
Abstract
Introduction:
Peripherally inserted central catheter tip migration is an infrequent event that occurs in neonatal, pediatric, and adult patients. We discuss a novel technique of utilizing intracavitary electrocardiogram to help confirm proper peripherally inserted central catheter tip repositioning, thereby reducing the need for serial radiographs.
Case presentation:
A case series of four patients will be discussed. The first three patients had peripherally inserted central catheter tips that were initially appropriately positioned but had later peripherally inserted central catheter tip migration. The use of intracavitary electrocardiogram was able to confirm the appropriate repositioning of the peripherally inserted central catheters without the need for serial radiographs. The fourth patient had several central lines in place, which led to difficulty in identifying the peripherally inserted central catheter tip location. The use of intracavitary electrocardiogram confirmed proper positioning of his peripherally inserted central catheter tip when standard radiographs could not provide clarity.
Discussion:
Several techniques have been published on methods to reposition a migrated peripherally inserted central catheter tip back to the superior vena cava/right atrial junction. These repositioning techniques often require fluoroscopic guidance or a confirmatory radiograph to assess the appropriate peripherally inserted central catheter tip location. At times, several radiographs may be required before the tip is successfully repositioned. This novel application of intracavitary electrocardiogram can help to minimize radiographs when peripherally inserted central catheter tip repositioning is required.
Introduction
Peripherally inserted central catheters (PICCs) have been used in adult intensive care units for several decades. 1 PICCs have been increasingly used in the care of critically ill neonatal and pediatric populations, and the availability of power-injectable PICCs has expanded their utility across the pediatric landscape.2,3 PICC placement at the bedside is a frequent practice to reduce complications inherent to transport as well as optimizing staffing resources and is often completed without adjunct fluoroscopy.4,5 Neonatal and pediatric PICC providers seek alternative methods for improving localization of the PICC tip position, preferably via non-irradiating technologies. One such method, intracavitary electrocardiogram (IC-ECG) monitoring,6,7 provides immediate feedback on the catheter tip position to guide the proceduralist in optimizing the tip position when accurate localization with ultrasound is not possible. During the use of IC-ECG, the PICC is advanced to the point where the maximal P-wave is identified, signifying the PICC location at the superior vena cava/right atrial (SVC/RA) junction. 6
Following the initial placement of an upper extremity PICC tip at the SVC/RA junction, tip migration may subsequently occur within the course of care, particularly in pediatric populations.8–12 Frequent sites for PICC tip migration include the internal jugular vein, brachiocephalic vein, or looping in the SVC. 10 Several “blind” techniques for repositioning PICC lines at the bedside have been described including abducting the arm, a high-flow flush technique (HFFT), or repositioning the patient.13–15 The HFFT involves a rapid manual flush of the PICC with a 10- or 20-mL syringe filled with 0.9% sodium chloride with the goal of redirecting the tip of the PICC to its original position. 15 Blind bedside techniques are often unsuccessful and may require several radiographs during the course of repositioning.15,16
In our pediatric intensive care unit (PICU), we occasionally encounter migrated PICC tips. At times, failure to appropriately reposition the PICC at the bedside has required the patient to travel to interventional radiology for repositioning under fluoroscopy. The risks of intra-hospital transport of the critically ill patient are well documented.4,5 In an effort to minimize radiation exposure and the potential risks of intra-hospital transport, we created an alternative solution for bedside PICC tip repositioning. Since we have utilized IC-ECG during initial PICC insertion, we felt this technology may be employed as a potential solution to this problem. We have now successfully incorporated the saline column method of IC-ECG to help guide the repositioning of PICC lines at the bedside. This application of IC-ECG is novel as most of the literature related to the utilization of IC-ECG have been for confirmation of the tip position at initial insertion. We will describe how IC-ECG can be applied following initial placement to confirm successful PICC tip reposition.
Case description
At the time of writing this article, we did not have a commercially available IC-ECG device. We therefore utilized the bedside monitor in conjunction with a created sterile device to provide an IC-ECG tracing with a saline column (Figure 1). To create the sterile device, we use a T-connector (CareFusion, San Diego, CA, USA) that is attached to the PICC. A 22-gauge 2.5-in spinal needle (BD, Franklin Lakes, NJ, USA) is inserted 2 cm through the injection port of the T-connector. The right arm lead is then attached to the spinal needle, and the system is flushed with normal saline. Through this device, we are then able to follow the IC-ECG tracing while providing a means to provide the HFFT through the T-connector and PICC.
