
Abstract
Purpose:
To evaluate the technical and clinical results of endovascular recanalization of thrombosed native hemodialysis fistula and the factors influencing patency.
Methods:
A retrospective study was conducted with 73 patients who had thrombosed arteriovenous fistulas and were treated with endovascular methods. Patient characteristics, arteriovenous fistula-related characteristics, and endovascular procedures were analyzed. Technical and clinical results and patency rates were evaluated. The factors influencing patency were analyzed using a univariate and multivariate Cox proportional hazards model.
Results:
Technical and clinical success rates were 93% (68/73) and 85% (62/73), respectively. At 3, 6, and 12 months, the primary patency rates were 87.9%, 73.3%, and 64.8%; assisted primary patency rates were 89.2%, 78.6%, and 70.7%; and secondary patency rates were 90.8%, 87.2%, and 83.1%, respectively. Previous intervention and cephalic arch stenosis were risk factors for lower primary and assisted primary patency (p < 0.05 for all). Cephalic arch stenosis was the only risk factor for lower secondary patency (p < 0.05). No major complications associated with the procedures were noticed.
Conclusion:
Endovascular treatment was effective for the immediate recanalization of thrombosed arteriovenous fistula. In addition, previous intervention and cephalic arch stenosis were significantly related to lower arteriovenous fistula patency.
Introduction
Properly functioning vascular access is fundamental to the survival and quality of life of hemodialysis patients. 1 The Kidney Disease Outcomes Quality Initiative (K/DOQI) recommends placement of native arteriovenous fistulas (AVFs) in preference to arteriovenous (AV) synthetic grafts (AVGs) or central venous catheters due to superior patency and lower infection rates.2,3 Despite these advantages of AVF, thrombosis of the draining vein results in eventual AVF failure. 4
The incidence of thrombosis is lower in AVFs than in AVGs.5,6 However, AVFs usually carry a heavier thrombotic burden than AVGs and usually accompany large aneurysms or diffuse aneurysmal changes.7–9 For the management of thrombosed AVFs, various percutaneous methods (i.e., mechanical thrombectomy, pharmacologic thrombolysis that is either systemic or locoregional, and pharmacomechanical thrombolysis) have been utilized in addition to surgical thrombectomy.10–15 Recently, newly designed devices have been developed with the application of hydromechanics.14,16,17 For example, the AngioJet rheolytic thrombectomy device uses high-pressure saline jets that induce the Venturi-Bernoulli effect and remove thrombi through the catheter without the risk of significant pulmonary embolism. However, aneurysmal segments usually contain a mass of chronic organizing thrombi, which makes removing the thrombi through the catheter with a small caliber difficult.
The success rates of endovascular declotting of AVF or AVG vary from 76% to 100%.16,18,19 However, only a few studies have reported the treatment of thrombosed AVF alone. Therefore, the purpose of this study was to evaluate the technical and clinical outcomes of endovascular recanalization of thrombosed AVF and the factors influencing patency.
Methods
Study population
Our institutional review board and ethical committee approved this retrospective study.
