
Abstract
Objective:
To evaluate the role of preoperative peripheral blood neutrophil-to-lymphocyte ratio in predicting early arteriovenous fistula failure. The impact of postoperative neutrophil-to-lymphocyte ratio on arteriovenous fistula failure was also investigated.
Methods:
Medical records from 470 patients who underwent first-time arteriovenous fistula creation were studied. Demographic, clinical, and laboratory data were obtained. Receiver operating characteristic curves were constructed to determine the optimal cutoff values of preoperative and postoperative neutrophil-to-lymphocyte ratios for predicting early arteriovenous fistula failure. Univariate and multivariate analyses were performed to evaluate whether the neutrophil-to-lymphocyte ratio parameters were prognostic indicators for arteriovenous fistula failure.
Results:
Complete data from 396 patients were studied. The prevalence of early arteriovenous fistula failure was 30.6%. The optimal cutoff values of preoperative and postoperative neutrophil-to-lymphocyte ratios for predicting early arteriovenous fistula failure were 2.7 (82.6% sensitivity and 52.0% specificity) and 2.9 (78.5% sensitivity and 73.1% specificity), respectively. By univariate and multivariate analyses, high preoperative and postoperative neutrophil-to-lymphocyte ratios were significantly associated with early arteriovenous fistula failure. The adjusted odds ratios were 5.46 (95% confidence interval: 3.15–9.48) and 7.19 (95% confidence interval: 4.12–12.55), respectively.
Conclusions:
High preoperative and postoperative neutrophil-to-lymphocyte ratios significantly predict early arteriovenous fistula failure.
Introduction
A native arteriovenous fistula (AVF) is a vascular access point for hemodialysis in end-stage renal disease (ESRD) patients and has been widely used for over five decades. 1 An AVF is recommended by the National Kidney Foundation Kidney Disease Outcomes Quality Initiative as the first choice for hemodialysis access because it yields superior results to other modes of access in terms of greater durability and fewer morbidities. 1 Despite its advantages, one of the drawbacks of an AVF is that it requires time to mature before its use. In addition, the rates of early AVF failure, mainly resulting from venous stenosis,2–4 have been reported to be as high as 20%–60%.5,6 The consequences of early AVF failure include the need for temporary hemodialysis catheter placement and further surgical intervention, which subsequently increase the risk of morbidity and mortality as well as hemodialysis access care costs. From a practical viewpoint, the identification of patients at risk for early AVF failure would be advantageous because these patients would be thoroughly counseled regarding their increased risk and receive a specialized treatment plan, such as close monitoring after AVF creation or use of other types of access instead.
Recent data have suggested a link between inflammation and early AVF failure. Several studies have reported a significant increase in C-reactive protein (CRP) in patients with early failure compared to those who had a successful AVF.7–9 However, its possible role as a predictor of AVF failure has not been confirmed as an independent factor. 9
Aside from CRP, features of red blood cells and white blood cell (WBC) differential including the neutrophil-to-lymphocyte ratio (NLR) have also been reported as prognostic indicators for AVF failure.9–11 The relationship between WBCs particular NLR, which reflect the inflammatory process, and AVF failure has been studied either as preoperative9,10 or postoperative markers. 11 Previous studies have showed that a high level of NLR was associated with AVF failure in either early 10 or late settings. 11 Hence, utilizing the leukocyte profile, which is simple, low-cost, and generally included in the preoperative and postoperative investigations, as an adjunctive tool to identify at-risk patients would then have a great cost benefit, especially in low-resource settings.
This study aimed to evaluate the role of preoperative peripheral blood NLR in predicting early AVF failure. The impact of postoperative NLR as well as the change in the preoperative/postoperative NLR on AVF failure was also studied.
