Moreover, most studies evaluating the surgical wound after THA have focused on the incidence of surgical site infection, and relatively few have assessed cosmetic outcomes.8,9 Consequently, the relationship between cosmetic outcomes and postoperative PROMs remains unclear after THA.
We hypothesiaed that subjective cosmetic outcomes would be correlated with PROMs following THA. In this study, we aimed to investigate the relationship between the cosmetic outcome and PROMs following THA and identify predictors of the cosmetic outcomes.
Methods
This study was approved by our institutional review board (IRB) (approval date: 21 February 2008; IRB number 1280), and all patients provided written informed consent.
Study design and population
Between May 2019 and April 2023, 243 hips underwent THA at our institution. The inclusion criterion for this study was patients who had undergone primary THA only for osteoarthritis (OA) of the hip, and a total of 150 hips met this criterion. The exclusion criteria were a history of previous surgery to the hip (0 hip), loss to follow-up within 1 year of surgery (11 hips), lack of complete questionnaire (0 hip), and need for reoperation during the follow-up period because accurate wound assessment could not be performed (0 hip). Finally, 139 THAs in 121 patients were included in the analysis.
Surgical procedure and perioperative management
Two experienced arthroplasty surgeons performed all THAs, and the surgical approach, either the modified Watson-Jones approach or the direct lateral approach,10,11 was selected on the basis of the surgeon’s preference. The acetabular and femoral components were selected as cementless THA, and cemented stems were used only in cases where press-fit was difficult. In the modified Watson-Jones approach, with the patient in the supine position, an 8-cm oblique incision was made along the anterior edge of the tensor fasciae latae, with the proximal end slightly anterior. The proximal end did not extend beyond the inguinal crease; if further exposure was needed, the incision was extended distally (Figure 1(a)). After the skin incision, the joint capsule was approached through the intermuscular interval between the tensor fasciae latae and gluteus medius. In the direct lateral approach, with the patients in the lateral decubitus position, a 10-cm incision was made, centered over the most lateral prominence of the greater trochanter, with 5 cm proximally and 5 cm distally. The proximal end was an oblique incision angled posteriorly, whereas the distal end was positioned over the anterior edge of the femur. If further exposure was needed, the incision was extended proximally and distally (Figure 1(b)). The anterior ⅓ of the gluteus medius was incised and retracted anteriorly to expose the joint capsule.
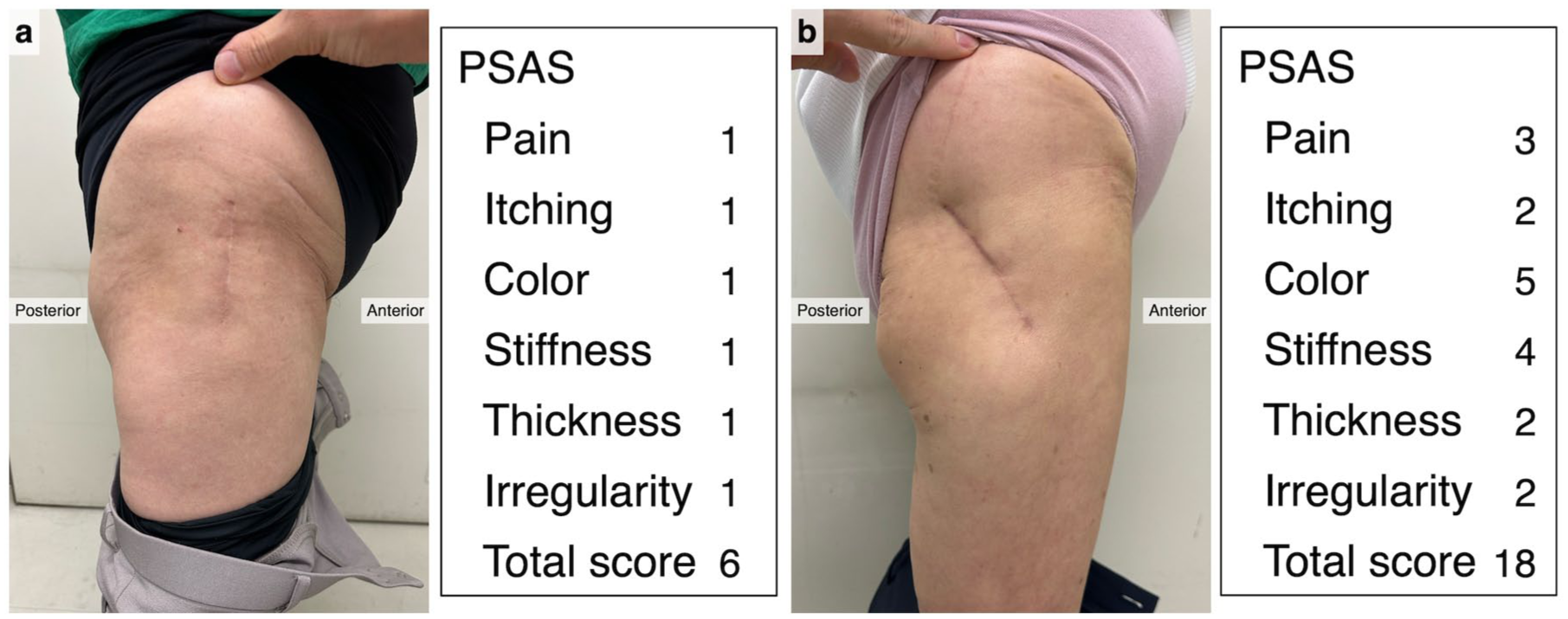
Representative photographs of a patient’s wounds after THA along with the PSAS scores (a) Photograph of the modified Watson–Jones approach, and (b) photograph of the lateral direct approach, both taken with the patient in the standing position. The PSAS is a subjective wound assessment tool evaluated by patients, and it consists of 6 items each scored from 1 (normal skin) to 10 (worst scar imaginable).
