
Abstract

Introduction
The guidelines for the vascular access management for clinical engineers were formulated by the Vascular Access Management Committee of the Japan Association for Clinical Engineers after the cross-country questionnaire survey of the existing state surrounding the vascular access management and subsequent discussion for 3 years, and were finally publicated in 2016 for the first time. During these procedures, various problems appeared up to the surface, of which two major issues were explained in the lecture:
Limits of vascular access puncture by clinical engineers should definitely be determined.
Application of diagnostic ultrasound imaging system in the puncture process to vascular access should adequately be regulated before confused diffusion to the clinical site.
The guidelines formulated according to the results of cross-country questionnaire survey
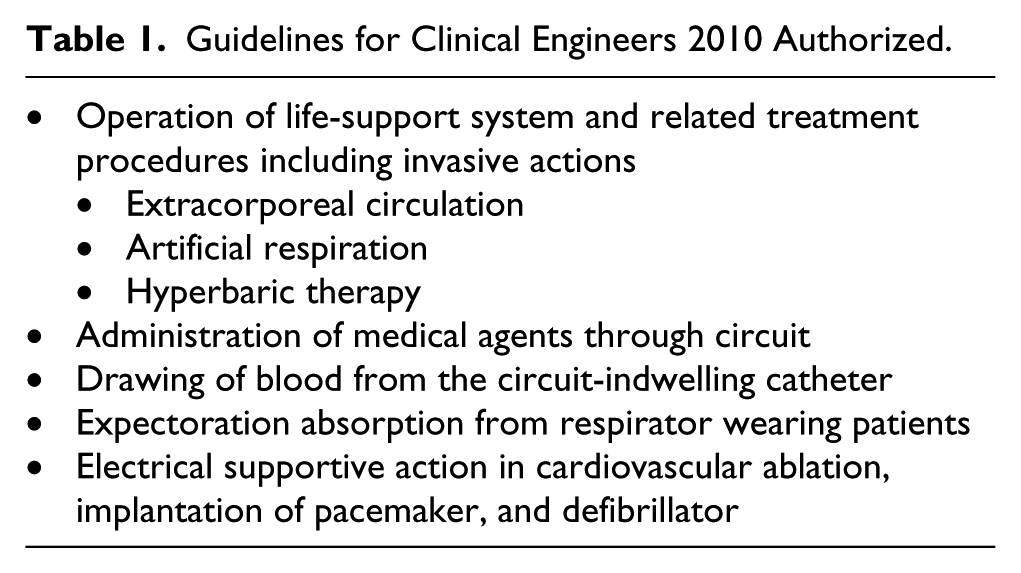
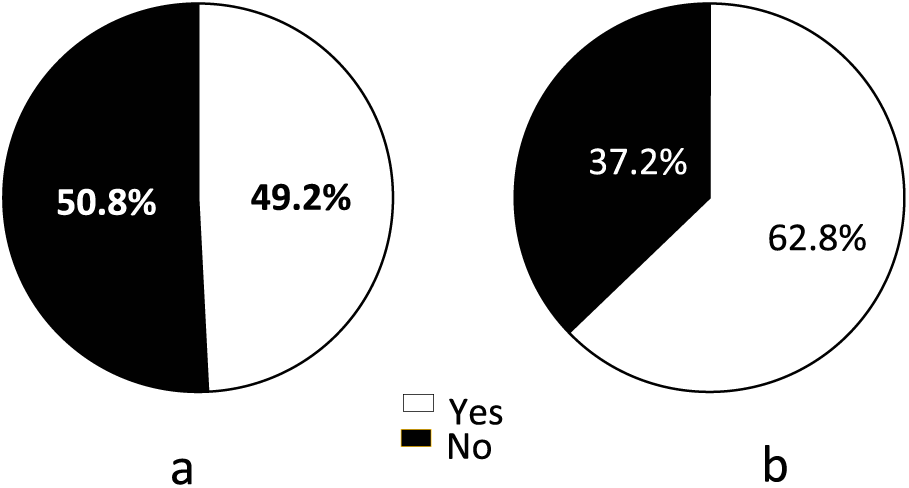
The clinical engineer system has diffused during these three decades as an expert in medical equipment and devices of high technology, to which legal system has also been straightened to support and authorize the activities of clinical engineers in Japan. The basic guidelines for the activities of clinical engineers that had been regulated previously in 2010 (Notification No. 1101-1, 2010, from Medical Affaires Section Manager, Ministry of Health, Labor and Welfare) determined definitely the operation of life support system and related treatment procedures including invasive actions as indicated in Table 1. However, detailed regulation about the puncture to vascular access as an activity of clinical engineers had not been well prescribed