
Abstract
Purpose:
To evaluate the feasibility and accuracy of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients during follow-up period.
Methods:
From March 2015 to October 2015, 126 patients involved in eight hospitals who underwent peripherally inserted central catheter placement received intracavitary electrocardiogram and chest X-ray to verify position of the catheter tip during follow-up period. Their intracavitary electrocardiogram was compared with surface electrocardiogram to judge catheter tip landing zone in one of three different anatomical zones. The amplitude of intracavitary electrocardiogram P wave and the ratio of intracavitary electrocardiogram P wave/surface electrocardiogram P wave were measured and showed correlation with catheter tip position confirmed by chest X-ray. Based on chest X-ray principle, all the cases were assigned into three intracavitary electrocardiogram groups to explore the optimal cut-off values for intracavitary electrocardiogram P wave and intracavitary electrocardiogram P wave/surface electrocardiogram P wave by analyzing the receiver operating characteristic.
Results:
No technique-related complications or adverse events occurred in this study. The matching rate between intracavitary electrocardiogram and chest X-ray method was 93.7%. The optimal cut-off values for intracavitary electrocardiogram P wave were set from 3.15 to 3.75 mV, and intracavitary electrocardiogram P wave/surface electrocardiogram P wave from 1.65 to 3.25.
Conclusions:
It is demonstrated in this retrospective multicenter study that the intracavitary electrocardiogram method for verifying tip position of peripherally inserted central catheter during follow-up period is feasible and accurate in all adult patients with cancer.
Introduction
As a commonly applied infusion device in clinical practice, the peripherally inserted central catheter (PICC) provides an appropriate vascular access for administration of intravenous drugs, parenteral nutrition, chemotherapies, and other treatments in cancer patients.1–4 However, catheter tip location exerts a crucial role in promoting catheter effectiveness, and malposition (e.g. in the upper part of the superior vena cava (SVC) or the lower portion of the right atrium (RA)) may cause catheter malfunction and complications, such as venous thrombosis, central line promulgated bacteremia, arrhythmias, valvular dysfunctions, and heart cavity injuries.4–9 Cadman et al. 10 reported that a 16-time increase for incidence of venous thrombosis at proximal third of the SVC and above compared to the distal third of the SVC and below. Numerous publications and clinical practice guidelines proposed that the lower one-third of the SVC or the cavo-atrial junction (CAJ) region are the optimal position for the tip of PICC.11–14 Verhey et al. 13 reported the basic principles of appropriate catheter placement, including catheter lying parallel to the vessel wall, high-blood flow location, catheter tip motion from cardiac pulsatility, and blood turbulence. The rationale for optimal central venous access device (CVAD) position is to optimize performance of the catheter and minimize risk to the patient with complications and subsequent interventions to restore CVAD function.
There are several methods that could control catheter tip position, including fluoroscopy, chest X-ray (CXR), trans-esophageal echocardiography (TEE), ultrasound, and intracavitary electrocardiogram (IC-ECG).1,15–17 Although the current “gold standard” practice of performing PICC tip confirmation is CXR, a few studies have demonstrated that locating the catheter tip by monitoring the dynamic alterations of the P wave using IC-ECG achieves a similar reliability as CXR.18,19 And the IC-ECG method has the advantages over CXR because of relatively lower financial costs, immediate correction of eventual malposition, reduced post-procedural repositioning requirement, and it is radiation-free.20–22
Besides initial, intraprocedural PICC tip location, catheter tip position should be verified during subsequent clinical infusion or when patient moves from home to a hospital or from one facility to another. For patients with cancer, PICCs are usually applied for weeks or even months during chemotherapy. Hence, it is significant for the catheter tip to remain in the optimal place for a long period.19,23 So, which is the best way to check catheter tip position should be considered. The 2016 Infusion Therapy Standards of Practice recommends that tip position of CVADs should be determined radiographically or by other imaging technologies, such as CXR or ultrasound, prior to initiation of infusion therapy or when clinical signs and symptoms suggest tip malposition. 14 There would appear to be numerous reasons why using a CXR to check CVADs position is not an ideal practice. They can be expensive, inaccurate, dependant on the skill of the interpreter, as well as exposing the patient to potentially unnecessary radiation.1,24 The standard intra-operative technique for catheter tip positioning is the dynamic electrocardiogram (ECG) method, and a number of trials have proven its feasibility, safety, and accuracy.4,15,25–27 However, during follow-up period, the catheter tip cannot be pulled out or pushed back in to check changes in P wave, so we can only get a static ECG. Whether IC-ECG could be used for assessment of PICC tip location during follow-up period remains unknown. In this study, the amplitude of IC-ECG P wave (IP) and the ratio of IC-ECG P wave/surface ECG P wave (IP/SP) were measured at follow-up period and showed correlation with catheter tip position, which was confirmed on CXR.
The aim of this retrospective multicenter study was to further investigate the diagnostic value of IC-ECG for verifying PICC tip position during follow-up period. Moreover, the receiver operating characteristic (ROC) curves and the area under ROC curve (AUC) were also analyzed for IP and IP/SP to find out the optimal cut-off values.
Materials and methods
Experimental design
This was a mixed-method retrospective multicenter study of IC-ECG PICC tip positioning of different cancer patients during follow-up period, from March 2015 to October 2015 (be part of the previous multicenter, open-label and randomized controlled (EGG) study (NCT02409589, https://clinicaltrials.gov/ct2/show/NCT02409589?term=NCT02409589&rank=1); study protocols (SPIRIT), Consolidated Standards of Reporting Trials (CONSORT) checklist, Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement, and Quality Assessment of Diagnostic Accuracy Studies (STARD) are available in Supplementary Materials S1 and S2, and S3 Files).