Methods
Study design and patient selection
This retrospective study was approved by the Vajira Institutional Review Board (Approval Number 025/2561). Medical records from ESRD patients who underwent first-time AVF creation at the Department of Surgery, Faculty of Medicine Vajira Hospital between January 2011 and June 2017 were reviewed. The inclusion criteria consisted of patients who underwent autogenous radiocephalic AVF creation and had available preoperative and postoperative complete blood counts (CBCs) that had been measured in the institutional laboratory. The CBCs must have been measured in the morning, within a week prior to and within 14 days after AVF creation. If several CBCs were measured, the one measured closest to the day of surgery was recorded. The exclusion criteria consisted of patients who had a WBC count greater than 10,000 cells/µL or any condition that may affect WBC and differential counts, such as immediate past, current history, or signs or symptoms of infection; hematologic disease; and recent (14 days or less) steroid intake. Patients whose dialysis started later than 3 months after AVF creation as well as those who were lost to follow-up during the first 3 months after surgery or had incomplete data were also excluded.
Patient care
As part of the standard ESRD care at the institution, blood parameters, including CBCs, were monitored at regular intervals (i.e. every 2–3 months) to assess patients’ general health status and as a surveillance for any consequences of chronic renal failure including anemic and thrombocytopenic conditions. 12 The CBC was also assessed before and after AVF surgery. All CBC specimens, including WBC and differential counts, were measured using an automatic counter (model Unicel DxH 800; Beckman Coulter, Inc., Brea, CA, USA). The laboratory personnel calibrated the machine three times daily for quality control. The acceptable range of intra-assay coefficients of variation for WBC and differential counts was less than 3%.
Follow-up evaluations were performed at 2 weeks after AVF surgery and then every month for an additional 3–6 months to monitor AVF success or failure as well as complications. If an AVF failed to function or any complications occurred, an additional intervention was implemented.
Data collection
The data collected included age; gender; body mass index (BMI); systolic and diastolic blood pressure; phase of AVF creation (before or after hemodialysis initiation); comorbid conditions that influence AVF function; current medications, including antithrombotic agents and statins; preoperative and postoperative NLRs; and the presence or absence of early AVF failure. Comorbid conditions included diabetes mellitus, hypertension, cardiovascular and cerebrovascular diseases, hyperlipidemia, and a history of heart failure.
The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. The optimal cutoff points on the receiver operating characteristic (ROC) curves of preoperative and postoperative NLRs were determined and used to divide the patients into two groups of high NLR (above cutoff point) or low NLR (at cutoff point or below). Changes in preoperative/postoperative NLRs were categorized into four subgroups: low/low, low/high, high/low, and high/high.
The diagnosis of early AVF failure was made when an AVF was not successfully cannulated or could not be used for hemodialysis by the third month following its creation despite interventions. 2 A successful AVF was defined when fistula cannulation could be used for hemodialysis.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics version 22.0 (IBM corporation, Armonk, NY, USA). Categorical variables are presented as numbers with percentages, and continuous variables are presented as the means with standard deviations. The chi-square test was used to compare categorical variables, and Student’s t-test was used to compare continuous variables. ROC curves were constructed to determine the performances of preoperative and postoperative NLRs to predict early AVF failure. The odds ratios (ORs) with 95% confidence intervals (CIs) of early AVF failure in patients with a high preoperative NLR, a high postoperative NLR, and changes in preoperative/postoperative NLR were analyzed by multivariate analysis and adjusted for potential confounding factors. A value of p < 0.05 was considered statistically significant.
Results
A total of 470 ESRD patients who underwent first-time AVF creation during the study period were identified. Of these, 74 patients (15.7%) were excluded due to the following reasons: suspicion or diagnosis of infection (n = 32), no dialysis commencement within 3 months of AVF creation (n = 7), loss to follow-up (n = 26), and incomplete data (n = 9). Hence, 396 patients were recruited into the study. Among these, 202 (51.0%) were male and 194 (49.0%) were female. The mean age was 61.2 ± 14.5 years (range 19–91 years).
