
Abstract
Introduction:
Providing peripheral intravenous access is one of the most commonly performed technical procedures in hospitals and it is mandatory for all patients undergoing surgery. Obtaining peripheral intravenous access may be difficult and this may cause delays in patient management, increased risk of adverse events and hospitalization costs. The aim of this study is to develop and validate a scale to identify patients at risk of peripheral difficult intravenous access, applicable to any adult patient undergoing surgery.
Methods:
A monocentric, observational study was conducted on adult surgical patients between September 2015 and April 2016. The primary outcome was the identification of parameters that could detect peripheral difficult intravenous access. Several parameters were taken into consideration, including patient details, healthcare professionals, and setting. The sample data were randomly divided into two subsets: a multivariate analysis was performed on the first one to define the Enhanced Adult DIVA score; the second subset was used for its validation.
Results:
We included 1006 patients (607 in the derivation, 399 in the validation cohorts respectively). The peripheral intravenous access was difficult in 127 patients (12.6%). The EA-DIVA score was devised with a score ranging from 0 to 12. The receiver operating characteristic (ROC) curve area under the curve (AUC) in the validation subset was 0.94. The validation study suggested a cut-off score of 8, which maximizes sensitivity (85.5%) and specificity (89.2%) in detecting difficult peripheral intravenous access, with a positive predictive value of 56% and a negative predictive value of 97.5%.
Discussion:
The EA-DIVA score is a simple tool to identify patients at high risk of peripheral difficult intravenous access. Its implementation is recommended in order to optimize peripheral intravenous access procedures.
Keywords
Introduction
Background
Providing a peripheral intravenous (PIV) access is one of the most common technical procedures in hospitals, and 70%–80% of all hospitalized patients require a PIV catheter.1–3 In particular, it is mandatory for all patients undergoing surgery, in order to allow fluids and drugs to be administered.
Nevertheless, obtaining PIV access may be difficult, even for highly qualified medical staff, 4 and it has been reported that up to 15% of venous placements may require a second attempt. 5 This could be frustrating both for the healthcare professional and for the patient, who often experiences pain and discomfort, especially when multiple attempts are necessary. 6 A difficult intravenous access (DIVA) may also be responsible for a delay in patient management, an increase in hospitalization costs and a risk of adverse events such as nerve damage, paresthesia, hematoma, and arterial puncture.7,8
Moreover, multiple attempts and inappropriately inserted devices could damage and limit the patients’ venous asset. In the absence of a commonly accepted definition of the term, we have defined patient venous asset as the clinically exploitable venous network system, useful for the administration of parenteral solutions and for blood sampling.
Unfortunately, it is not always easy to predict which patients are likely to have peripheral DIVA, and thus an evaluation algorithm would be useful to guide the decision-making. 9
Many authors have investigated patient-related risk factors for peripheral DIVA, especially in Emergency Departments (EDs).4,8,10,11 A recent study showed that the most important risk factors for peripheral DIVA are diabetes, intravenous drug abuse, and sickle cell disease, whereas obesity, dialysis, and chemotherapy were not found to influence the probability of success. 12 Another study examined the prevalence of difficult venous access in patients with multimorbidity, identifying the female gender as an associated risk factor. 13
To date, there are two scales available: the pediatric DIVA scale and, more recently, a modification of the DIVA scale that could be applied to the adult population (A-DIVA). In both studies validating these scales, the primary outcome of interest was the failure of venous cannulation on the first attempt.14,15 Some hospitals developed an internal scale specific to oncology patients and therefore not suitable for all hospitalized patients. 16
Objectives
The aim of this study was to develop and validate a scale that is specifically designed to be applicable to all adult patients during the presurgical clinical examination, in order to identify patients at risk of peripheral DIVA, with the ultimate purpose of taking preventive action to prevent discomfort and risks to the patient, as well as to avoid delays in operating theater schedules and in patient management.
Methods
Study design and setting
A prospective cohort study was performed between September 2015 and April 2016 in the operating theaters of the IRCCS Policlinico San Matteo (Pavia, Italy), a 1200-bed university hospital. At our institution, from 2011 and until 24 May 2018 (date of European GDPR), all patients admitted to our research and teaching hospital (as in-patients or out-patients) signed a consent form granting permission to use their health-related data for observational research purposes (for interventional research, study-specific forms are required) or for teaching purposes. This procedure was approved by the ethical review board.
Participants
All adult patients undergoing a surgical procedure (elective or urgent) were eligible, excluding patients with a peripheral vascular access already in place and patients in the delivery room.
The primary outcome was the identification of difficult venous access, which for the purposes of our study was defined as cases in which more than three attempts were necessary to obtain successful, stable PIV access using short peripheral cannulas. An attempt was defined as any instance in which the needle was inserted through the skin, and was defined as “successful” when a short peripheral cannula was inserted and a saline flush could be infused without signs of subcutaneous injection (e.g. subcutaneous edema, swelling, pain). On the contrary, it was defined as “failed” whenever the catheter needed to be removed from the patient.