Operators, cardiologists, and radiologists from eight hospitals in Jiangsu province of China participated in the study: Drum Tower Hospital (Unit A), People’s Hospital Affiliated to Jiangsu University (Unit B), Nanjing Hospital Affiliated to Nanjing Medical University (Unit C), the First Affiliated Hospital of Soochow University (Unit D), the Second Affiliated Hospital of Nanjing Medical University (Unit E), the Second Affiliated Hospital of Soochow University (Unit F), Nanjing Jinling Hospital (Unit G), and Jiangsu Cancer Hospital (Unit H).
Enrolled patients from each unit were given a unique number and received IC-ECG and CXR to check PICC tip position in original positioning hospital at the 1 month follow-up. All ongoing and related experiments with IC-ECG intervention were confirmed to be registered. The experimental protocol was centrally examined. The independent Medical Ethics Committee (IEC) of Drum Tower Hospital (NCT02409589), Medical School of Nanjing University approved this trial on 10 March 2015.
Aims of the study
The study aims to evaluate the practicability of IC-ECG method for location of the tip of PICCs in adult patients with cancer during follow-up period:
A feasibility assessment was performed on the incidence of perfect match between IC-ECG and CXR method.
An accuracy assessment was performed by calculating the optimal cut-off values for IP and IP/SP.
Patients
Based on the previous multicenter, open-label, randomized controlled (EGG) study (NCT02409589), a total number of 1003 adult patients underwent PICC placement and received chemotherapy 1 month later. Among these, 872 patients were treated in general hospitals surrounding their home while 131 patients remained in the hospital where their PICC was inserted; among these, 5 patients showed unsuitable external baseline ECG: their intravascular P-wave could not be measured. Finally, 126 adult patients were included in the study, aged 18–80 years, and received ECG control, CXR, and chemotherapy in the initial hospital where the PICC was inserted. Signed informed consent of each enrolled patient was obtained before the trial. Exclusion criteria were as follows: loss to follow-up (Jiangsu Cancer Hospital); death; without visible P wave on the standard baseline ECG; cardiovascular diseases such as valvular heart disease, atrial fibrillation, supraventricular tachycardia, pulmonary heart disease, or history of pacemaker installation; and cardiac surgery that may affect P waves.
PICC and monitor characteristics
A single-lumen PICC kit (Groshong NXT Clear Vue, 4 F) produced by Bard Access Systems, Inc. (Utah, USA) was used during previous multicenter, open-label, randomized controlled study catheterization. A C100 specialized cardiovascular monitor provided by Shenzhen Comen Medical Instruments Co., Ltd was applied for positioning and recording the tip of PICCs in this study, in accordance with each center’s protocol and our pilot study.
Checking catheter tip position by IC-ECG method
Patient with catheterization was lying in a supine position, the upper arm and torso was maintained at a 45°~90° angle, that is, the natural flexed position. The connector cable with crocodile clamp was clipped on a needle inserted through a perforable heparin cap and connected directly to the “red” electrode of the ECG monitor, usually placed on the right shoulder of the patient. We used a gravity drip method to continuously infuse normal saline solution through the catheter, so as to open the Groshong valve and find a stable intracavitary-type of IC-ECG curve. The IC-ECG and surface ECG records were printed out. The IP and the IP/SP were measured (Figure 1).
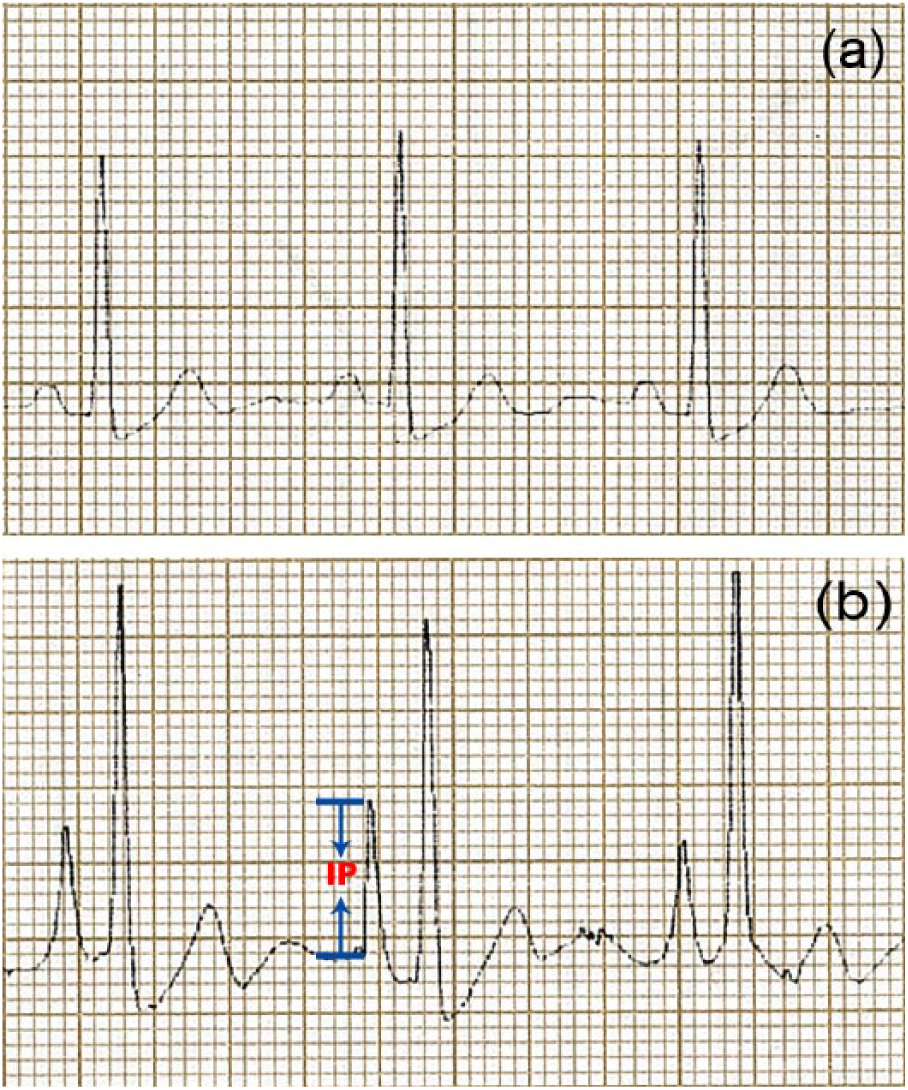
Images of the voltage change for IP wave and the ratio of IP/SP: (a) the surface ECG P wave and (b) the IC-ECG P wave.