Between January 2009 and December 2016, 79 patients with thrombosed AVF were treated with endovascular methods among 213 patients with dysfunctional AVF. Of these patients, six were excluded because they were not followed up in our hospital (n = 3) or AVF creation dates were not identified (n = 3). Therefore, 73 patients were included in this study and were treated with endovascular methods. The electronic medical records of these patients were reviewed retrospectively, including patient characteristics, AVF-related characteristics, and endovascular procedures. The characteristics of the patients and the AVFs are listed in Table 1.
The basic characteristics of the patients and AVFs.
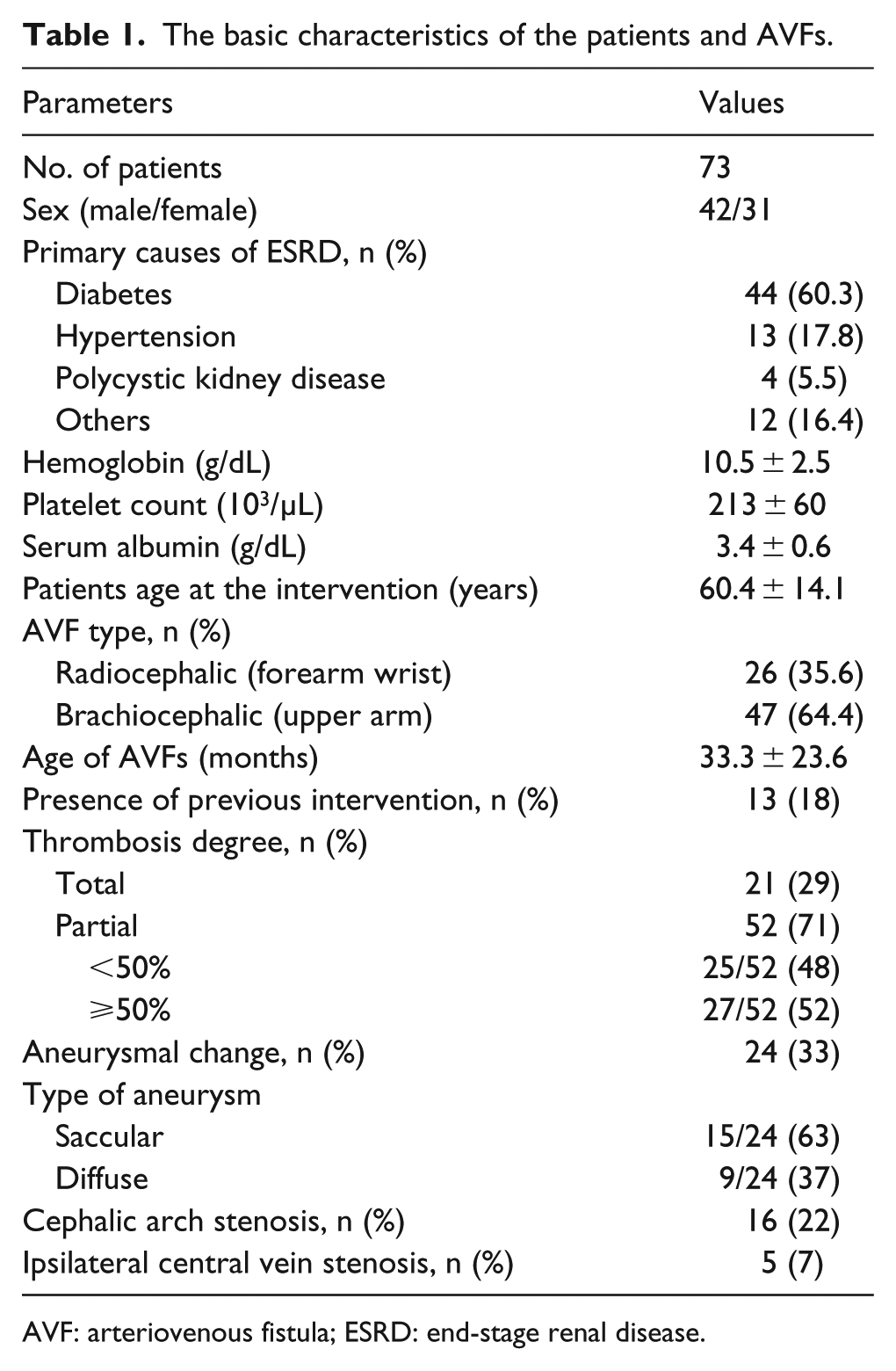
AVF: arteriovenous fistula; ESRD: end-stage renal disease.
Endovascular procedure
Written informed consent was obtained before initiation of treatment. Intravenous access was established with an 18-gauge intravenous catheter before the procedure. Prophylactic antibiotics were not administered. Recanalization was performed either with single or two bidirectional punctures according to the physical and ultrasound (US) examination. Puncture sites were anesthetized with 1% lidocaine hydrochloride. All punctures were performed with the use of a micropuncture set (Cook Medical Inc, Bloomington, IL, USA) under US guidance. In the case of bidirectional puncture, the initial puncture was made distal to the AV anastomosis site to establish venous outflow. In the presence of an aneurysmal change, this segment was avoided as a puncture site.
After inserting a 6- or 7-Fr vascular sheath, patients received 3000 IU of heparin intravenously. A 5-Fr angiographic catheter (Cook) was passed through the thrombosed segment using 0.035-inch angled guide wire (Terumo, Tokyo, Japan). According to the thrombotic burden, a mixture of 100,000 U of urokinase with 500 IU of heparin or 200,000 U of urokinase with 1000 IU of heparin was administered through the thrombotic segment. Subsequently, thrombectomy, thrombolysis or a combination of both was performed to remove thrombi. Thrombectomy was performed with either mechanical thrombectomy using a rotational percutaneous mechanical thrombectomy device (PTD) (Arrow-Trerotola percutaneous thrombectomy device, Arrow, Reading, Pennsylvania) or aspiration thrombectomy using a soft-tip guiding catheter (Envoy, Codman Neurovascular, Raynham, MA, USA). Thrombolysis was performed using multi-side hole infusion catheters (Cragg-McNamara valved infusion catheter, Covidien; Multi-sideport catheter infusion set, Cook).
Adjunctive percutaneous transluminal angioplasty (PTA) with a 4–7 mm balloon catheter was performed to treat stenosis at the AV anastomosis site and/or outflow draining vein. In cases of focal thrombosis, primary PTA was performed without thrombectomy or thrombolysis. PTA was performed until stenotic segments were sufficiently dilated (less than 30% residual stenosis). The size of the balloon used was determined by the size of the adjacent non-aneurysmal draining vein. As needed, high-pressure noncompliant balloons were used for PTA.
After the recanalization procedure, completion angiography was performed from the AV anastomotic site to the superior vena cava. For central vein stenosis with arm edema or high venous pressure disturbing hemodialysis, PTA or stent insertion was performed during the follow-up period. Hemostasis of the puncture site was performed with manual compression in all patients.