The AVF creation was performed prior to the dialysis in 230 patients (58.1%) and after hemodialysis initiation in 166 patients (41.9%). The prevalence of early AVF failure was 30.6%. The characteristic features of patients who had AVF failure or success are presented in Table 1. The patients with AVF failure had significantly higher mean preoperative and postoperative NLRs but lower mean BMI, systolic and diastolic blood pressure, and rate of AVF created in the pre-dialysis phase compared to the patients with successful AVF. The other characteristic features of age, gender, the presence of comorbidities, and the use of antithrombotic agent and statin were similar between both groups.
Characteristics of the study population.
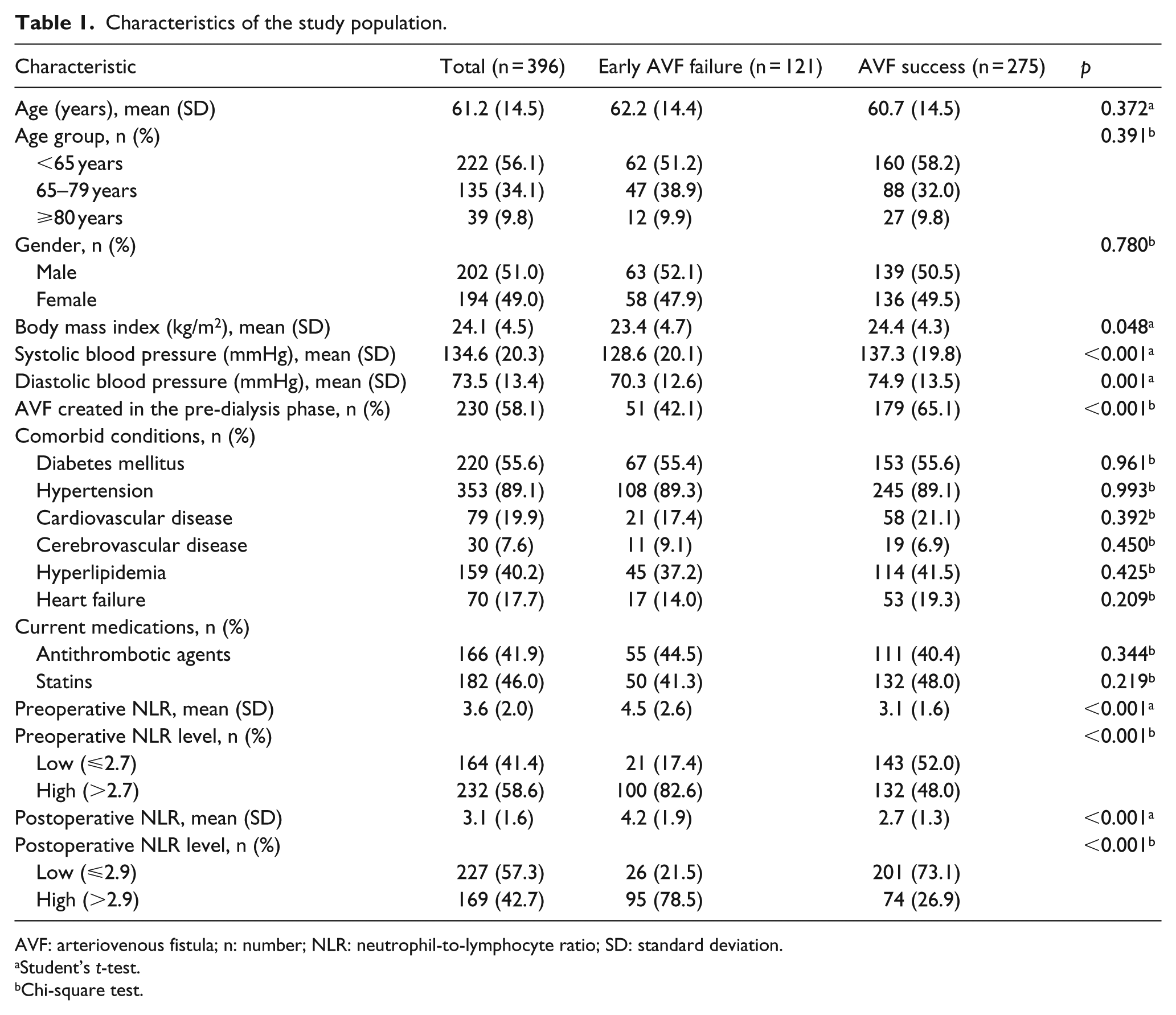
AVF: arteriovenous fistula; n: number; NLR: neutrophil-to-lymphocyte ratio; SD: standard deviation.