Variables
We collected the following parameters, potentially associated with DIVA:
Demographic data—sex, age, type of surgery, and relevant department/ward;
Medical history—coagulopathies (e.g. hemophilia, thrombocytopenia, vitamin K deficiency), overweight condition (body mass index (BMI) > 25), tobacco use (active smoker, any quantity), dermatological issues (e.g. psoriasis, erysipelas, dermatomyositis, keloids, burns, scars, and tattoos), or agitation (e.g. uncooperative patient or patient disoriented in time and space);
Vascular history—previous known difficulty in venous access, venous disease (e.g. deep vein thrombosis, lymphedema, or varicose veins), peripheral neuropathies (e.g. chronic inflammatory, demyelinating polyneuropathy, arm or limb paresis, Lyme disease), presence of arteriovenous fistula, previous infusion of chemotherapeutic agents, drug abuse (either active or past), or anticoagulant or antiplatelet drug intake;
Peripheral venous system characteristics—signs of previous venipuncture, signs of either past or actual phlebitis, or extravasations;
Availability of both sides of the body (amputation, surgical needs, etc.);
Presence of a long-term vascular access (i.e. midline catheter, peripherally inserted central catheter, port-a-cath) or need to position a central venous catheter;
Type of operator and technical data about venipuncture—operator (nurse, resident, or staff physician), number of attempts, time required to obtain a stable access (more or less than 10 min), need to refer to another operator, need to resort to ultrasonography, or venipuncture site (hand, forearm, antecubital area, arm, inferior limb);
Elective versus urgent procedure.
Data sources
As soon as the patient arrived in the preoperative holding area, the healthcare professional placing the intravenous line (a resident, a staff anesthesiologist, or a nurse) chose the best anatomic site for cannulation according to her or his clinical judgment. In our operating theaters, the usual sequence for searching a suitable site for PIV access starts from the distal part of the limb up to the proximal part. Upper limbs are preferred to the lower ones whenever possible.
At the time of the study, Venflon catheters were used (BD Infusion Therapy AB, Helsingborg, Sweden). The venipuncture was performed according to the routine procedure: site selection, tourniquet placement, clinical evaluation of site, catheter size selection, skin disinfection, catheter placement, and dressing. The duration of the procedure was recorded in minutes from the time of site selection to the time of dressing. All data were recorded anonymously on a paper chart.
Study size
The sample size for the derivation cohort was based on the following assumptions: AUC-ROC of the multivariate logistic model of 0.95 (vs an alternative model with AUC-ROC 0.85), approximately 15% of patients with difficult venous access, 99% power, 5% alpha error, with the standard deviations in patients with and without DIVA. The sample size for the validation cohort was based on a feasibility sample of 400 patients, which allowed the same estimation with 96% power (which is deemed satisfactory). Therefore, the total sample size was 1000 patients.
Quantitative variables and statistical methods
The sample was randomly divided into two subsets: derivation (60% of the overall sample) and validation (40% of the overall sample) subsets. The procedure was as follows: in Stata 15, we generated a (pseudo)random number with uniform distribution (we set a specific seed, to ensure reproducibility), ranging from 0 to 1; subjects with random number < 0.4 were assigned to the validation cohort.
The score was developed in a number of steps in the derivation subset; after derivation, the same steps were then repeated in the validation subset, in order to assess internal validity.
In the initial models, all attempts on patients were used (with attempts classified as successful or unsuccessful) and multilevel logistic regression models with random effect per patient were fitted. Since sites of attempted cannulation were not associated to success, subsequent models were fitted on individual patients. We deem this strategy to be appropriate, since its aim is to identify “difficult” patients before any attempt at access is made (e.g. in preoperative clinical assessment).
Univariate logistic regression models were fitted to explore the association of history and clinical characteristics with DIVA. A multivariate logistic regression model was fitted, including clinically relevant variables: history of previous peripheral DIVA, vascular depletion (previous use of chemotherapy or intravenous drug abuse, previous venipunctures), coagulative disorders (including anticoagulant or antiplatelet drug intake), neurovascular disease (peripheral neuropathy and/or vasculopathy), clinical examination (dark, thick, or fragile skin evaluated by healthcare professionals according to their experience), vein evaluation (not visible, not palpable, rolling, or winding vein), and overweight and availability of one body side only (presence of arteriovenous fistula or phlebitis, surgical needs, amputation); ORs and 95% confidence intervals (CIs) were calculated.
The overall performance of the models was assessed by means of the C-statistics (AUC-ROC), pseudo-R2, Akaike Information Criterion Brier’s score, and D-statistics. Calibration was assessed both graphically (with deciles of predicted probabilities) and (in the validation subset only) by assessing slope and intercept of the linear predictor. Sensitivity, specificity, positive and negative predictive values, and proportion of patients correctly classified were also calculated.
From the final multivariate model, the coefficient for each binary variable was rounded up to the nearest higher integer. A total score was calculated by adding up individual scores.
ROC curve analysis was then performed on the total score. We decided to dichotomize patients simply into “not-difficult access” and “difficult access,” rather than using a more precise stratification system, since the final aim is to screen patients so that they can be evaluated for more advanced measures.
Sensitivity, specificity, positive and negative predictive values, and proportion of patients correctly classified at several cut-offs were also calculated. The final cut-off was chosen in such a way as to maximize sensitivity and specificity. Stata computer software version 15.0 (Stata Corporation, College Station, TX, USA) was used for statistical analysis.
Results
Participants
Overall, 1006 patients were included (607 in the derivation cohort and 399 in the validation cohort); of these, 127 patients (12.6%) were found to have peripheral DIVA (72 in the derivation and 55 in the validation cohorts, respectively).
