
Abstract
Aim:
In modern healthcare there is increased focus on optimizing efficiency for every treatment or performed procedure, of which reduction of costs is an important part. With this study, authors aimed to calculate the cost of peripheral intravenous cannulation including all components that influence its price.
Methods:
This observational cost-utilization study was conducted between May and October 2016. Hospitalized adults were included in this study, who received usual care. Peripheral intravenous cannulation was carried out according to current hospital protocols, based on international standards for peripheral intravenous catheter insertion. Device costs were assumed equal to the number of attempts multiplied by the fixed supply costs and applicable costs for additional attempts, whereas personnel costs for both nurses and physicians were based on their hourly salary.
Results:
A total of 1512 patients were included in this study, with a mean of 1.37 (±0.77) attempts and a mean time of 3.5 (±2.7) min were needed for a successful catheter insertion. Adjusted mean costs for peripheral intravenous cannulation were estimated to be €11.67 for each patient, but costs increase as the number of attempts for successful cannulation increases. The cost for patients with a successful first attempt was lower, at approximately €9.32 but increased markedly to €65.34 when five attempts were needed.
Conclusion:
Prevention of multiple attempts may lower the costs, and furthermore, additional technologies applied by nurses to individual patients based on predicted difficult intravenous access will make the application of these additional technologies, in turn, more efficient.
Introduction
In modern healthcare there is increased focus on improving clinical outcomes, improving safety, maximizing patient satisfaction and optimizing efficiency for every treatment or performed procedure, of which reduction of costs is an important part. 1 This applies to all activities, including routine procedures such as peripheral intravenous cannulation (PIVC). PIVC is routinely used for short-term intravenous administration of fluids, medications, blood products and contrast media, with an estimated prevalence of 80% in hospitalized patients.2–4
Costs related to PIVC vary considerably, depending on several factors, including the type of catheter inserted and the type and extent of supportive technology employed. 5 Previous studies have found that the average cost for a straightforward insertion of a short peripheral intravenous catheter, which is successful on the first attempt, ranges from €25 to €35.5–7 Nonetheless, cannulation costs consist of different components, including costs for equipment, salary of clinicians, and the number of attempts needed for success. Logically, personnel time is the largest cost factor in establishing successful intravenous access, especially when personnel time increases. 1
In recent literature, several studies were published describing the costs of PIVC, mostly related to the price of catheter replacement due to complications.5–9 To add to this, total cannulation costs were normally based on the price of used devices and a clinician’s monthly salary, of which nursing salary is less expensive than physicians’. 8 No distinction was made between cannulation costs with respect to the number of attempts needed for successful cannulation, while it seems obvious that more time is needed if multiple attempts are necessary. Consequently, extended time needed to obtain intravenous access will result in longer staffing time per patient, in which costs will increase further when physicians are called to gain vascular access after previous failed attempts.
With this study, authors aimed to calculate the cost of PIVC including all components that influence its price. For this, it is assumed that PIVC costs are based on the number of attempts needed for successful intravenous access, time needed for each attempt to obtain successful vascular access, observed and measured staff time and salary for creating venous access, and device costs.
Methods
Design
This observational cost-utilization study was conducted at the Catharina Hospital (Eindhoven, The Netherlands), which is a 700-bed tertiary teaching hospital. Patient enrolment occurred between May and October 2016 in the preoperative holding area of the theatre complex. Anaesthesiologists and nurse anaesthetists at all levels of experience were eligible, on a voluntary basis, to participate in this study. The current study is based on a previous dataset and was set up as follow-up analyses. 3
Participants
Hospitalized adults were eligible to participate in this study if scheduled for a surgical procedure, regardless of their American Society of Anesthesiology (ASA) classification, demographics, and medical history. Patients were excluded if they did not understand or answer the questionnaire (due to physical or communicational disorders), were unresponsive or when an intravenous access had already been gained. Patients received usual care throughout the study.