Student’s t-test.
Chi-square test.
Figure 1 shows the ROC curves of preoperative and postoperative NLRs. The calculated areas under curves were 0.695 (95% CI: 0.640–0.750) and 0.785 (95% CI: 0.734–0.836), respectively. The optimal cutoff point of preoperative NLR was 2.7 which yielded 82.6% sensitivity and 52.0% specificity to predict early AVF failure. Regarding postoperative NLR, the optimal cutoff point was 2.9. At this cutoff value, the sensitivity was 78.5% and specificity was 73.1%. Details of the predictive performances of both optimal cutoff points are shown in Table 2.
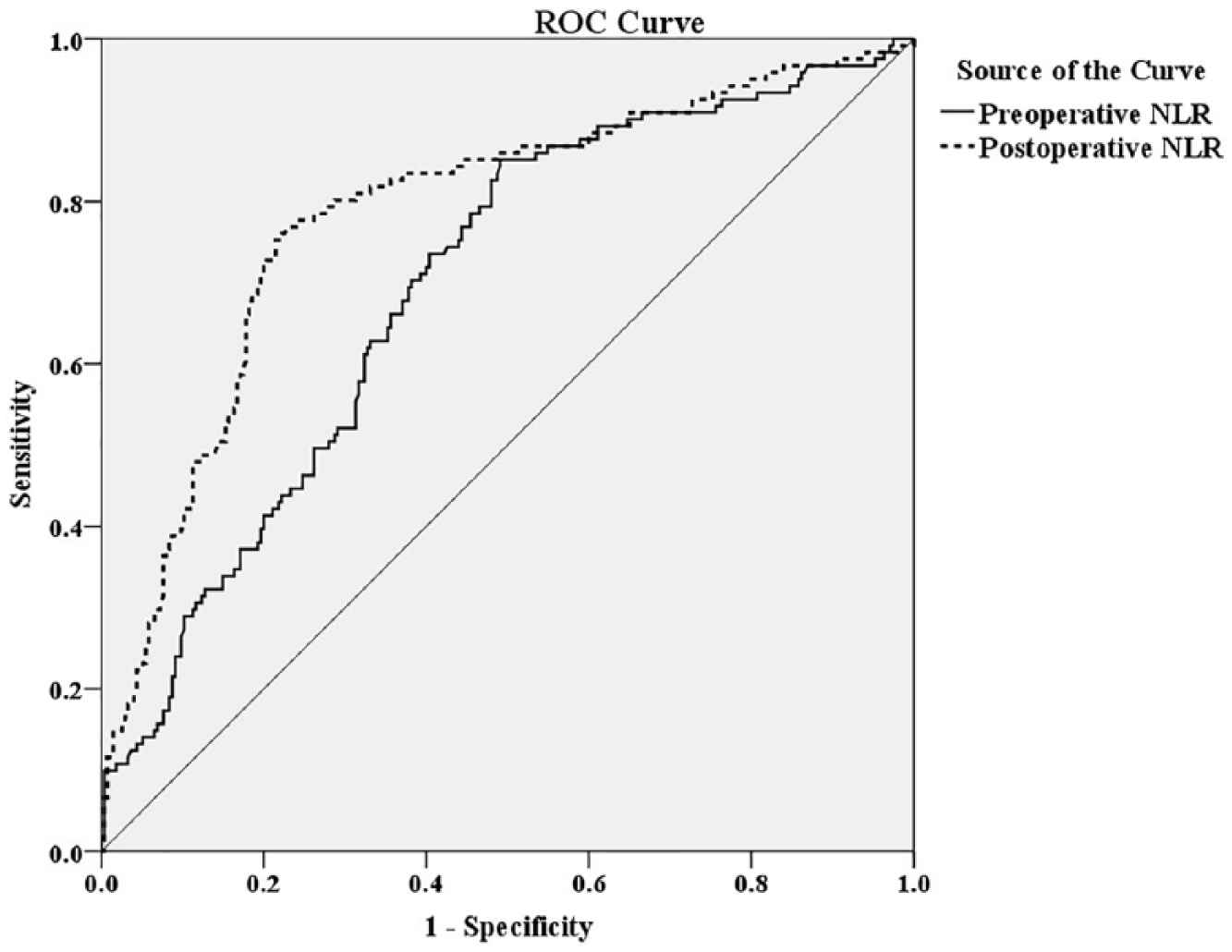
Receiver operating characteristic curves of preoperative and postoperative peripheral blood neutrophil-to-lymphocyte ratios for predicting early arteriovenous fistula failure.
