
Abstract
Purpose:
The aim of this study is to determine the prevalence of infiltration and extravasation among children staying in a children’s hospital and the interventions carried out when infiltration or extravasation occurred.
Methods:
A prospective and descriptive research design was used in the study, conducted between September 2015 and February 2016, and determined the prevalence of infiltration and extravasation and their characteristics. The study sample consisted of 297 peripheral catheters in 173 pediatric patients.
Results:
Of 297 peripheral catheters, 50.8% were located on the right and 30.6% were inserted in the dorsal metacarpal vein. Infiltration and extravasation occurred in 2.9% and 2.3% of the patients, respectively. The prevalence of infiltration and extravasation was 5.5 and 4.4 per 1000 patient-days, respectively. The applied interventions after infiltration or extravasation included covering with a gauze dressing or alcohol-soaked cotton, cold application, irrigation with physiological saline, and elevation.
Conclusion:
The infiltration and extravasation prevalence were found to be high, but the interventions to address them were inadequate. Training and implementation strategies should be planned for pediatric nurses to prevent infiltration and extravasation.
Introduction
Peripheral intravenous (PIV) interventions are frequently applied in short-term IV fluid and medication therapy for pediatric patients. PIV interventions threaten patient safety and cause preventable and predictable complications.1,2 The most important complications of PIV interventions are infiltrations and extravasations. 3 Newborns and little children are more exposed to infiltration and extravasation (I/E) injuries than adults due to developmental and physiological factors such as communication skills, activity levels, and fragile vein structures.4,5 Infiltrations and extravasations generally occur with symptoms, including swelling or color changes such as redness or whiteness at the PIV catheter site, pain, an increase or decrease in temperature at the infiltration site, or a change in the quality of pulse under the infiltration site. 6
The concentration or volume of medications and the area or duration of exposure to these medications affect I/E. 5 In addition, mechanical factors during or after the insertion of the catheter, such as the pressure of the pump device, patients’ activity level, nurses’ ability and intervention technique, and physiological factors due to problems that already exist or develop later such as the vascular structure and size, also play an important role. 3 The fact that I/E are traumatic for patients, and their treatment and care involves high costs, has led to the development of strategies to determine their causes, prevent them from occurring, and ensure effective treatment and care. 7 Prevention and effective management of I/E are among the basic responsibilities of nurses. Prevention of I/E should be a part of an institution’s policies related to ensuring safe nursing care. Protocols based on scientific evidence should be followed to ensure patient safety and improve nursing care. 8
There are limited data available on the rates of I/E and they are generally high.4,9–13 High and variable I/E rates in the literature gave the researchers the idea of re-evaluating their own rates. The objectives of this study were to describe the prevalence of I/E (as the rate per patient-days) at our facility, identify the agents causing I/E injuries, and describe the managed interventions when I/E occurred in hospitalized pediatric patients.
Methods
Study design and sample
This descriptive study was conducted at a children’s hospital in Turkey between September 2015 and February 2016. The Ege University Children’s Hospital setting was composed of 150 beds across neonatal-pediatric intensive care units and neurology, nephrology, cardiology, respiratory, hematology, and general pediatric wards. The inclusion criteria for the study sample were being patients aged between 0 and 18 years, having a PIV catheter insertion, and being hospitalized. The hospitalized infants and children who had PIV catheters were included in the study by the researchers starting from the insertion of the catheter. Patients were followed during hospitalization by the researchers every day. Sample size for prevalence study was calculated as 125 patients in accordance with a precision of 5%, confidence interval of 95%, and expected prevalence of 8.93 per 1000 patient-days according to Taylor’s results 14 with unknown population. 15 We included 173 patients in the study, taking into account loss of sample. The prevalence of I/E was calculated per 1000 patient-days.
