
Abstract
Background:
2-stage revision arthroplasty remains the current gold standard for treatment of chronic periprosthetic joint infection (PJI) of the hip and knee in the United States. Rates of infection eradication have been shown to vary from 60% to 91%. The purpose of this study was to determine the true fate the of 2-stage exchange protocol for PJI using an updated classification system for PJI treatment outcomes as well as the effect of systemic host and local extremity grades on outcomes.
Methods:
A retrospective review of a PJI registry was performed from a single institution from January 2010 through December 2021. All patients having undergone a planned 2-stage exchange after primary or revision total knee arthroplasty (TKA) and total hip arthroplasty (THA) for chronic PJI defined by Musculoskeletal Infection Society criteria were included. Perioperative variables and tiered outcome at final follow up were collected.
Results:
In total, 589 cases (561 patients) met final inclusion criteria and were included in the analysis. 394 cases (66.9%) retained their implants at median follow-up of 3.7 years (IQR 1.8, 7.7). 311 cases (52.8%) underwent successful two-stage revision with prosthesis retention without ongoing use of suppressive antibiotics, while another 83 cases (14.1%) retained their prosthesis with use of suppressive antibiotics. 152 cases (25.8%) underwent subsequent septic or aseptic revision, amputation, arthrodesis, spacer retention while 40 (6.8%) died during the study period.
Conclusions:
At 3.7 years after surgery, 66.9% of 2-stage exchanges for PJI resulted in retained prosthesis with or without use of suppressive antibiotics. The remaining 33.1% of this population underwent additional surgery (25.8%), or were deceased (6.8%).
Introduction
The gold standard for treatment of chronic periprosthetic joint infection (PJI) in the United States remains 2-stage exchange for patients that are able to undergo this procedure.1,2 The overall success rate of 2-stage revision arthroplasty has been shown to vary from 60% to 91% in patients who successfully complete the second stage.3 –10 However, these success rates frequently do not report on patients who fail to complete the second stage, and therefore may overestimate the effectiveness of this treatment. Additionally, definitions of success have historically not been standardised. 2 prior studies have shown an attrition rate of 18–30% and a mortality rate of 5–24% after resection and spacer placement.3,11 In addition, many of these studies are based on small case series or national registries. Thus, the main purpose of this study was to identify the outcome of two-stage revision for chronic hip and knee PJI in a large patient group using a new standardised tiered outcome system that includes retention with antibiotic suppression, mortality, and attrition in between explant and reimplantation. 12 In addition, several host, surgical, and microbiologic factors also influence this success rate.3,5 A secondary objective of this study was to assess for factors predisposing to failure through the entire two-stage protocol.
Questions
With this study, we sought to determine the true fate of two-stage treatment of PJI. That is, how many patients retained their implant with and without suppressive antibiotics. We utilised a tiered outcome system to categorise success.
Additionally, we sought to determine which of the following variables correlated with reduced rates of failure following 2-stage revision for PJI: gender, age, host comorbidity type, or local extremity grade.
Material and methods
This study received ethical approval from Wake Forest University Health Sciences (IRB00085294) 6/5/2025-6/4/2026.
A retrospective review of a single institution PJI registry was performed to identify 791 cases (726 patients) (Figure 1). This represents a consecutive series of patients who underwent at least an arthroplasty resection in a planned 2-stage exchange after primary or revision total knee arthroplasty (TKA) or total hip arthroplasty (THA). Patients were also included if they had a previous 2-stage exchange or resection prior to referral. Patients included in the final analysis were those who had a PJI defined by Musculoskeletal Infection Society (MSIS) criteria. 13 Patients in this study underwent a first stage resection procedure between January 2010 and December 2021.