Predictive performances of the optimal cutoff points of preoperative and postoperative NLRs.
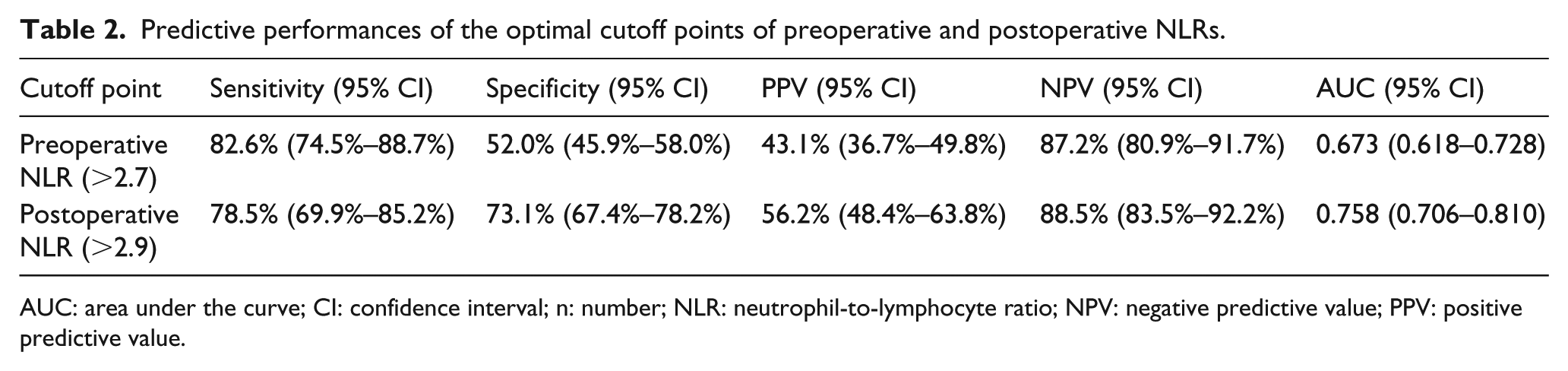
AUC: area under the curve; CI: confidence interval; n: number; NLR: neutrophil-to-lymphocyte ratio; NPV: negative predictive value; PPV: positive predictive value.
Among the 396 patients, 232 (58.6%) had high preoperative NLR (NLR > 2.7), whereas 169 (42.7%) had high postoperative NLR (NLR > 2.9). The crude ORs of significant variables in Table 1 and their adjusted ORs are shown in Table 3. Both preoperatively and postoperatively high NLRs were independent prognostic factors for early AVF failure. The adjusted ORs were 5.46 (95% CI: 3.15–9.48) for high preoperative NLR and 7.19 (95% CI: 4.12–12.55) for high postoperative NLR. On the contrary, a rise in systolic blood pressure and AVF created in the pre-dialysis phase was protective factor for AVF failure. The adjusted ORs were 0.98 (95% CI: 0.97–0.99) and 0.44 (95% CI: 0.26–0.75), respectively.