Descriptive data
General data and all data related to the different parameters considered in the univariate analysis and associated with peripheral DIVAs are shown in Table 1, for both subsets.
Parameters associated to peripheral DIVA in the derivation and validation cohorts (univariate analysis).
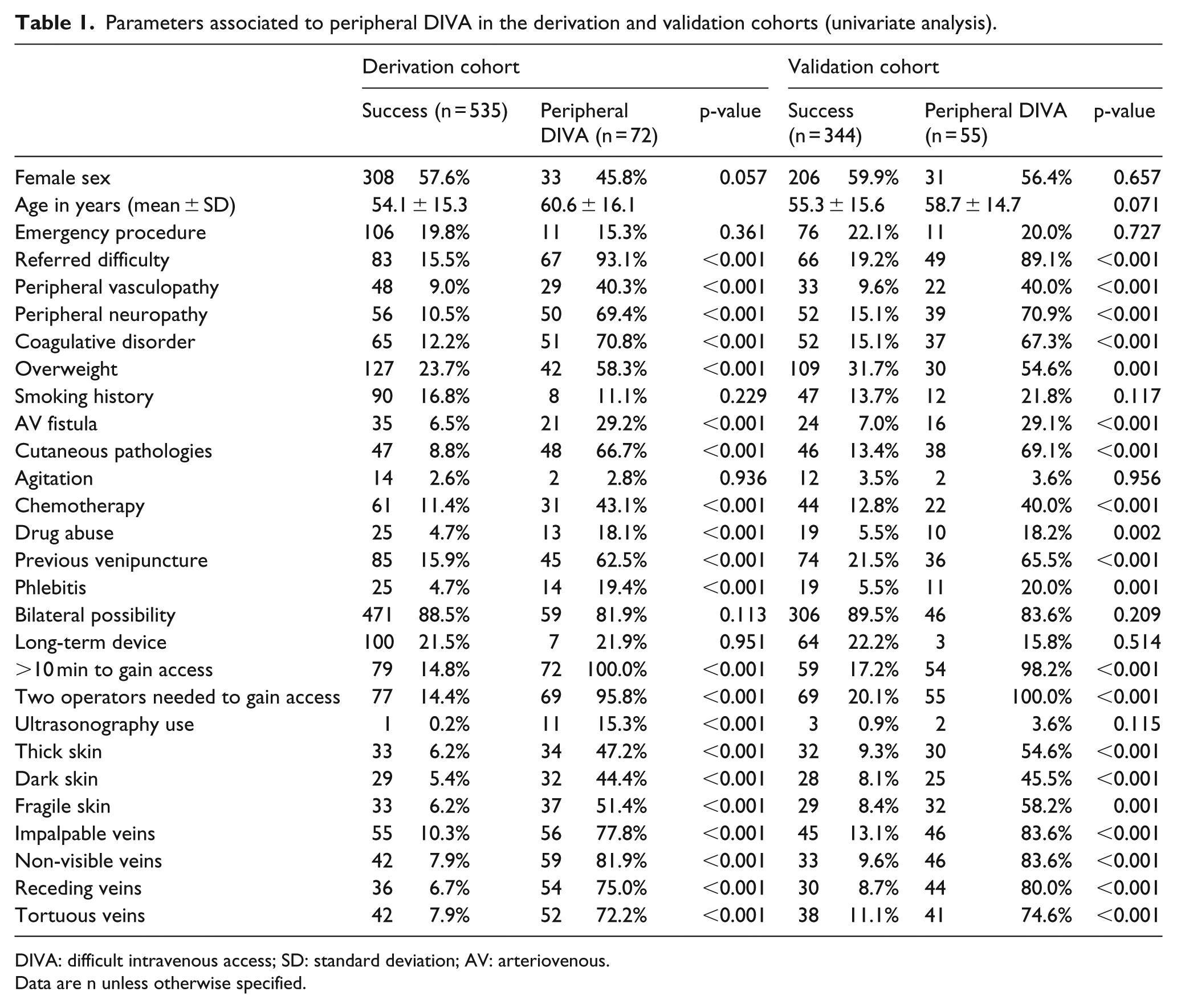
DIVA: difficult intravenous access; SD: standard deviation; AV: arteriovenous.
Data are n unless otherwise specified.
Outcome data and other analyses
Our model showed good properties (Table 2), with high discrimination (C-statistics close to 1; Figure 1), good calibration (Supplementary Figure 1), low Brier’s score (close to 0) and high Somers’ D in both cohorts.
Multivariate logistic regression model for difficult intravenous access (DIVA; with general performance measures of the model) in the derivation and validation cohorts.
