
Abstract
End-stage kidney disease patients who are candidates for surgical arteriovenous fistula creation commonly experience obstacles to a functional surgical arteriovenous fistula, including protracted wait time for creation, poor maturation, and surgical arteriovenous fistula dysfunction that can result in significant patient morbidity. The recent approval of two endovascular devices designed to create a percutaneous arteriovenous fistula enables arteriovenous fistula creation to be placed in the hands of interventionalists, thereby increasing the number of arteriovenous fistula providers, reducing wait times, and allowing the patient to avoid surgery. Moreover, current studies demonstrate that patients with percutaneous arteriovenous fistula experience improved time to arteriovenous fistula maturation. Yet, in order to realize the potential advantages of percutaneous arteriovenous fistula creation within our hemodialysis patient population, it is critical to select appropriate patients, ensure adequate patient and dialysis unit education, and provide sufficient instruction in percutaneous arteriovenous fistula cannulation and monitoring. In this White Paper by the American Society of Diagnostic and Interventional Nephrology, experts in interventional nephrology, surgery, and interventional radiology convened and provide recommendations on the aforementioned elements that are fundamental to a functional percutaneous arteriovenous fistula.
Keywords
Introduction
With the advent of the Fistula First Initiative, the prevalence of arteriovenous fistulae (AVF) in US hemodialysis patients is approaching 70%, yet poor AVF maturation and dysfunction remain. Development and approval of endovascular devices to create a percutaneous arteriovenous fistula (pAVF, also known as an endovascular or “endoAVF”), rather than standard surgical arteriovenous fistula (sAVF) creation, will expand the number of AVF providers, decreasing the long wait time for AVF creation found in many areas of the United States. Early studies with the two approved devices, Avenu Medical’s Ellipsys (https://www.youtube.com/watch?v=kPfTDaTQLa0) and BD Bard’s WavelinQ (https://vimeo.com/295441830), demonstrate a shorter time to pAVF maturation with less associated dialysis catheter exposure and avoidance of surgery in this fragile patient population.1,2
This American Society of Diagnostic and Interventional Nephrology White Paper reviews elements critical for pAVF functional success that are equally as important as the technical procedure itself—patient selection, patient and dialysis unit education, and pAVF maturation assessment, cannulation, and monitoring.
Importance of the multidisciplinary team
Why is a team approach needed?
Dialysis vascular access care is often fragmented with suboptimal communication between patients, families, nephrologists, dialysis units, surgeons, and interventionalists. Typically, vascular access procedures are planned and executed by one provider such that details of what was done or why may be lacking. Communication and education among all stakeholders are necessary for successful creation and maintenance of all forms of accesses, but particularly for pAVFs, given their differences and novelty.
Who are the team members?
The patient and their relevant loved ones (supporters) must understand their dialysis options and the advantages and disadvantages of a pAVF compared with an sAVF. In order to properly inform the patient, the nephrologist must understand the technology, appropriate patient selection, and whether the pAVF or sAVF will provide the prescribed dialysis dose. The dialysis unit should understand the anatomic and physical examination nuances of a pAVF and techniques for successful cannulation. A close working relationship between the interventionalist and surgeon is necessary in the event of a complication, need for secondary procedure, or conversion to an alternate access.
How can team member engagement be achieved?
Multidisciplinary meetings and shared decision-making are recommended for successful patient screening and procedural and cannulation outcomes. Timely communication with dialysis centers, and support by providing patient and staff educational materials and on-site ultrasound-guided initial cannulation (as necessary), will help achieve successful pAVF use.
Patient selection for pAVF creation
Patient eligibility
Who is the ideal patient for a pAVF?
The ideal pAVF patient is one whose anticipated life expectancy exceeds 1 year and is not a candidate for a distal (wrist) AVF. In addition, the patient should meet the vascular anatomy parameters outlined under “Vascular eligibility” for each of the Food and Drug Administration (FDA)-approved pAVF devices.
Are there contraindications to pAVF creation?
A lack of surgical support is a contraindication to pAVF creation, as the target vein(s) may require superficialization or revision.
When can a pAVF be created?