Procedure of intravenous cannulation
PIVC was carried out according to current hospital protocols, based on international standards for PIVC.10,11 Before cannulation, a tourniquet was secured around the chosen arm to ensure dilation of the veins, at least 10 centimetres proximal to the antecubital fossa. 12 The access sites were decontaminated with 2% chlorhexidine gluconate in 70% alcohol.10,11 Cannulation was performed on the upper extremity, in which short intravenous catheters sized 14–22 gauge having a length of less or equal to 7.5 centimetres (Venflon Pro Safety; BD Infusion Therapy AB, Helsingborg, Sweden) were inserted. 13 Cannulation was performed by nurse anaesthetists, as per routine. According to hospital protocols and international standards, another clinician was required to perform cannulation after two failed attempts by one clinician.11,13
Measurements
Besides patient demographics (sex, age, body mass index (BMI), and ASA classification), the clinician performing PIVC collected procedure-related data (size of the catheter, site of cannulation, and whether or not the catheter was inserted in the dominant side), the number of attempts needed to successfully insert an intravenous catheter, time needed for successful cannulation and the clinician performing PIVC. To minimize bias and to maximize validity of the results, both clinicians and patients were not aware of the outcome of interest. An attempt was defined as one percutaneous needle puncture, regardless of the amount of subcutaneous exploration from a single puncture site.10–12 After a failed attempt, a new attempt was considered as any change in localizing a vein, followed by a new percutaneous puncture. 10 After each puncture, the clinician checked and registered whether the attempt was successful or not. PIVC was defined successful if blood returned in the catheter and/or a saline flush could be injected without compromising the vein or without signs of subcutaneous infiltration. 10 Time needed for PIVC was registered in minutes, from applying the tourniquet until the catheter was inserted successfully, including time needed for preparations (e.g. selection of devices and supply, or putting on gloves) and confirming a patient’s consent for intravenous therapy.
Healthcare resource costs
Device costs were assumed equal to the number of attempts multiplied by the fixed supply costs and applicable costs for additional attempts, whereas personnel costs for both nurses and physicians were based on their hourly salary, including surcharges. Based on these data, costs of PIVC can be calculated according to the following formula:
PIVC costs = device costs + personnel costs, whereby
Device costs = fixed supply costs + (catheter costs × number of additional attempts) and
Personnel costs = surcharges + salary per hour × time to successful cannulation.
A standardized list of equipment for PIVC was formulated according to hospital protocols, based on international guidelines. 10 Fixed supply costs needed for PIVC included the costs for cannulation and access devices, needle-free caps, catheter hubs, administration ports integral to an administration set, a fluid administration set that will be connected to the intravenous catheter, gauzes, disinfection, tape and transparent film dressings to stabilize the peripheral catheter. For hospitalized adults, fixed supply costs were estimated at €5 for PIVC. The price of a short peripheral intravenous catheter was €2.50 for the first attempt at creating intravenous access. Each additional attempt added €2.50 for the new intravenous catheter. Data regarding device costs were obtained from the hospital purchasing department.
Calculation of personnel salary, for both nurses and physicians, were based on salaries as determined in the Collective Labour Agreement for Hospitals in the Netherlands and calculated following data from the Manual of Healthcare Costs Investigation and the Guideline for Conducting Economic Evaluations in Healthcare as published on the webpage of the Dutch Government.14,15 The mean salaries for nurse anaesthetists was €34 per hour (ranging from €28 per hour up to €39 per hour). For physicians, the mean salary per hour was €110 per hour (ranging from €58 to €164 per hour). Represented salaries depended on level of experience.
