
Abstract

This study aimed to evaluate the safety and feasibility of totally implantable venous access device (TIVAD) placement in patients’ home. The importance of TIVAD is increasing, particularly for patients receiving medical treatment at home. A TIVAD could be used for a long period of time, and the risk of infection is low compared with peripherally inserted central catheter. 1 In Japan, TIVAD placement is typically performed in the hospital. For patients receiving home medical treatment, repeated outpatient treatment and hospitalization are a heavy burden on the patients and their family. It is desirable for them to place TIVAD in the patient’s home. Six consecutive patients who had TIVAD placement in their homes from September 2015 to May 2017 were enrolled in the study (Table 1). All patients received home medical treatment because they wanted to spend the rest of their lives at home and were in need of TIVAD placement. We evaluated their adaptation to TIVAD placement according to the Guideline of Home Parenteral Nutrition. 2 We used the PowerPort isp MRI (Bard Access Systems Inc., Salt Lake City, UT, USA). TIVAD placement was performed by puncturing the right internal jugular vein or cephalic vein as previously reported.3,4 Data on patients’ cases, average operative time, safety, complications, and prognoses were obtained. Written informed consent from each patient was obtained before the procedure. TIVAD placement was performed on four patients with malignant tumors, one patient with multiple system atrophy (MSA) where gastrostomy could not be performed, and one patient with vascular dementia following cerebral infarction whose family refused gastrostomy. No perioperative complications were observed. Mean operation time was 37 min and mean time to prepare TIVAD placement in the patients’ home was 65 min. The average follow-up period was 268 days. Four patients died because of the original disease, one patient died because of complicated pneumonia, and one patient survived. Postoperative complications were not observed (Table 1). Preparing strategies and ensuring a suitable surgical environment are important. A manual for TIVAD placement was prepared to ensure that the procedure is performed with no failure and delay. Problems such as arrhythmia and infection are also important. We monitored cardiac arrhythmias with a heart rate monitor during procedure and ensured that the catheter was not inserted deep into the right atrium. In addition, we performed the placement using maximal barrier precaution and administered antibiotics just before placement. We washed all sites including subcutaneous wound and skin incision with normal saline and then closed incisions.
Comparison of patients and results.
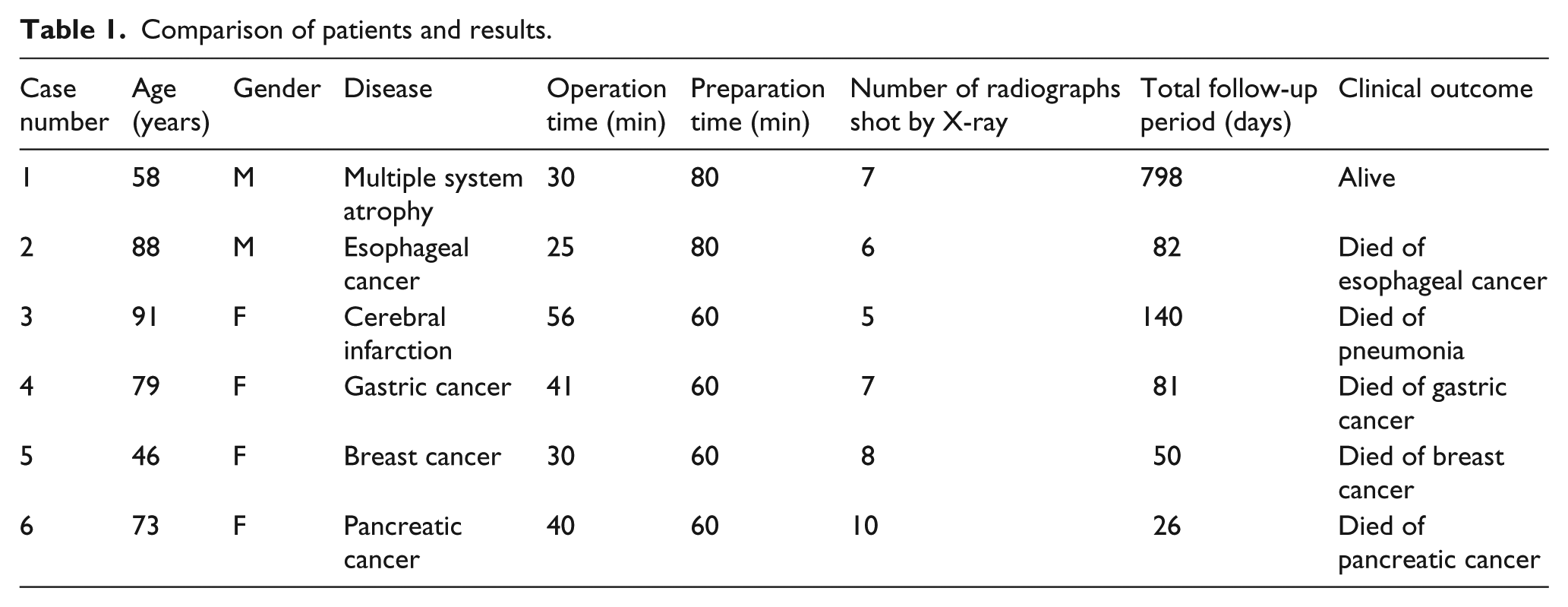
Consequently, no complications were observed in all patients. The time required for placement in the patient’s home (34.3 min) was not significantly different from that in the hospital (37 min), which we previously reported. 3 The average radiographic shots by X-ray shooting was 7.2 times, which involved a lower dose of radiation compared with X-ray fluoroscopy. Considering all indications, we found that TIVAD placement could be performed safely even in the patients’ home, especially for cancer patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.