Crude and adjusted ORs for early AVF failure according to various variables.
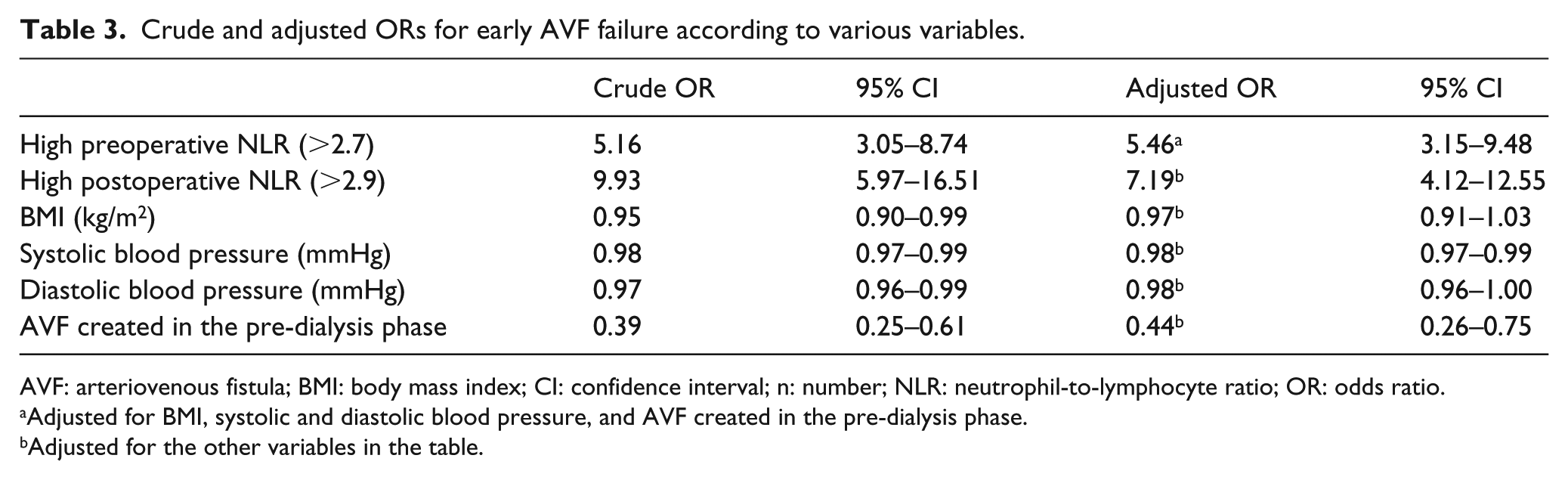
AVF: arteriovenous fistula; BMI: body mass index; CI: confidence interval; n: number; NLR: neutrophil-to-lymphocyte ratio; OR: odds ratio.
Adjusted for BMI, systolic and diastolic blood pressure, and AVF created in the pre-dialysis phase.
Adjusted for the other variables in the table.
The impact of NLR was explored according to the time of AVF creation in relation to the dialysis. The risks of AVF failure in association with high preoperative or postoperative NLRs were attenuated if the AVF creation was performed prior to the dialysis. The adjusted ORs of preoperative and postoperative NLRs dropped to 4.48 (95% CI: 2.08–9.61) and 6.05 (95% CI: 2.87–12.73), respectively. In contrast, when an AVF was performed after the dialysis, the risks of AVF failure were fortified with increased adjusted ORs of preoperative and postoperative NLRs to 7.23 (95% CI: 3.24–16.15) and 9.06 (95% CI: 3.81–21.58), respectively.
The rates of early AVF failure in relation to the changes in preoperative/postoperative NLR are presented in Table 4. Patients with high/high NLRs had the highest AVF failure rate, followed by the low/high, high/low, and low/low subgroups. The high/high and low/high NLRs were identified as independent predictors of AVF failure. The adjusted ORs were 19.14 (95% CI: 9.24–39.62) and 4.71 (95% CI: 1.73–12.82), respectively.