In both approaches, the joint capsule was preserved, and acetabular and femoral components were implanted. After implantation, the joint capsule was repaired with polyfilament sutures (Vicryl Plus 0; Johnson & Johnson, New Brunswick, NJ). Subsequently, the fascia was closed using polyfilament sutures (Vicryl Plus 0; Johnson & Johnson), and subcuticular skin closure was performed using single-stitched interrupted monofilament sutures (PDS II 3-0; Johnson & Johnson). After subcuticular skin closure, the skin was protected with wound tape (Steri-Strip, 3M, Saint Paul, MN and Opsite Post-Op Visible, Smith & Nephew, London, UK) in both groups. Following the clinical pathway, all patients were admitted to the hospital several days before THA and remained hospitalised for 3 weeks postoperatively, during which they underwent a standardised physical therapy regimen with full weight-bearing on postoperative day 1. The wound tape was routinely removed at 2 weeks postoperatively. After hospital discharge, the patients were scheduled for regular clinical evaluations at 3, 6, and 12 months following THA and every 1 year thereafter.
Outcome measures
The following preoperative patient characteristics were collected: age, sex, body mass index (BMI), American Society of Anesthesiologists score, 12 number of other comorbidities, 13 and severity of OA by Kellgren–Lawrence grade. 3 The number of other comorbidities referred to the presence of the following: heart disease, hypertension, diabetes, gastrointestinal disease, lung disease, renal failure, liver disease, and neurological disease. 3 Additionally, the percentages of smokers and those with diabetes, which have been reported to affect wound healing,14,15 were also collected.
Preoperative PROMs were assessed using the Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ) 16 and Central Sensitization Inventory (CSI). 17 The JHEQ is a self-reported questionnaire used to evaluate clinical outcomes of hip disease and includes pain (28 points), movement (28 points), and mental (28 points) subscales. The total score ranges from 0 to 84 points, where higher scores indicate a better outcome. The CSI is a validated tool used to identify symptoms associated with central sensitisation syndromes, including persistent pain and heightened pain sensitivity. A CSI score ⩾40 is considered indicative of central sensitisation. 18
Intraoperative data, including the length of skin incision, surgical approach, operative time, and intraoperative blood loss, were collected. Postoperative cosmetic outcomes were assessed using the Patient Scar Assessment Scale (PSAS) from the Patient and Observer Scar Assessment Scale (version 2.0) at the final follow-up after THA. 19 The PSAS is a subjective wound assessment tool evaluated by patients that consists of six items: pain, itching, color, stiffness, thickness, and irregularity. Each item is scored from 1 (normal skin) to 10 (worst scar imaginable), with the highest or best possible score of 6 and the worst possible score of 60 points. Postoperative PROMs were assessed using Forgotten Joint Score-12 (FJS-12) 20 and JHEQ at the final follow-up. The raw FJS-12 score was transformed to a linearly scaled score from 0 to 100, using the following formula: final total score = 100 − ([sum{item 1 to item 12} − 12] / 48 × 100). 21
The primary outcome was the PSAS score at the final follow-up after THA, and the secondary outcomes were the FJS-12 and JHEQ scores at the final follow-up after THA. The relationship between the PSAS score and PROMs (FJS-12 and JHEQ scores) after THA was evaluated, and the factors associated with the cosmetic outcome (PSAS score) were also investigated.