Costs for add-on devices that are used on conjunction with the administration set and can be connected to the infusion system, including three-way taps or stopcocks, ramping ‘traffic light’ systems, extension sets, blind hub caps, injectable caps or connectors, needleless systems and filters, were not included in the cost calculation, because these devices were not used in the standardized procedure of PIVC. 13
Data analyses
The Kolmogorov–Smirnov test assessed the normality assumption for continuous variables. Continuous variables with a normal distribution were expressed as the mean (standard deviation), while those without a normal distribution were expressed as the median with their minimum and maximum value. Discrete variables were expressed as frequencies with percentages. No statistical analyses were performed; data were described and shown numerically or graphically.
Ethical considerations
The Medical research Ethics Committees United (MEC-U, Nieuwegein, the Netherlands) reviewed the study protocol (ref: 2015-21). Written informed consent was obtained from all participants before inclusion.
Results
A total of 1512 patients were included in this study, of which 680 (45%) were male. In the studied cohort, 363 (24%) patients were classified as ASA physical state 1, whereas 711 (47%), 408 (27%) and 3 (2%) were classified as being ASA 2, 3 and 4 respectively. The mean age of the studied cohort was 55 (±17) years, and the mean BMI was 28 (±8). All patients were in a stable hemodynamic condition.
A mean of 1.37 (±0.77) attempts was needed for a successful PIVC, with a maximum of eight attempts in two patients. Intravenous cannulation was successful on the first attempt in 77% of patients, with a total number of 2064 punctures performed throughout the study cohort. Data regarding PIVC are represented in Table 1.
Baseline and demographic characteristics.
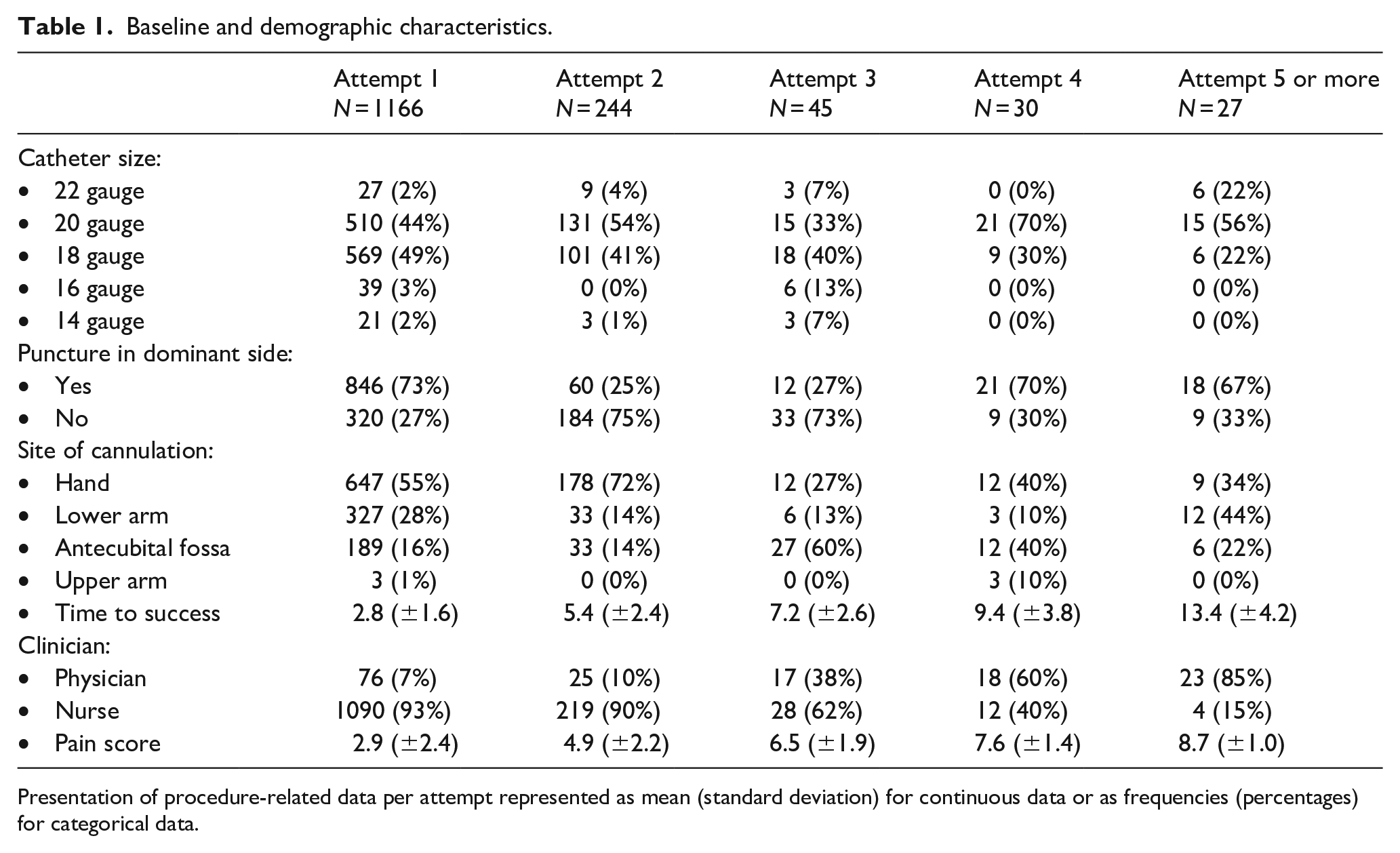
Presentation of procedure-related data per attempt represented as mean (standard deviation) for continuous data or as frequencies (percentages) for categorical data.
A mean time of 3.5 (±2.7) min was needed for a successful PIVC across the sample of patients, but increased up to 19.1 min when eight attempts were needed for successful cannulation. Instead of nurses performing PIVC, physician participation increased if the number of failed attempts increased. While successful PIVC on the first attempt was performed by nurses in 93% of patients, when five or more attempts were needed it was physicians who performed the procedure in 85% of patients.