Definitions and statistical analysis
Total thrombosis was defined as the presence of thrombosis from the AV anastomotic site to the cephalic arch in the case of a brachiocephalic fistula or thrombosis from the AV anastomotic site to the antecubital fossa level in the case of a radiocephalic fistula. Technical success was defined as the absence of a residual flow-limiting thrombus and a residual diameter stenosis of less than 30% after treatment. Clinical success was defined as the successful use of the fistula within a 4-week period after intervention.16,20 An aneurysm was defined as a dilation that was more than twice the normal segment of the outflow vein and a dilation that was more than 2 cm in diameter.21,22 Thrombolysis was defined as requiring more than 1 h of continuous infusion of a thrombolytic agent through a multi-side hole catheter. Primary patency was defined as the interval following intervention until the next access thrombosis or repeated intervention. Assisted primary patency was defined as the interval after intervention until access thrombosis or a surgical intervention that excludes the treated lesion from the access circuit. Secondary patency was defined as the interval after intervention until the access was surgically declotted, revised, or abandoned. Complications were categorized into major or minor types. Major complications included those requiring prolonged hospitalization, causing permanent adverse sequelae, or death. Minor complications were those requiring no treatment or treatment by an interventionist in an angioroom without prolonged hospitalization or consequences. 23
A Kaplan–Meier analysis was performed to calculate the primary, assisted primary, and secondary patency rates. The factors that were regarded to independently influence the patency rates were analyzed with a univariate Cox proportional hazards model. Significant variables (p < 0.2) in the univariate analysis were evaluated with a multivariate Cox proportional hazards model using the backward stepwise elimination method. A two-sided p-value <0.05 was considered statistically significant. All analyses were performed with IBM SPSS Statistics software (version 20; IBM Corp, USA).
Results
A total of 73 patients were treated with endovascular methods for thrombosed AVFs (26 radiocephalic—forearm wrist; 47 brachiocephalic—upper arm). Draining vein obstruction was observed in forearm cephalic vein (n = 25), upper-arm cephalic vein (n = 32), and cephalic arch (n = 16). The basic characteristics of the patients and AVFs are listed in Table 1.
An adjuvant thrombolytic agent was used in 60 patients. Recanalization was performed with thrombectomy, thrombolysis, PTA, or a combination of these methods (Figure 1). In eight (11.0%) patients with partial thrombosis, the flow was restored by PTA alone without any additional thrombectomy procedures. In 22 (30.1%) patients without chronic wall adherent thrombi, aspiration thrombectomy with additional PTA was performed. In 40 (54.8%) patients with heavy thrombosis, mechanical thrombectomy was performed as an initial procedure for thrombectomy with or without additional aspiration thrombectomy. Thrombolysis was adopted as the first treatment of choice in three (4.1%) patients. The mean procedure time from initial puncture to completion fistulography was 76.1 (±51.7) min. The catheter indwelling time for thrombolysis was not included in the procedure time (Table 2).
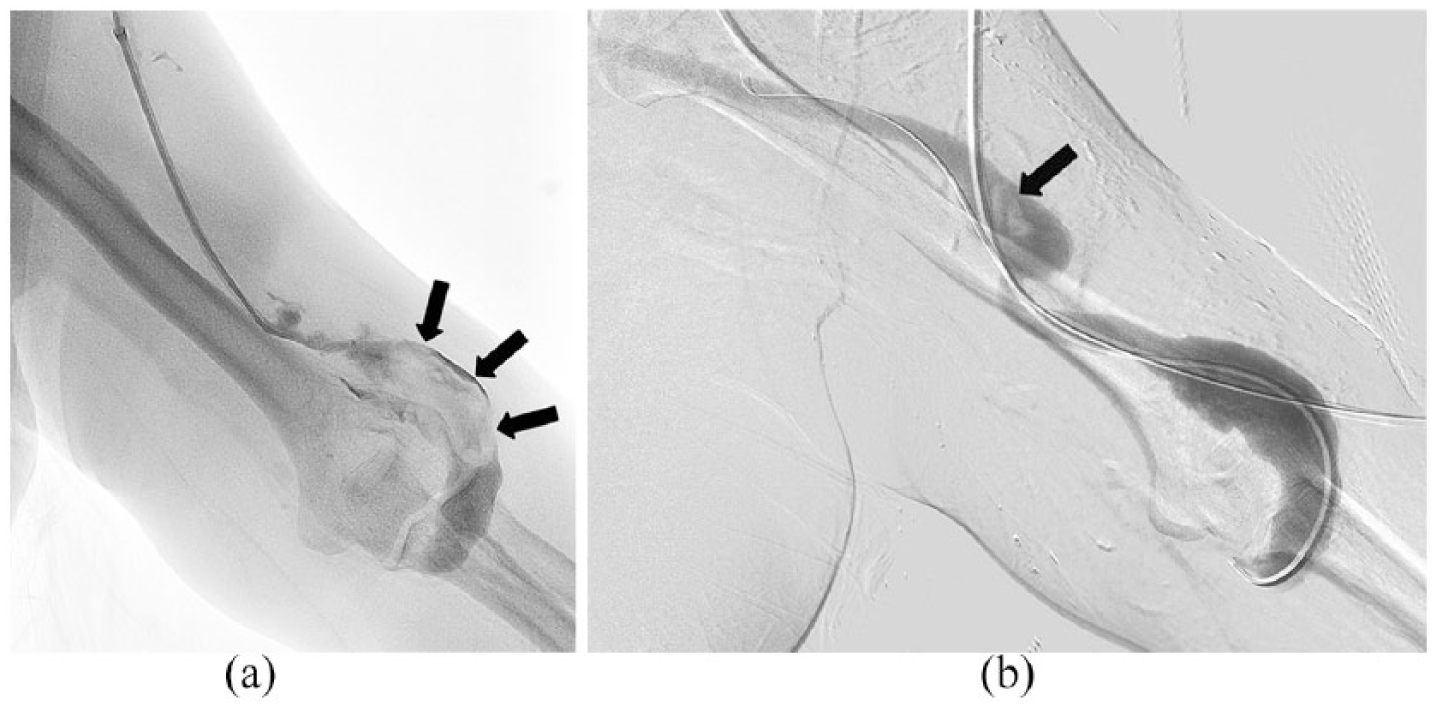
A 60-year-old woman presented with left upper-arm brachiocephalic AVF malfunction: (a) fistulogram showing filling defects suggesting total thrombosis of the AVF. The proximal portion of the AVF shows thrombosis in a diffuse aneurysmal change (arrows) and (b) after repeated mechanical and aspiration thrombectomy, thrombi were nearly removed and the flow was restored despite the presence of small amounts of minimal residual thrombi (arrow).