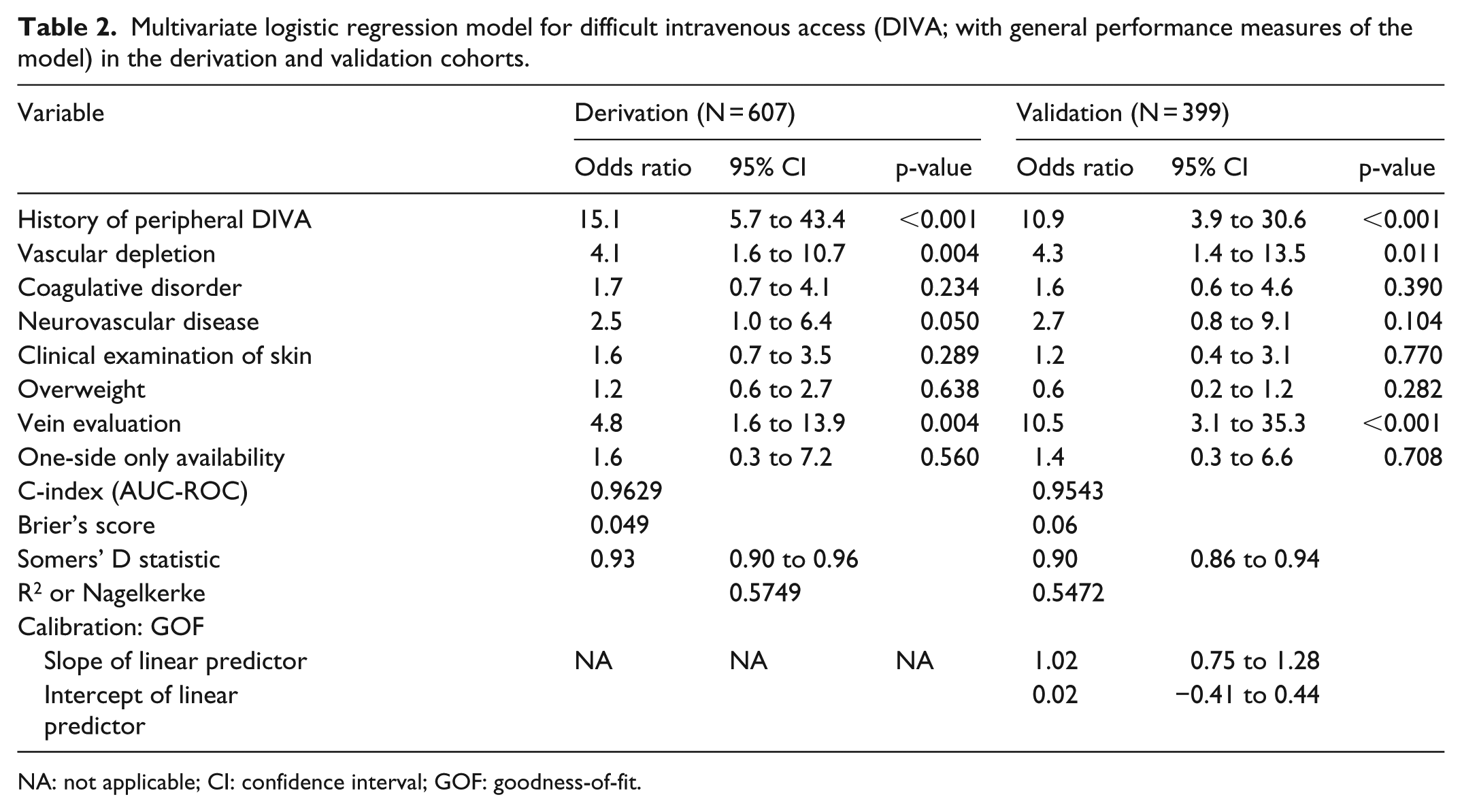
NA: not applicable; CI: confidence interval; GOF: goodness-of-fit.
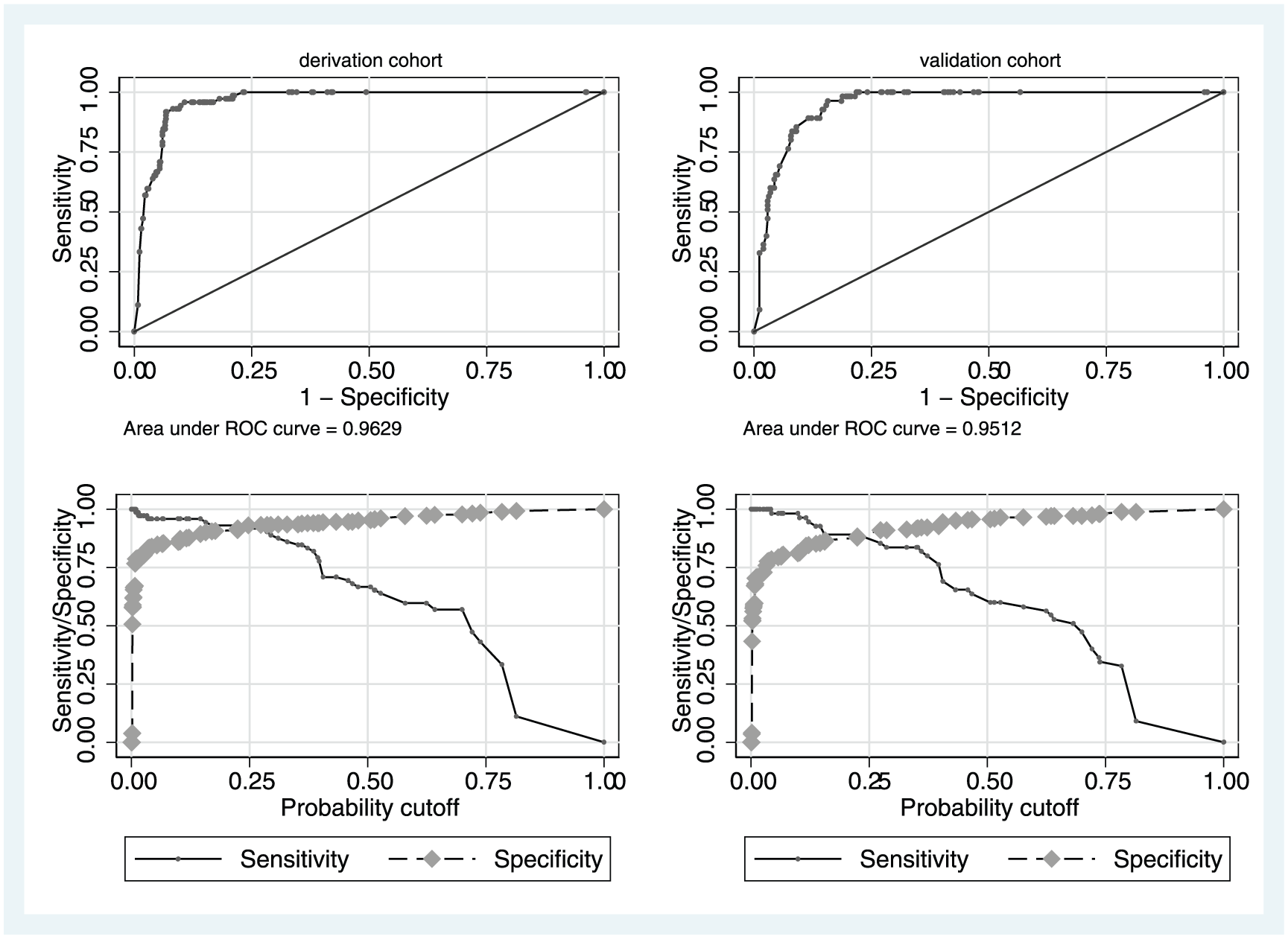
Discrimination and predictive validity of the final multivariate logistic regression model for lack of successful cannulation.
The slope of linear predictor in the validation cohort was notably excellent too (with slope close to 1 and intercept close to 0). The scores assigned to individual variables are shown in Supplementary Table I.