Statistical analysis
Continuous variables are described as means and standard deviations, whereas categorical variables are expressed as absolute frequencies and percentages. Correlations between the PSAS total score and PROMs (FJS-12 and JHEQ scores) were analysed using Spearman rank correlation coefficients. Additionally, to investigate the predictors of the cosmetic outcome, multiple linear regression analysis was conducted with the PSAS total score as the dependent variable and age, sex, BMI, smoking, diabetes, CSI, follow-up period, length of skin incision, surgical approach, operative time, and intraoperative blood loss as independent variables. The sub-analysis comparing the PSAS score between different approaches was performed using the Mann–Whitney U test. Statistical significance was set at p < 0.05, and statistical analyses were conducted using R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient demographics are presented in Table 1, and the mean follow-up period after THA was 24 months. Cosmetic outcomes and PROMs at the final follow-up are presented in Table 2. The PSAS total score was negatively correlated with the FJS-12 total score (r = −0.430, p < 0.001) and JHEQ total score (r = −0.243, p = 0.004) (Table 3). Among the JHEQ subscales, the PSAS total score was negatively correlated with the pain (r = −0.221, p = 0.009) and mental subscales (r = −0.288, p < 0.001), excluding movement.
Patient demographics.
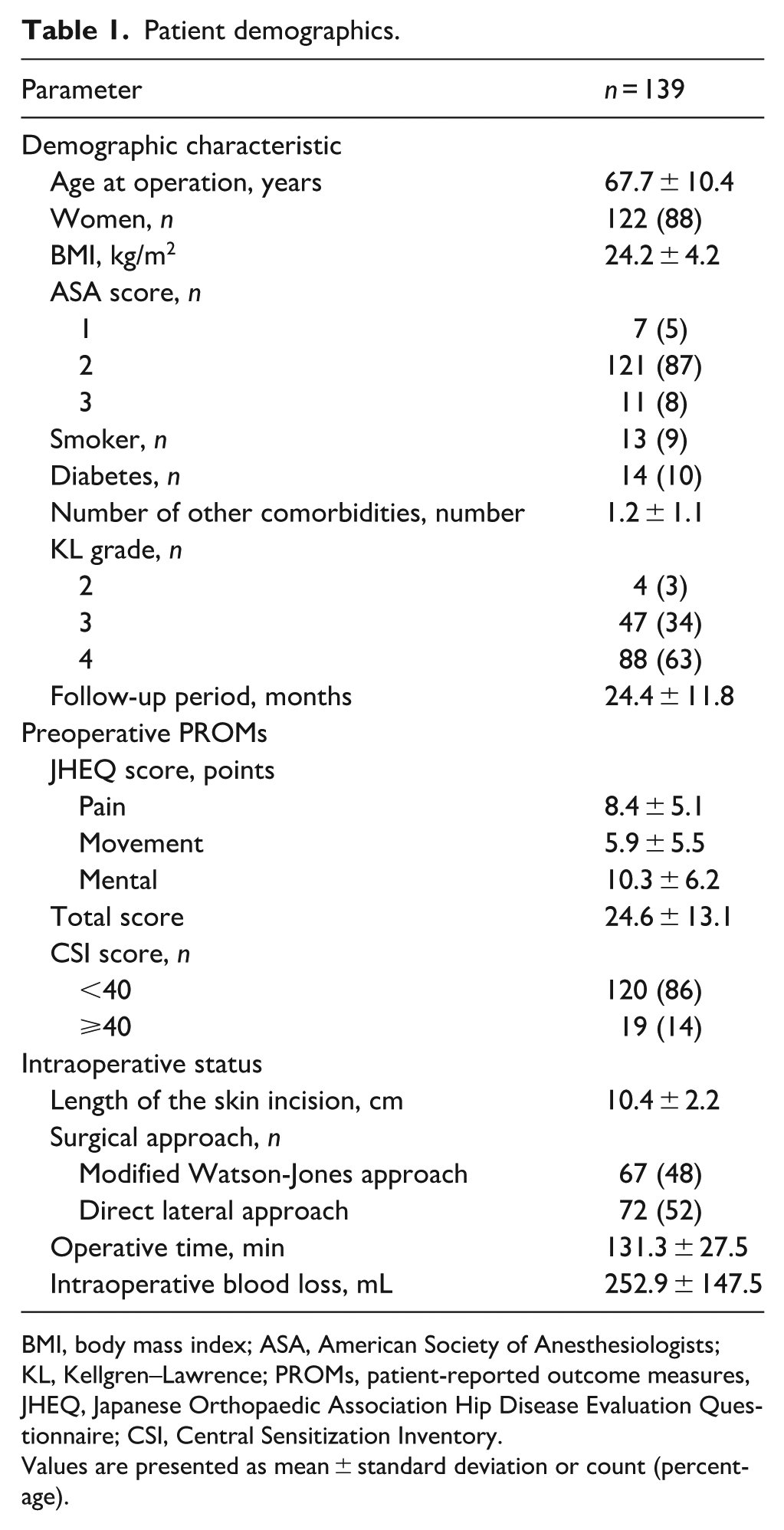
BMI, body mass index; ASA, American Society of Anesthesiologists; KL, Kellgren–Lawrence; PROMs, patient-reported outcome measures, JHEQ, Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; CSI, Central Sensitization Inventory.