Endovascular treatment and the results.
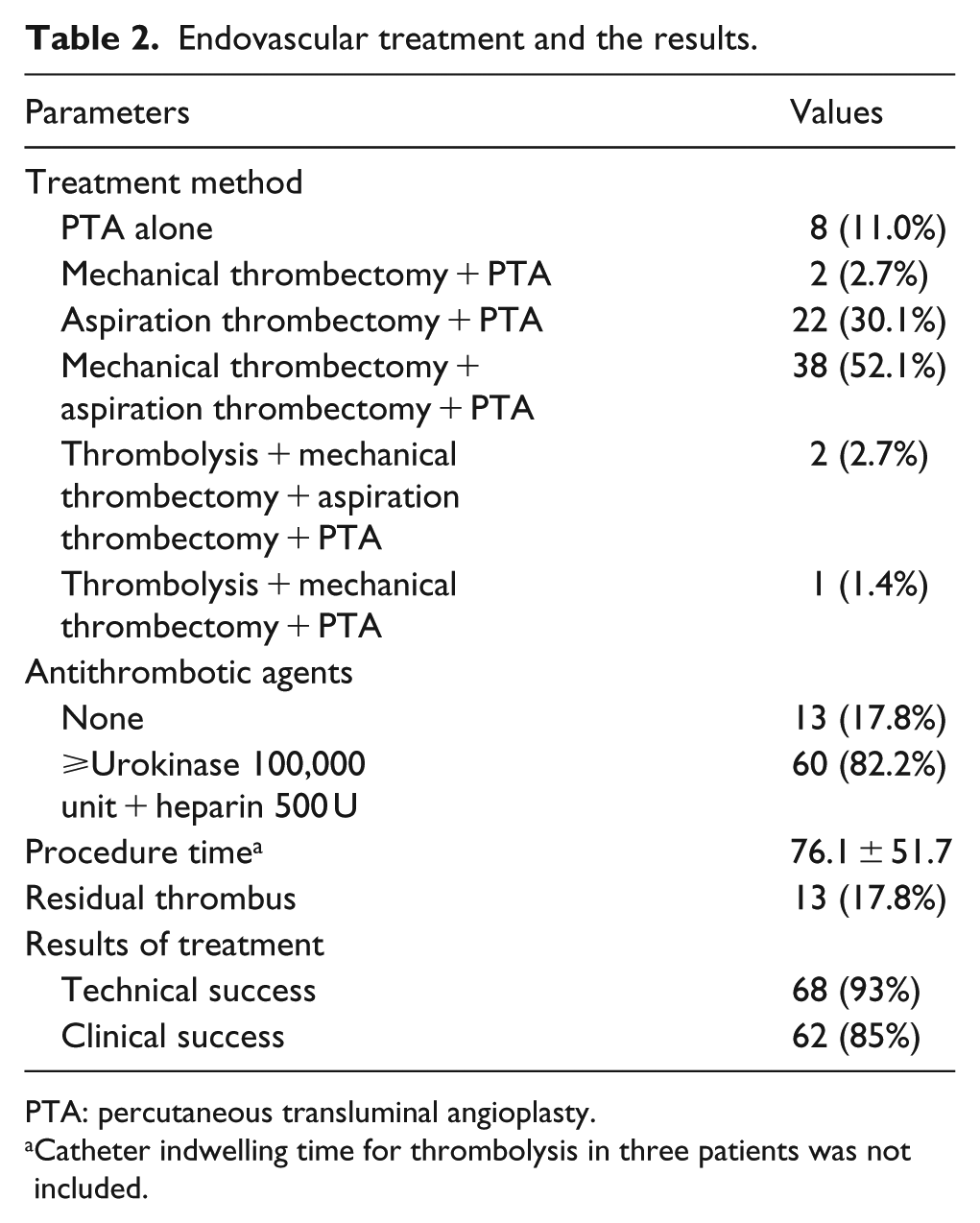
PTA: percutaneous transluminal angioplasty.
Catheter indwelling time for thrombolysis in three patients was not included.