Main results
The individual overall score therefore ranged from 0 to 12 points. The median overall score was 2 (interquartile range (IQR): 1–6) in the derivation cohort and 2 (IQR: 1–7) in the validation cohort (Supplementary Figure 2). The ROC curve analysis of the final score (Figure 2) indicates a very high discriminatory power in both cohorts.
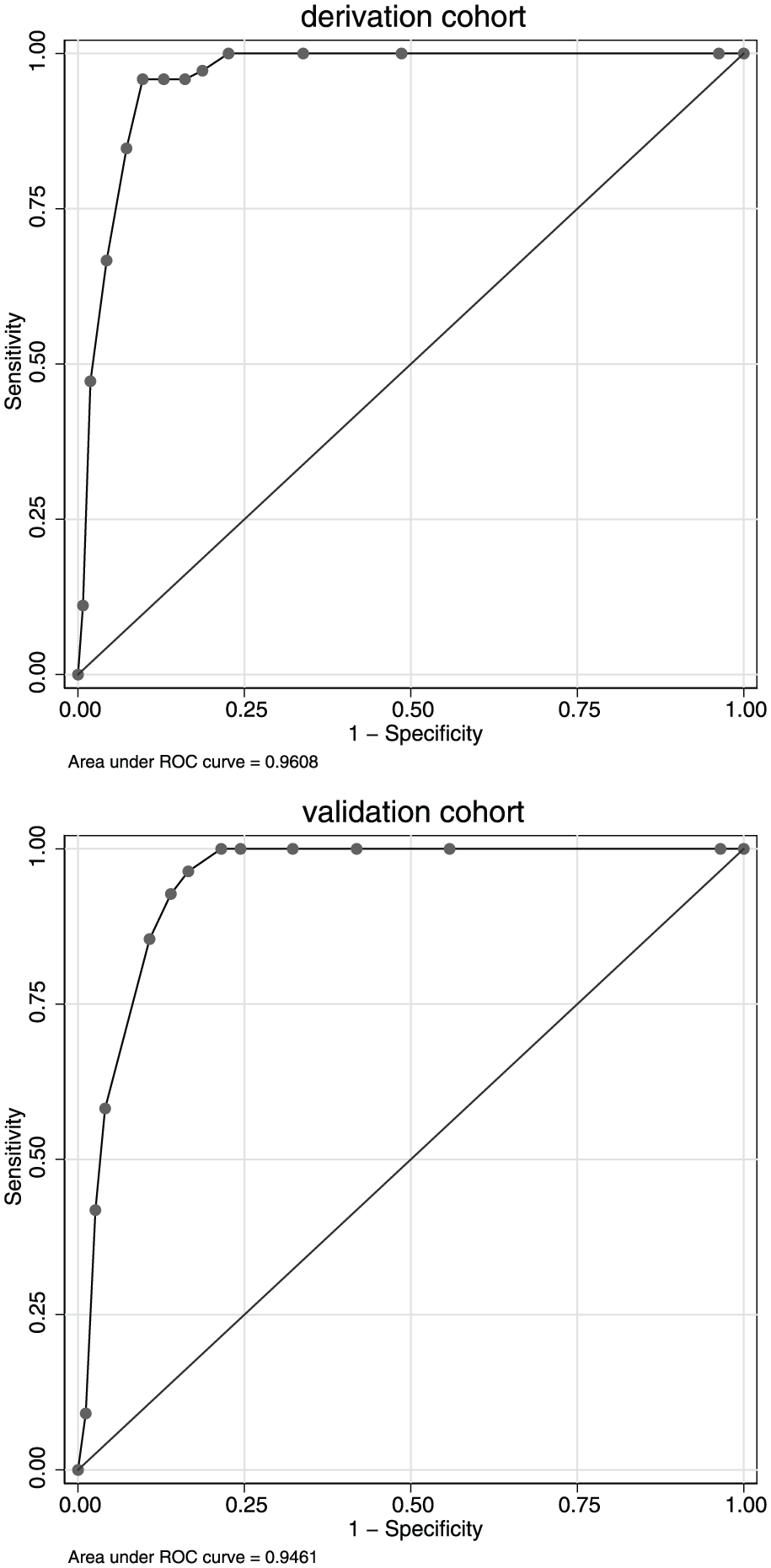
ROC analysis of the final score.
