
Abstract
Background:
Robotic-assisted total hip arthroplasty (RA-THA) has been shown to improve the accuracy of component positioning, but the learning curve for efficient operative performance remains debated.
Methods:
We retrospectively reviewed 579 consecutive RA-THA procedures performed between June 2021 and June 2023 at a single centre using the MAKO robotic system. Surgeon 1 performed cases via the direct anterior approach (DAA), and Surgeon 2 via the posterolateral approach (PL). A historical cohort of conventional manual THA served as a control group. Operative time was the primary outcome. Learning curves were assessed using cumulative summation (CUSUM) analysis, with proficiency defined as the inflection point at which operative times stabilised. Demographic variables were compared among learning-phase, proficiency-phase, and conventional cohorts.
Results:
A total of 434 DAA and 145 PL RA-THA cases were analysed. For the DAA cohort, proficiency was achieved after 73 cases; mean operative time decreased from 97.9 ± 17.5 minutes during the learning phase to 79.7 ± 16.6 minutes during the proficiency phase (p < 0.001). For the PL cohort, proficiency was achieved after 41 cases; operative time decreased from 89.7 ± 21.6 minutes to 72.8 ± 14.5 minutes (p < 0.001). Compared with conventional THA, proficiency-phase RA-THA operative times were slightly shorter for the DAA (−3 minutes, p = 0.045, small effect size) and comparable for the PL approach (p = 0.632). No significant differences in baseline demographics were observed among groups.
Conclusions:
Robotic-assisted THA is associated with substantial learning curves for operative efficiency, with longer thresholds observed for the DAA compared with the PL approach. Although RA-THA has been associated with early improvements in implant positioning accuracy, operative efficiency appears to improve more gradually with experience. Institutions adopting RA-THA should anticipate approach-specific learning curves, implement structured training pathways, and prepare surgical teams for an initial adaptation period.
Keywords
Introduction
Total hip arthroplasty (THA) is widely regarded as 1 of the most successful procedures in modern orthopaedic surgery; however, accurate acetabular component positioning remains critical to long-term implant survival and functional outcomes.1 –3 Malpositioning of the acetabular component has been associated with instability, accelerated polyethylene wear, and an increased risk of revision surgery.3,4 Despite advances in surgical technique, conventional manual THA relies heavily on surgeon experience and anatomic landmarks, which may result in variability, particularly in patients with complex anatomy or altered pelvic mechanics.5,6
Robotic-assisted total hip arthroplasty (RA-THA) has emerged as a technological advancement designed to improve the accuracy and reproducibility of implant positioning.7,8 Computed tomography (CT)-based robotic systems, such as the Mako platform, allow detailed preoperative planning and intraoperative execution with haptic guidance, enabling surgeons to optimise component orientation and restore hip biomechanics with greater precision. 9
Despite these advantages, adopting robotic technology introduces a learning period during which operative efficiency may be reduced. The learning curve is most commonly reflected by prolonged operative times, although its magnitude and duration remain debated. A recent systematic review reported a modest learning curve of approximately 12–17 cases for operative time, with immediate improvements in component positioning accuracy. 10 A subsequent scoping review described a wider range of proficiency thresholds, from 7 to 35 cases, and highlighted heterogeneity across surgical approaches, platforms, and outcome measures. 11
These findings underscore the importance of evaluating learning curves within the context of local practice patterns and surgical approaches. The objective of this study was to determine the learning curve for operative efficiency in RA-THA and to assess whether this learning curve differs between the direct anterior (DAA) and posterolateral (PL) approaches using cumulative summation (CUSUM) analysis.
Methods
Study design and patient selection
This retrospective study was approved by the institutional ethics committee. The MAKO Robotic Arm Interactive Orthopaedic System (Stryker, Mahwah, NJ, USA) was introduced at our orthopaedic department in June 2021. All consecutive patients who underwent primary RA-THA for end-stage primary osteoarthritis between June 2021 and June 2023 were eligible for inclusion.