Crude and adjusted ORs for early AVF failure according to changes in preoperative/postoperative NLRs.
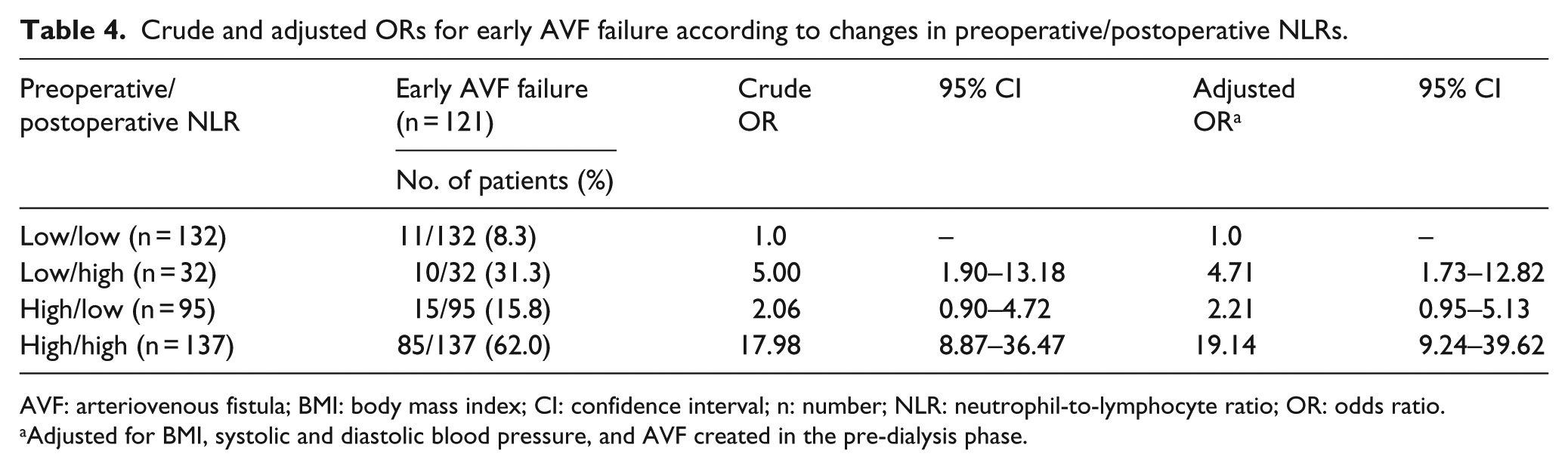
AVF: arteriovenous fistula; BMI: body mass index; CI: confidence interval; n: number; NLR: neutrophil-to-lymphocyte ratio; OR: odds ratio.
Adjusted for BMI, systolic and diastolic blood pressure, and AVF created in the pre-dialysis phase.
Discussion
Over the past decades, extensive research has been conducted to improve the patency of AVFs. An association between inflammation and AVF failure was reported in many studies.13–15 Inflammation in the setting of AVF surgery can originate either from a systemic inflammation caused by uremia itself or from a local inflammatory response following the injury due to fistula creation.14–18
Among various measurable parameters in peripheral blood that reflect the systemic inflammatory state, the NLR is a simple parameter that shows a positive correlation with levels of other inflammatory markers including CRP, interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) in ESRD patients.19–21 To date, only one study has reported an effect of high preoperative NLR on early AVF failure. 10 This report by Usman et al. on 300 patients who underwent AVF creation identified the NLR as a predictor of early AVF failure with an adjusted OR of 1.39. 10 At a cutoff value of ⩾2.65, the sensitivity and specificity for predicting early AVF failure were high (98% and 80%, respectively). In line with the findings of Usman et al., this study found that a high preoperative NLR was an independent risk factor for early AVF failure; however, with greater OR of 5.46. At a slightly higher cutoff value of 2.7, this study found lower sensitivity (82.6%) and specificity (52.0%) for predicting early AVF failure compared to their study. The differences might rest on many factors. Aside from different characteristic features of populations studied, criteria used to define early AVF failure and various variables included in the multivariate analysis were also different. This study framed a 3-month period as the maximal duration to define early AVF failure, whereas their study allowed a shorter period of 8 weeks. 10
In clinical practice, the preoperative NLR would probably be more useful than the postoperative one because the AVF creation could be selected in those with low risk of early failure. Regarding the clinical utility of postoperative NLR, one study reported it as a useful prognostic marker for late failure. 11 This study, therefore, investigated and found postoperative NLR and the change in the preoperative and postoperative NLR were independent indicators for early AVF failure. The sensitivity and specificity of postoperative NLR were, respectively, slightly lower (78.5% vs 82.6%) and much higher (73.1% vs 52.0%) than those of preoperative NLR. From the statistical point of view, a test or parameter that yields a higher specificity would reflect a higher possibility of the diagnosis. Hence, the postoperative NLR might serve better to identify individuals at risk of early AVF failure and to alert a surgeon for an awareness, early detection, or early intervention after surgery.