Evaluating catheter tip landing zone by comparing P wave of IC-ECG with surface ECG
The principles of IC-ECG method at the initial catheterization tip position are as follows:4,15,24,28,29
Record the maximum P-wave height: the PICC tip is located at the entrance to the atrium (close to the crista terminalis, at the CAJ);
Obtain a gradual reduction of the P-wave height, about 50% of the maximum P-wave height (the tip is located in the lower one-third of the SVC, just above the CAJ);
The “normal” dimensions of P-wave, that are similar to those on the “surface” or trans-parietal ECG (the tip is back again in the upper part of the SVC);
The P-wave gradually decreases and/or develops into biphasic (negative/positive), followed by overtly negative; typically, a small negative incision appears prior to the standard positive wave (the catheter/guidewire has entered the RA).
The IC-ECG method for initial catheter positioning is a dynamic process; however, during follow-up period, we cannot pull the catheter out or push back in to check changes in P-wave, and we could only get a static IC-ECG to assess the catheter tip position. So in this study, we allocated the catheter tip position to three different anatomical zones based on the IC-ECG principle as follows:
Zone 1—outside SVC (no significant alterations in IC-ECG P-wave relative to surface ECG);
Zone 2—in the region of the SVC (enlargement of IC-ECG P-wave relative to surface ECG and no inversion or negative deflections were seen);
Zone 3—within the scope of the RA (seen some inversion or negative deflections, biphasic, and negative at IC-ECG P-wave relative to surface ECG).
Checking catheter tip position by CXR
Although full evaluation of the CXR based on the radiologist’s report was essential, the specific assessment on the tip localization using the radiograph should be performed by the physician who tested the catheter with IC-ECG.
In this study, we adopted the following radiologic criteria that could accurately locate the tip position as described in the updated literature:4,15
Radiologic landmark of the CAJ: 3 cm below the tracheal carina or just under the inferior border of the right bronchia;
Radiologic landmark of the lower third of the SVC: below the carina but within a distance of 3 cm. The SVC was further divided into upper third and middle third part;
Radiologic landmark of the upper third of the RA: 3–5 cm below the carina.
Based upon the above criteria, all the cases were assigned into three IC-ECG groups: Group 1—outside SVC, the upper third and the middle third part of SVC; Group 2—the lower third part of SVC and CAJ; Group 3—the RA.
Results of the two techniques (IC-ECG and CXR) evaluating catheter tip landing zone
The results of the two techniques evaluating catheter tip landing zone were described as a “perfect match” (both techniques agree on the fact that a catheter tip is located in the same zone) and “mismatch” (a catheter tip is located in different zones by the two techniques, respectively).
Data collection and statistical analysis
In this study, two radiologists and IC-ECG experts independently analyzed the IC-ECG and CXR data. A third radiologist discussed disagreements of CXR recordings, and finally solved by consensus. IC-ECG allocated groups were blinded to radiologists. Physical and laboratory examinations were assessed before verifying PICC tip position.
General information: age, gender, body mass index (BMI), weight, side of insertion, and patients’ position during CXR;
Tip position landing zone according to physician’s evaluation by IC-ECG (Zone 1, 2, or 3);
Position of the tip according to CXR (Group 1, 2, or 3);
Position of the tip as verified by CXR and IC-ECG classified according the following scheme: perfect match, both techniques agree on the fact that a catheter tip is located in the same zone; mismatch, a catheter tip is located in different zones by the two techniques, respectively;
The IP and the IP/SP.
According to collected data, the feasibility was represented by the percentage of perfect match between IC-ECG and CXR. The accuracy was expressed as the optimal cut-off values for the IP and the IP/SP.
Based on different classification of variables, we utilized the most appropriate tests for analyzing data in computer-based archive. The categorical data (age, weight, height, etc.) were expressed as mean ± standard deviations, and measured data were expressed as percentages (perfect match, mismatch between the evaluation results of IC-ECG and CXR).