Exclusion criteria included femoral neck fractures, bilateral procedures, revision arthroplasty, and incomplete operative time data. All procedures were performed by 2 senior orthopaedic surgeons experienced in primary THA but without prior clinical experience using robotic or navigation systems. For comparison, a historical control cohort was assembled consisting of patients who underwent conventional manual THA in the year preceding implementation of the robotic system, using identical inclusion and exclusion criteria.
Preoperative planning
All robotic-assisted procedures incorporated CT-based preoperative planning using Mako software. 3-dimensional reconstructions of the pelvis and femur were generated to determine optimal implant sizing, acetabular cup orientation, and anticipated restoration of leg length and offset.
In the conventional cohort, preoperative planning was performed using standardised anteroposterior pelvic radiographs to estimate component size, neck resection level, and anticipated leg-length restoration. In both groups, the default target orientation for the acetabular component was 40° of inclination and 20° of anteversion. In robotic-assisted cases, these parameters could be adjusted intraoperatively to account for patient-specific anatomy, bony impingement, and spinopelvic considerations.
Surgical technique
Surgeon 1 performed all procedures using the direct anterior approach, whereas Surgeon 2 utilised the posterolateral approach. Both surgeons completed dedicated industry-supported training in RA-THA before initiating clinical use.
Conventional THA was performed using standard handheld reaming and manual cup insertion. Acetabular orientation was guided by anatomic landmarks, including the transverse acetabular ligament and acetabular walls. Fluoroscopy was routinely used for DAA cases.
Robotic-assisted THA was performed using the MAKO system with haptic-guided acetabular reaming and cup placement according to the preoperative plan. The femoral component was also preoperatively templated to optimise metaphyseal fit, offset, and leg length. Intraoperatively, the robotic platform provided real-time feedback on neck resection level and broach version. All robotic-assisted cases used the Accolade II femoral stem and Trident PSL acetabular shell (Stryker, Kalamazoo, MI, USA). Conventional cases were implanted with the Corail femoral stem and Pinnacle acetabular shell (DePuy Synthes, Warsaw, IN, USA). Differences in implant systems and instrumentation were acknowledged as potential contributors to operative efficiency.
Operative time
Operative time was defined as the interval from initiation of limb preparation to application of the final sterile dressing. Robotic system setup and registration were included in the recorded operative time. Data were extracted from intraoperative records within the electronic health record.
Data analyses
Learning curves were assessed using cumulative summation analysis. Robotic-assisted cases were ordered chronologically for each surgeon, and the deviation between each individual operative time and the overall mean operative time was calculated. The inflection point at which the CUSUM curve changed from an upward to a downward trajectory was interpreted as the transition from the learning phase to the proficiency phase. Cumulative summation analysis was chosen to enable objective identification of inflection points in operative performance without predefined case thresholds. Linear regression fitting was used to illustrate overall trends in the acquired data.
Baseline demographic characteristics were compared among the conventional, learning-phase, and proficiency-phase cohorts. Continuous variables were reported as means with standard deviations (SD) and analysed using one-way analysis of variance (ANOVA). Categorical variables were presented as absolute values and percentages and compared using Pearson’s chi-square test. A 2-sided p-value < 0.05 was considered statistically significant. All statistical analyses were performed using Python software.
Results
During the study period, 579 RA-THA procedures were performed. Surgeon 1 (DAA) completed 434 cases, while Surgeon 2 (PL) completed 145 cases.
Direct anterior approach
The mean operative time for the 434 RA-THA cases performed via DAA was 82.7 ± 18.0 minutes (range 39–160). A gradual decrease in operative duration was observed over time (R² = 0.075, Figure 1).