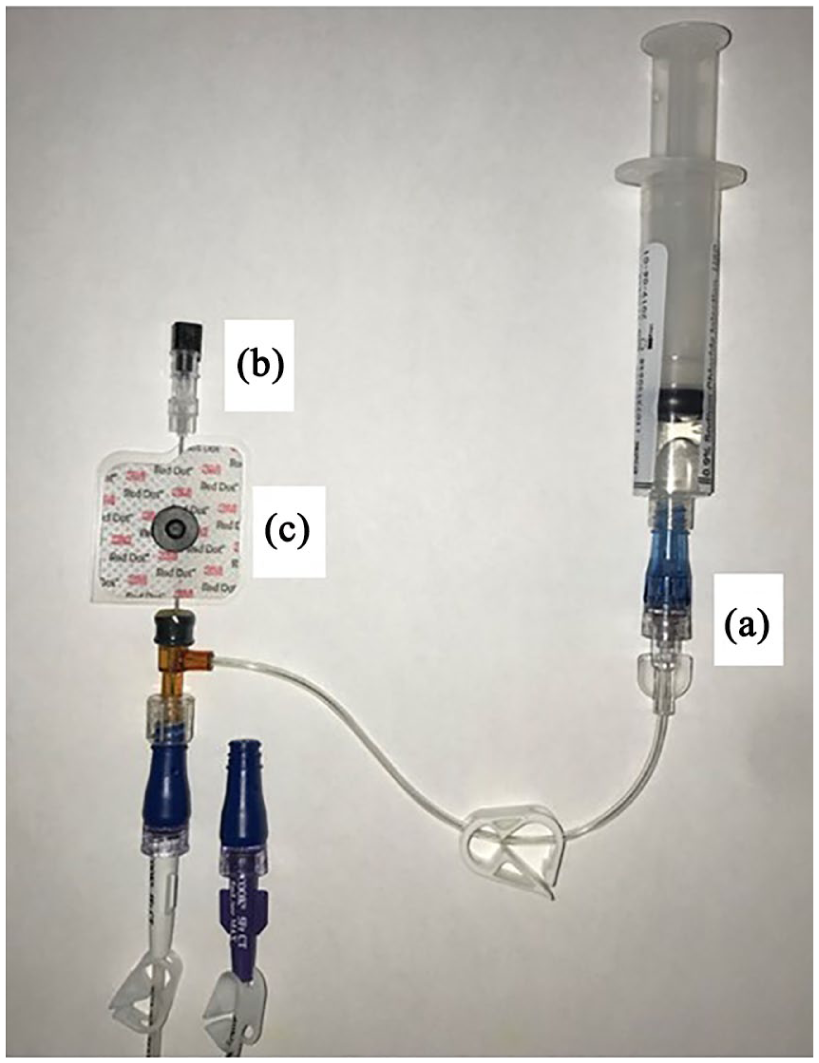
Device to provide a saline column for IC-ECG and a route for power flushing. A saline flushed T-connector (a) is attached to the PICC line. Through the injection port of the T-connector a 22-gauge spinal needle (b) is inserted 2 cm. An ECG sticker (c) and the right arm chest lead are attached to the spinal needle.
Once the device is connected to the patient, a baseline examination of the P-wave morphology is attained. The proceduralist then can perform maneuvers in an attempt to reposition the PICC. These maneuvers may include the HFFT, arm abduction, or repositioning of the patient. Following each maneuver, the P-wave morphology is assessed to see if the PICC tip is now optimally positioned. After confirming the appropriate PICC tip position with IC-ECG, a single chest radiograph is performed to document the position of the PICC. The following cases will be presented to further describe the benefits of IC-ECG in the management of PICC migration and tip localization.