Total costs for PIVC increased as the number of attempts needed for successful cannulation increased. The costs for PIVC were estimated to be €9.32 with a successful first attempt, but increased to €65.34 when five attempts were needed, based on clinician deployment (Figure 1). With a mean of 1.37 attempts and mean of 3.5 min per patient needed to obtain intravenous access, costs were estimated to be €11.67 for each patient. As represented in Table 2, the cost for PIVC increased as the deployment of a physician increased (Figure 2). The lowest cost for PIVC was registered if cannulation was successful on the first attempt, as performed by a nurse with the lowest hourly salary (€8.79). On the contrary, the highest cost for PIVC was registered if cannulation was successful on the fifth attempt and performed by a physician with the highest hourly salary (€121.78). Where eight attempts were needed for successful cannulation, the estimated cost was €163.88.
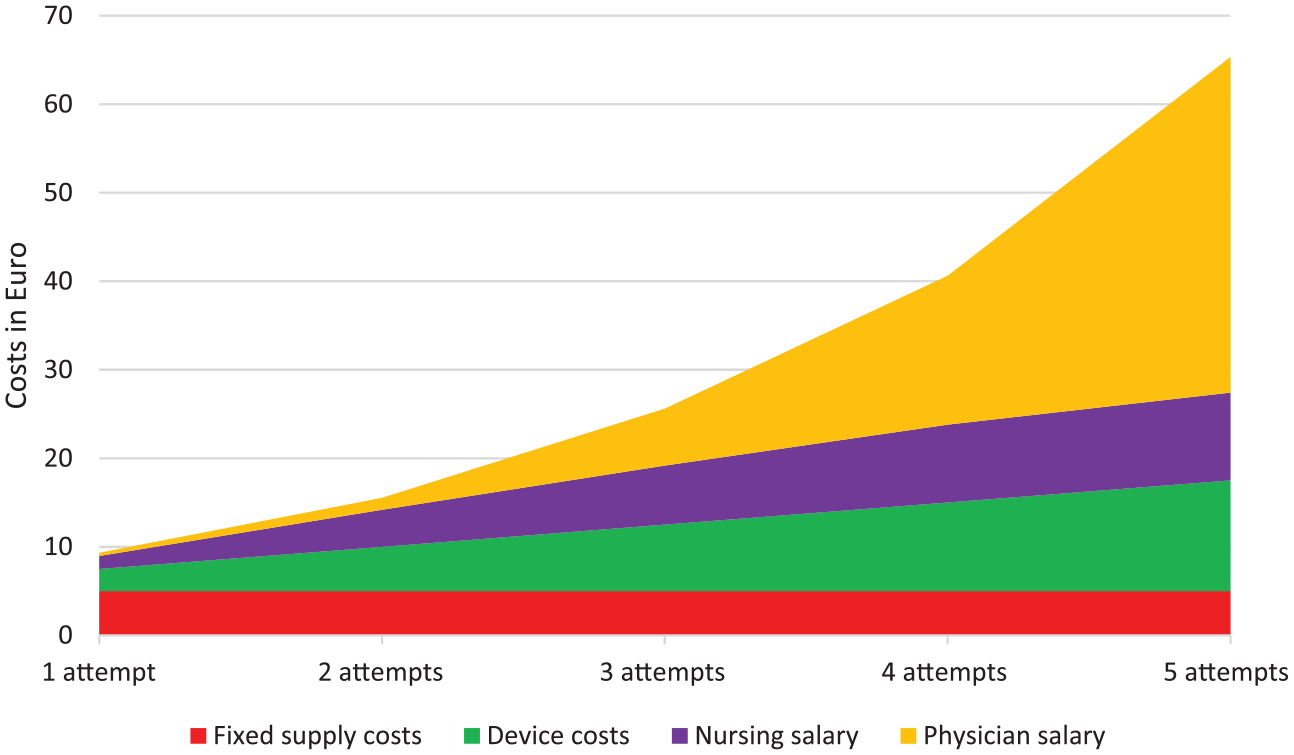