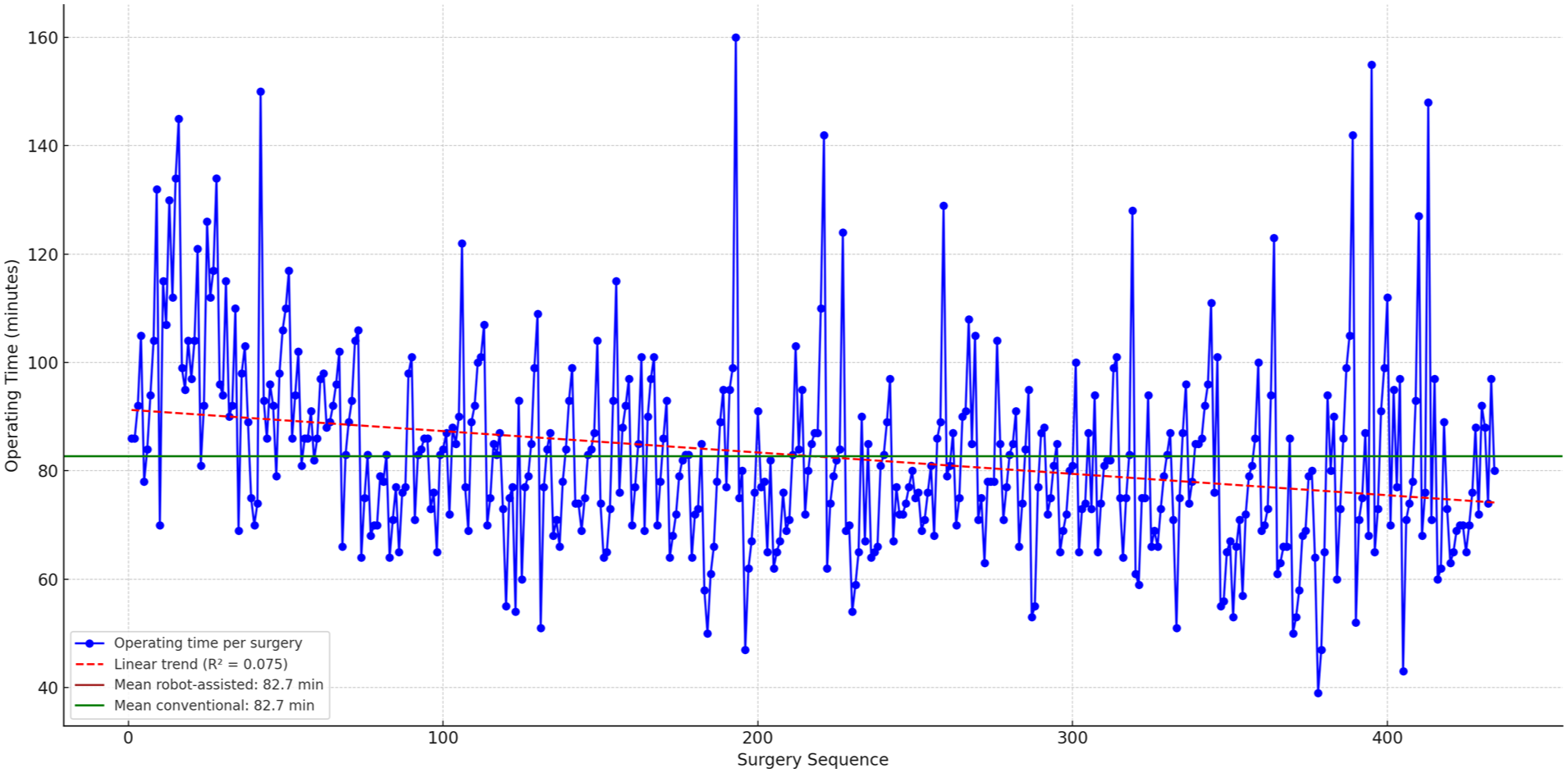
Operative time by case number (direct anterior approach).
Cumulative summation analysis demonstrated a peak at case 73, indicating the transition from the learning phase to the proficiency phase (Figure 2). Mean operative time decreased significantly from 97.9 ± 17.5 minutes during the learning phase to 79.7 ± 16.6 minutes during the proficiency phase (p < 0.001).