Data collection
After written consent was obtained from the parents of children who had IV catheters, the patients were followed during their hospitalization. Their demographic and catheter characteristics were determined by researchers using “The Evaluation Form of IV Insertion Site in Pediatric Patients.” The patients included in the study were followed and evaluated according to the occurrence of I/E in the catheter, the reason for removing the catheter, and reinsertion of the catheter by the research team every day between 4:00 pm and 6:00 pm. If I/E developed, researchers noted the localization with “The Evaluation Form of IV Insertion Site in Pediatric Patients with I/E.” Infiltrated or extravasated IV fluid, medication therapy and its flow rate, and the time of noticing the I/E and applied interventions were determined from the notes of bedside nurses.
If a patient had other IV catheters inserted again, these other catheters were followed by the researchers. Researchers evaluated the I/E site, photographed the I/E site, and determined the stage using the Infiltration Scale 2 or the Extravasation Scale. 16
Data collection forms
The evaluation form of IV insertion site in pediatric patients
This form, developed by researchers, included questions about age, gender, diagnosis, date of IV catheter insertion, IV insertion site, IV fluid, and medication therapy flowing through the IV catheter, date of, and reason for, removing the IV catheter, and total patient-days.
The evaluation form of IV insertion site in pediatric patients with I/E
This form, developed by researchers, included questions about the localization of I/E, IV catheter insertion day when I/E occurred, time of noticing I/E (time that passed until the I/E), infiltrated or extravasated IV fluid(s) and medication therapy(ies), and applied interventions for I/E by bedside nurses.
The Infusion Nurses Society infiltration scale
The scale was developed by the Infusion Nurses Society (2006). It evaluates the infiltration site by rating it on a scale of 0–4 (Grade 0 = no symptoms; Grade 1 = skin blanched, edema <1 in (2.5 cm) in any direction, cool to touch, and with or without pain; Grade 2 = skin blanched, edema 1–6 in (2.5–15 cm) in any direction, cool to touch, and with or without pain; Grade 3 = skin blanched, translucent, gross edema >6 in (15 cm) in any direction, cool to touch, mild-to-moderate pain, and possible numbness; Grade 4 = skin blanched, translucent, skin tight, leaking, skin discolored, bruised, swollen, gross edema >6 in (15 cm) in any direction, deep pitting tissue edema, circulatory impairment, moderate-to-severe pain, infiltration of any amount of blood product, irritant, or vesicant). The inter-rater reliability of the infiltration scale was statistically significant (k = 0.393, p < 0.001). 2 The mean time taken to finish was 1.3 min. 2
Extravasation scale (National Cancer Institute common terminology criteria for adverse events version 4.0 classification)
This enables the extravasation in the patient to be monitored and recorded. This classification was made based on the National Cancer Institute common terminology criteria for adverse events (version 4.0; NCI-TCAE). 16 It evaluates the extravasation site by rating it on a scale from 0 to 5 (Grade 1 = no symptoms; Grade 2 = erythema with associated symptoms (e.g. edema, pain, induration, and phlebitis); Grade 3 = ulceration or necrosis, severe tissue damage, and operative intervention indicated; and Grade 4 = life-threatening consequences and urgent intervention indicated; and Grade 5 = death). 16
Ethical considerations
Written approvals were received from the Ege University Faculty of Nursing Ethics Committee (IRB: 2015-192) and Ege University Children’s Hospital, where this study was conducted. Written informed consent was obtained from the children’s parents and from children aged 7–18 years.
Data analysis
Patient and catheter characteristics were analyzed using the Statistical Package for Social Sciences (SPSS) program version 23.0. Number and percentage were used to assess the data about patient and catheter characteristics. The I/E prevalence was determined by calculating the I/E per 1000 indwelling patient-days (infiltration number/patient-days × 1000; extravasation number/patient-days × 1000).
Results
Patient characteristics
Among the patients, 17.9% were 12 years and older and 52% were girls and hospitalized in general pediatric wards. One catheter was followed in 78.6% of the patients. I/E occurred in 2.9% (n = 5) and 2.3% (n = 4), respectively, of the patients. The mean indwelling patient-days was 3.0 ± 1.8 (minimum 1 and maximum 10). In this study, 173 pediatric patients were followed for 908 patient-days. The prevalence of I/E was 5.5 and 4.4 per 1000 patient-days (Table 1).