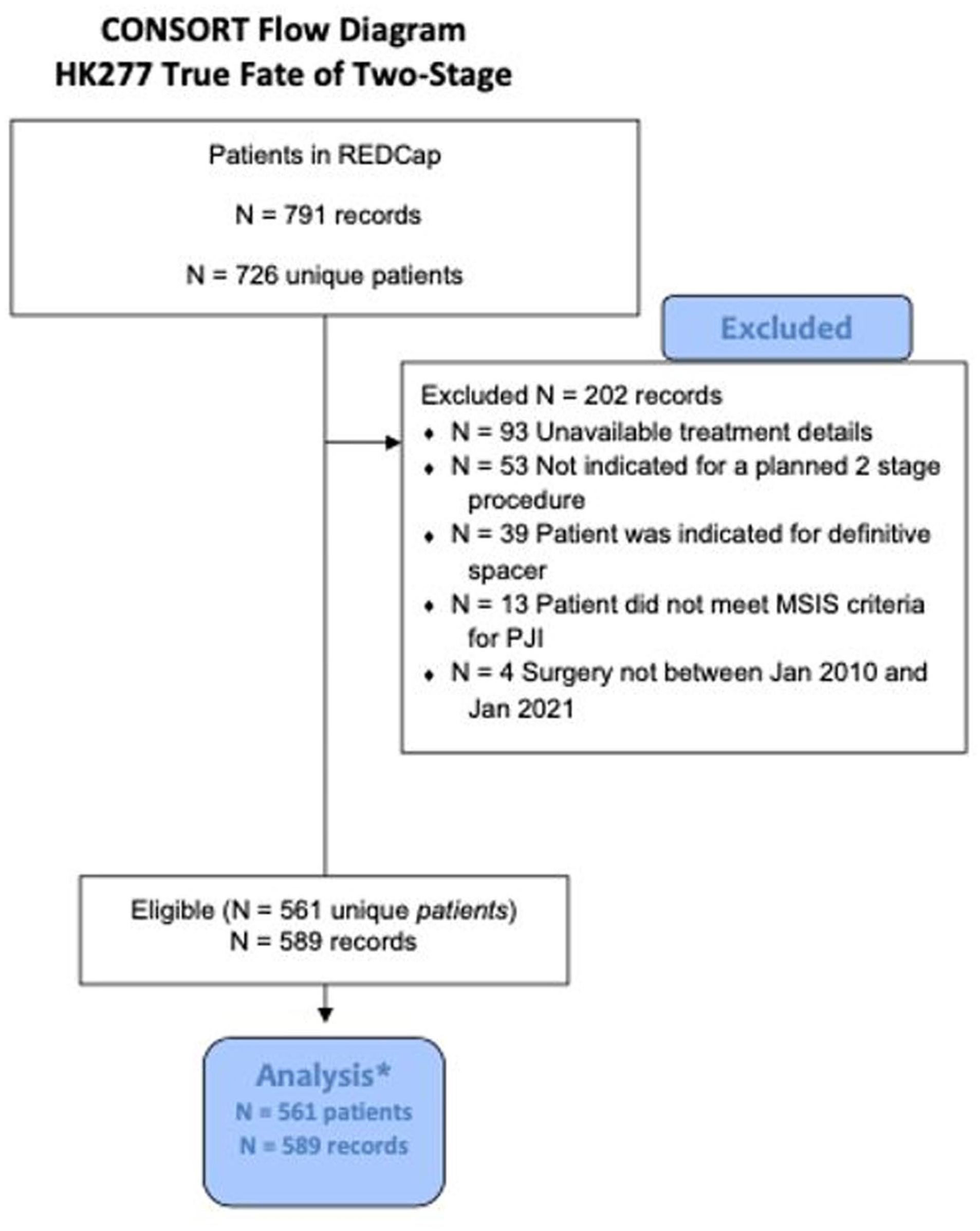
Consort Flow Diagram: HK277 True Fate of Two-Stage. Flow chart demonstrating the initial study population of 791 cases, exclusions according to our criteria, and the final study population of 589 cases.