Values are presented as mean ± standard deviation or count (percentage).
Cosmetic outcomes and PROMs at the final follow-up after THA.
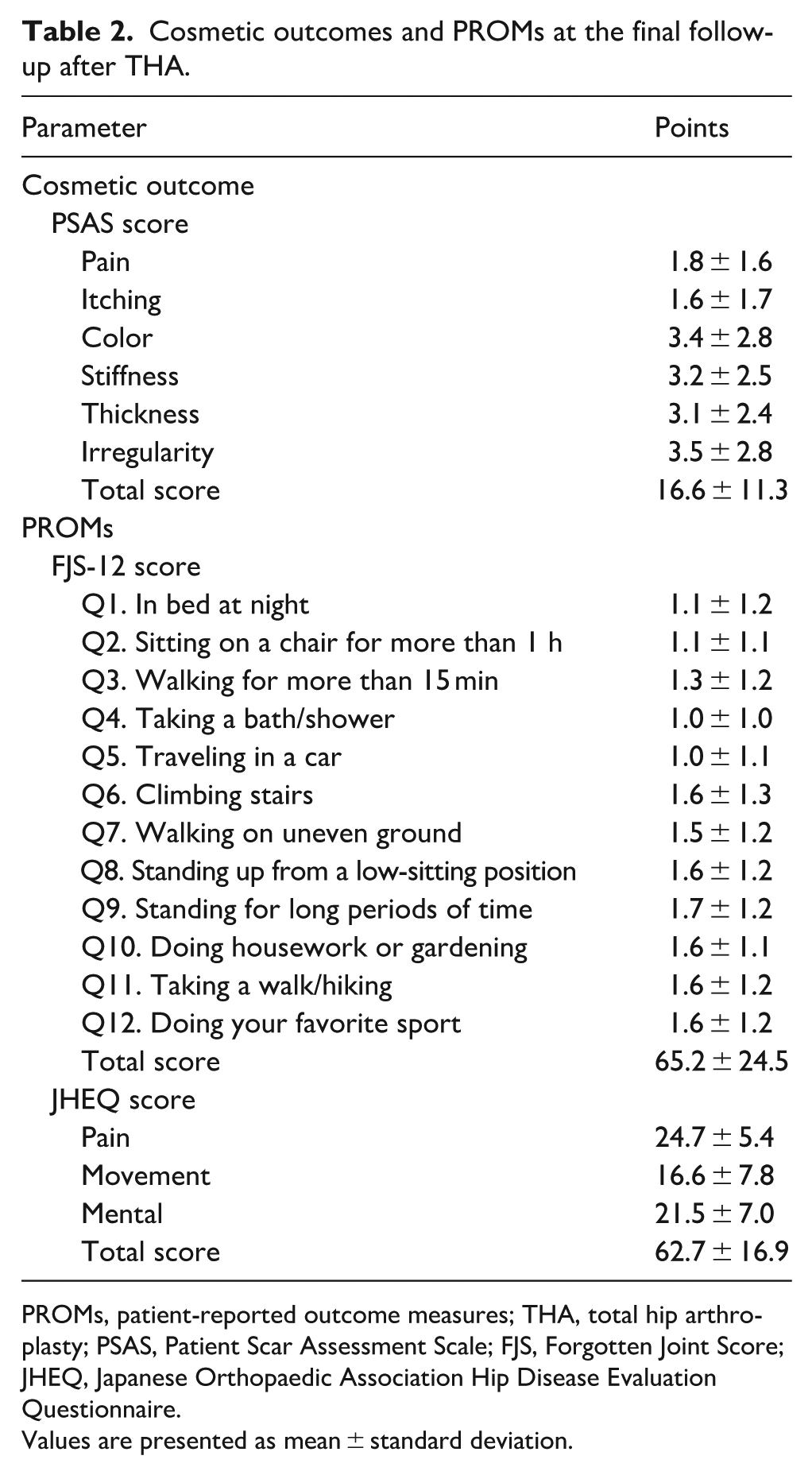
PROMs, patient-reported outcome measures; THA, total hip arthroplasty; PSAS, Patient Scar Assessment Scale; FJS, Forgotten Joint Score; JHEQ, Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire.
Values are presented as mean ± standard deviation.
Correlations between the cosmetic and clinical outcomes at the final follow-up year after THA.
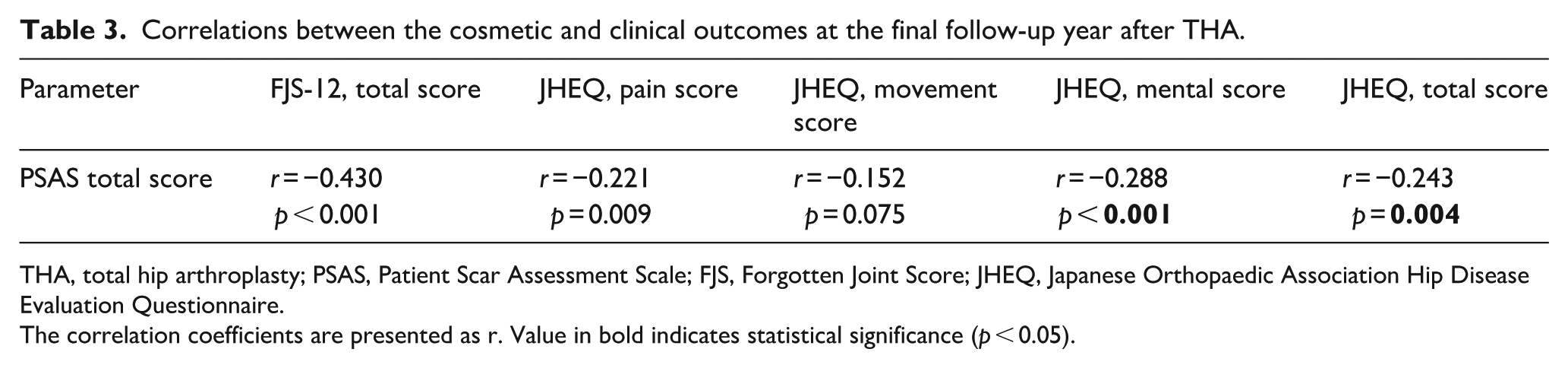
THA, total hip arthroplasty; PSAS, Patient Scar Assessment Scale; FJS, Forgotten Joint Score; JHEQ, Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire.