in this previous basic guidelines, and then the Vascular Access Management Committee decided to formulate new and practical guidelines in 2012. A nationwide questionnaire survey that covered 3656 hemodialysis treatment–related facilities was carried out to reveal the existing state about the vascular access management, and 2136 valid responses (58.4%) were obtained during 2012–2013. According to this survey, blood purification therapy was carried out in 87.5%, and the puncture procedures to vascular access were also carried out in 91.7% of all facilities by clinical engineers (Figure 1) at the clinical site. Of various types of vascular access, Japanese clinical engineers punctured not only to arteriovenous fistula (AVF) and arteriovenous graft (AVG) but also to subcutaneously fixed artery, but direct puncture to arteries was in the minority (Figure 2). Puncture not only to AVF and AVG but also to the subcutaneously fixed artery was authorized by the present guidelines based on the interpretation that these procedures were considered as a connecting action of extracorporeal circulation routes to the vascular access, just like an electric cord to a receptacle plug. Puncture to other superficial veins but the vascular access was also authorized. However, puncture directly to artery was accurately determined as out of the duty of clinical engineers. These regulations are summarized in Table 2.
Guidelines for Clinical Engineers 2010 Authorized.
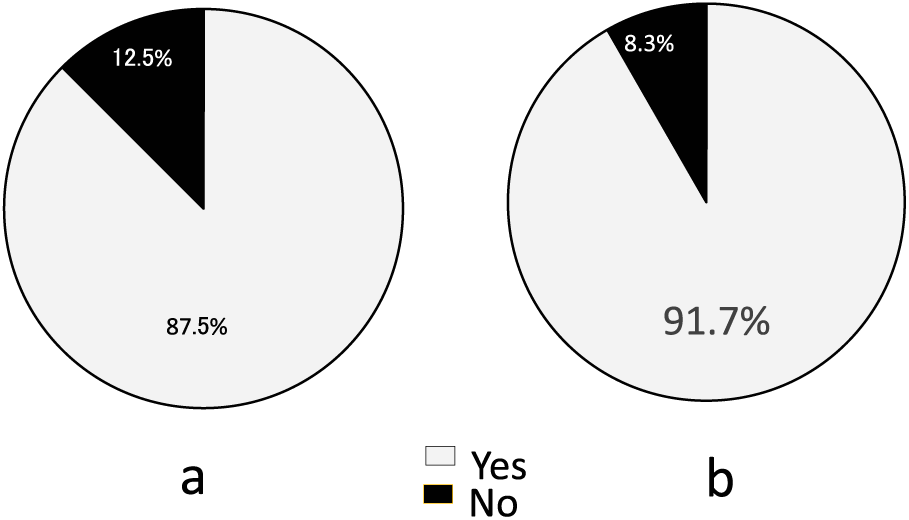
Results of the cross-country questionnaire survey on the vascular access management: (a) Is blood purification therapy carried out mainly by clinical engineers? (b) Is vascular access punctured by clinical engineers?