Ipsilateral central vein stenosis was observed in five patients. In one patient with a previous left innominate vein stent insertion, mild in-stent stenosis was observed without symptoms. Four patients with arm edema or high venous pressure disturbing hemodialysis underwent PTA (n = 1) or stent insertion (n = 3) during the follow-up period.
During the thrombectomy of the aneurysmal segment, rotational PTD failure occurred in two patients. In one patient, the device was twisted and removed using a wire cutter. In this patient, the procedure was completed with a new device. In another patient, device fracture occurred, and the device was removed using a snare catheter. However, this patient refused continuation of the procedure.
Cephalic arch rupture after PTA occurred in four patients. In these cases, extravasation stopped with prolonged balloon tamponade (n = 3) and thrombin injection in pseudoaneurysm (n = 1). In one patient, a stent graft (Viabahn, W.L. Gore & Associates, Flagstaff, Arizona) was placed to draining vein rupture that was not controlled by prolonged balloon tamponade.
Technical and clinical success rates were 93% (68/73) and 85% (62/73), respectively. Residual thrombus was found in all cases with technical failure (n = 5). Upon completion of angiography in 68 cases with technical success, a non-flow-limiting residual thrombus was noticed in eight cases. In one case with technical failure due to more than 30% of non-responding residual stenosis, hemodialysis was successful (Table 2).
