
Abstract
Objective:
Postoperative renal dysfunction necessitating hemodialysis after implantation of ventricular assist devices presents a challenge with respect to establishment of hemodialysis access. Lack of pulsatile flow has led to concerns that arteriovenous fistulas will not mature. This study aims to evaluate arteriovenous fistula as a method of hemodialysis.
Methods:
Consecutive patients who underwent implantation of a ventricular assist device between 1988 and 2016 with a subsequent need for hemodialysis were identified. Retrospective data were collected for patients requiring hemodialysis through an arteriovenous fistula or arteriovenous graft. Access flow rates and duration of patency are reported.
Results:
Sixty-four patients were identified (10 required long-term hemodialysis, 5 via arteriovenous fistula, 1 via arteriovenous graft). All six patients receiving long-term hemodialysis access were on continuous-flow ventricular assist devices. Brachiocephalic arteriovenous fistulas were performed in all arteriovenous fistula patients, and the average preoperative vein diameter was 4.1 ± 0.9 mm. On 30-day follow-up, the average flow rate was 1262 ± 643 mL/min (880–2220). In arteriovenous fistula patients, one died at 30 days, one arteriovenous fistula required ligation for steal syndrome at 5 months, and one was abandoned after 10.7 months for low flow. Of remaining fistulas, one was converted to an arteriovenous graft at 1.7 years for malfunction (with 5.3 month patency), and one remains open at 4.0 years.
Conclusion:
Arteriovenous fistulas should be considered in selected patients with ventricular assist devices as a means of long-term hemodialysis access to avoid use of catheters. Maturation and usage of primary arteriovenous fistulas is possible despite lack of pulsatile flow.
Introduction
Heart transplantation is the definitive treatment for end-stage heart failure. However, fewer than 3000 heart transplants are performed annually. Mechanical circulatory support devices provide an alternative to transplantation, and ventricular assist devices (VADs) are increasingly used either as destination therapy (DT) or as a bridge to transplantation (BTT). Implantation of these devices now exceeds 20,000 annually. 1 VADs may be implanted to augment left (LVAD: left ventricular assist device) or right (RVAD: right ventricular assist device) heart function.
Hemodynamic instability and subsequent renal dysfunction is a common clinical scenario in advanced heart failure patients, particularly those requiring VAD implantation. The incidence of acute kidney injury (AKI) after continuous-flow LVAD implantation ranges between 7% and 38% in recent studies (depending on how AKI is defined).2,3 Postoperative renal dysfunction necessitating long-term hemodialysis (HD) after LVAD implantation presents a challenge with respect to establishment of dialysis access. A central venous catheter (CVC) is the most common dialysis access modality in this population; however, catheter use places patients at an increased risk of LVAD infection and subsequent sepsis. The landmark REMATCH (Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart) trial reported sepsis as the leading cause of death in the LVAD arm of the study. 4 Another study reported that 12 out of 30 (40%) patients who required post-LVAD HD for AKI died from sepsis. 5
Arteriovenous fistula (AVF) is the recommended dialysis access for end-stage renal disease (ESRD) patients. The continuous and non-pulsatile flow produced by modern LVADs has been postulated to preclude successful maturation of an AVF or maintenance of an arteriovenous graft (AVG). Recent reports of ESRD patients successfully undergoing dialysis through an AVF while on LVAD support have challenged the dogma that maturation is not possible.6,7 We report our institutional experience aiming to evaluate primary AVF or AVG as a method of dialysis access in patients on continuous-flow LVAD support.
Materials and methods
The research protocol was reviewed and approved by the Institutional Review board of the University of Pittsburgh. The need for patient consent was waived.
Patients and procedures
We identified all patients with VADs who required postoperative HD between 2002 and 2016 and reviewed those who underwent placement of an autogenous AVF or prosthetic AVG between 2011 and 2016. Data were collected on preoperative demographics and comorbidities, procedural details, perioperative morbidity and mortality, and long-term patency and access-related complication rates. Follow-up was recorded until failure of HD access.
Statistical analysis
De-identified data were analyzed through a database using Microsoft Excel (Microsoft Corporation, Redmond, WA). Descriptive statistics were applied where appropriate.