Patient characteristics.
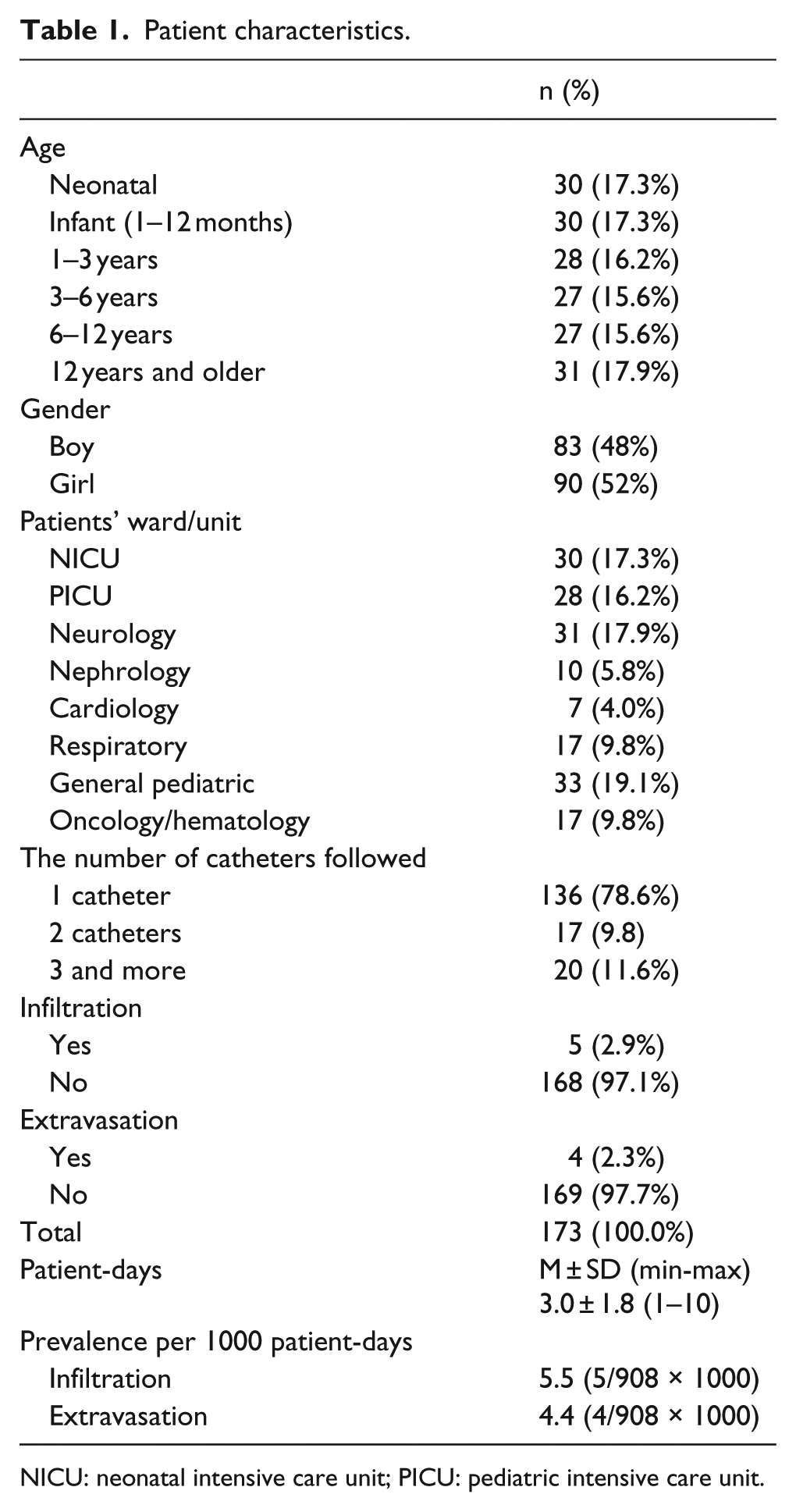
NICU: neonatal intensive care unit; PICU: pediatric intensive care unit.