Independent variables included basic demographics, surgical information, and organism data (Table 1) while dependent variables included the tiered outcome at final follow-up (Table 2).
Patient demographics.
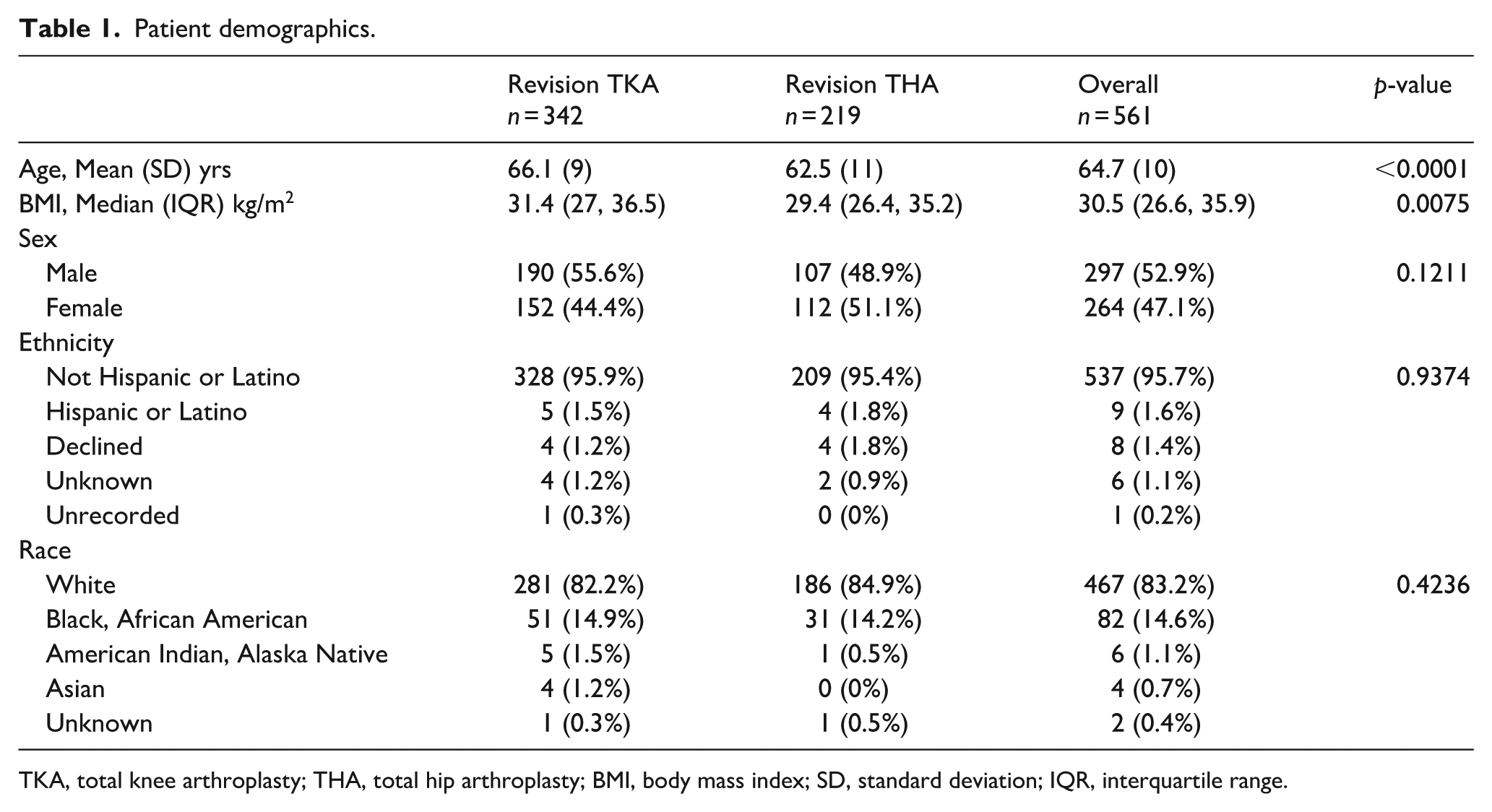
TKA, total knee arthroplasty; THA, total hip arthroplasty; BMI, body mass index; SD, standard deviation; IQR, interquartile range.