The primary patency rates at 3, 6, and 12 months were 87.9% (95% confidence interval (CI): 80%–96%), 73.3% (95% CI: 62%–85%), and 64.8% (95% CI: 52%–78%), respectively; and assisted primary patency rates at 3, 6, and 12 months were 89.2% (95% CI: 82%–97%), 78.6% (95% CI: 68%–89%), and 70.7% (95% CI: 59%–83%), respectively; and secondary patency rates were 90.8% (95% CI: 84%–98%), 87.2% (95% CI: 79%–96%), and 83.1% (95% CI: 73%–93%), respectively (Table 3). Previous intervention and cephalic arch stenosis were the risk factors for lower primary (p = 0.006, 95% CI: 1.449–9.063, hazard ratio (HR): 3.624 and p = 0.012, 95% CI: 1.255–6.236, HR: 2.797) and assisted primary patency (p = 0.007, 95% CI: 1.413–8.708, HR: 3.508 and p = 0.014, 95% CI: 1.220–5.975, HR: 2.700) (Tables 4 and 5). Cephalic arch stenosis was the only risk factor for lower secondary patency (p = 0.041, 95% CI: 1.046–8.773, HR: 3.030) (Table 6).
The patency rates of AVFs after endovascular treatment.

AVF: arteriovenous fistula; CI: confidence interval.
Analysis of prognostic factors influencing primary patency using univariate and multivariate Cox proportional hazards model.
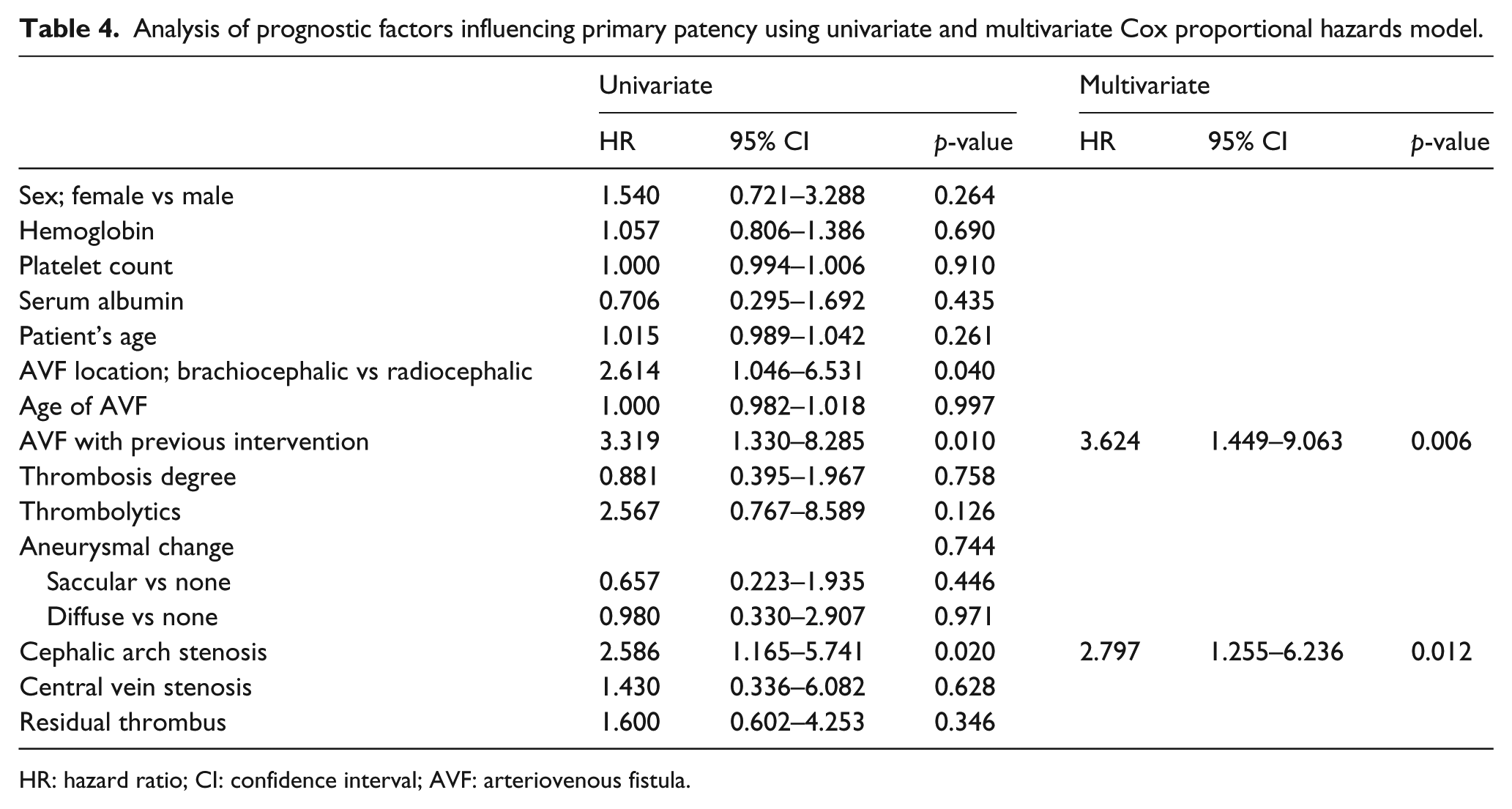
HR: hazard ratio; CI: confidence interval; AVF: arteriovenous fistula.
Analysis of prognostic factors influencing assisted primary patency using univariate and multivariate Cox proportional hazards model.
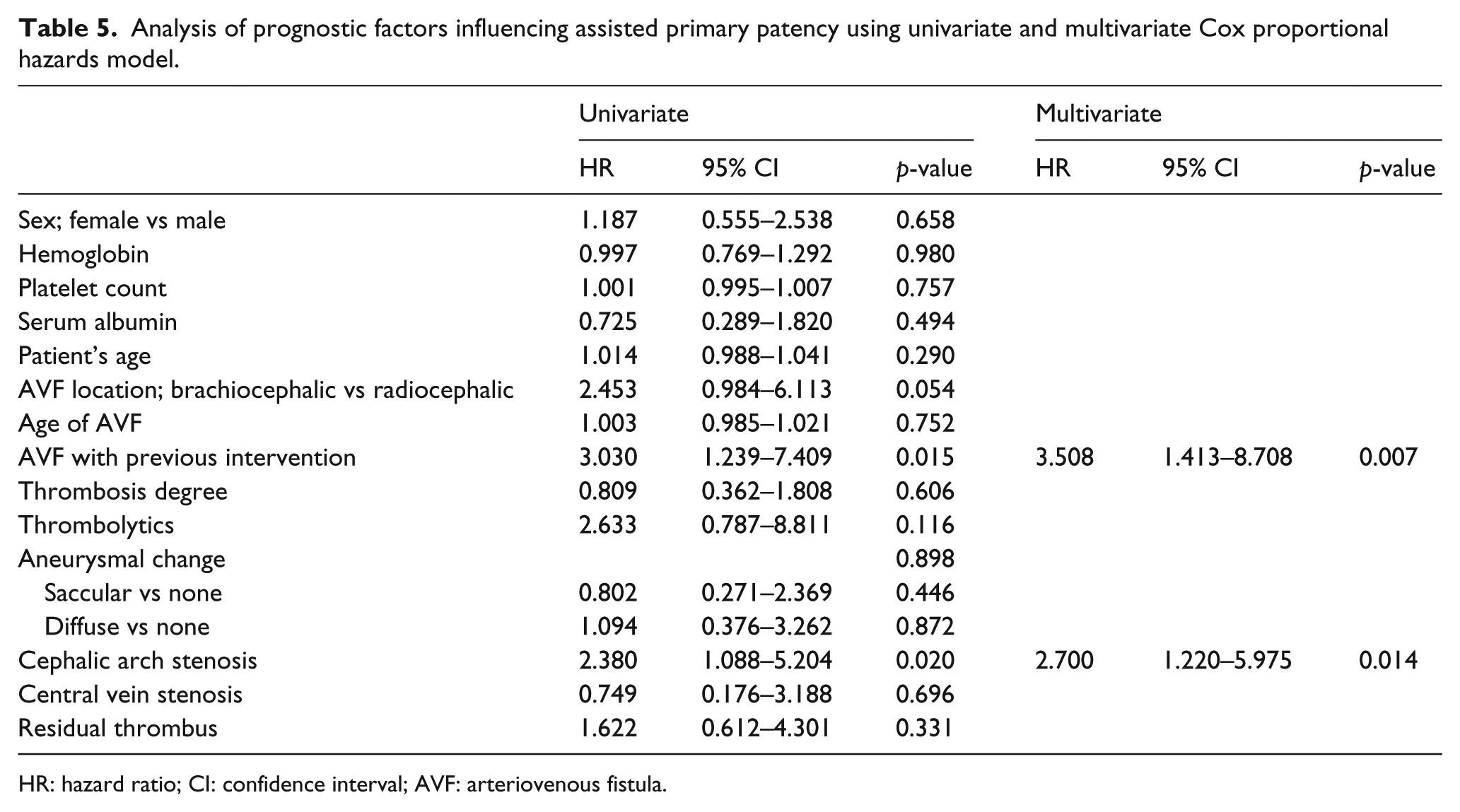
HR: hazard ratio; CI: confidence interval; AVF: arteriovenous fistula.