We developed an eight-criteria scale (EA-DIVA (Enhanced Adult DIVA) score), shown in Table 3, with a chosen cut-off of 8; the score performance at the cut-off point is shown in Table 4.
Operative EA-DIVA score.
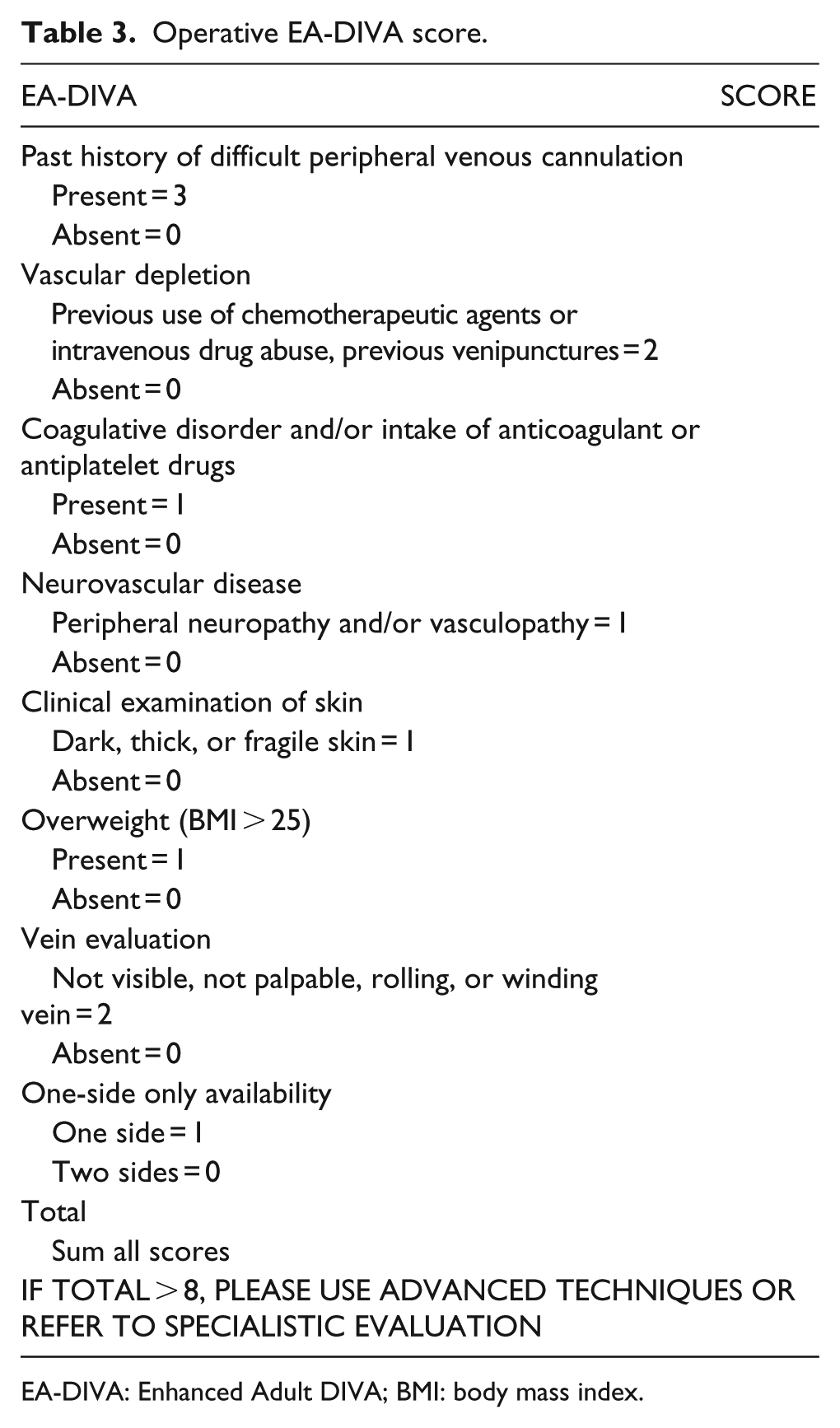
EA-DIVA: Enhanced Adult DIVA; BMI: body mass index.
Score performance at the cut-off.