Tiered outcome at final follow-up.
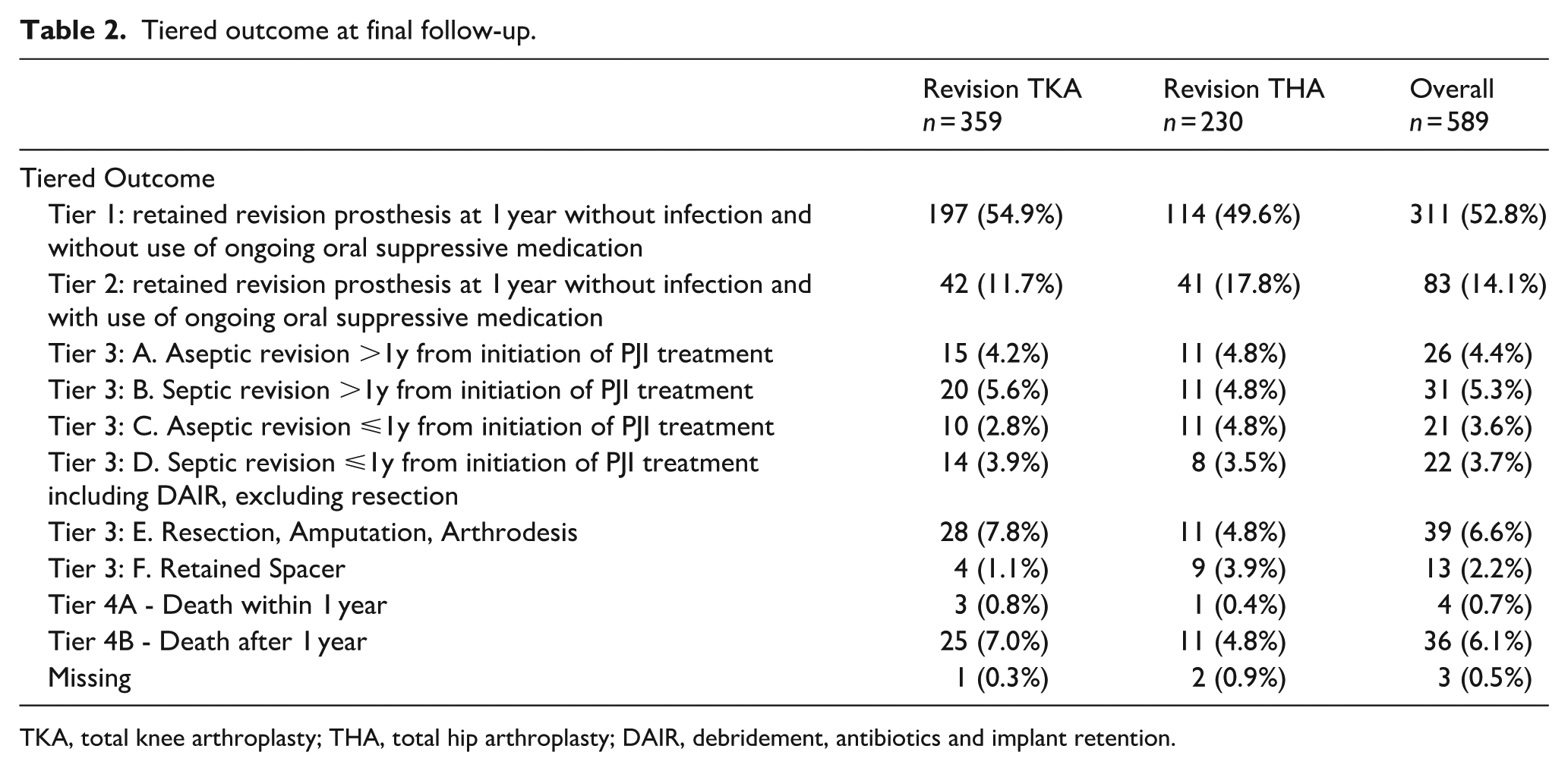
TKA, total knee arthroplasty; THA, total hip arthroplasty; DAIR, debridement, antibiotics and implant retention.