Catheter characteristics
In this study, 297 catheters were followed inserted in 173 patients. Of the 297 peripheral catheters in the study, 50.8% were located on the right, 30.6% were inserted into the dorsal metacarpal vein, and 55.9% were removed due to obstruction (Table 2). Of the peripheral catheters, 72.1% (n = 214) were used for medication therapy. The average number of flowing medications was 2.1 ± 1.3 (minimum 1 and maximum 8). Of the peripheral catheters, 37% (n = 110) were used for antibiotic treatment and 24.2% (n = 72) were used for antifungal medication therapy. Of these, 63.3% (n = 188) were used for continuous IV fluid infusion. Of the catheters used for continuous IV fluid infusion, 48.4% (n = 91) were used for administering 5% dextrose + 0.9% NaCl.
Catheter characteristics.
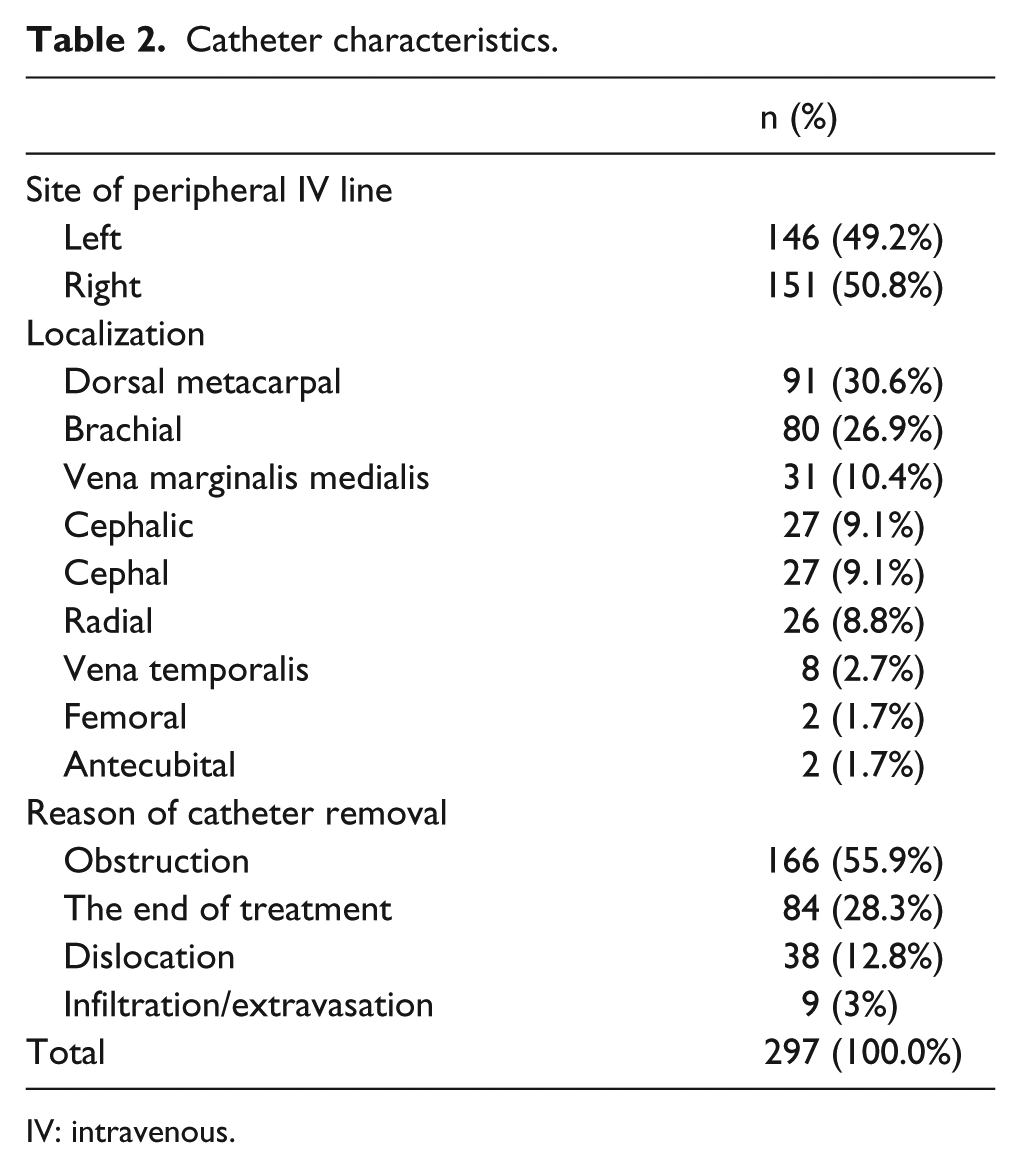
IV: intravenous.