IBM SPSS Statistics version 22.0 for Windows 10 (International Business Machines Corp., New York, USA) and the Microsoft Excel 2016 for Windows 10 (Microsoft Corp., Washington, USA) were utilized for statistical processing. Continuous data were expressed as median with interquartile range (IQR) and analyzed by the Mann–Whitney U test. Two-sided p values <0.05 indicated statistical significance. The optimal cut-off values for IP and IP/SP were calculated according to ROC curves. The “Youden index” described the maximum vertical distance between the ROC curve and the diagonal or chance line. The optimal cut-off values for the IP and IP/SP, Youden index, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated in the study.
Results
Patient characteristics
In total, 126 intention-to-treat (ITT) patients were enrolled in this study (Figure 2). There were 54 men (42.9%) and 72 women (57.1%). Mean age was 55.5 ± 12.2 years (range = 18–80) and BMI (kg/m2) was 22.9 ± 3.0. Most PICCs were inserted on the right side (76.2%) and 23.8% on the left side; 100% were on standing position during CXR (Table 1).
Demographic details of the study participants (ITT, N = 126).
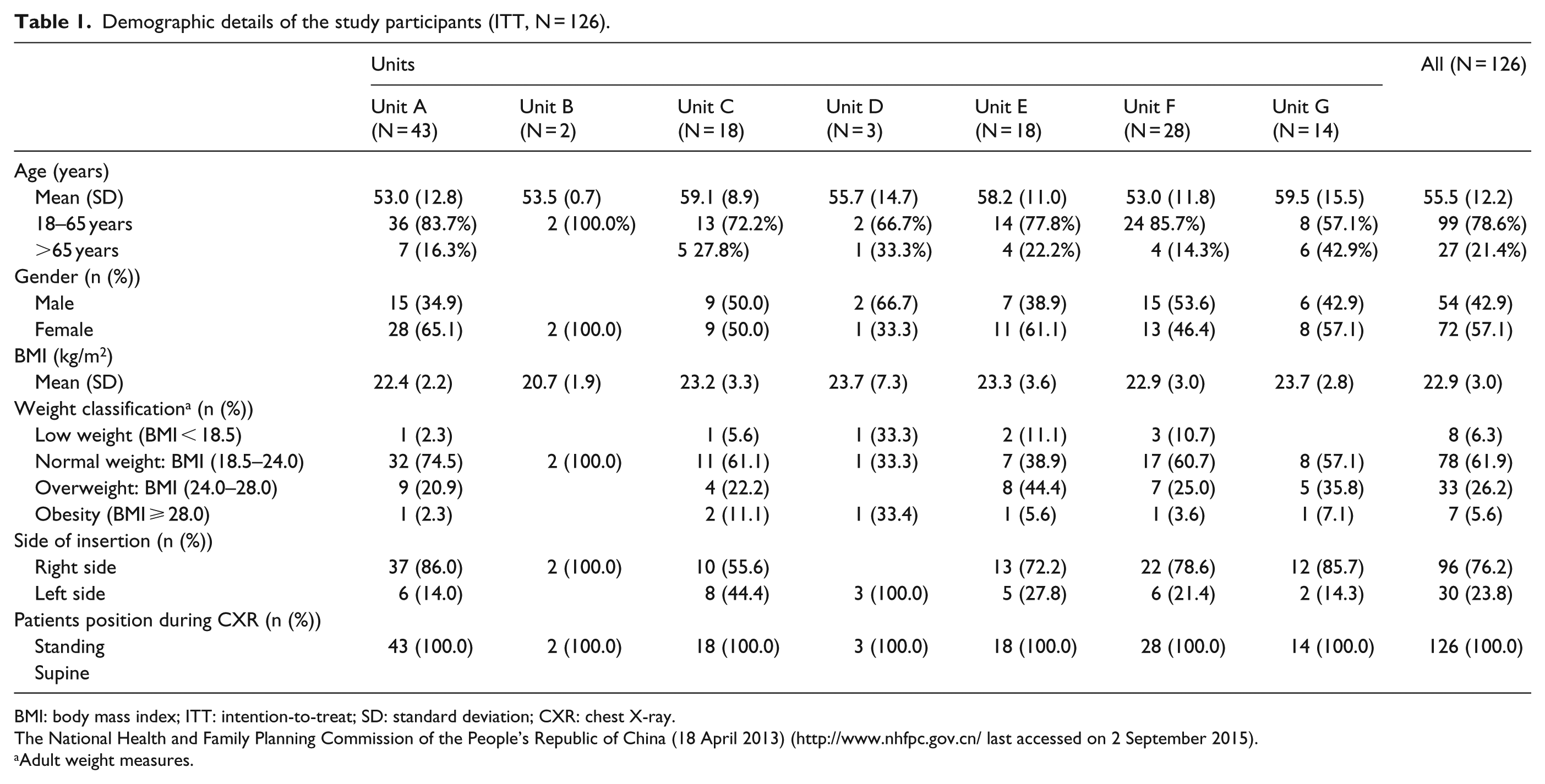
BMI: body mass index; ITT: intention-to-treat; SD: standard deviation; CXR: chest X-ray.
The National Health and Family Planning Commission of the People’s Republic of China (18 April 2013) (http://www.nhfpc.gov.cn/ last accessed on 2 September 2015).
Adult weight measures.