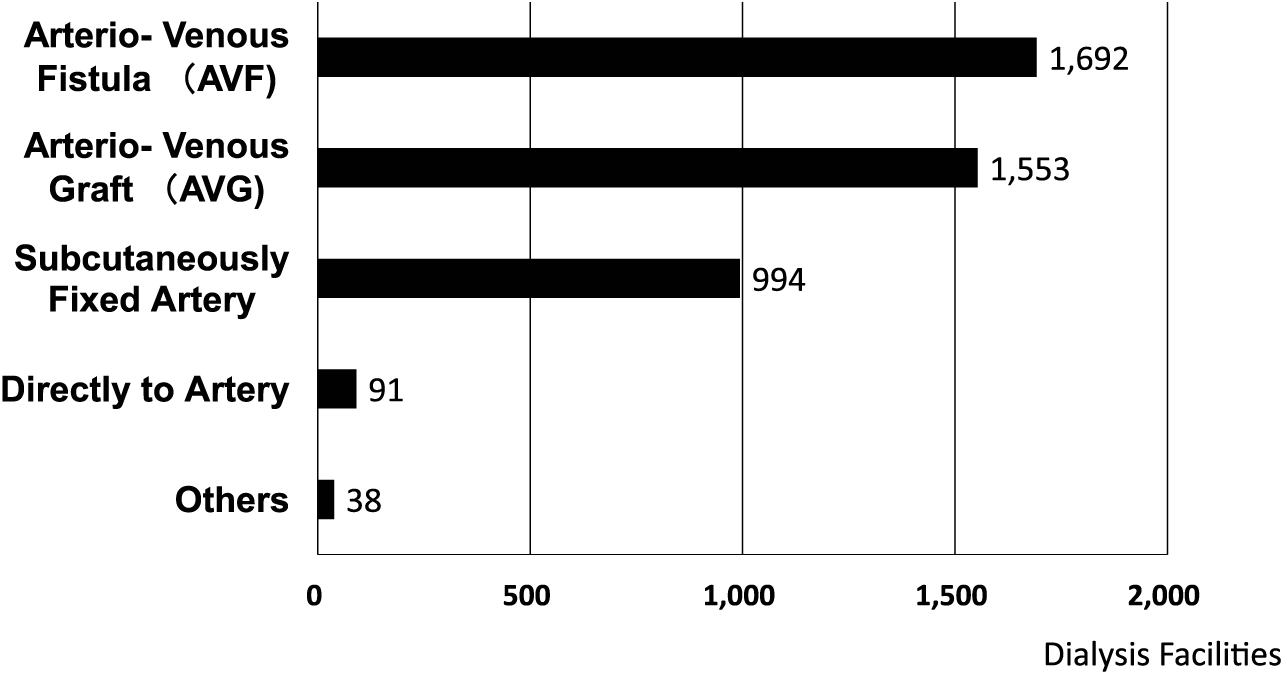
Results of the cross-country questionnaire survey on the vascular access management. What kind of vascular access punctured by clinical engineers?
Vascular access puncture by clinical engineers.
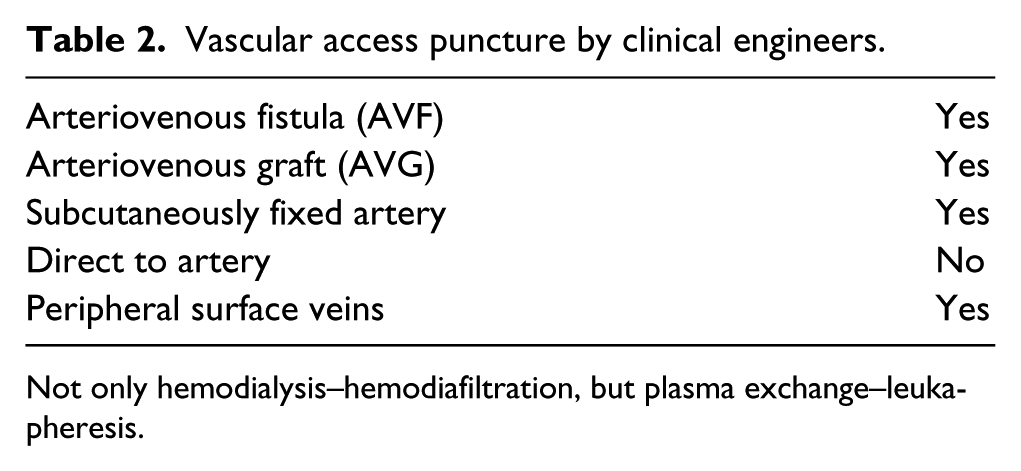
Not only hemodialysis–hemodiafiltration, but plasma exchange–leukapheresis.