Case 1
An 11-month old female (6.4 kg) with a past medical history of Caroli disease presented with progressive hepatic failure. Prior to her liver transplant, she had a single lumen left subclavian broviac placed. Following her liver transplant, she required placement of a PICC for additional secure access. A 3-Fr single lumen polyurethane power-injectable PICC was placed in her right basilic vein without difficulty. A micro-introducer kit utilizing a modified Seldinger technique was employed to access the vessel. IC-ECG was utilized to identify the tip position at the SVC/RA junction and, per unit protocol, chest radiography confirmed the final tip location (Figure 2(a)).
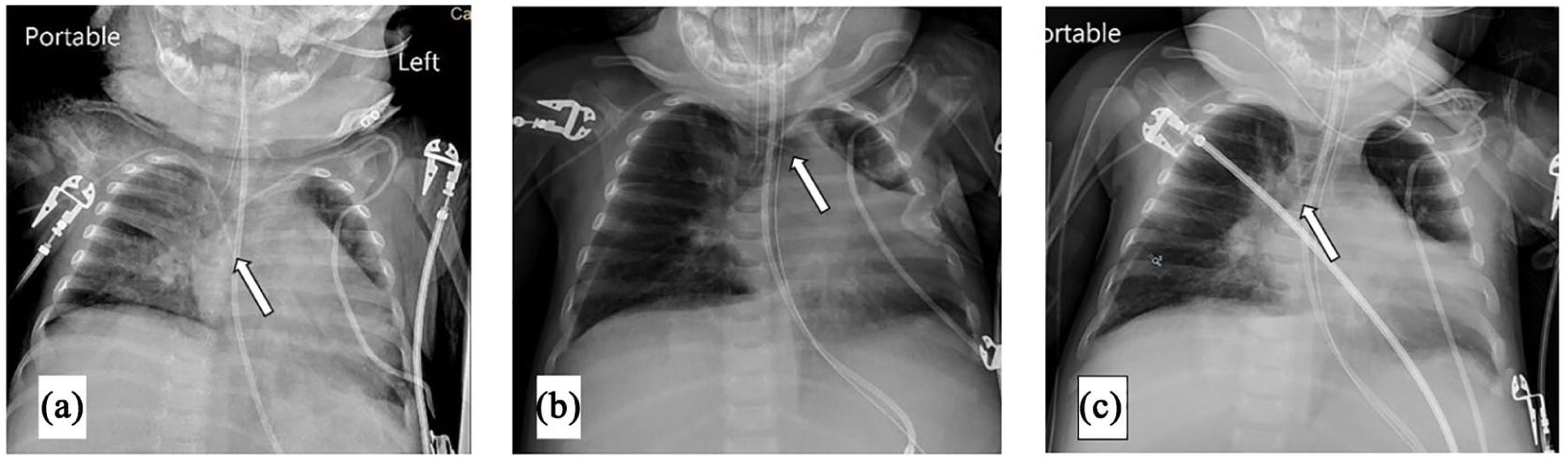
(a) Initial placement CXR with tip of PICC at the SVC/RA junction. (b) CXR showing tip of PICC in the left brachiocephalic vein requiring repositioning. (c) CXR showing tip repositioned back at the SVC/RA junction.
Two days after placement of the PICC, her routine morning chest radiograph revealed that her PICC was malpositioned with the tip in the left brachiocephalic vein (Figure 2(b)). Her medical team attempted to reposition the line at the bedside by means of the HFFT and abducting her arm. The team completed three attempts and three chest radiographs before her PICC was appropriately repositioned.
Two days later the tip of her PICC again was malpositioned in the left brachiocephalic vein. We then utilized IC-ECG to help guide the repositioning. As expected, the initial P-wave morphology was not similar to the morphology on the date of placement. We then proceeded to use the HFFT and abduct her arm. On the third attempt, the IC-ECG tracing showed the expected changes in the P-wave morphology, confirming the optimal tip position at the SVC/RA junction. We then performed a chest radiograph to document the appropriate tip position (Figure 2(c)).
Case 2
A 4-year old male (16 kg) with a past medical history significant for chronic static encephalopathy, myoclonic epilepsy, and a left middle fossa arachnoid cyst who was status post a cystoperitoneal shunt and cyst fenestration presented with a shunt infection. He required a right brachial 3-Fr single lumen polyurethane power-injectable PICC for his prolonged antibiotic therapy.