Analysis of prognostic factors influencing secondary patency using univariate and multivariate Cox proportional hazards model.
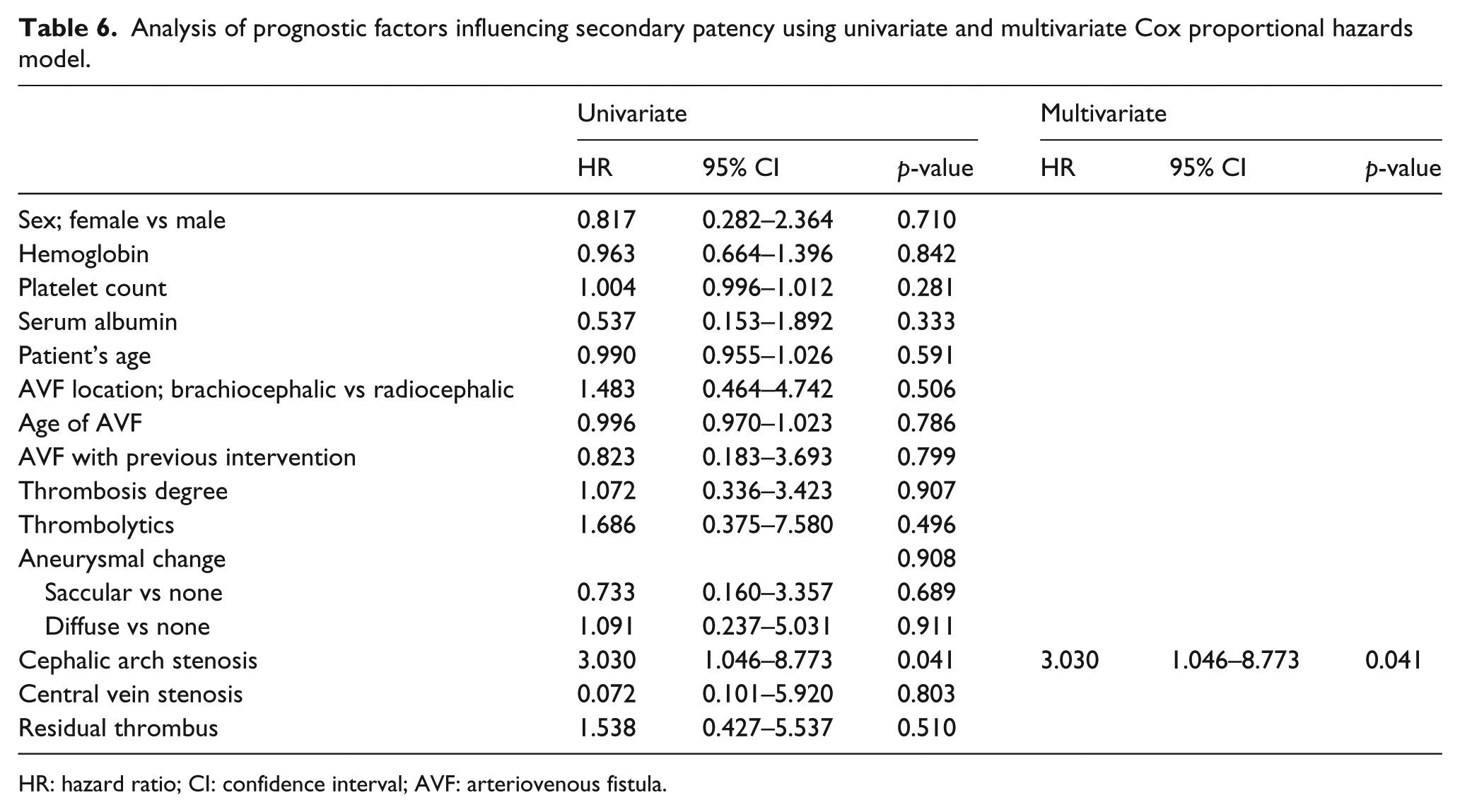
HR: hazard ratio; CI: confidence interval; AVF: arteriovenous fistula.
After recanalization procedures, there were no symptomatic pulmonary artery embolisms or major complications associated with the procedures.
Discussion
Recently, various attempts have been made to remove thrombi in AVFs using single or combined endovascular techniques with relatively high success rates.8–19,24–27 However, there was a lack of evaluation of how thrombosis influenced patency rates and whether thrombosis was the determining factor. Our study shows that thrombosis itself is not a determinant for lower patency of the AVF, and once the AVF is recanalized successfully, the patency can be prolonged.