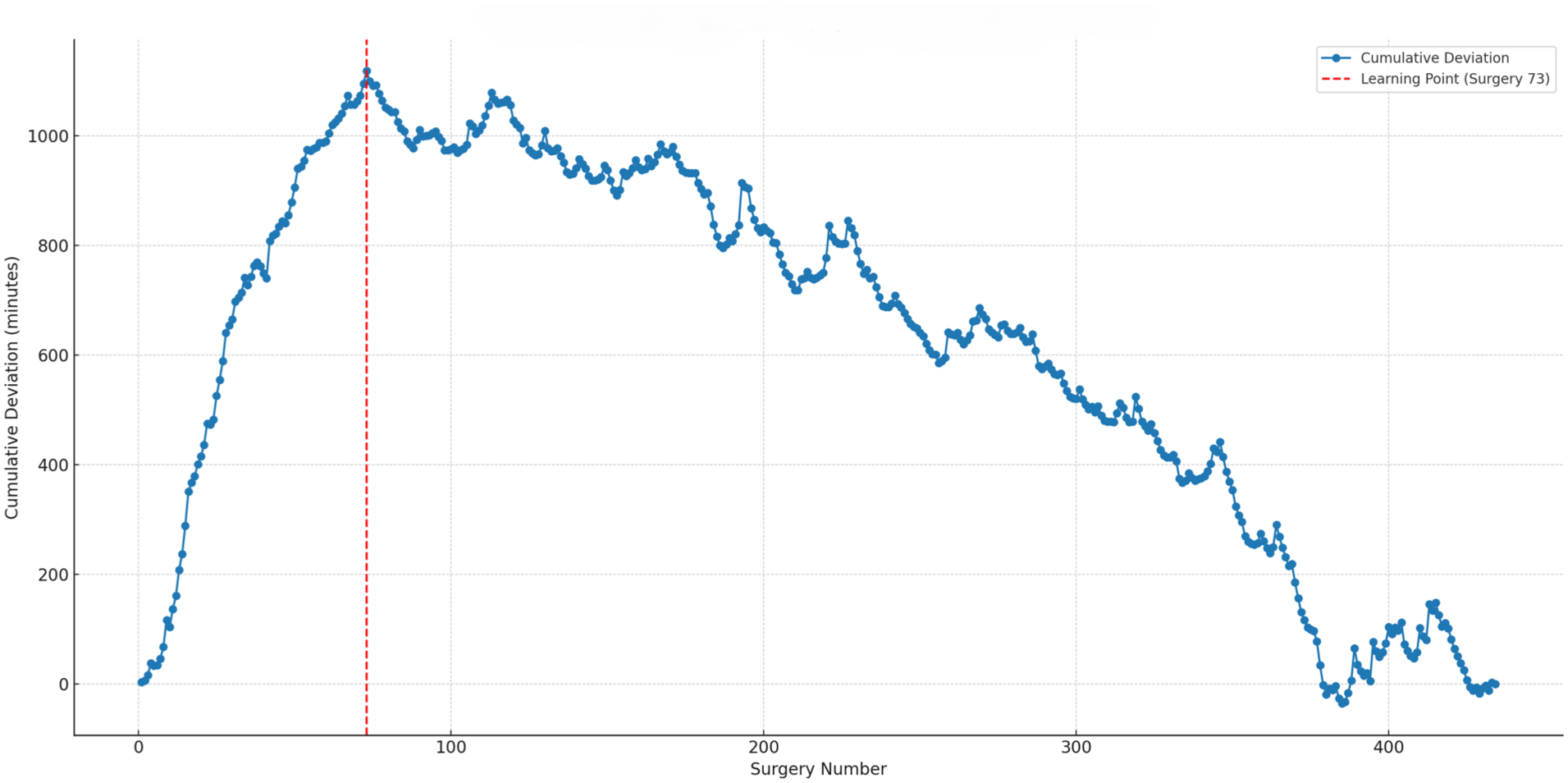
CUSUM analysis of operative time (direct anterior approach).
When compared with the conventional THA cohort, operative time during the proficiency phase of RA-THA was slightly shorter (79.7 ± 16.6 vs. 82.7 ± 18.3 minutes), with a statistically significant difference (p = 0.045). However, the effect size was small (Cohen’s d = 0.17), corresponding to an average reduction of approximately 3 minutes. Baseline demographic characteristics were comparable among the conventional, learning-phase, and proficiency-phase cohorts (Table 1).
Demographics for direct anterior approach.