Patients were excluded if they were less than 18 years old, were indicated for a definitive spacer prior to resection, underwent planned single-stage revision, or if there was inadequate detail in the registry for analysis.
Details of the 2-stage exchange protocol are as follows: patients with a chronic PJI who were indicated for 2-stage exchange. In the first stage procedure, the resection, patients underwent debridement of synovium, all prosthetic material, and 2 mm of bone surfaces using a saw or reamer where appropriate. Canals were reamed. Cultures were obtained from synovial fluid, synovium, canals, and bony membranes to guide antimicrobial therapy. Patients then underwent irrigation of the joint with 3 separate 3L bags or normal saline under pulsatile lavage. Between saline lavages, the joint was soaked with dilute hydrogen peroxide, and then povidone iodine. All 2-stage procedures employed the use of a high dose antibiotic laden cement spacer, constructed using Palacos bone cement. Each pack of cement contained 2 grams of vancomycin and 2.4 grams of tobramycin to create the spacer with gram positive and negative local coverage. Number of packs used was determined on a case-by-case basis and was left to the treating surgeon’s discretion based on desired fixation and bone defects encountered during surgery. In all cases, patients received IV antibiotics via PICC line for 6 weeks. The choice of antibiotic was determined by operative cultures and in collaboration with infectious disease consultation. After 6 weeks of IV antibiotics, the patients went through a 2-week drug holiday at which point the patient underwent a complete infectious workup to determine candidacy for reimplantation. The criteria for reimplantation included negative cultures on joint aspiration, down trending ESR/CRP, healed wound with no erythema, and no clinical concern for ongoing infection. Results from workup were interpreted by the treating surgeon in conjunction with all clinical available information. After second stage reimplantation, the patients received a minimum 6 months of oral antibiotic guided by cultures and under the advice of a consulting infectious disease physician. Implant type, mode of fixation, use of cement was determined on a case-by-case basis according to the treating surgeon. Chronic indefinite oral suppressive antibiotic beyond 6 months was utilised based on patient and physician preference according to a discussion which incorporated benefits and risks.
Study data were collected and managed using REDCap electronic data capture tools hosted locally.14,15 REDCap (research electronic data capture) is a secure, web-based software platform designed to support data capture for research studies, providing: (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
Statistical methods
Basic descriptive statistics were used including frequency and proportions. Normality testing was performed by looking at histograms and quantile-quantile plots, as well as with Shapiro-Wilk tests. Medians and interquartile ranges (IQR) are reported for any continuous variable that violated the normality assumptions. For categorical variables, chi-square or Fisher’s exact tests were used as appropriately. For numerical variables, t-tests or Wilcoxon Rank Sum tests were used as appropriately. Multivariable logistic regression was used to determine the association of treatment failure after controlling for sex, age at surgery, McPherson systemic host and local extremity. 16 Statistical significance was set to p < 0.05. All analysis were made using SAS Version 9.4 (Cary, NC, USA).
Results
In total, 589 cases (561 patients) met final inclusion criteria and were included in the analysis. Of these, 359 cases (61.0%) were for knee PJI and 230 cases (39.0%) were for hip PJI. Of these, 550 (98%.0) underwent reimplantation. Median follow-up was 3.7 years (IQR 1.8, 7.7). 311 (52.8%) cases retained their prosthesis at one year without infection and without use of ongoing oral suppressive medications (Table 2). Another 83 (14.1%) of cases retained their prosthesis at 1 year without infection with ongoing use of oral suppressive medications.