Advanced chronic kidney disease (CKD) and end-stage kidney disease (ESKD) patients are eligible for a pAVF with the same timing criteria as for sAVF creation. 3
Is body habitus a limiting factor?
Obesity alone is not a limiting factor for pAVF creation. In fact, the venous system is often better preserved in obese patients, as superficial veins may be more difficult to palpate and cannulate, thereby avoiding injury from frequent phlebotomy or infusion. If the targeted outflow vein(s) is too deep, a staged lipectomy, transposition, or elevation procedure may be necessary (similar to sAVFs) and should be part of the access creation planning and patient discussion. 4
What additional factors should be considered for a pAVF?
Factors to consider when creating an sAVF versus pAVF include patient preference, comorbidities, vascular anatomy, skin integrity, available provider expertise, and equipment.
Does creation of a pAVF jeopardize opportunities for a future distal wrist AVF?
Importantly, the creation of a pAVF does not preclude a future ipsilateral distal radial–cephalic AVF. A wrist radial–cephalic sAVF remains the first option when feasible and when expected to be successful with prompt maturation. The decision to create a pAVF versus an sAVF should be individualized by discussing patient expectations and preferences while considering individual provider outcomes with each technique.
Vascular eligibility
What should the patient examination include?
All patients preparing to undergo AV access creation should have a history taken for use of peripherally inserted central catheter (PICC) lines, cardiac rhythm devices, and upper extremity surgery. Physical examination should include a modified Allen test to assess arterial supply to the hand and palmar arch(s), bilateral upper extremity blood pressure measurements, signs of prior AV access surgery, clinical findings of venous hypertension such as the presence of collateral veins, and skin irregularities (areas of thin/aging skin, keloid scars, etc.).
Baseline vascular criteria
An eligible pAVF patient has a proximal radial or ulnar artery ⩾2.0 mm in diameter with a concomitant patent perforating vein ⩾2.0 mm in diameter in continuity with the upper extremity cephalic and basilic veins. Arteries with dense transmural calcification should be avoided, while compressible arteries with mild to moderate intimal and medial calcification may be considered for pAVF inflow.
What are the potential sites for pAVF creation?
The pAVF configuration depends on both the vascular suitability and the technology being used for pAVF creation. pAVFs are created between an artery and a deep adjacent vein providing flow through the perforating vein into the superficial veins. The WavelinQ device is approved to establish a pAVF at the proximal radial or ulnar artery using venous and brachial artery catheters, while the Ellipsys device creates a pAVF at the proximal radial artery using a single venous entry catheter.1,2 The venous outflow cannulation target of these pAVFs is described below.
Draining and outflow veins
There are typically three veins (cephalic, basilica, and one of the paired brachial veins) which become the outflow for pAVFs and develop into a functional AVF. The order of preference for venous outflow depends on individual anatomy. The cephalic vein, the preferred option when available, requires a secondary procedure only when too deep for cannulation, while the basilic and brachial veins will typically require later staged elevation or transposition.
What percentage of patients have eligible anatomy for a pAVF?
Based on pivotal trial reports, 72%–75% of patients had suitable anatomy for pAVF creation.1,2 A reasonable amount of expertise and training is needed to visualize the perforator veins and their outflow, as well as diameter and vessel locations using duplex ultrasound. Ultrasound vessel mapping is recommended for all initial pAVF evaluations. Some practitioners may obtain a venogram in selected patients with a tourniquet applied at the level of the axilla to visualize forearm outflow and the perforator veins, then imaging the draining and central veins. The WavelinQ device uses fluoroscopy and the Ellipsys uses ultrasound for pAVF imaging.
What about patients with complex vasculature?
Patients with either a distal ulnar or radial artery occlusion (not both) are often good candidates for a proximal radial or proximal ulnar pAVF when clinical and objective evidence demonstrates adequate arterial flow into the palmar arch. For example, individuals with a distal occlusion of the radial artery are good candidates for a proximal radial artery AVF, leaving the intact ulnar artery to supply interrupted flow distally into the palmar arch. Even those patients who have had a radial artery harvest for coronary artery bypass grafting may have the proximal radial artery intact with continued flow through the recurrent radial artery into the forearm, and an sAVF or pAVF using the proximal radial artery might be feasible. 5
Patient education
How does a pAVF differ from an sAVF?