Thrombosis in AVFs usually exhibit a chronic wall adherent nature and heavy burden.7,8 Therefore, in many cases, removing the thrombi with a single technique was impossible and a combination of endovascular methods, especially in aneurysmal segments, was needed. We mainly adopted rotational PTD and catheter-based aspiration for thrombectomy and achieved similar success rates to those of previous studies. In our study, 48 AVFs (66%) showed more than 50% thrombosis including total thrombosis (Table 1). Our results showed high technical (93%) and clinical (85%) success rates, even with relatively high rates of heavy thrombosis. During the procedures, thrombi could be removed regardless of their burden, but there was wide variation in the procedure time depending on the presence of chronic thrombi within the aneurysmal change. When we performed thrombectomy using rotational PTD, external massage for the aneurysmal segment was effective in removing chronic thrombi. However, when the thrombi were resistant to this technique, combination treatment with minimal venotomy could be considered. 8
In our study, the mean procedure time was 76.1 (±51.7) min, which was similar to or shorter than those of previous reports for recanalization of thrombosed AVF.8,11,14 However, the procedure was relatively time consuming and a great deal of effort was required by the operators. Nevertheless, this procedure was worth performing because of limited vascular resources for desirable hemodialysis sites, and the abandonment of malfunctioning AVFs may prohibit further hemodialysis. Therefore, salvaging thrombosed AVFs is essential to maintain appropriate hemodialysis and decrease the morbidity and mortality of patients requiring hemodialysis.
Among the independent factors, cephalic arch stenosis was the significant risk factor for lower primary, assisted primary, and secondary patency. The cephalic arch is the final outflow tract of the cephalic vein before its confluence with the axillary vein. According to the previous reports, the prevalence of cephalic arch stenosis ranged from 30% to 77%.28–30 Endovascular treatment of this lesion is technically difficult because of its resistance to balloon angioplasty and high rupture rates. 29 In our study, cephalic arch rupture was occurred in four patients, despite we chose the balloon with the reference of adjacent cephalic vein. Therefore, excessive dilatation should be avoided for the stenotic cephalic arch, especially when there was a considerable size discrepancy between stenotic cephalic arch and the adjacent draining vein. Even the cases that the cephalic arch was not ruptured showed recoiling after balloon angioplasty and residual stenosis. These cases also showed early occlusion of the AVF. Therefore, stenotic cephalic arches can be regarded as the main cause of early failure of the AVF. Recently, for these lesions, various methods such as cutting balloon angioplasty or stent graft placement were used to treat cephalic arch stenosis and showed better results than conventional balloon angioplasty.31–33
Previous intervention was also a risk factor for lower primary and assisted primary patency. The presence of a previous intervention suggests that the AVF has underlying problems that require intervention and that the AVF is prone to repeated thrombosis. In our cases, AVFs with previous interventions showed recurrent draining vein stenosis that was treated previously. However, this was not the risk factor for lower secondary patency, which means that once the recanalization succeeds, the secondary patency of AVF can be prolonged by additional endovascular treatment.
There have been a few studies on the relationship between patency and blood flow during and after interventional procedures.34,35 According to these studies, an immediate hydrodynamic outcome was not a prognostic factor for primary patency, but low fistula age and a history of previous intervention were found to reduce primary patency. In this study, cellular injury and neointimal hyperplasia induced from angioplasty are referred to as the important predisposing factors for repeated intervention. This result is in accordance with our result that previous intervention causes lower primary and assisted primary patency.
During mechanical thrombectomy using a rotational PTD device, we experienced device failure in two patients, which occurred during thrombectomy for the aneurysmal segment. According to a previous report, rubber-tip disconnection and fragmentation of the rotatory basket were reported during thrombectomy with a rotational PTD device.36,37 These events occurred in an angulated vessel or indwelling stent or aneurysmal segment. Therefore, careful use of the PTD is recommended in such situations to avoid complications.
In comparison with open surgical thrombectomy, endovascular thrombectomy has several advantages in addition to less surgical trauma. First, endovascular procedures can be performed rapidly without delay for the preoperative preparation. Second, if the AVF is successfully recanalized, hemodialysis can be resumed immediately. Third, there is no need for temporary hemodialysis catheter indwelling during the recovery of the wound after surgical thrombectomy. Considering these advantages, endovascular thrombectomy is recommended as a first treatment of choice in patients with thrombosed AVFs. Our study showed that thrombosed AVFs could be recanalized eventually by endovascular treatment. Therefore, thrombosed AVFs should not be abandoned even if they are occluded with chronic thrombi, and active efforts should be made to salvage them.
However, there are some limitations in our study owing to its retrospective nature and non-randomization. First, the interventional protocol was not uniformly designed for each interventionist. Therefore, the decision regarding recanalization methods was subjective and operator dependent. Second, our study was limited by the relatively small size of the study population and there may be several independent factors that were not evaluated. In addition to the factors analyzed in our study, there are some preconditions to be considered. Optimal surgery to create hemodialysis access is an important prerequisite, and the results of the recanalization procedures performed in a dedicated hemodialysis intervention center would be better. Third, our study was performed at a single institution, and there may be a selection bias. Therefore, additional prospective studies with a larger number of cases are needed to confirm the prognostic factors influencing thrombosed AVFs.
In conclusion, endovascular treatment was effective for the immediate recanalization of thrombosed AVF. In addition, previous intervention and cephalic arch stenosis were significantly related to lower AVF patency.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.