Exploration of costs for each attempt.
Costs as calculated for each attempt.

Exploration of the elements that determine the total costs per attempt of peripheral intravenous cannulation. Clinicians’ costs were calculated based on the percentage of intravenous cannulations as performed by the depending clinician, multiplied by the time needed to successful cannulation and the salary per hour.
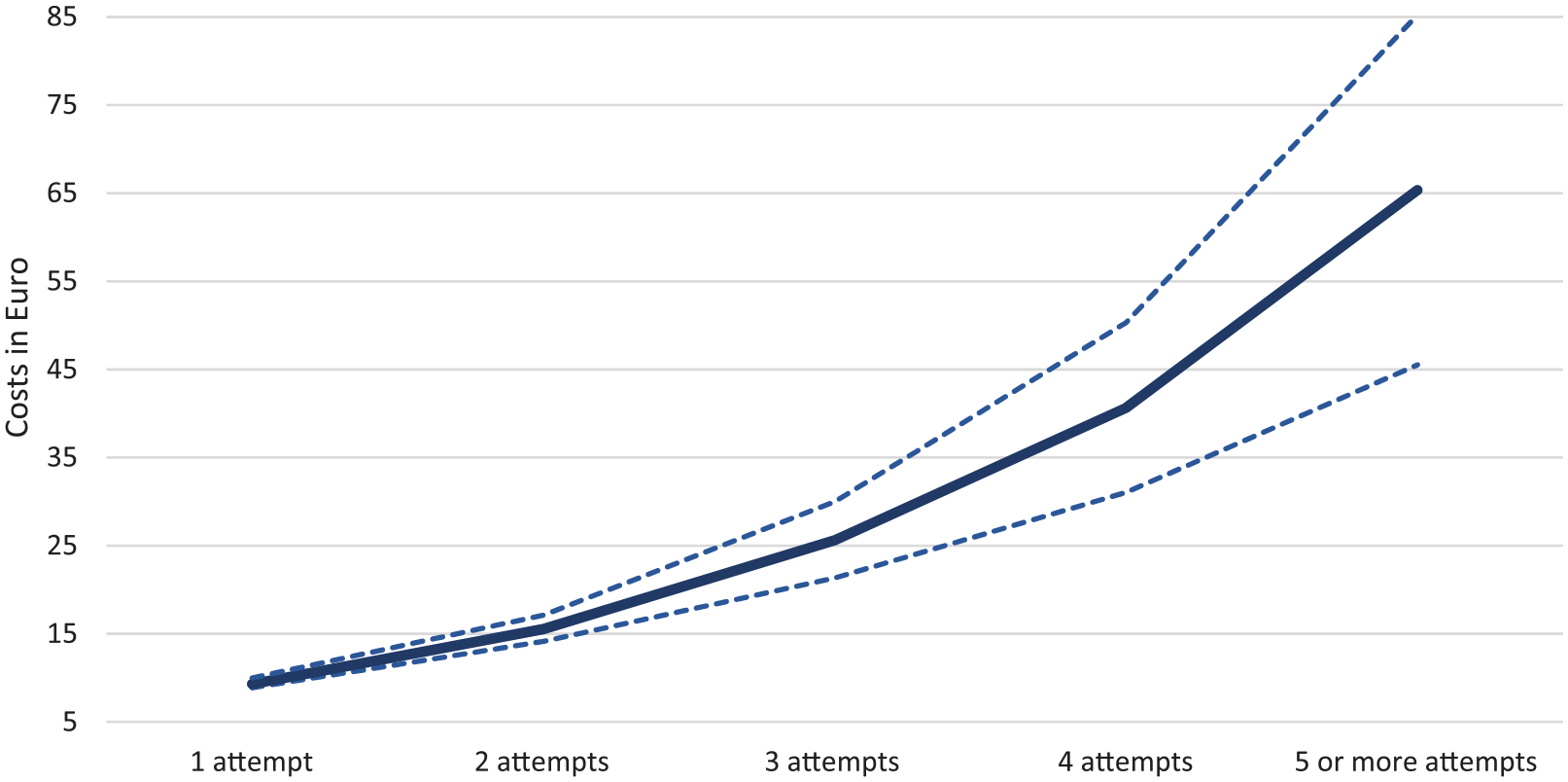
Graphical presentation of cannulation costs.
Discussion
The current study aimed to determine the cost of PIVC in adult patients, of which the total cost is based on the number of attempts needed for successful intravenous access, time needed for each attempt until vascular access is obtained successfully, observed and measured staff time and salary for creating venous access, and device costs. The adjusted mean cost was estimated to be €11.67 per patient for intravenous cannulation, assuming an average 1.37 attempts and 3.5 min. The cost for patients with a successful first attempt was lower, at approximately €9.32 but increased markedly to €65.34 when five attempts were needed. To continue, the cost of PIVC increased as the number of cannulation attempts increased.