His initial PICC was placed at the bedside with the use of IC-ECG to confirm placement at the SVC/RA junction (Figure 3(a)). A micro-introducer kit utilizing the modified Seldinger technique was employed to access the vessel. Several days following his PICC placement, his line was noted to be in the left brachiocephalic vein (Figure 3(b)). We were able to utilize the saline column method of IC-ECG to aid in the repositioning of his PICC. It required two attempts with the HFFT and arm abduction before IC-ECG showed the expected change in the P-wave morphology. One chest radiograph was performed to document the appropriate tip position (Figure 3(c)).
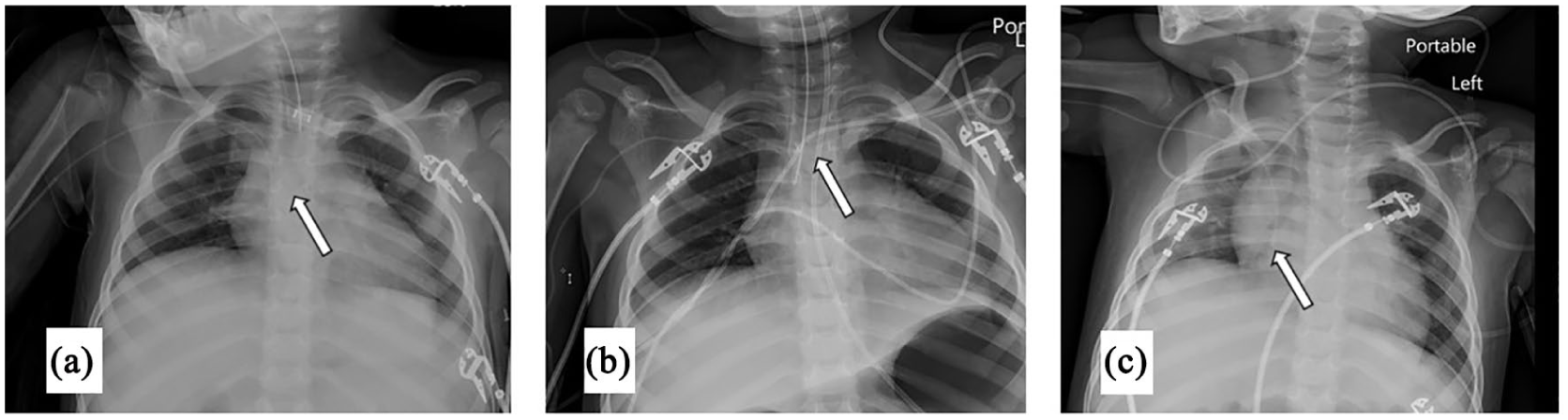
(a) Initial placement CXR with tip of PICC at the SVC/RA junction. (b) CXR showing tip of PICC in the left brachiocephalic vein requiring repositioning. (c) CXR showing tip repositioned back at the SVC/RA junction following extubation later the same day.
Case 3
A 14-month old female (7 kg) with a past medical history of trisomy 21, transitional atrioventricular (AV) canal status post repair, pulmonary hypertension, chronic lung disease, and reactive airway disease presented with acute on chronic respiratory failure due to respiratory syncytial virus. She was mechanically ventilated and required secure access to manage her continuous infusions. She had a bedside placement of a 2.6-Fr double lumen silicone-based non-power-injectable PICC in her left basilic vein. A micro-introducer kit utilizing the modified Seldinger technique was employed to access the vessel. IC-ECG was used at line insertion to confirm the tip position at the SVC/RA junction and, per unit protocol, chest radiography documented the appropriate tip position (Figure 4(a)).