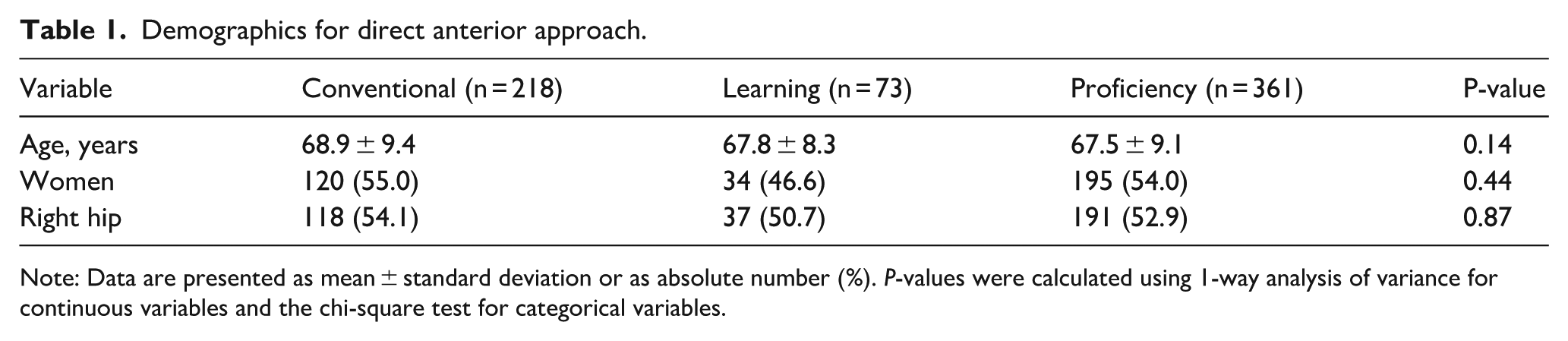
Note: Data are presented as mean ± standard deviation or as absolute number (%). P-values were calculated using 1-way analysis of variance for continuous variables and the chi-square test for categorical variables.
Posterolateral approach
For the 145 RA-THA cases performed via PL, the mean operative time was 77.6 ± 18.4 minutes range 45–184 with a consistent downward trend over time (R² = 0.126, Figure 3).
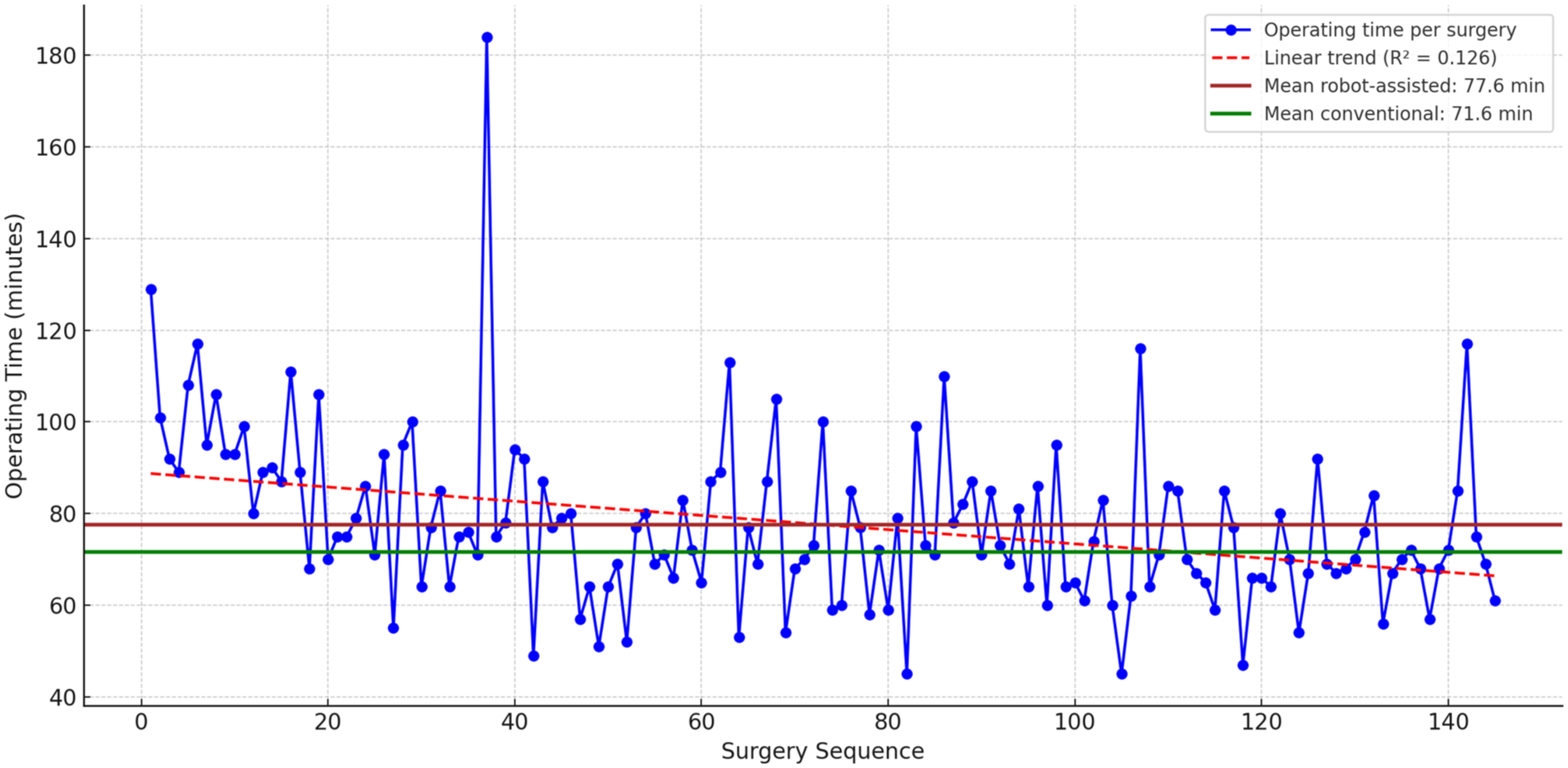