Despite the relatively low cost of PIVC when compared to many other invasive procedures in daily healthcare this cost is unavoidable, and is therefore a substantial expense. To highlight the broader financial impact of PIVC for a 700-bed tertiary hospital with admissions of 25,000 patients per year (as is the case in the hospital in which the current study was performed), the annualized cost is estimated to be €291,750 when 1.37 attempts and 3.5 min are needed per patient. When considering our data, 77% of patients needed one attempt to successful cannulation, resulting in an annualized cost of €179,410 for a hospital with admissions of 25,000 patients per year. On the other hand, our findings predict that 2% of patients will require five or more attempts for successful cannulation at a cost of €65.34 per patient, or a total annual cost of €32,670 for these patients. However, estimated costs are conservative and vary greatly in different hospitals depending on acuity of patients and the level of experience of clinicians. 9 Besides being time consuming to medical professionals and expensive for the hospital, failed attempts create a painful, uncomfortable and stressful experience for an already anxious patient, and are associated with additional risks as nerve damage, paresthesia, hematoma and arterial puncture. 16 In the long-term, particularly if multiple attempts are needed and complications influence further treatment, failed cannulation affects patients’ mobility and social life. 16
Economic evaluations and cost-utility studies have been widely applied in health policy to inform resource allocation decisions. 17 Establishing intravenous access is part of routine care and a requirement prior to treatment, but costs for PIVC increase with an increased number of attempts needed to create vascular access. The application of additional technology to improve vessel identification, such as ultrasound or electrical stimulation to create venous dilation, has been shown to be effective in improving first attempt success rates.18–21 Nonetheless, efficiency and efficacy is not automatically guaranteed by simply applying technology, and may not in the first instance reduce procedure-related costs, because of the initial investment required and the time and resources needed for training healthcare providers on their use.22–24 In addition, it seems obvious that prospective selection of patients at risk of difficult intravenous access is key in reducing costs, especially considering the simple fact that additional techniques can be applied to the right patients and will be used by trained and experienced clinicians. 3 Costs associated with the deployment of additional technology, including conditions for use, were out of the scope of this study, but should be part of future research projects investigating costs related to PIVC. To add on this, recent literature suggests the use of ultrasound in patients with a known difficult intravenous access instead of exposing them to multiple attempts. 25
Costs for PIVC can be divided into device costs and costs related to the deployment of healthcare providers. Device costs are fixed components of the total cost, and a reduction in these costs is difficult to achieve. On the other hand, personnel time is the largest cost factor in establishing successful intravenous access, particularly when multiple attempts are needed for successful cannulation. 1 Moreover, nursing salary is significantly lower than a physician’s salary. Creating an effective system to maximize first attempt success in PIVC through the selection of proficient nurses, using the most optimal techniques to improve cannulation success and reduce complications, should be important from a clinical outcome and financial standpoint. 1
Limitations
Compared to clinical trials, which report the consequences of an intervention, economic evaluations require reporting for additional items, such as resource use, costs, preference-related information and cost-effectiveness results. 17 The calculated costs for PIVC vary considerably between healthcare institutions, depending on geographic and institutional factors, the type of devices inserted, and the profession and hourly salary of the clinician who is responsible for intravenous access. 5 This possibly affects the generalizability of the results of this study to other populations, healthcare settings, or even countries.
To continue, there was potential selection bias in which the most experienced clinicians might be selected in this study, especially in those patients needing multiple attempts for successful cannulation. This could have resulted in overestimated success rates or times for successful cannulation. 1
Finally, the employment of additional technologies and strategies to increase success for PIVC were not included in this study. A comprehensive and complete overview of the costs of PIVC should weigh the need for additional equipment or interventions, and its related costs. 6
Conclusion
Adjusted mean costs for PIVC were estimated to be €11.67 for each patient, but costs increase as the number of attempts for successful cannulation increases. Avoidance of these healthcare related costs is hardly possible by virtue of the fact that obtaining intravenous access is a necessary action to start many kinds of therapies. Multiple attempts are a burden for patients and expensive to the healthcare system, and preventable when state-of-the-art techniques are used. Prevention of multiple attempts may lower the costs, and furthermore, additional technologies applied by nurses to individual patients based on predicted difficult intravenous access will make the application of these additional technologies, in turn, more efficient.
Footnotes
Acknowledgements
Authors thank all nurse anaesthetists and PACU nurses for their cooperation and commitment during the collection of data.
Authors’ contributions
Fredericus HJ van Loon is the main investigator and was involved in study conception and design, generating the protocol and administrating it at the institutional review board, drafting of the manuscript, analysis and interpretation of data. Tina Leggett was involved in study conception and design, drafting of the manuscript, critical revision of the article, analysis and interpretation of data. Arthur RA Bouwman generated the protocol and administrated it at the institutional review board, and was involved in critical revision of the article. Angelique TM Dierick-van Daele helped in critical revision of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.