The remaining 192 (29.6%) of patients met criteria for failure requiring aseptic revision, resection arthroplasty, amputation, arthrodesis, retained spacer, or death. Of these, 40 patients (6.8%) died during the study and met criteria failure.
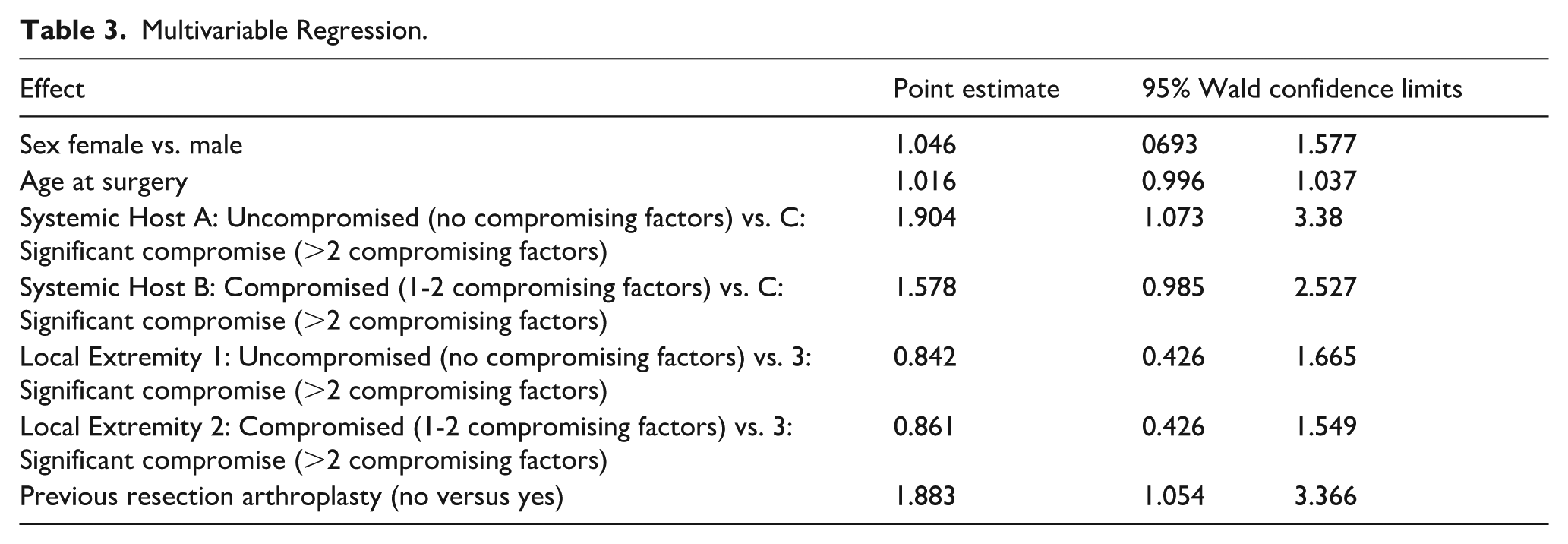
The logistic regression analysis showed that the patients with McPherson host grade A were less likely to fail when compared to patients with McPherson host grade C independent of the other variables in the regression model The logistic regression analysis also showed that patients with McPherson host grade B were less likely to fail when compared to patients with McPherson host grade C independent of the other variables in the regression model. A history of prior 2-stage revision arthroplasty for PJI was also an independent risk factor for failure, portending almost a two-fold higher risk of failure compared with patients who had no prior resection. Neither age, gender, or any of the other variables in the regression model were significant (Table 3).
Multivariable Regression.