Results
Sixty-four patients with LVADs requiring postoperative HD were identified. Of those 64 patients, only 10 required long-term (post discharge) HD, and the remaining 54 had renal recovery. Six of those 10 requiring long-term HD underwent placement of an AVF (5) or AVG (1) (Table 1), with the remaining four utilizing tunneled dialysis catheters (TDCs) for long-term access. Implantation of the lone AVG was due to inadequate peripheral vein diameters. Placement of AVF or AVG was not attempted if vein mapping demonstrated inadequately sized veins for access, patients were too critically ill to undergo further interventions, or life expectancy was limited. Two of four who did not receive an attempt at access placement had inadequate vein diameters and limited life expectancy, and the remaining two patients were too critically ill for access placement. All four of the patients in the TDC only cohort died within 21 months of initiation of HD with three dying within 6 months of initiation of HD. Thirty percentage of all TDCs (3/10) required at least one replacement (two for infection, one for malfunction). The mean number of total TDC days in patients who received AVF or AVG was 291 ± 189 days with catheter removal being achieved at a mean of 72 ± 28 days. Catheter removal was achieved in three of six patients who underwent access placement.
Preoperative and postoperative characteristics.
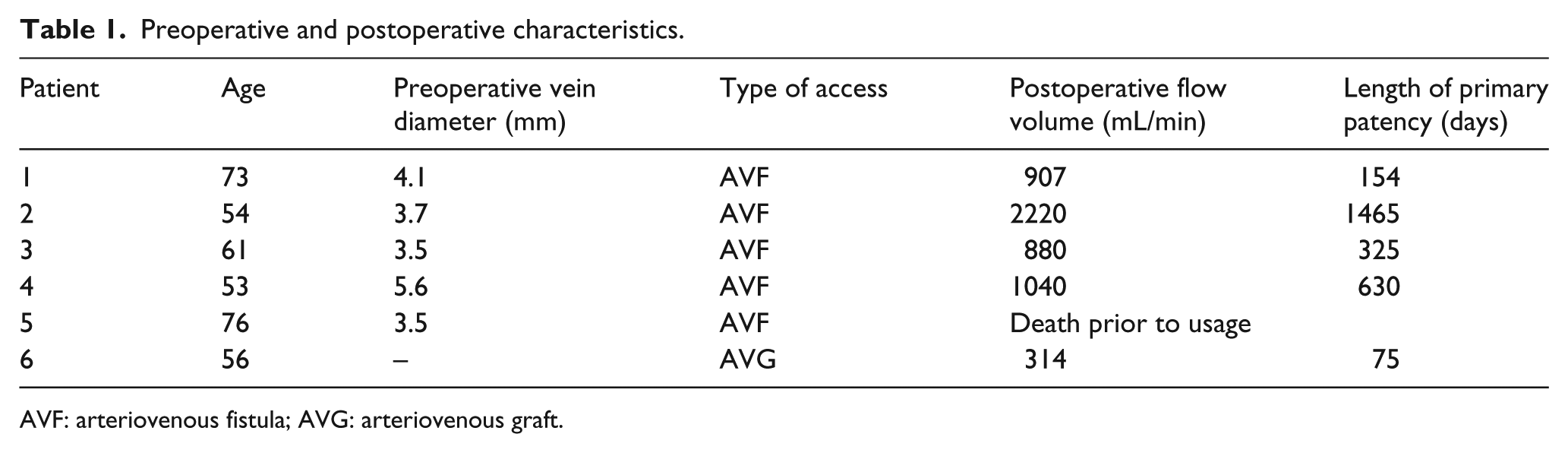
AVF: arteriovenous fistula; AVG: arteriovenous graft.
All patients were on continuous-flow VAD, and 3/6 were on DT. All patients were male with a median age of 58.5 years (range 53–76). All patients were on anticoagulation. All AVFs were of a brachiocephalic configuration at the antecubital fossa, and the single AVG implanted was a brachio-brachial forearm loop graft. The average preoperative target vein diameter was 4.1 ± 0.9 mm without a tourniquet. Moderate sedation with local anesthetic infiltration was used for all patients, and ultrasound examination was repeated in the operating room prior to incision. One of the AVF patients died within 30 days with a patent but unused fistula. On 30 day follow-up in the remaining patients, the average flow rate was 1262 ± 643 mL/min (range 880–2220). One AVF required ligation for ischemic steal syndrome at 5 months prior to use with a flow volume of 907 mL/min. The AVG was successfully accessed at 1 month but later became infected and required explantation at 3 months. The remaining 3 AVFs were successfully used for HD. One was abandoned at 10.7 months for low flow, one was converted to an AVG at 1.7 years for malfunction and lasted 5.3 months, and one remains open throughout the study period at 4.0 years.