A pAVF is created percutaneously using a needle and special device, rather than surgically, so it lacks a traditional surgical scar and may not be easily recognized by care providers. Thus, the pAVF outflow veins could inadvertently be injured with phlebotomy, blood pressure cuff inflation, or IV needle insertion. Therefore, patient and supporter education must focus on protecting the pAVF; this is best achieved during informed decision-making before creation and reinforced at the time of pAVF creation by the physician and supporting dialysis access care team. Medical alert bracelets indicating pAVF presence are also helpful for patients with communication difficulties or where English is not their first language.
How can the patient take care of their access site?
As with any access, a patient must avoid inadvertent injury to the pAVF. First, the proceduralist can provide both documentation (including a diagram indicating the vessels used and location) and proceduralist contact information. Prior to cannulation, an ultrasound and a photo of the arm with the outflow cannulation zone clearly marked can be taken. These materials can be saved on the patient’s phone and sent to the managing nephrologist, dialysis unit, and other providers. Other methods are similar to sAVF protection, including the use of patient wrist bands stating “no venipuncture, IV or BP” and so on. 3
The patient should be instructed on care of the access arm, including washing it daily with soap and warm water and before each dialysis treatment, avoiding phlebotomy or blood pressure measurements, and checking it daily to ensure it is working normally and has blood flow (One-Minute Access Check). 6
Can a patient with a pAVF self-cannulate?
The patient should be informed and offered the option for self-cannulation by the outpatient dialysis facility. Therefore, pre-procedure planning should include every attempt to place the pAVF in the non-dominant arm, allowing the dominant arm to perform the cannulation. There are several advantages to self-cannulation, including reduced risk of cannulation injury from multiple dialysis personnel, control over infection risk, and ensuring proper cannulation and site rotation. Patients can start with small steps in the cannulation procedure, learn at their own pace, and master as much of the procedure as they can.
pAVF maturation assessment
How long does it take for a pAVF to mature?
Following creation of a pAVF, the typical time to physiologic maturation is 6–10 weeks. If pAVF physiologic maturation is achieved at 4 weeks, it is reasonable to attempt cannulation sooner, depending on individual dialysis unit expertise.
How is pAVF maturation defined?
Physiologic maturation is defined as a blood flow volume (Qa) in the brachial artery of >500 mL/min and a cannulatable vein diameter of >5 mm; 7 a diameter of >4 mm may be acceptable if the vein is palpably superficial or there is ultrasound-guided cannulation available at the dialysis facility. 2
How is pAVF maturation assessed?
Physiologic maturation is assessed with ultrasound and physical examination. An ultrasound brachial artery Qa measurement may be obtained at 1 week to assess patency of the pAVF. A second ultrasound may be obtained at 4 weeks to assess physiologic maturation—to assess brachial artery and outflow vein Qa, and superficial outflow vein diameter, as pAVFs often have a bifurcated outflow. Deep veins (brachial) should be evaluated for excessive shunting to a non-targeted outflow vein.
Physical examination is a crucial component of the maturation assessment and should be performed at each follow-up visit post-creation. It may be performed monthly if the patient is pre-ESKD or more often when dialysis initiation is indicated and should include visual examination of the outflow veins that will be used for cannulation. By palpation, the veins should feel full without a tourniquet. A tourniquet should be applied to determine which outflow veins augment to select potential cannulation sites.
What ultrasound parameters should be expected at week 1 in a pAVF?
If the brachial artery Qb is >500 mL/min 1 week following pAVF creation, physiologic maturation is likely to occur. If the Qb is <500 mL/min, a 2-week post-procedure evaluation is indicated. The proper timing for intervention with balloon angioplasty for non-maturation differs between the two devices, and the interventionalist should be aware of the appropriate recommendations.
What ultrasound parameters should be expected by week 4 in pAVFs?
At 4 weeks following pAVF creation, brachial artery Qa should be >500 mL/min; if it is <500 mL/min, a fistulogram, often from a distal arterial approach, should be performed to evaluate the arterial anastomosis and juxta-anastomotic segment with the intention to treat if a high-grade stenosis is present.