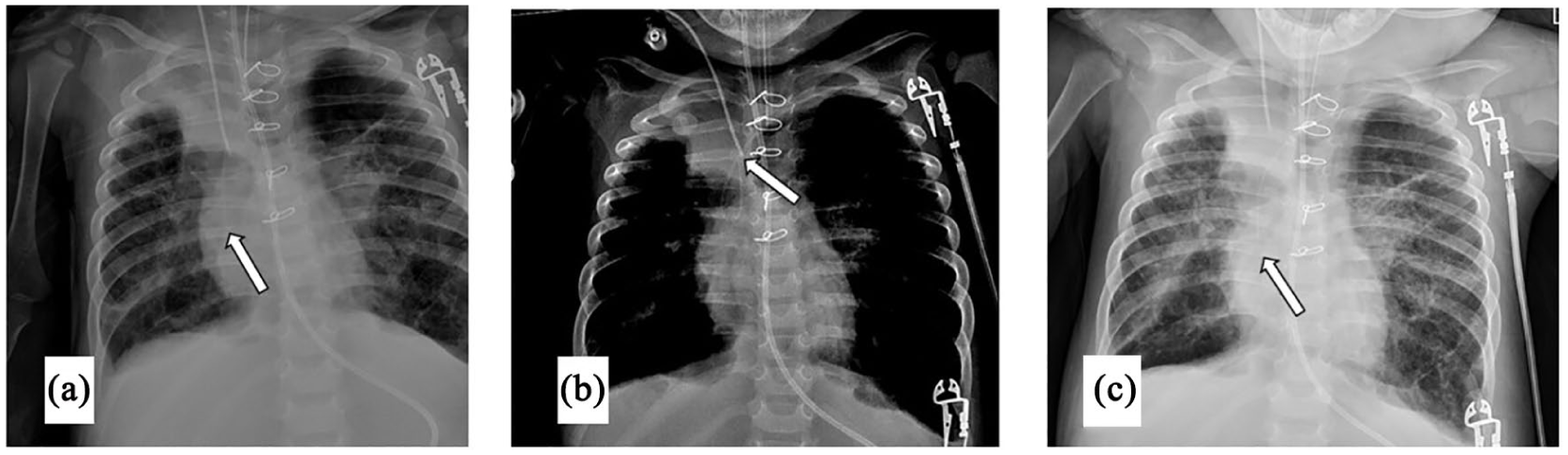
(a) Initial placement CXR with tip of PICC at the SVC/RA junction. (b) CXR showing distal end of PICC curled in the SVC requiring repositioning. (c) CXR showing tip repositioned back at the SVC/RA junction.
The following morning a chest radiograph to evaluate the endotracheal tube position revealed that her PICC was looped in the SVC (Figure 4(b)). IC-ECG utilizing the saline column method demonstrated ECG morphology, which had changed since initial insertion. We used the HFFT once resulting in IC-ECG morphology consistent with the SVC/RA position. A chest radiograph confirmed appropriate line repositioning (Figure 4(c)).
Case 4
A 17-year old male (55 kg) with relapsed stage IV neuroblastoma was transferred to the PICU for the treatment of worsening respiratory distress. He progressed to acute respiratory distress syndrome (ARDS) and required a 4-Fr double lumen polyurethane power-injectable right basilic PICC for his continuous infusions and antibiotics. At that time, he already had two implanted ports, one in his left internal jugular vein and one in his right subclavian vein in place. His PICC was placed by an interventional radiologist with the tip at the SVC/RA junction (Figure 5(a)). A micro-introducer kit utilizing the modified Seldinger technique was employed to access the vessel.
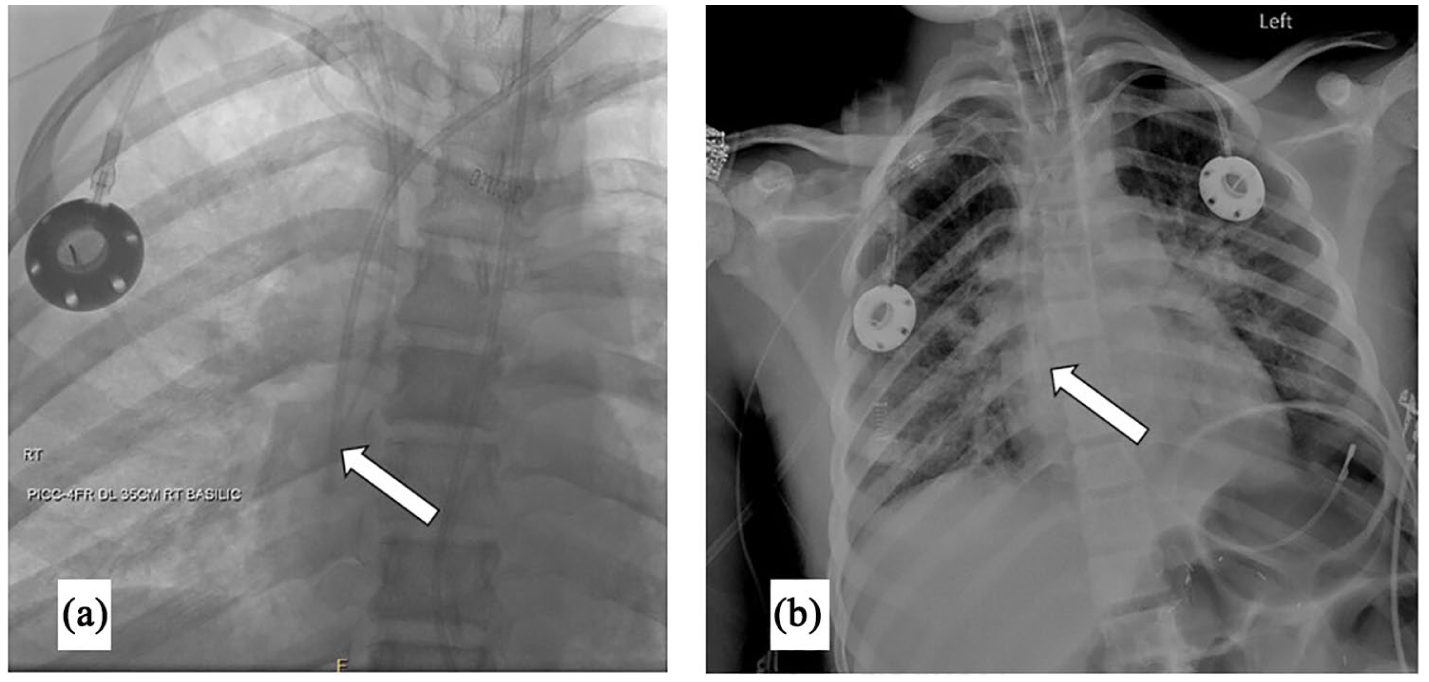
(a) Fluoroscopic image showing the PICC tip at the SVC/RA junction. (b) Bedside CXR with limited ability to view the PICC tip related to competing central catheters.
The following morning, the PICC tip position was difficult to identify on the chest radiograph due to the other overlying central catheters (Figure 5(b)). We again employed the saline column method of IC-ECG and were able to confirm the appropriate position of his PICC without the need for further chest radiographs.
Discussion