The correlation coefficients are presented as r. Value in bold indicates statistical significance (p < 0.05).
Multiple linear regression analysis showed that only surgical approach was a predictive factor for the PSAS total score after THA, with a partial regression coefficient of 8.0 (95% confidence interval, 1.5 to 14.5; p = 0.017) for the direct lateral approach (Table 4). According to the sub-analysis, patients who underwent surgery with the modified Watson–Jones approach showed better PSAS scores than those who underwent surgery with the direct lateral approach in the pain, itching, stiffness, thickness, and irregularity items as well as in the total score (Table 5) (Figure 1).
Results of the analysis of factors predictive of the PSAS total score at the final follow-up after THA.
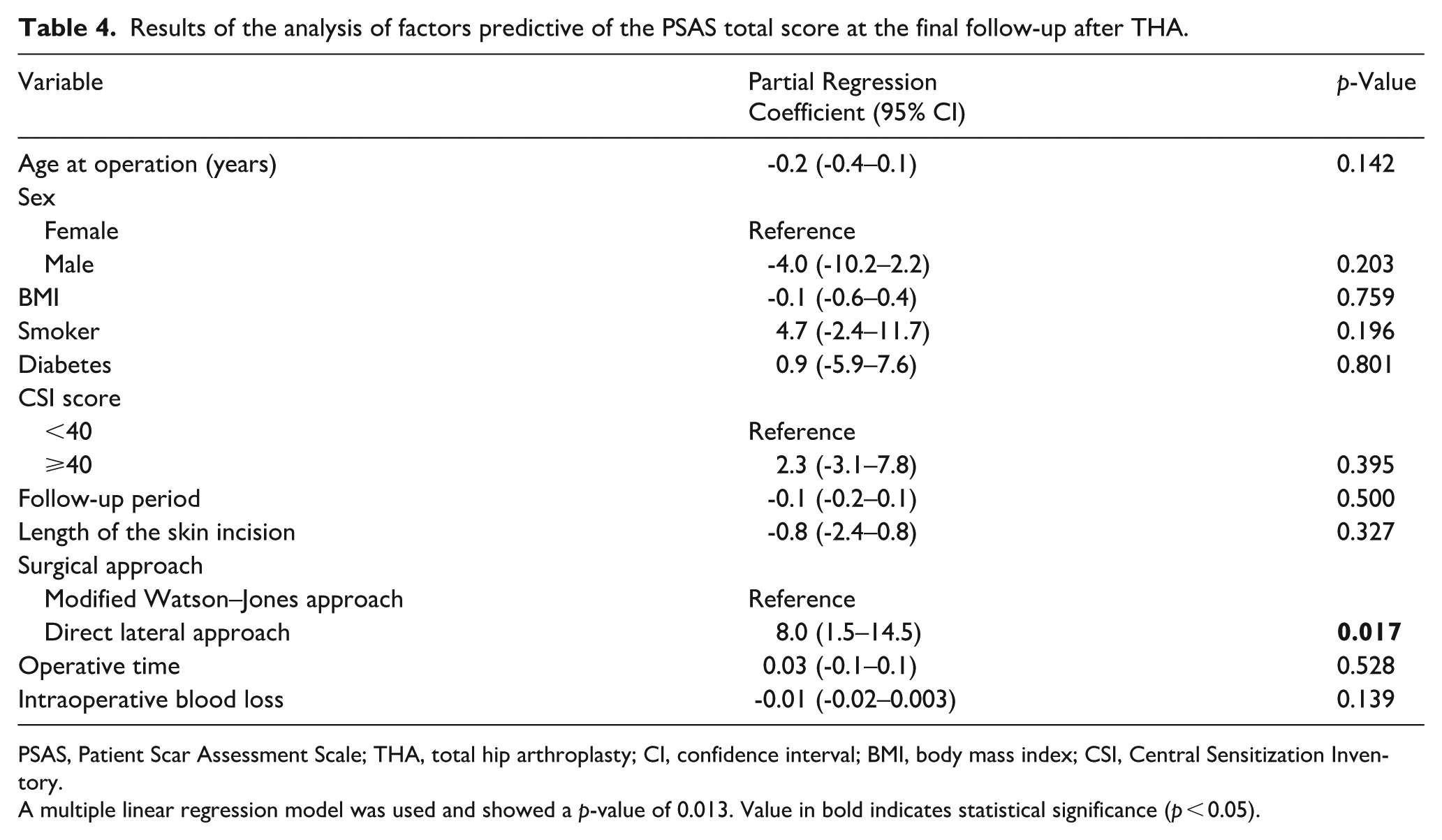
PSAS, Patient Scar Assessment Scale; THA, total hip arthroplasty; CI, confidence interval; BMI, body mass index; CSI, Central Sensitization Inventory.