Characteristics of I/E events
Table 3 presents information about the I/E site, infiltrated or extravasated IV fluid and medication therapy, day of catheterization when I/E developed, time of noticing I/E, interventions for I/E, and the degree of infiltration or extravasation of nine pediatric patients. Most of the patients with I/E were aged between 1 and 12 years (n = 7, 77.8%) and 66.7% were boys (n = 6). The majority of the infiltration or extravasation incidents occurred in the brachial vein (n = 5, 55.5%). Infiltration or extravasation was noticed in the first 5 min in some cases (n = 2, 22.2%), while the majority of the incidents were noticed later (> 5 min; n = 7, 77.7%). Extravasation was observed 2 days later in one patient and was discovered by a bedside nurse at catheter change. The applied interventions after I/E developed included covering with a gauze dressing (n = 4), covering with alcohol-soaked cotton (n = 2), cold application (n = 1), irrigation with physiological saline (n = 2), elevation (n = 2), and dressing with Bactroban cream (n = 2). Among the infiltration or extravasation incidents, 77.7% (n = 7) were evaluated as Grade 1 infiltration or extravasation, while two cases (22.2%) with extravasation were evaluated as Grade 3 (Table 3).
Infiltration/extravasation event properties of nine pediatric patients who experienced an infiltration and extravasation.
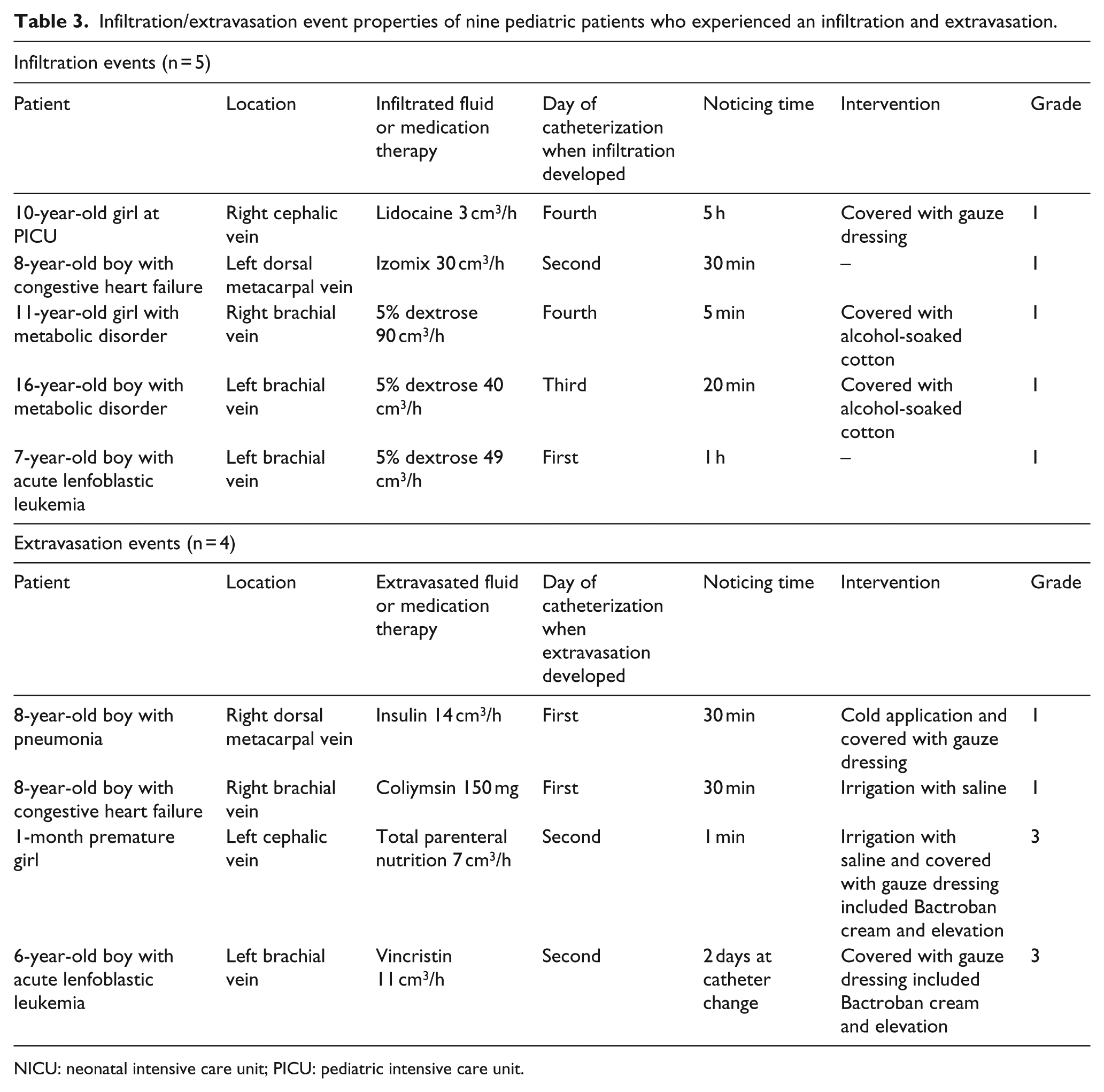
NICU: neonatal intensive care unit; PICU: pediatric intensive care unit.
Discussion
Newborns and infants have a higher tendency toward I/E due to their fragile vein structures and physiological structures. 4 In this study, 77.8% of the children with I/E were aged between 1 and 12 years. Of the patients included in the study sample for 6 months, 2.9% had infiltration and 2.3% had extravasation. The rates of I/E were 5.5 and 4.4 per 1000 patient-days, respectively. A study conducted by Paquette et al. 9 determined that 42 patients had documented extravasation for an overall incidence of 0.04% per patient-day in their study. Wilkins and Emmerson 10 determined a prevalence of 38 per 1000 neonates who sustained an extravasation injury that caused skin necrosis in the neonatal