If brachial artery Qa is >500 mL/min but blood flow volume is inadequate in the outflow veins, redirecting the flow into the superficial veins should be considered. If needed, coil embolization of a competing brachial vein can be performed to redirect flow into the superficial circulation. Coiling, ligation, or banding of the median cubital vein to favor flow into the cephalic vein may be considered, but there is no evidence to date to support its impact on long-term functionality and durability of a pAVF.
What ultrasound parameters indicate that the pAVF has reached physiologic maturation?
The benchmark flows needed to support sustained dialysis in the ipsilateral brachial artery are ⩾800 and ⩾500 mL/min in the cannulation vein segment(s).1,2 If Qa is >800 mL/min in the brachial artery and a cannulatable outflow vein diameter of >5 mm, the outflow veins should be marked with indelible ink to aid in the first few cannulations and the pAVF should be cannulated using a tourniquet. If the pAVF can sustain a dialysis blood pump speed (Qb) of 400–450 mL/min with two needles, the fistula is considered mature for typical North American dialysis prescriptions. The dialysis prescription should be assessed to accommodate the Qb setting that is achievable within safe arterial and venous pressure limits. In other areas of the world or other dialysis techniques (e.g. long nocturnal dialysis) that may only require Qb < 300, a pAVF outflow vein Qa of 350 mL/min may be acceptable.
What additional procedures may be necessary to promote pAVF use?
Balloon angioplasty or side branch ligation may be required for pAVF maturation, highlighting the need for excellent multidisciplinary communication among team members, as the creating proceduralist may be different than the one maintaining or salvaging the pAVF. As with other vascular access procedures, all pAVF procedures are done after determining that the arterial supply to the hand is adequate, and hand ischemia is not anticipated.
Dialysis team education for pAVF cannulation
The goal of the two available pAVF devices is to create vascular access flow through the perforating (deep communicating) vein in the mid-proximal forearm into the superficial venous system (Figure 1). The resulting proximal radial artery or ulnar artery AVFs have similar configurations to those used by many surgeons for several decades.1,5,8,9 Both devices create pAVFs that can reliably provide 800–1000 mL/min of brachial artery Qa 13 months after creation.1,5,10 The time to two-needle