PICC tip migration leading to post-placement malposition is a rare event. There is literature describing the incidence of malpositioned PICCs on initial insertion, but there are no clear data on the incidence of PICC tip migration.16–18 It is likely that, given patient anatomic size and catheter size differences, PICC tip migration occurs more frequently in pediatric populations. 12 Several methods of repositioning a migrated PICC have been suggested.13,14,16 Some of these methods may provide an immediate reposition of the line, such as the HFFT, where the others may require time for the line to passively reposition itself. Previously, the only means to have real-time assessment of the PICC tip position was with fluoroscopy. Ultrasound is a promising technology to assess vascular access device location and, similar to IC-ECG, does not expose patients to ionizing radiation. Ultrasound has been successfully used in the neonatal and pediatric population to confirm varied central catheter tip positions. There are occasions where ultrasound may not provide an adequate view of the SVC/RA junction, particularly in larger children or adults as well as those supported with mechanical ventilation.19,20 When the SVC/RA junction is unable to be visualized by ultrasound, the need for an alternative, non-radiographic method to localize the PICC tip is suggested.
This novel application of IC-ECG can be performed with easily accessible hospital supplies to provide immediate feedback to the proceduralist, ensuring appropriate return of the PICC tip to the SVC/RA junction. One limitation to this method is that the PICC tip should be at the SVC/RA junction with appropriate P-wave morphology on initial insertion. If the PICC was secured above the SVC/RA junction following initial insertion, then P-wave morphological change may not occur despite return to the prior tip location. We strongly recommend this technique in critically ill children to provide timely and accurate repositioning of PICCs without the need for serial chest radiographs or transportation off the unit to a fluoroscopy suite.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Per local institutional review board (IRB) guidelines, the case series was not deemed a research study and therefore did not require IRB approval.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained for placement of PICCs. No written consent was required by the author’s institution for a case presentation including deidentified patient data.