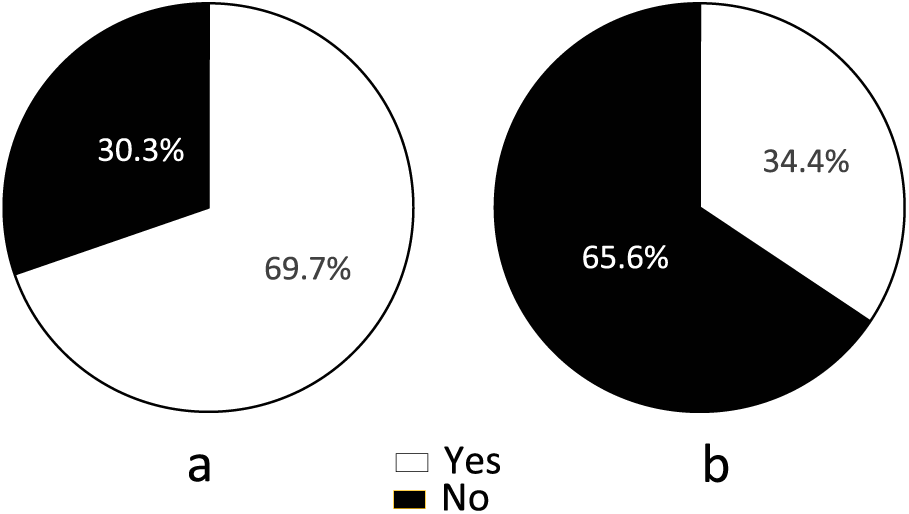
Another major problem was about an application of diagnostic ultrasound imaging system that had already been widely diffused in evaluating the potency of vascular access at the clinical site of hemodialysis therapy. The results obtained by the questionnaire survey revealed that ultrasound devices had already been utilized in the management of vascular access in almost half of all hemodialysis treatment–related facilities in 2013 (Figure 3(a)), while those devices were employed without any practical education or training by following other persons almost in one-third of all clinical engineers (Figure 3(b)). To make matters worse, ultrasonic findings of vascular access had not been recorded in almost 30% (Figure 4(a)), and ultrasonic examination was carried out without any diagnostic criteria in almost two-thirds of all facilities (Figure 4(b)). According to these results, the Committee determined the following measures to be promoted in the following years to improve and keep the standard skill of clinical engineers by the Japan Association for Clinical Engineers:
A prescribed form to which clinical engineers fill out about the results of ultrasonic examination of vascular access as a routine management check sheet including diagnostic criteria by accumulating scores was proposed within the guidelines,
To which should be specified the responsibility for final diagnosis after the revision and certification by doctor(s).
Meeting and/or lectures composed not only of basic curriculum but also of practice and on-the-job training, for example, employing vascular access simulator.
Results of the cross-country questionnaire survey on the vascular access management: (a) Is diagnostic ultrasound imaging system employed in the vascular access management? (b) Are clinical engineers educated and/or trained on ultrasonic device in the vascular access management?
Results of the cross-country questionnaire survey on the vascular access management: (a) Are ultrasonic findings kept on record? (b) Is ultrasonic examination carried out according to certain criteria?
Conclusion and prospects
A system of clinical engineer was established 30 years ago, and has diffused throughout the country, that provided a sophisticated hemodialysis treatment peculiar to Japan. Formerly, accumulated experiences, something of craftsmanship, were required to realize the physical findings accurately in the puncture of vascular access. Application of diagnostic ultrasound imaging system to the clinical site seems almost a revolutionary change to provide a hemodialysis treatment of higher quality. When we find ourselves face up to advances in medical technology, what has been the sense of training to acquire the clinical craftsmanship during the past three decades. Apart from such hard experiences, I think indeed that to see is to believe, just like that a bamboo pole cannot be compared with a missile. We are now in the midst of paradigm change in the vascular access management. All clinical engineers should be diligent to master the practical procedures of ultrasonic examination not to fail to catch this paradigm change, since incomprehension of the means seems to result in the unhappiness both in patients and in medical staff. All clinical engineers should master and utilize diagnostic ultrasound imaging system intelligently as eye-installed hands in the following decade. The Association wishes that the present guidelines would be a means to provide a hemodialysis treatment of higher quality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.