A multiple linear regression model was used and showed a p-value of 0.013. Value in bold indicates statistical significance (p < 0.05).
Comparison of PSAS scores between the 2 approaches.
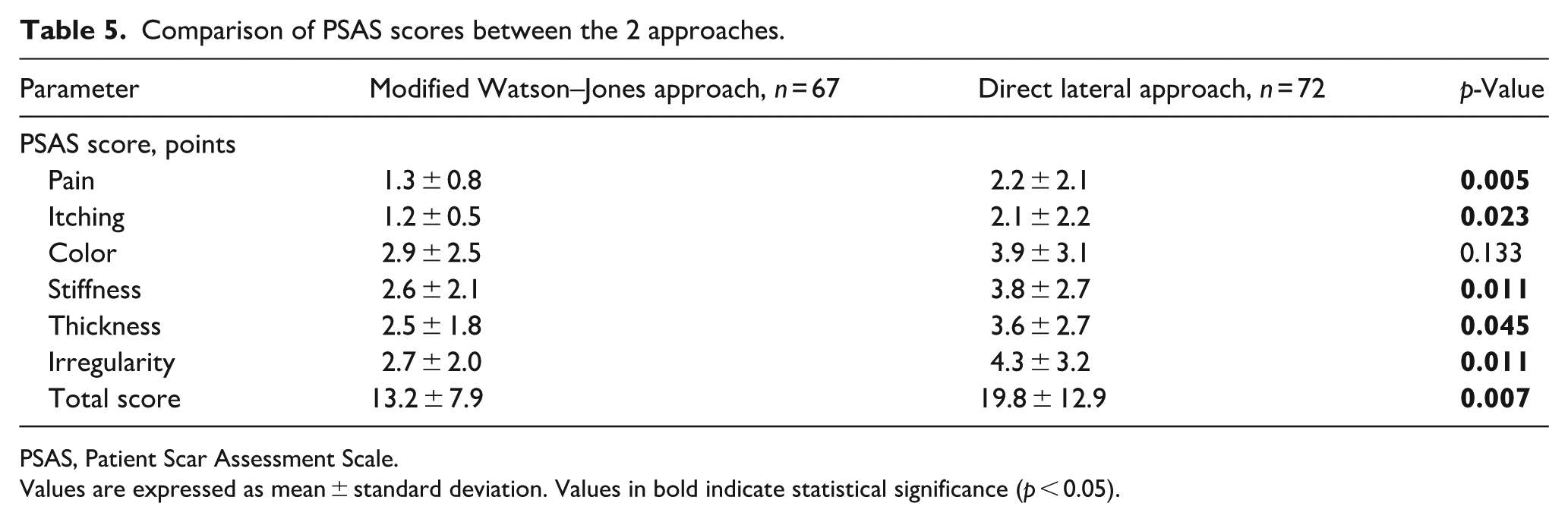
PSAS, Patient Scar Assessment Scale.
Values are expressed as mean ± standard deviation. Values in bold indicate statistical significance (p < 0.05).
Discussion
This study confirmed our hypothesis that subjective cosmetic outcomes were correlated with PROMs after THA. The present study demonstrated that the PSAS score was negatively correlated with the FJS-12 and JHEQ scores, suggesting that better cosmetic outcomes were associated with better PROMs after THA. Furthermore, the surgical approach was associated with the cosmetic outcome. To our best knowledge, this is the first study to investigate the relationship between cosmetic outcomes and PROMs after THA.