Operative time by case number (posterolateral approach).
Cumulative summation analysis identified a peak at case 41, corresponding to the transition to the proficiency phase (Figure 4). Mean operative time decreased from 89.7 ± 21.6 minutes during the learning phase to 72.8 ± 14.5 minutes during the proficiency phase (p < 0.001).
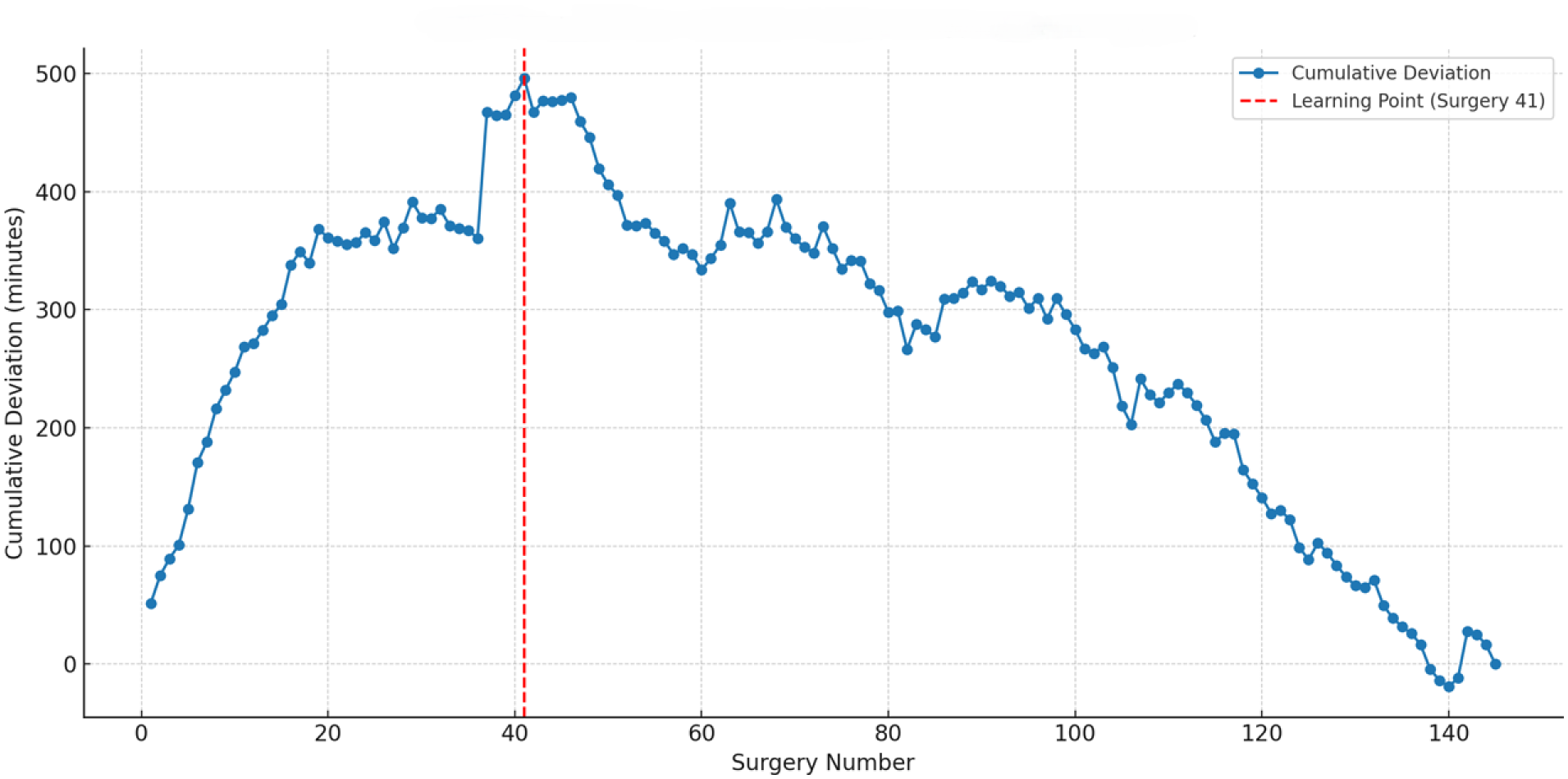
CUSUM analysis of operative time (posterolateral approach).
Comparison with conventional PL THA showed no significant difference between proficiency