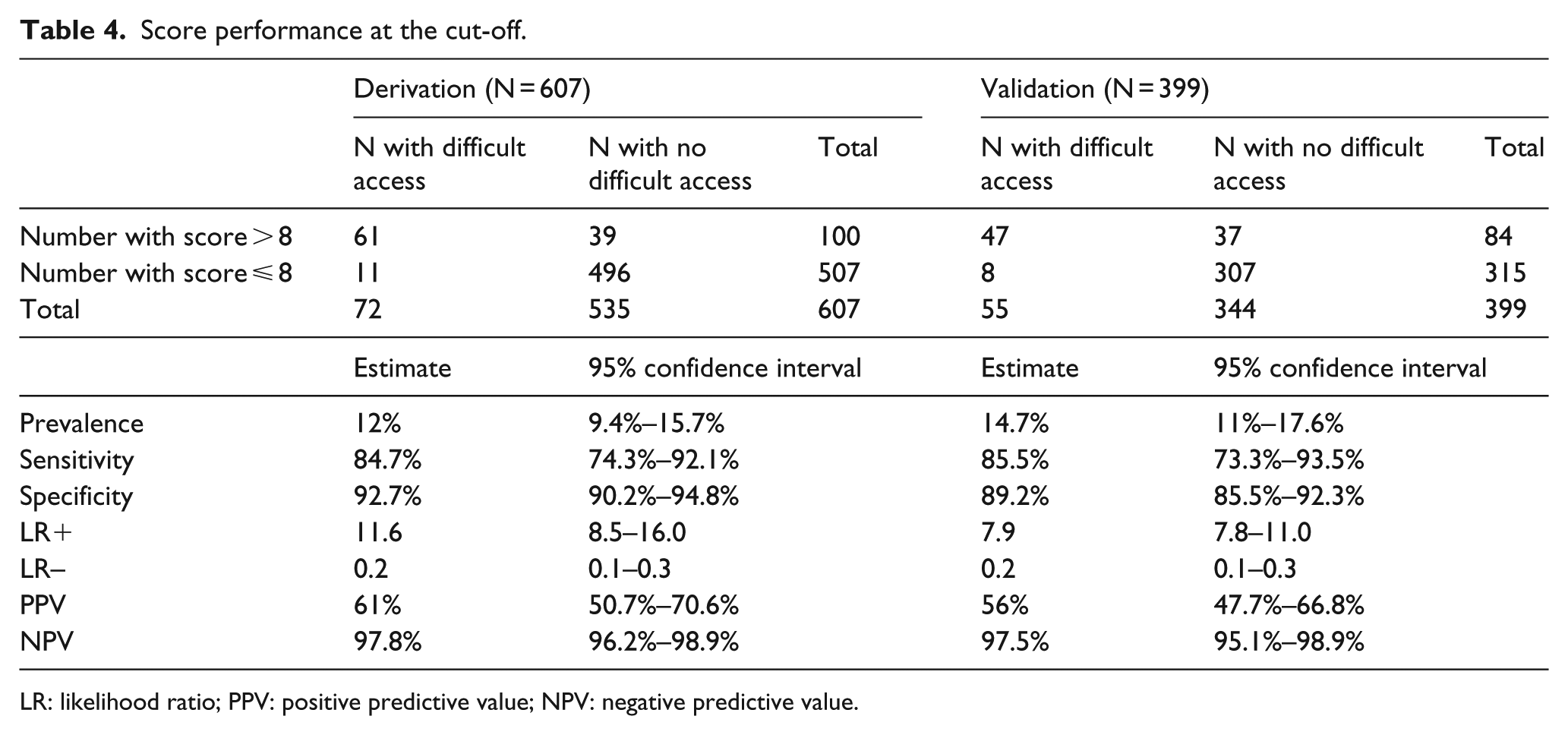
LR: likelihood ratio; PPV: positive predictive value; NPV: negative predictive value.
Discussion
Key results
We developed and validated the EA-DIVA score, a new scale to assess the difficulty of venous access in patients undergoing elective or urgent surgery. This scale is different to the previously published ones.14–16
The EA-DIVA score has eight simple criteria to be assessed in a preoperative appointment or during hospital admission. With a cut-off of 8 points out of 12, the EA-DIVA score has good discriminatory properties, since it can clearly distinguish patients with easy access from those at risk of a difficult one, thus reducing the complications associated with the procedure. 17
Previous studies regarding chemotherapy and DIVA provide inconsistent results. The A-DIVA study group did not find any association between the use of chemotherapeutic agents and the rate of failure in ensuring PIV access, neither in the univariate nor in the multivariate analysis. 15 On the contrary, in a recent study Fields et al. 12 found that chemotherapy is a relevant risk factor for peripheral DIVA. Our data coincide with the latter study: we observed a relationship between vascular depletion (due to chemotherapy or to other causes) and DIVA, even though this correlation was not as strong as the one for history of peripheral DIVAs.
In order to simplify the usability of our scale, we clustered the most relevant visual aspects of venous access detection (i.e. veins not visible, not palpable, or elusive) into a simple and single parameter: “Vein evaluation.” We believe in the importance of a holistic evaluation of the actual visible venous pool, rather than considering single measurements like the diameter of the vein as a parameter to evaluate the difficulty of PIV access. 15
We included a parameter for clinical examination of the skin (dark, thick or fragile skin, scars, wounds, or burns) in order to offer a more complete approach in a hospital setting, which is characterized by different types of patients in terms of age and origin.