Discussion
2-stage exchange remains the gold standard for treatment of chronic PJI, but much of the literature ignores the fact that a significant minority of patients fail to undergo the second stage altogether. We aimed to provide a more accurate picture of the outcome of 2-stage exchange by elucidating the attrition rate between stages, determining the reasons why patients fail to undergo the second stage, and describing the reasons for failure after reimplantation. With this data, better counsel can be offered to patients who present with chronic PJI and are indicated for 2-stage exchange. In this study, we found that only approximately 50% of patients who undergo a planned 2-stage exchange achieve infection-free second stage revision without suppressive antibiotics. Another 14% of patients achieved a symptom-free second stage revision with ongoing suppressive antibiotics. Another 25.8% of the patients met criteria for failure, having required repeat exchanges, debridement, or salvage operation. 40 (6.8%) patients died by final follow-up.
Petis et al. 6 reported on 164 hips who underwent two-stage exchange for PJI. At 1 year after reimplantation, 10% of patients met criteria for reinfection. By 15 years after reimplantation, 15% of patients were reinfected while another 11% were maintained on chronic antibiotic suppression. The same institution also analysed 245 knees with no prior history of infection who underwent 2-stage exchange for PJI. 5 At 1 year after surgery, 4% of patients met criteria for reinfection with an additional 9% of patients being maintained on chronic antibiotic suppression. Rates of reinfection continued to increase reaching 17% by year 15. Risk factors for reinfection included BMI > 30 kg/m2, McPherson host grade C, and prior surgery. This is supported by 2 other studies that have also reported increased risk with a BMI > 30 kg/m2 and a history of prior revision as risk factors for failure.17,18 Other risk factors noted in the literature include a history of a sinus tract, operative time >4 hours, or infection with enterococcus species.17,18 In contrast to these analyses, our study evaluated outcomes of 2-stage revision in all comers including those with a prior history of infection as well as those with articulating, non-articulating, and static spacers. Similar to our study, McPherson host grade correlated with risk of failure for knee infection. The McPherson extremity grade, however, did not reach significance in our study.
Nodzo et al. 8 evaluated 3 different types of articulating antibiotic spacers for PJI of the knee. The overall rate of infection eradication was 83%, but no significant difference was noted between the spacer subtypes. In 1 of the only prospective studies on 2-stage revision arthroplasty for knee PJI, Nahhas et al. 19 evaluated 68 patients who were randomised to placement of a static or articulating spacer. Improved range of motion (ROM) was noted in the articulating cohort. 6 patients died and 7 were lost to follow-up within 2 years. Cancienne et al. 20 evaluated a national database of Medicare patients undergoing spacer placement for chronic hip PJI. Of 7146 patients, 4301 (60.2%) were reimplanted at an average of 124 days after the first stage. The remaining patients passed away, required repeat debridement, underwent resection arthroplasty, or retained their spacer. Wang et al. 3 evaluated a single centre PJI registry of 616 patients indicated for 2-stage revision arthroplasty for PJI. Of 616 patients, 505 (82.0%) went on to the second stage. Of the 111 patients that did not undergo reimplantation, >½ were deemed medically unfit for a second operation. The remaining patients either opted to retain their spacer or underwent a salvage procedure. Another recent study assessing attrition found that only 61/89 (68.5%) of patients underwent reimplantation. 11 In contrast, 98% of patients in our study underwent reimplantation. We attribute this in part to the fact that patients in our study were treated at a dedicated PJI centre with organised protocols, standardised treatment algorithms, and multidisciplinary approach to care.
Toulson et al. 4 reported on their single institution experience with 2-stage revision arthroplasty for hip PJI. Out of 87 patients indicated for 2-stage revision, 82 (94.3%) underwent reimplantation. They further assessed for higher failure rates with multi-drug resistant organisms. No significant difference in eradication was noticed with 80 out of 84 original infections being cleared. The same institute later evaluated for increased failure rates in patients undergoing 2-stage exchange for knee PJI. 21 Of 75 infections indicated for 2-stage exchange, eradiation and reimplantation was achieved in 68 of cases (90.7%). Again, no difference was noted in success between organisms including multi-drug resistant bacteria. While not powered for this analysis, our study did not find a correlation with bacteria subtype and odds of failure.