phase times (72.8 ± 14.5 minutes) and conventional cases (71.6 ± 20.8 minutes; p = 0.632). Baseline demographic variables did not differ significantly among the conventional, learning-phase, and proficiency-phase groups (Table 2).
Demographics for posterolateral approach.
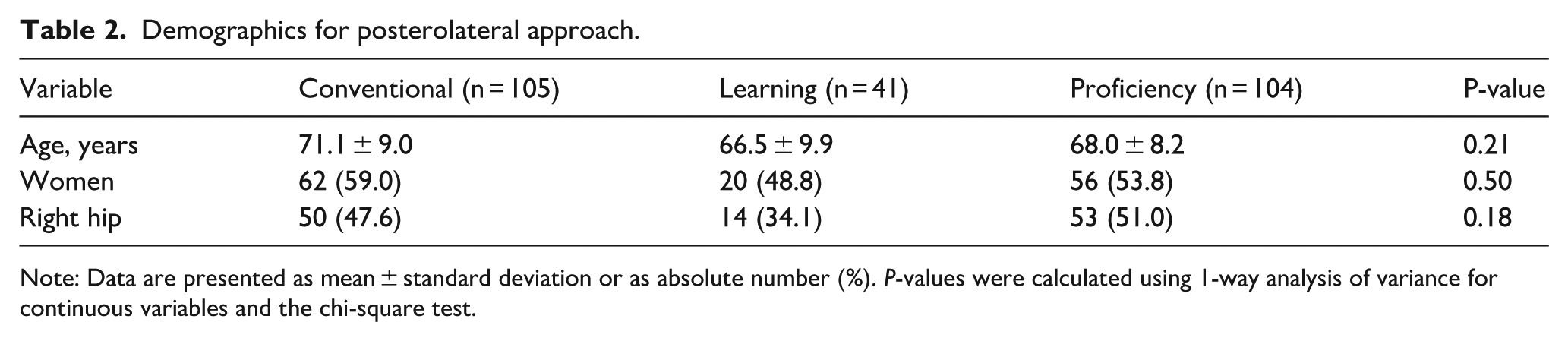
Note: Data are presented as mean ± standard deviation or as absolute number (%). P-values were calculated using 1-way analysis of variance for continuous variables and the chi-square test.