In addition, we applied parameters of “one-side only availability” and “neurovascular disease” (the latter includes phlebitis, limb paresis, or peripheral neuropathy) as the surgical subspecialties considered for our analysis often included patients with venous access limited to a single arm (vascular surgery) or patients from the neurosurgery and stroke unit.
Other anamnestic data, such as coagulation disorders, anticoagulant drugs, or antiplatelet drugs, were relevant in our statistical model. A possible clinical explanation may be related to a higher tendency to create hematomas after a failed attempt in these patients, thus making it impossible to find new PIV access in the same area and consequently limiting the accessible venous pool. Further studies are needed to better interpret this correlation.
We did not observe a difference between elective and urgent surgery patients, contrary to other studies.15,17,18 This may be due to the fact that our series included surgical operations that were not yet complicated by hemodynamic alterations, and not only patients with hypovolemia, hypotension, or shock.
In the A-DIVA study, BMI had a significant effect in the univariate analysis, but it was not included in the multivariate analysis because of a p-value limited to <0.01. In our scale, an overweight condition is taken into account. Different sampling or larger cohorts may clarify this issue.
For our scale, we selected the cut-off of 8 points out of 12, because this could reliably predict those patients with no difficulty (negative predictive value of 97.5% in the validation cohort), while at the same time identifying patients at high risk of peripheral DIVA (positive predictive value of 56% in the validation cohort), without overloading the preoperative procedures (only one-fifth of the patients fall within this high-risk category).
Limitations
The main strength of this study is the large sample size of both the derivation and the validation cohorts, entirely made up of prospectively enrolled patients. Nevertheless, we acknowledge some potentially relevant limitations, such as the fact that the scale was only internally validated; 19 for this reason, we are currently planning a validation in a different population. A further limitation is the qualitative nature of our parameters “clinical examination of skin” and “vein evaluation.” Moreover, we mainly included Caucasians in our study, with only a limited proportion of patients with dark skin, and thus our results might not accurately reflect other races.
Interpretation
In practice, our scale might help clinicians in choosing the best strategy for peripheral vein cannulation well in advance of surgery. For instance, a proactive strategy for patients with a score greater than 8 could be to assign the task to more expert personnel or to use ultrasonography from the outset, to guide cannulation. In doing so, patients will have the advantage of obtaining PIV access in a dedicated setting, before they reach the operating theater. In addition, a proactive approach could reduce the number of central venous catheters placed as final solutions after multiple unsuccessful attempts, in favor of a higher rate of peripheral vein or deep vein ultrasound-guided cannulations. 20
The identification of the correct type of venous catheter tailored to the needs of the individual patient and the early involvement of an expert in the case of peripheral DIVA may ensure benefits not only in terms of time-saving but also in terms of cost-effectiveness. In clinical practice, we suggest adopting our scale before any attempt is made to cannulate, in order to plan proactive measures in advance for patients who are most likely to need them. If the score is higher than 8, the proper strategy will depend on local procedures and clinical context. If the scale is used in the operating theater or in cases of emergency, our proposed strategy is to use ultrasonography immediately in order to better evaluate the patient’s vein asset.17,21 If no superficial veins are available, we suggest choosing a mini-midline (i.e. long peripheral cannula, approximately 8–10 cm in length) or a midline catheter and proceed to a deep vein cannulation. On the other hand, if the scale is used in presurgical evaluation or in a medical ward, the more sensible choice might be to assign the task to an expert and to schedule the venipuncture in advance.
Generalizability
Finally, our score was developed in the preoperative setting, but we believe that it could be useful in other contexts. In fact, the patient-related characteristics included in our score are easily identifiable not only in surgical patients but also in medical patients (i.e. in general wards) or in emergency room (ER) patients. Another potential development would be its inclusion in the Emergency Medical Services (EMS) system, to flag up likely DIVA and allow operators to choose an alternative promptly if a life-saving infusion is needed (intraosseous (IO) access) or to act as a preventive measure, opting to wait for an expert to carry out PIV access in hospital if it is not mandatory in the prehospital setting.
Further studies are needed to confirm the validity of EA-DIVA in hospital wards, ER, and EMS, but it is realistic to assume its usefulness in those settings as well.
Conclusion
We developed and validated an eight-item scale that adequately predicts peripheral DIVAs for both elective and emergency surgery, hypothetically applicable also in medical ward, ED, and EMS, in order to safeguard the comfort of the patient. Its use may also lead to a better individualization of preoperative procedures, thus resulting in an advantage in terms of costs and time-saving.
Supplemental Material
Supplemental_material – Supplemental material for EA-DIVA score (Enhanced Adult DIVA score): A new scale to predict difficult preoperative venous cannulation in adult surgical patients
Supplemental material, Supplemental_material for EA-DIVA score (Enhanced Adult DIVA score): A new scale to predict difficult preoperative venous cannulation in adult surgical patients by Giuseppe Civetta, Sergio Cortesi, Mattia Mancardi, Antonella De Pirro, Marta Vischio, Marco Mazzocchi, Luigia Scudeller, Andrea Bottazzi, Giorgio A Iotti and Alessandra Palo in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors would like to thank Lorenzo Bellini, MD, Eric Arisi, MD, and all the medical and nursing staff working in the operating theater of the DEA department at Fondazione IRCCS Policlinico San Matteo of Pavia for their invaluable help in data collection. They would also like to thank Daniele and Davide Bongetta for their suggestions during the writing phase.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.