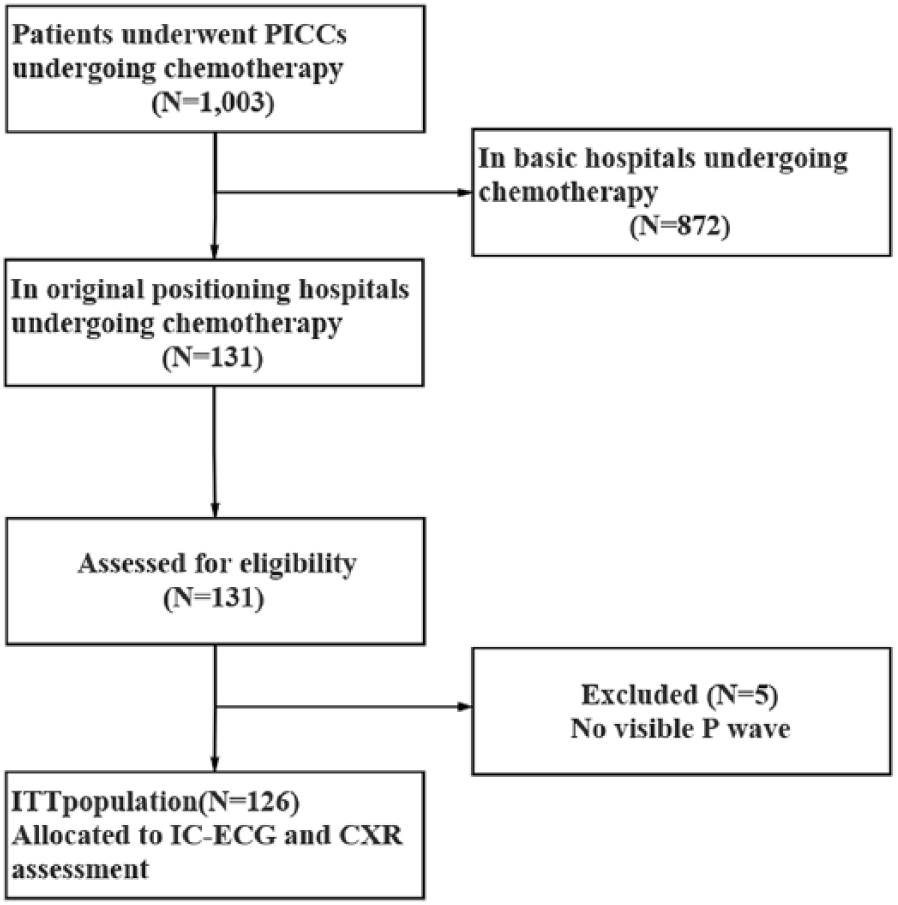
Flow chart of the intention-to-treat (ITT) population (N = 126).
Feasibility of PICC tip positioning
No technique-related complications or adverse events occurred in this study. Table 2 shows in 126 cases, using ECG guidance, by physician evaluation of IC-ECG method, 1.6% outside SVC (Zone 1), 93.7% in the region of the SVC (Zone 2), and 4.7% within the scope of the RA (Zone 3). The incidence rate of perfect match and mismatch between the physician evaluation of IC-ECG method and CXR were 93.7% and 6.3%, respectively (Table 3).
Catheter tip position of the centers (ITT, N = 126).
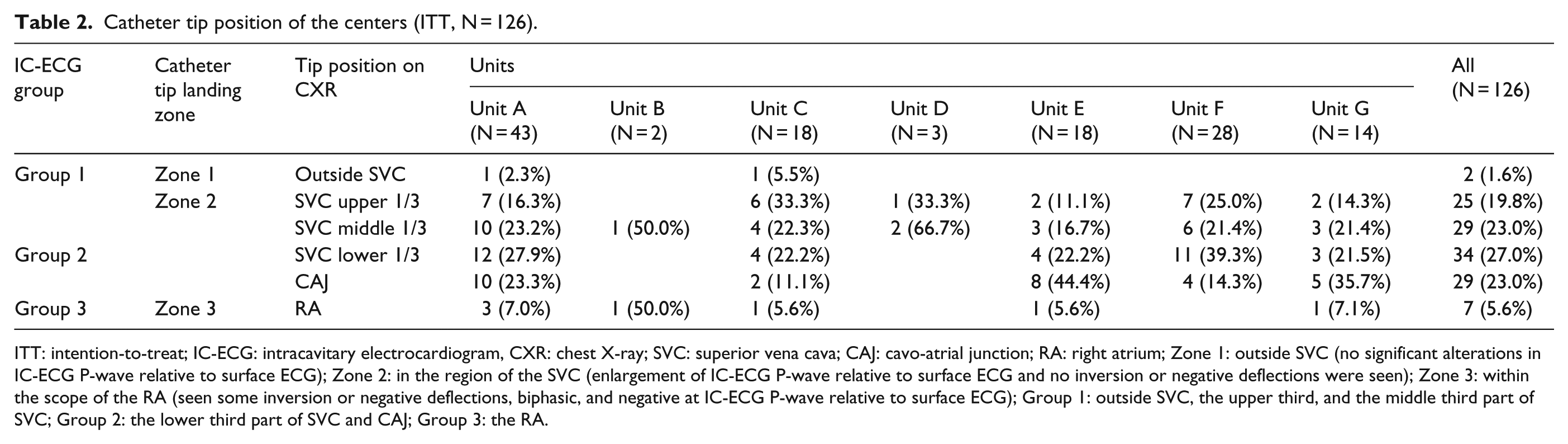
ITT: intention-to-treat; IC-ECG: intracavitary electrocardiogram, CXR: chest X-ray; SVC: superior vena cava; CAJ: cavo-atrial junction; RA: right atrium; Zone 1: outside SVC (no significant alterations in IC-ECG P-wave relative to surface ECG); Zone 2: in the region of the SVC (enlargement of IC-ECG P-wave relative to surface ECG and no inversion or negative deflections were seen); Zone 3: within the scope of the RA (seen some inversion or negative deflections, biphasic, and negative at IC-ECG P-wave relative to surface ECG); Group 1: outside SVC, the upper third, and the middle third part of SVC; Group 2: the lower third part of SVC and CAJ; Group 3: the RA.