cannulation was also similar for pAVFs created by both devices in the initial trials (100–111 days).1,2 Cannulation education for pAVFs at the point of care will be a key element for success. Centers with availability of ultrasound for selected cannulations and expert cannulation teams may have shorter time to pAVF use and catheter removal, although many patients with pAVFs achieved early cannulations and catheter removals without the aid of ultrasound.
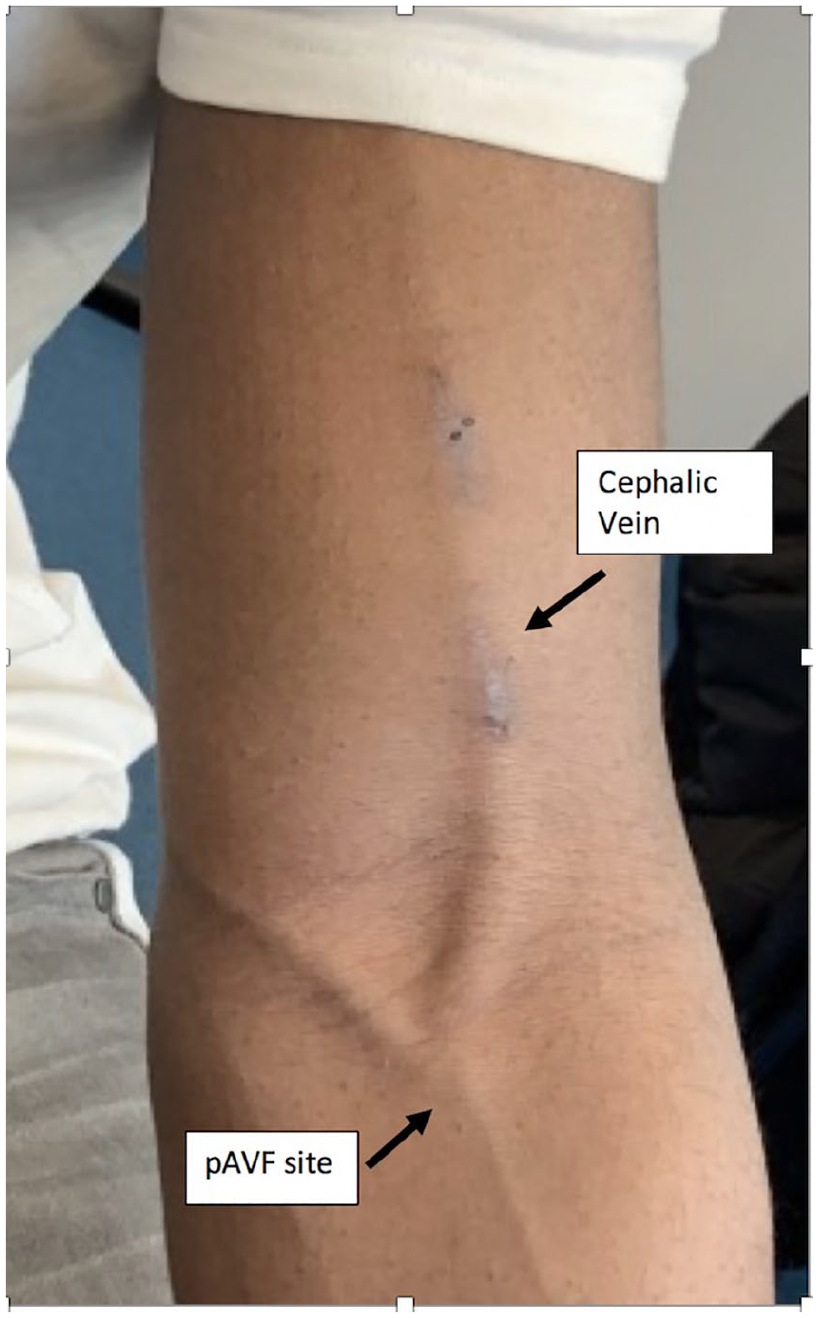
Ellipsys percutaneous arteriovenous fistula. Note the cephalic and median cubital veins available for cannulation. Flow volume is 946 mL/min and cephalic vein diameter is 6.8 mm.
What should happen prior to the first pAVF cannulation?
The physician creating the pAVF should schedule patient follow-up 1–2 weeks after the procedure to evaluate the patient and assess the pAVF diameter for outflow size and flow volume to determine pAVF progress toward maturation. A goal of initial cannulation within 6–10 weeks of creation is reasonable in properly selected patients for pAVFs; if the pAVF is not progressing toward maturation, then an ultrasound (if not already done) ± fistulogram and intervention as indicated is recommended.
What role does the interventionalist have in promoting successful cannulation?
It is recommended that a “cannulation map” be made prior to cannulation, detailing cannulation zones, blood flow direction, vessel depth from the skin to determine the needle angle of entry, and cannulation zone length for successful needle placement. This can be easily created with ultrasound imaging. If a specific needle length is recommended (3/5-inch needle for shallow vessel, 1 inch for typical depth vessel, or 1¼ inch for deep vessel), it should be highlighted on the cannulation map, and the map should be updated if any interventions impact the pAVF. This map is a critical part of the patient’s medical record and should be accessible to anyone needing to cannulate the pAVF should the patient be hospitalized.
Prior to cannulation, the targeted outflow cannulation sites should be marked, ideally by ultrasound (Figure 2), and the cannulation plan should be reviewed by both the patient and relevant dialysis unit staff, for example, a head nurse and vascular access coordinator. Photographs of the pAVF marked with the cannulation zones should be found in the patient’s medical record and used by an expert cannulator assigned for the first few cannulations, as similarly recommended for all vascular access patients.