Discussion
This study evaluated the learning curve for operative efficiency in robotic-assisted total hip arthroplasty across 2 surgical approaches at a high-volume European centre. Our findings demonstrate that proficiency in operative time was achieved after 73 cases with the DAA and after 41 cases with the PL approach.
Several earlier investigations have suggested relatively short learning curves for RA-THA. Redmond et al. 12 demonstrated a learning curve characterised by decreasing operative time and fewer acetabular component outliers, with stabilisation after approximately 35 cases. Using cumulative summation analysis, Kayani et al. 13 identified a 12-case learning curve for operative time, while no learning curve was observed for accuracy of acetabular component positioning. Similarly, Kong et al. 14 and Guo et al. 15 reported stabilisation of operative duration after approximately 14 and 13 cases, respectively, with maintained or improved accuracy compared with conventional THA. More recent studies have highlighted platform-specific variability, with reported learning curves ranging from 7 to 17 cases depending on robotic system design and workflow.16 –19 Notably, Schwartz et al. 20 demonstrated that high-volume surgeons achieved operative-time proficiency after approximately 20 cases, whereas medium- and low-volume surgeons exhibited longer and less predictable learning curves.
Systematic reviews provide additional context. A recent meta-analysis estimated a modest learning curve of 12–17 cases for operative time, while a scoping review reported a wider range from 7 to 35 cases with a weighted mean of 16.4.10,11 Consistent with these findings, Hecht et al. emphasised that although accuracy benefits appear immediate, improvements in operative efficiency require additional experience. 10
Our results, showing 73 cases for DAA and 41 for PL, are considerably higher than the thresholds reported in most prior studies. Several explanations can be considered. The DAA is generally considered more technically demanding than the PL approach, requiring precise exposure and soft tissue handling in a limited operative corridor, which may have prolonged the transition to proficiency. In addition, the entire surgical team had no prior experience with navigation or robotic systems, and the adjustment period extended beyond the surgeons to include nurses, anaesthesiologists, and support staff. Implant selection may also have played a role, as Stryker implants (Accolade II stem, Trident shell) were used in the robotic-assisted group, while DePuy Synthes implants (Corail stem, Pinnacle shell) were used in the conventional group, potentially influencing operative efficiency through differences in instrumentation and familiarity. Moreover, our institution functions as a referral centre, and the diverse patient population likely added complexity and variability to procedures. Despite these factors, operative times following the learning phase were comparable to those of conventional THA. This finding reinforces the notion that RA-THA does not inherently compromise long-term efficiency and that the initial increase in operative time represents a transitional phase rather than a permanent drawback.
Our findings have important implications for surgeons and institutions implementing RA-THA programs. Expectations regarding the duration of the learning curve should be realistic and tailored to the chosen surgical approach. While robotic technology may facilitate early accuracy and reproducibility, operative efficienc – particularly for the direct anterior approach – may require a substantially larger case volume than previously reported. Structured training pathways, dedicated team education, and proctoring may help shorten this transition period. Hospital administrators should also anticipate longer operative times during early adoption phases when planning operating room utilisation and resource allocation.
This study has several limitations. It was conducted at a single institution with 2 surgeons, which may limit generalisability. However, the large number of cases and consistent methodology strengthen the reliability of the findings. Operative time was used as the primary surrogate for efficiency; clinical, radiographic, and patient-reported outcomes were not assessed.
Conclusion
Robotic-assisted total hip arthroplasty is associated with distinct and approach-dependent learning curves for operative efficiency. In this series, proficiency was achieved after 73 cases using the direct anterior approach and after 41 cases using the posterolateral approach. These thresholds exceed those reported in much of the existing literature, underscoring the influence of surgical approach complexity, team adaptation, and real-world practice conditions. Although robotic systems may mitigate learning curves for accuracy, gains in operative efficiency require sustained experience. Structured training programs, realistic benchmarks, and team-wide preparation are essential for successful integration of RA-THA into contemporary orthopaedic practice.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PDR: reports personal fees from Enovis and Stryker outside the submitted work.
All other authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.