Overall accuracy (ITT, N = 126).

IC-ECG: intracavitary electrocardiogram; CXR: chest X-ray. P—perfect match: both techniques (IC-ECG and CXR) agree on the fact that a catheter tip is located in the same zone; M—mismatch: a catheter tip is located in different zones by the two techniques (IC-ECG and CXR), respectively.
Accuracy of PICC tip positioning
Group 2 had higher IP than Group 1 (4.71 vs 3.17; p < 0.05), while lower than Group 3 (4.71 vs 6.25; p < 0.01). In addition, Group 2 had higher IP/SP than Group 1 (3.81 vs 2.73; p < 0.05), while lower than Group 3 (3.81 vs 5.03; p < 0.01) (Table 4). ROC curve analysis indicated the optimal cut-off values for IP were set from 3.15 to 3.75 mV, while IP/SP from 1.65 to 3.25. Based on these values, IP1 ⩾ 3.15 mV had a sensitivity of 70%, a specificity of 59%, a PPV of 80.0%, and a NPV of 45.7%, and for the combination of IP2 ⩽ 3.75 mV were 83%, 48%, 83.3%, and 47.6%, respectively. The corresponding values for IP/SP1 ⩾ 1.65 were 97%, 30%, 80.0%, and 76.2%, and for the combination of IP/SP2 were 75%, 57%, 80.0%, and 50.0% (Table 5). ROC curve analyses for IP and IP/SP were calculated where the AUC of IP1 was 0.67 (95% confidence interval (CI) = 0.54~0.80) and of IP2 was 0.67 (95% CI = 0.56~0.78). Meanwhile, the AUC of IP/SP1 was 0.66 (95% CI = 0.53~0.79) and of IP/SP2 was 0.67 (95% CI = 0.56~0.78) (Table 5 and Figure 3).
Characteristics of the study population (ITT, N = 126).
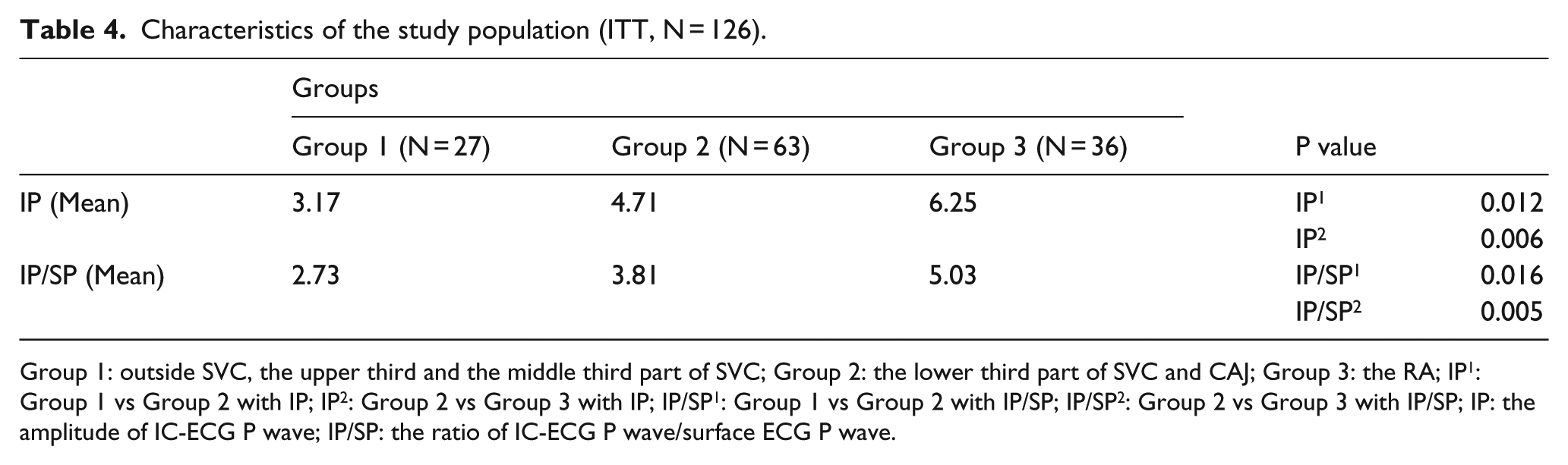
Group 1: outside SVC, the upper third and the middle third part of SVC; Group 2: the lower third part of SVC and CAJ; Group 3: the RA; IP1: Group 1 vs Group 2 with IP; IP2: Group 2 vs Group 3 with IP; IP/SP1: Group 1 vs Group 2 with IP/SP; IP/SP2: Group 2 vs Group 3 with IP/SP; IP: the amplitude of IC-ECG P wave; IP/SP: the ratio of IC-ECG P wave/surface ECG P wave.