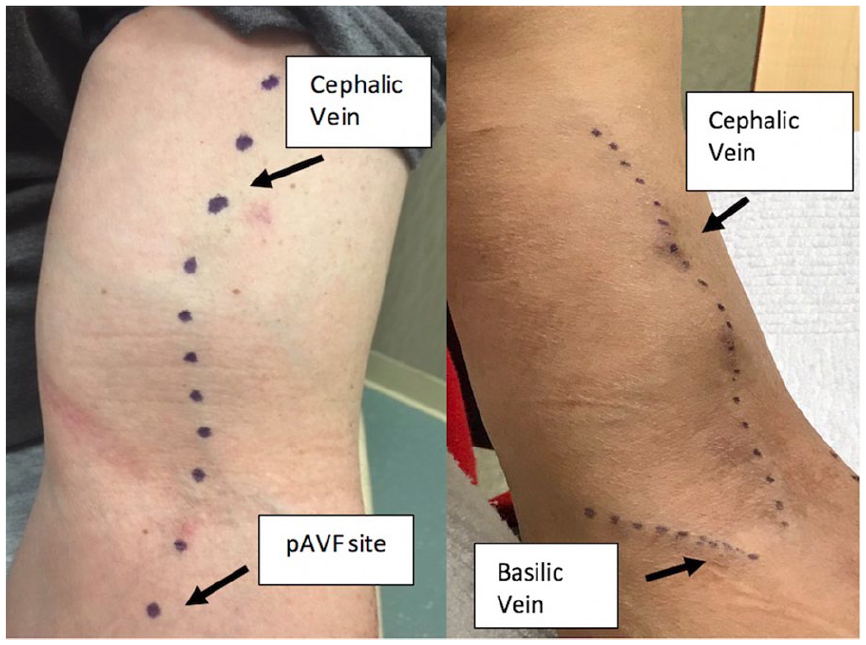
Percutaneous AVF and marking by ultrasound for cannulation.
The cannulation technique of a pAVF is similar to an sAVF
It is important to ensure that the staff members are familiar with their individual dialysis unit cannulation policy, as pAVF cannulation builds on existing techniques. A tourniquet should be used, regardless of the size or appearance of vessel, as it helps to engorge, visualize, palpate, and stabilize the pAVF. The perforating vein joins the superficial veins below the elbow crease, and since there is no surgical scar here, this segment frequently offers a reliable pAVF cannulation segment.
Ultrasound availability and use for the first cannulation has proven to be valuable in select patients, particularly in obese individuals.11–13
How is the cannulation site selected?
One must be mindful of patient comfort during a dialysis session and consider arm positioning (e.g. patient works on computer and knits) when selecting suitable cannulation sites. The most common suitable vein will be the upper arm cephalic, although significant outflow may develop into the basilic system. Sites closer to the elbow crease may be cannulated with the needle in a retrograde position to minimize needle movement with arm motion.
If cannulation of the median cubital vein is difficult or additional flow through the cephalic vein is needed for reliable cannulation, then banding, ligation, or coil occlusion of the median cubital vein may be necessary, directing all outflow into the cephalic system. These interventions, if needed, parallel the same maturation processes often required for establishing a functional sAVF. Occasionally, the patient’s cephalic vein is inadequate, and all flow is into the basilic or brachial vein. A staged elevation or transposition will typically be needed for those individuals, just as with sAVFs.
What is the recommended position for the patient and cannulator?
We recommend that the patient’s arm be extended in a comfortable position on the chairside table, resting on a pad or pillow, and that the cannulator be seated at the same level as the pAVF. The seated position stabilizes the cannulator, prevents bending over the pAVF, and allows to better control the forward pressure when puncturing the skin, tissue, and vessel with the needle tip. A new cannulator commonly applies excessive pressure to the needle wings, and thus the cutting bevel, and can easily enter the vessel and depress the vessel leading to a backwall puncture and infiltration. It is recommended that the cannulator remains seated until the needles are fully stabilized with tape as per facility policy and procedure.
What needle size and pump speed should be used initially?
We suggest that the initial dialysis cannulation protocol for sAVFs should be followed for pAVFs, including using a single, smaller (17 Ga) needle for the arterial limb and returning through the catheter (if present) and progressing to higher pump speeds and dual-needle cannulation as tolerated.
Providers and patients using a catheter should be educated in advance of a possible decline in dialysis adequacy with pAVF use, since a lower pump speed may be required (~350 mL/min) until optimal pAVF flow rates are achieved (similar to sAVFs). Of note, if two well-developed outflow veins develop, for example, median cubital/basilic and cephalic, cannulation of these may result in improved dialysis adequacy, given the lack of recirculation in this setting.
Which cannulation technique is recommended for pAVFs?