intensive care unit. Ghanem et al. 11 stated that 78 pediatric patients were referred to plastic surgeon due to extravasation in a single-center study. Major and Huey 17 reported that the infiltration rates before and after the improvement strategies focused on evidence-based education, intravenous (IV) catheter securement, and family engagement, which they developed to reduce pediatric infiltrations, were 13.5% and 7.1%, respectively. A quasi-experimental study conducted by Park et al. 12 on the management of pediatric infiltration found that the infiltration rates were 0.9% in the experimental group and 4.4% in the control group. Taylor 14 reported that the infiltration rates before and after the evidence-based education that was provided to nurses to reduce pediatric infiltration were 20.0% and 11.8%, respectively. Tofani et al. 4 decreased I/E events from 4.2 to 1.8 per 1000 line-days with their quality improvement project. The literature shows that the rates of I/E in pediatric patients are different from each other and generally high.12,14,17 It also shows that I/E rates can be reduced by initiatives.4,14,17
Near-infrared technology can also be used to prevent PIV-related complications. 18 Increasing the success of the procedure avoids delay in treatment and reduces catheter complications.19–21 I/E occurred mostly in the brachial veins of the patients to whom IV fluid and medication therapy were given via continuous infusion in this study. Park et al. 12 stated that the majority of the infiltration incidents occurred in the dorsal metacarpal vein. Paquette et al. 9 observed that extravasation occurred in the right dorsal metacarpal vein in 29% of the patients. The upper extremity is more at risk of I/E because it is more likely to move. Nurses should keep bear information in mind while inserting catheters. 22 The I/E that occurred in the majority of children with chronic illnesses were observed in their dorsal metacarpal and brachial and cephalic veins in this study. For example, nurses used an inappropriate IV insertion area according to patients’ age, and one infiltration event occurred in the right cephalic vein of a 10-year-old girl at a pediatric intensive care unit in this study.