Regarding the impact of the change in the preoperative/postoperative NLR on AVF outcomes, the findings of adjusted ORs of 2.21, 4.71, and 19.14 for early AVF failure in patients with high/low, low/high, and high/high NLRs, respectively, in this study indicated a direct association of the magnitude of the OR with the degree of change in preoperative/postoperative NLR. These findings revealed the importance of evaluating the NLR at both the preoperative and postoperative time points, as patients in the low/low subgroup appeared to have a good prognosis, whereas those in the high/high subgroup had a worse outcome. Moreover, the results of this study showed that patients with high preoperative NLRs who had a low NLR in the postoperative period had a better AVF outcome than patients whose NLRs remained high after surgery. These results suggested that a change in preoperative/postoperative NLR may reflect the dynamic alterations of the patient’s inflammatory status as well as the impact of AVF placement on the inflammatory response. The underlying mechanisms responsible for a decrease in the NLR after AVF surgery are needed to be explored further. Future research is also required to determine the effects of dynamic changes of host inflammatory response on the outcomes of AVF in both the short-term and long-term periods.
This is the first study to evaluate the impact of both preoperatively and postoperatively high NLRs and the preoperative/postoperative change on the risk of early AVF failure. The findings of this study suggested that the risk of AVF failure was accentuated when the AVF creation was performed after hemodialysis initiation. The strength of this study was that the AVF created in each patient was new. Hence, the effect of multiple venous injuries could be reduced. In addition, blood samples from all patients were taken in the morning; therefore, the diurnal variation in WBCs, which may affect NLR measurements, was lessened. Furthermore, all the CBC specimens were examined using the same automated hematology analyzer with regular calibration to establish accurate and reliable results. Nevertheless, this study was limited by being an observational study. Therefore, some data might have been missing or unavailable, for example, the type of anastomosis, blood flow measurement, and cannulation techniques. In addition, the predictive abilities of NLR and CRP for early AVF failure in combination could not be explored because data on CRP were not available in most patients. Another potential limitation was that comorbidities which may have some degree of inflammation were present in almost all the patients. Nevertheless, these potential confounders were controlled for by multivariate analysis. Finally, the cutoff value for high NLRs used in this study was set for a Thai population cohort. Hence, this value might not be suitable for other populations with a dissimilar distribution of NLRs.
Conclusion
In conclusion, the results of this study demonstrated an association of either preoperatively or postoperatively high NLRs with the risk of early AVF failure. These data may serve as a foundation to develop future research on the role of anti-inflammatory medications in the prevention of AVF failure. Given that this study evaluated only the impact of the change in preoperative/postoperative NLR on AVF outcomes in early period of 3 months, further studies to determine whether preoperative/postoperative NLR values can also be used as prognostic indicators of AVF patency in a long-term period are needed.
Footnotes
Acknowledgements
The author thanks Drs Chadakarn Phaloprakarn and Siriwan Tangjitgamol for their scientific advice and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received research grant from Faculty of Medicine Vajira Hospital, Navamindradhiraj University.