Rope ladder cannulation will be appropriate for most patients, with buttonhole cannulation used in selected patients, per the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines. Expert cannulators note that a pAVF feels softer as the needle tip enters the vessel and that blood flashback is often less vigorous than an upper arm sAVF, and thus, wet needle cannulation may be helpful.
With tourniquet in place, cannulation should proceed with light pressure to avoid vessel collapse and backwall injury. Vessel depth is used to determine the needle angle, and typically, a 20–35° angle is used for pAVF cannulation. The cannulation zone length must also be clearly identified. The standard metal fistula needles come in 1-inch or 1¼-inch lengths, while a shorter, 3/5-inch metal fistula needle may be beneficial. The needle direction for the venous needle should always point toward the venous return to the central system. The arterial needle can be pointed toward the inflow (retrograde) or toward the venous return (antegrade), depending on the cannulation zone length and unit-specific policy/procedure for cannulation. Outside the United States, plastic cannulae are commonly used to cannulate pAVFs, especially if the cannulation zone crosses the elbow crease, where there is increased risk of infiltration related to arm movement.13–15
What parameters are important to monitor during dialysis?
The arterial and venous pressures should be monitored in these moderate flow pAVFs, with particular attention to the arterial pressure, as it may become too negative to support a standard blood pump speed.
pAVF monitoring and surveillance
How should a pAVF be monitored?
Access monitoring utilizing the standard physical examination or the One-Minute Check is recommended per facility policy and procedure for all pAVFs. 6 The augmentation test may vary if the pAVF outflow has significant side branches or several outflow segments. Further, in the setting of multiple egress vessels, the arm elevation maneuver with resultant AVF collapses to ascertain draining vein stenosis does not exclude a downstream stenosis in one segment. This is may be problematic when the main draining vein is being cannulated, as typical signs of an outflow vein stenosis are absent, although there might be a failure to deliver adequate dialysis (i.e. high recirculation).
When an abnormality, such as high pressure, low flows, recirculation, and/or difficult cannulation, is detected, a prompt referral should occur for evaluation by the treating physician, ensuring that communication occur between all members of the multidisciplinary team.
What is the best way to conduct flow surveillance of a pAVF?
The presence of a pAVF must be clearly delineated in the patient’s medical record for accuracy in reporting and tracking. Ultrasound measurement of Qa using brachial artery flow is a reliable and reproducible surrogate for AVF flow and has become a common adjunct for evaluation and treatment decisions, but this is not readily available in the dialysis unit.
Both the Transonic Ultrasound Dilution and the Fresenius Online Clearance methods require reversal of the bloodlines to the needle connection point to create reversed flow within the AV access. If the pAVF has branch flow and both needles are not in the same vessel, the Qa measurement cannot be properly determined and will not be accurate. The Vasc-Alert’s Vascular Access Pressure Ratio and other Transonic measurements including delivered flow, recirculation, or cardiac output are not impacted by the branch flow needle placement.
Conclusion
The pAVF is a vascular access option that may be an appropriate part of a patient’s ESKD Life-Plan while on dialysis. 3 pAVFs offer several potential advantages, including (1) reduced delays in AVF creation and pre-operative procedures by expanding the number of AVF providers to include interventionalists; 16 (2) providing more anatomical options for AVF creation, thereby increasing the patient’s vascular access capital; and (3) increased patient choice of procedures for those who prefer to avoid an open surgical procedure for AVF creation, with comparable short-term outcomes. Longer term outcomes will add to the body of knowledge, and a team approach will support this innovative vascular access creation procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.W. is the speaker for BD and Avenu Medical; A.C.A. is the speaker for BD; S.B. is the consultant for BD and WL Gore; D.B.-M. is the employee of Transonic; R.I.C. is the stockholder in Avenu Medical; J.E.H. is the Avenu Medical stockholder, consultant, intellectual property, royalty, and consultant medtronic; W.C.J. is the stockholder and consultant for Avenu Medical and speaker for Davita and WL Gore; T.F.L. is the patient advocate in Avenu Medical; C.E.L. is the consultant for BD; and D.R. is the consultant for BD and WL Gore. K.A., A.K.A., and V.D.N. report no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.