Results of ROC curve analyses for IP and IP/SP.
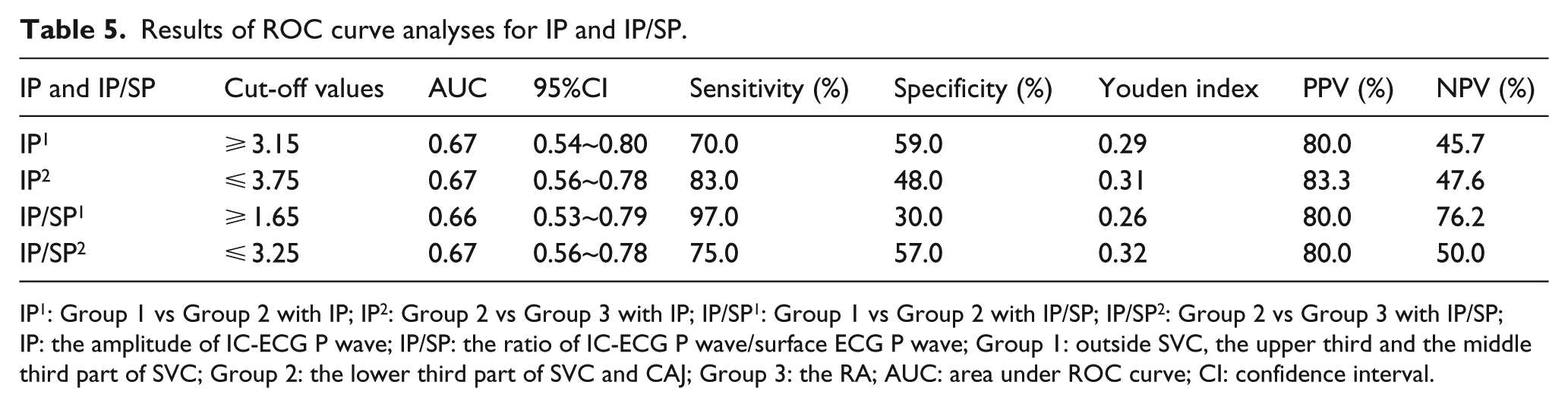
IP1: Group 1 vs Group 2 with IP; IP2: Group 2 vs Group 3 with IP; IP/SP1: Group 1 vs Group 2 with IP/SP; IP/SP2: Group 2 vs Group 3 with IP/SP; IP: the amplitude of IC-ECG P wave; IP/SP: the ratio of IC-ECG P wave/surface ECG P wave; Group 1: outside SVC, the upper third and the middle third part of SVC; Group 2: the lower third part of SVC and CAJ; Group 3: the RA; AUC: area under ROC curve; CI: confidence interval.

Area under ROC curve: (a) Group 1 vs Group 2 with IP; (b) Group 2 vs Group 3 with IP; (c) Group 1 vs Group 2 with IP/SP; and (d) Group 2 vs Group 3 with IP/SP.
Discussion
This retrospective study is part of our previous multicenter study that aims to elucidate the clinical diagnostic value of IC-ECG method for control of the PICC tip position during follow-up period in cancer patients. From the perspective of general clinical practice, our study pointed out several suggestions:
During follow-up period before surveillance catheter tip position, physicians can analyze whether the catheter tip is within part of the SVC by comparing P wave morphology of IC-ECG with that of surface ECG.
According to the calculation of IP and IP/SP cut-off values, we can evaluate whether catheter tip position is in or out of the lower one-third of SVC and CAJ, so that we can further determine whether or not CXR for the tip position is required.
CXR serves as the global standard for the accurate confirmation of the CVAD. 21 However, in many countries, including Canada, the United States, Germany, and Italy, ECG-guided CVAD placement is considered to be as effective as a CXR. 27 Our previous multicenter, open-label, randomized controlled (EGG) study (NCT02409589) indicated that in 1007 cases, the IC-ECG-guided method showed a higher positioning accuracy (89.2%) compared with traditional anatomical landmarks for PICC placement in adult cancer patients suffering from chemotherapy. 28
IC-ECG-guided catheter placement shows advantages of real-time procedure and accurate tip confirmation. By using this method, the operator could monitor the tip position in the catheter without the danger of inserting too deep. However, during follow-up period, the catheter tip cannot be pulled out or pushed back in to check changes in P wave, so we can only get a static ECG compared to intra-operative dynamic ECG.
In this study, it is feasible to check catheter tip position by analyzing P wave of IC-ECG and surface ECG. A perfect match between the IC-ECG and CXR was 93.7%; mismatch was only observed in 6.3% of cases. There is significant correlation between the method of IC-ECG and CXR. We have identified the amplitude of IP 3.15~3.75 mV and the ratio of IP/SP 1.65~3.25 as optimal cut-off values for confirming position of the tip of PICCs. When IP and IP/SP is within this cut-off range, the catheter tip is surely within the lower one-third of the SVC or CAJ and the corresponding patients could be free from CXR for tip position confirmation. On the contrary, the patients whose IP and IP/SP is out of this cut-off values still need further CXR to confirm the exact position of catheter tip, which means just a part of the patients could be free of unnecessary CXR tip position confirmation.