Vadiee and Backstein 22 reported their outcomes after repeat 2-stage revision arthroplasty for recalcitrant PJI in 23 patients. At an average of four years post reimplantation, the success rate was 74% with 14 infection free cases. Kheir et al. 23 evaluated 40 patients who underwent repeat 2-stage revision arthroplasty for hip PJI. Of these, 61.6% achieved infection control with 13% of patients requiring chronic antibiotic suppression. Our study evaluated both first time infections as well as recurrent infections in patients who had undergone prior revision arthroplasty or debridement. Similar to this study, 14% of patients were maintained on chronic antibiotic suppression.
While the optimal protocol for antibiotic therapy continues to be elucidated, the importance of antibiotic treatment in the setting of PJI cannot be understated. In their award-winning study, Frank et al. 24 reported a significant decrease in PJI recurrence rates following 3 months of oral antibiotic treatment following second stage arthroplasty. Additional support for chronic antibiotic suppression was reported by Siqueira et al., 25 in which patients receiving 6 months of treatment following 2 stage revision or debridement, antibiotics and implant retention (DAIR) for PJI demonstrated a 27.4% increase in 5-year survival compared to the non-suppressed group. In another recent study on patients who were not candidates for surgical intervention, suppressive antibiotic treatment alone yielded infection control in 67% of patients at 21 months median follow-up. 26 Patients with non-tumour prostheses and patients with coagulase-negative staphylococcal infections demonstrated even better outcomes. The presence of a draining sinus tract portends a higher risk for non-operative treatment of PJI and failure of isolated antibiotic treatment with over 50% of patients requiring revision surgery or experiencing recurrent bacteraemia. 27 A more thorough investigation regarding the value of suppressive antibiotic therapy in the 2-stage cohort is currently underway.
There were several strengths of this investigation that should be highlighted. First, this is one of the largest cohorts of 2-stage exchange procedures published to date. Next, we included all patients indicated for 2-stage exchange, including those patients with a prior failed resection procedure, which makes the results more generalisable to complex referral practices. Additionally, we performed a detailed categorisation of failure mechanism, including failure to undergo the second-stage. This provides a more accurate description of the final destination for these patients. Finally, we utilised a well-established set of criteria for outcomes reporting, which will help position these outcomes in the greater context of PJI literature.
There are some limitations in current study worth noting. First, the data were collected in retrospective fashion, which leaves room for error. However, the registry from which the data was obtained has a full-time manager dedicated to the completeness and accuracy of the contents. Next, this study represents only data from a single centre of surgeons, so generalisability may be limited. However, our tertiary care centre draws referrals from a 4-stage region, which helps to broaden the study’s applicability. Finally, we did not query the social security database to confirm mortality in our cohort, so mortality reported may underestimate the true rate.
At a dedicated PJI centre with abundant resources for complex patient care, the 2-stage revision arthroplasty approach for our cohort of patients with chronic hip and knee PJI resulted in implant retention in approximately ⅔ of cases. However, nearly 15% of these cases remained on chronic antibiotic suppression. High failure and mortality suggest the need for significant improvement in surgical treatment protocols for this vulnerable population.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Herndon- Paid consultatnt DePuy, and Johnson and Johnson Co, Solventum, Medtronic, Polaris Rowe- Employee of Stryker Fehring- Research support, royalties, payment for lectures/presentations, paid consultant for DePuy a Johnson and Johnson Co. Otero- American Association of Hip and Knee Surgeons, committe member, Paid consultant, research support as a principal investigator for DePuy, a Johnson and Johnson Co, Paid consultant, research support, and royalties for Zimmer Biomet, Paid consultant for Onkos.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.