Discussion
Long-term patency of HD access remains a challenge in all patients with ESRD and primary patency of AVFs has been reported as low as 72% at 6 months. 8 New generation LVAD systems such as the Heartmate II (Thoratec Corporation, Pleasanton, CA) provide non-pulsatile continuous flow, which can alter flow and vascular reactivity of AVFs. These changes in hemodynamics have been thought to prevent maturation of AVFs. In patients who receive an LVAD system as DT, 77.6% have a life expectancy that exceeds 1 year. Many more patients successfully utilize LVADs as a BTT or bridge to recovery (BTR). 9 Patients who require long-term HD may benefit from AVF or AVG as a means of access.
Analysis of the United States Renal Data System (USRDS) database has shown a median time to TDC removal of 70 days for AVGs and 155 days for AVFs. 10 Maturation of AVFs commonly takes up to 8–10 weeks and patients remain at risk for CVC infections during this time period. While prosthetic AVGs are accessible in a shorter time period compared to AVF, prosthetic AVGs carry their own risk of blood stream and graft infections; pooled rates of access-related blood stream infections in the United States are highest for CVCs (0.25 events per 100 catheter days) followed by AVGs and finally AVFs.11,12 CVC-related blood stream infections may be life-threatening and pose an even higher risk for the LVAD patient population, and thus, rapid removal is of utmost importance. The lower rate of access-related blood stream infections associated with AVFs and AVGs may be advantageous to this patient population as infection of VAD hardware may be fatal.
Our study demonstrated that maturation and subsequent long-term use of AVFs is possible in patients with LVADs with adequate vein diameter and of appropriate surgical risk. Three of five AVFs remained usable for at least 10.7 months. Two patients maintained patency of their AVFs for greater than 18 months (1.7 and 4.0 years). These findings suggest that AVF maturation is independent of pulsatility as previously suspected. Maturation may be blood pressure dependent; however, pulse pressure variation may not be required if continuous flow supplied by VADs is sufficient for maturation as we have shown. Previous small series or case reports have also demonstrated that maturation is possible.6,7,13 Within these reports, maturation was recorded and AVF usability was documented for up to 511 days. Long-term data on AVF usability, primary patency, and secondary patency rates are yet to be determined in the VAD population. The success of autogenous accesses in our cohort may be related to the large average target vein diameter (4.1 ± 0.9 mm). It is known that target vein diameters greater than 4.0 mm are associated with a significant benefit in maturation rates. 14 Ultrasound examination of venous anatomy is done without a tourniquet in our institution and all surgeons reevaluate the venous anatomy in the operating room prior to incision. Large variations exist in our group with regard to the choice of anesthetic, although the majority are done under local rather than regional anesthesia. Within our institution, patients who are deemed medically stable after implantation of VADs and require long-term HD are routinely evaluated for placement of AVF or AVG. Patients with peripheral veins measuring greater than 3 mm would undergo exploration of the vein and AVF creation if adequate, and those with poor quality veins will be considered for an AVG. In this VAD cohort specifically, more proximal fistula creation was preferred due to hemodynamic considerations.
In this study cohort, one patient underwent AVG placement due to inadequate peripheral vein diameters. Despite successful use of the graft after incorporation, this was explanted due to infection after only 3 months. This demonstrates that use of prosthetic grafts in this patient population is possible; however, this would not be considered a successful long-term outcome. More evidence is required before surgeons should consider AVG as a standard option for this patient population.
Limitations to this study include small sample size, single institution experience, and its retrospective nature. Despite these limitations, our study demonstrates that in patients with a VAD, maturation of an AVF is possible. Consideration for AVG placement may be given in patients who do not have options for autogenous AVF. Safety and efficacy are unable to be assessed in this small study cohort, and further research should be considered in this patient population.
Conclusion
Patients who require long-term HD after implantation of VADs (as bridge or DT) might benefit from placement of autogenous HD access. Maturation and successful use of autogenous HD access is possible despite the lack of pulsatility in newer-generation VADs. AVFs may function in well-selected patients, but more research is needed to provide specific guidance on this unique patient population.
Footnotes
Authors’ note
Presented at the 31st annual EVS (Eastern Vascular Society) Meeting, Georgia, 5–8 October 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by Grant 2T32HL098036-06 from the National Institutes of Health.