As we know, standing position may “elevate” the position compared to supine position, with a difference of 2–3 cm. 15 Patients with catheterization received IC-ECG assessment in supine position; when receiving CXR assessment in standing position, the tip of PICC is approximately in a 2 cm “higher” location, which is still in the area of lower third part of SVC. So the tip position of PICC is still near the CAJ at lower part of the SVC no matter in standing or supine position.
Some limitations existed in this study. The sample size was relatively small. Several factors could affect the accurate reading of the P wave shape and amplitude variations, such as a single type of disease, PICC kit, guidance method, and ECG monitor device. It is difficult to identify the standard P wave on the surface ECG due to severe arrhythmias. In addition, the specificity of IC-ECG technology will be affected because of the accuracy of this study is based on the CXR confirmed, and more accurate judgment technology can be used to evaluate the specificity of IC-ECG method in terms of catheter position. In-depth studies are needed to elucidate whether the optimal cut-off values defined in this study are widely used. And in the future, we will make further study in this field. What’s more, sufficient number of patients would be recruited in future researches.
Conclusion
In summary, in this analytical, observational, diagnostic, and retrospective multicenter study, the IC-ECG method is feasible and accurate for locating the tip of PICCs during follow-up period in patients with cancer. Analyzing P wave of IC-ECG and surface ECG may help to check catheter tip malposition. Meanwhile, according to the optimal cut-off values of the IP and the IP/SP, a number of patients can be free from unnecessary CXR for finding tip position. By these means of checking PICC’s tip position before starting intravenous treatment, medical safety can be significantly improved.
Supplemental Material
S1_File._CONSORT-2010-Checklist – Supplemental material for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study
Supplemental material, S1_File._CONSORT-2010-Checklist for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study by Ting Yu, Ligui Wu, Ling Yuan, Robert Dawson, Rongmei Li, Zhenzhu Qiu, Xiancui Wu, Ping Chen, Jing Qi, Yiqun Yang, Yuling Feng, Wei Xu, Weiwei Kong, Yang Chen, Shanping Li, Xiang Wu and Tingting Yan in The Journal of Vascular Access
Supplemental Material
S2_File._STROBE-statement – Supplemental material for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study
Supplemental material, S2_File._STROBE-statement for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study by Ting Yu, Ligui Wu, Ling Yuan, Robert Dawson, Rongmei Li, Zhenzhu Qiu, Xiancui Wu, Ping Chen, Jing Qi, Yiqun Yang, Yuling Feng, Wei Xu, Weiwei Kong, Yang Chen, Shanping Li, Xiang Wu and Tingting Yan in The Journal of Vascular Access
Supplemental Material
S3_File._STARD-2015-checklist – Supplemental material for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study
Supplemental material, S3_File._STARD-2015-checklist for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study by Ting Yu, Ligui Wu, Ling Yuan, Robert Dawson, Rongmei Li, Zhenzhu Qiu, Xiancui Wu, Ping Chen, Jing Qi, Yiqun Yang, Yuling Feng, Wei Xu, Weiwei Kong, Yang Chen, Shanping Li, Xiang Wu and Tingting Yan in The Journal of Vascular Access
Supplemental Material
S4_File._Numbers_of_initially_PICC_insertion_patients – Supplemental material for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study
Supplemental material, S4_File._Numbers_of_initially_PICC_insertion_patients for The diagnostic value of intracavitary electrocardiogram for verifying tip position of peripherally inserted central catheters in cancer patients: A retrospective multicenter study by Ting Yu, Ligui Wu, Ling Yuan, Robert Dawson, Rongmei Li, Zhenzhu Qiu, Xiancui Wu, Ping Chen, Jing Qi, Yiqun Yang, Yuling Feng, Wei Xu, Weiwei Kong, Yang Chen, Shanping Li, Xiang Wu and Tingting Yan in The Journal of Vascular Access
Footnotes
Author Contributions
T.Y., L.Y., and L.G.W. contributed to the conceptualization. T.Y., L.Y., L.G.W., Rob, R.M.L., Z.Z.Q., X.C.W., P.C., J.Q., Y.Q.Y., Y.L.F., W.X., W.W.K., Y.C., S.P.L., X.W., and T.T.Y. contributed to data curation. T.Y. did the formal analysis. L.Y. provided the funding acquisition. T.Y., L.Y., L.G.W., Rob, R.M.L., Z.Z.Q., X.C.W., P.C., J.Q., Y.Q.Y., Y.L.F., W.X., W.W.K., Y.C., S.P.L., X.W., and T.T.Y. did the investigation. T.Y., L.Y., L.G.W., and Rob provided the methodology. L.Y. contributed to project administration. T.Y., L.Y., and L.G.W. contributed to the resources. T.Y. contributed to the software. T.Y. contributed to the supervision. T.Y., L.Y., L.G.W., and Rob did the validation. T.Y., L.Y., L.G.W., and Rob contributed to visualization. T.Y., L.Y., and L.G.W. contributed to the writing of the original draft. T.Y., L.Y., L.G.W., and Rob contributed to writing—review and editing. T.Y. and L.G.W. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We declare that the new IC-ECG guidance system used in the study had been offered a National Utility Model Patent (No.: ZL-2014-2-0436176.7, authors: Ling Yuan, et al.) previously. But we still adhere to JVA policies on sharing data and materials. What’s more, we declare that no part of this paper has been published or submitted elsewhere.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Drum Tower Hospital–based Science and Research Fund (No: 2015-001) and the Key Project of Medical Science and Technology Development, Nanjing Health Bureau (No: ZKX15017).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.