This study showed that mostly the administration of IV fluids as a continuous infusion caused I/E, and 5% dextrose was infiltrated in 33.3% of cases. Paquette et al. 9 determined that 5% dextrose was responsible for 31% of the extravasation incidents. Although 5% dextrose is in the low-risk group in terms of extravasation, it can be responsible for I/E due to the physiological structures of pediatric patients. 5 This kind of intravenous solution is also important in managing I/E sites. In the literature, dextrose, total parenteral nutrition (TPN), antibiotics, and potassium or calcium chloride usually caused I/E.9,10,11,12 The pressure used during infusion and the flow rate should also be taken into account. 23
Preventing I/E is one of the basic responsibilities of nurses. When the first symptoms of I/E are seen, IV fluid therapy should be stopped immediately, the IV set should be removed from the IV catheter, the residual IV fluid and medication therapy from the IV catheter should be aspirated, the IV fluid should be aspirated manually from the tissue, and the antidote for the infiltrated medication should be used. The extremity should be elevated for 24–48 h after the I/E.3,7 Local thermal application should be performed for 15–20 min every 4 h to reduce reaction and absorption in the extravasation site.3,7 Hyaluronidase, which accelerates tissue healing, can be safely used in pediatric patients. 24 This study indicated that the majority of the infiltration or extravasation incidents were noticed within 5 min (n = 7, 77.7%). Evidence-based interventions were lacking and inappropriate treatments were applied, such as covering with alcohol-soaked cotton by bedside nurses, in this study. The antidote was not administered to any patients. Paquette et al. 9 treated 50% of the cases of extravasation with the appropriate antidote.
In this study, 77.7% (n = 7) of I/E incidents were evaluated as Grade I, while 22.2% (n = 2) of extravasation incidents were evaluated as Grade III (Table 3). Park et al. 12 also found infiltration Grade II in 76.4% of the experimental group and in 74% of the control group. Early noticing of I/E prevents a possible tissue necrosis. Assessment of the catheter site once every hour for the symptoms of I/E allows early intervention and prevents the progress of infiltrations and extravasations.3,7 This study presented high rates of I/E incidents and showed that nurses did not know how to attempt to manage these incidents and did not use I/E protocol.
Conclusion
Although there are limited studies on I/E rates, it can be seen that the I/E rates in this study are still high compared to other studies. The pediatric population is a risky group in terms of I/E and this group should be monitored more carefully due to PIV complications. I/E developed in the upper extremities, due to dextrose solution, and developed between 1 and 4 days after catheter insertion in most patients with I/E. This study found that the interventions applied when I/E occurred were insufficient. When I/E events occur, there is no checklist or I/E protocol, including initiatives that clinicians can use. The institution policies should be regulated, and the awareness and knowledge of nurses about this issue should be increased via educational programs in order to prevent I/E and provide appropriate treatment and care after I/E occur. Prevention and management of I/E are among the basic responsibilities of nurses. The results of this study showed the need to provide training for nurses immediately and to improve I/E prevention and management protocols.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.