This study showed that the PSAS score was correlated with the FJS-12 score, which is a PROM used to evaluate a patient’s ability to forget the artificial joint in everyday life. 20 Discomfort at the surgical site may lead to discomfort in the hip joint, potentially worsening the FJS-12 score. Additionally, the PSAS score was correlated with the pain and mental subscales of the JHEQ but not with the movement subscale. The PSAS contains a pain item, and as wound pain contributes to the clinical outcome of pain, this might explain the correlation between the PSAS and JHEQ pain scores. Since the PROMs such as the Hip Disability and Osteoarthritis Outcome Score 22 and Oxford Hip Score, 23 which are often used to evaluate postoperative THA outcomes, include pain items, they might be influenced by the PSAS. Furthermore, PROMs are influenced by the patient’s mental condition.4,17,24 Surgical wound dehiscence has a negative impact on the patient’s mental health, 25 which in turn could have influenced the PROMs after THA. However, the opposite effect is also plausible. Patients who feel better overall, experience less pain, or are more satisfied with their surgical outcome may tend to perceive their surgical scar more favorably than their counterparts, rather than scar appearance directly influencing PROMs. Additionally, the observed correlation explains only approximately 18% of the variance in PROMs, indicating a modest association. Therefore, the direction and clinical significance of the relationship between cosmetic outcomes and PROMs remain unclear and warrant further investigation.
The only predictor of the PSAS score was surgical approach, and the modified Watson-Jones approach had better PSAS scores than the direct lateral approach in the items of pain, itching, stiffness, thickness, and irregularity. 2 main factors may explain this difference. First, the direct lateral approach involves a skin incision directly over the greater trochanter, which may lead to wound irritation and increase the risk of developing trochanteric bursitis. 26 This may have contributed to increased postoperative discomfort, resulting in higher pain and itching scores. Second, the modified Watson-Jones approach uses a more anteriorly placed incision, which is less affected by tensile forces during hip flexion. Incisional tension has been reported as a risk factor for hypertrophic scars and keloid formation.27,28 Therefore, reduced tension in the modified Watson-Jones approach may have resulted in better cosmetic outcomes in terms of stiffness, thickness, and irregularity. These findings suggest that the location and orientation of the skin incision, rather than the surgical approach itself, may play a more critical role in determining postoperative wound cosmesis.
This study has some limitations. First, it only included patients with OA. We excluded those with rheumatoid arthritis or idiopathic osteonecrosis, who may be receiving steroid therapy that could affect cosmetic outcomes. By focusing on only OA, we believe that we minimised the influence of the medication. Second, only 2 types of surgical approaches were examined. Considering that our findings suggested the association between cosmetic outcomes and other surgical approach, further research is needed to evaluate the impact of different incision types on cosmetic outcomes after THA. Third, the study population consisted exclusively of Japanese patients. Because perceptions and expectations of scar cosmesis can differ by culture and ethnicity, generalisability of our study findings to other populations may be limited. Further evaluation in more diverse cohorts is needed. Fourth, pain is included as one of the PSAS items and is also captured in the PROMs used in this study. Although the pain item in the PSAS primarily reflects wound-related pain, whereas the pain domain in the PROMs represents overall joint or activity-related pain, some degree of overlap may exist between the 2. This partial overlap in measurement domains could have contributed to the observed correlations between cosmetic outcomes and PROMs. Fifth, although the surgical approach was associated with cosmetic outcomes, we could not clarify the effects of incision location and skin tension. Future studies designed to analyse these aspects are warranted. Lastly, although we observed a significant association between cosmetic outcomes and PROMs, the cross-sectional study design precludes any inference regarding causality. As discussed earlier, it is possible that patients with favorable PROMs may also tend to perceive their cosmetic outcomes more positively than those with unfavorable PROMs. Therefore, further studies are needed to clarify the causal relationship between these factors.
In conclusion, favourable cosmetic outcomes were correlated with favourable PROMs after THA, although the strength of this association was modest. There were also differences in cosmetic outcomes depending on the surgical approach. Given the cross-sectional nature of this study, the direction and clinical importance of the association between cosmetic outcomes and PROMs remain unclear and warrant further investigation.
Footnotes
Acknowledgements
We are grateful to Yoichi Ohta and Shigekazu Mizokawa for his assistance with the surgeries. We also thank the medical staff at the institution for their help with data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.