
Abstract
Iatrogenic arteriovenous fistula of major neck vessels is a rare complication but can occur after central venous catheterization. Symptoms can range from nothing to severe heart failure and management can be particularly complex. We report a case that we treated recently in our department.
Introduction
Iatrogenic arteriovenous fistulae of major cervical vessels are rare complications that if left untreated can lead to heart failure. Surgical and endovascular methods have been reported in the literature to treat such lesions.1 –3 We describe the case of a patient having a jugulo-subclavian fistula following central venous catheterization that was diagnosed incidentally 2 years later by a clinically marked cervical bruit.
Case report
An asymptomatic 72-year-old male patient with a previous history of cardiac surgery was referred by his primary care physician for a strong bruit over the right common carotid artery. Physical examination revealed a palpable thrill over the right clavicle. Ultrasound imaging demonstrated a high-flow (2 L/min) arteriovenous communication between the origin of the right subclavian artery and the jugular vein (Figure 1). Computed tomography angiography confirmed the above findings but excluded endovascular options due to the localization of the fistula almost at the bifurcation of the right innominate artery (Figures 2 and 3).
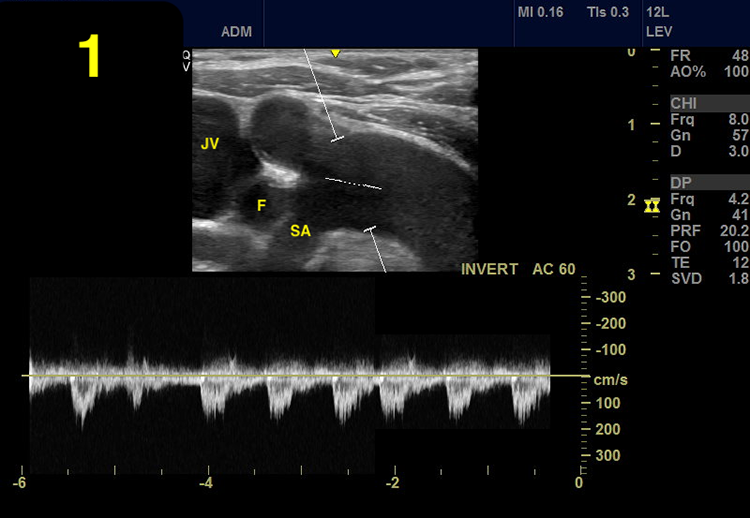
Spectral analysis Doppler ultrasound showing high-velocity low-resistance flow arteriovenous fistula between the right subclavian artery and the right jugular vein. Subclavian artery (SA), jugular vein (JV), and fistula (F) are noted.
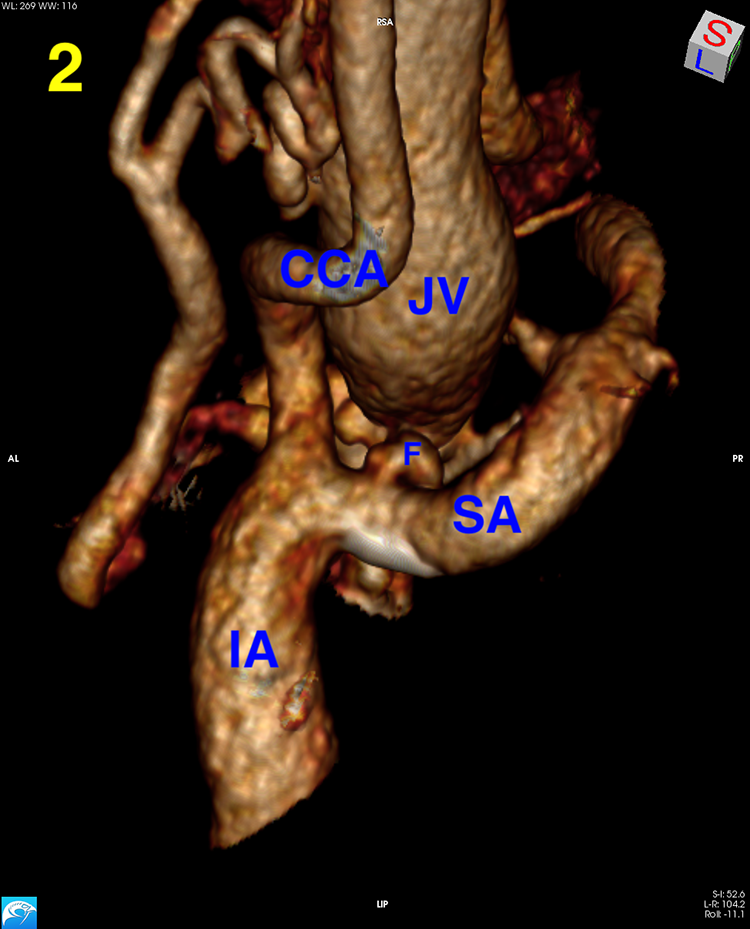
Medial view of a 3D reconstruction CT scan showing the communication between the right subclavian artery and the right jugular vein at the bifurcation of the innominate artery. JV: right internal jugular vein; IA: innominate artery; CCA: common carotid artery; SA: right subclavian artery; F: fistula.
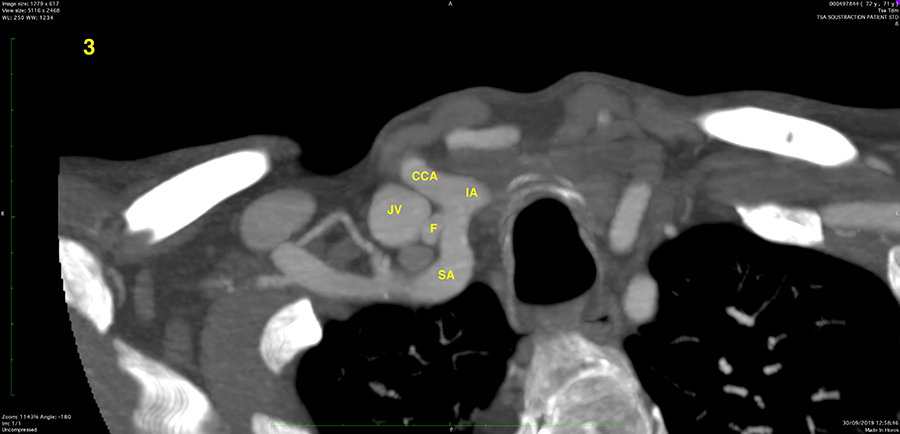
Axial CT scan view. CCA: common carotid artery; SA: right subclavian artery; JV: right jugular vein.
An elective surgical repair was decided. Under general anesthesia, and in supine position with extension and left rotation of the neck, the patient was prepped for right carotid artery approach and median sternotomy if required. We performed a supraclavicular approach of the innominate artery bifurcation. After section of the clavicular tendon of the sternocleidomastoid muscle, the right internal jugular and common carotid artery were identified, dissected, and controlled with vessel loops. Following the carotid artery proximally allowed us to control the innominate artery and identify the arteriovenous communication at the origin of the subclavian artery (Figure 4, Supplemental Video 1, 2). As the arteriovenous communication was clearly visible, we decided that no vessel cross clamping or reconstruction was necessary. A suture ligation with a 5-0 polypropylene suture was performed in both ends of the fistula. The thrill and internal jugular vein distention disappeared immediately. The total operative time was 30 min and the procedure was well tolerated. The patient was extubated in the operative room and the postoperative course was uneventful. The patient was discharged on the fourth postoperative day after adjustment of his blood pressure medication.
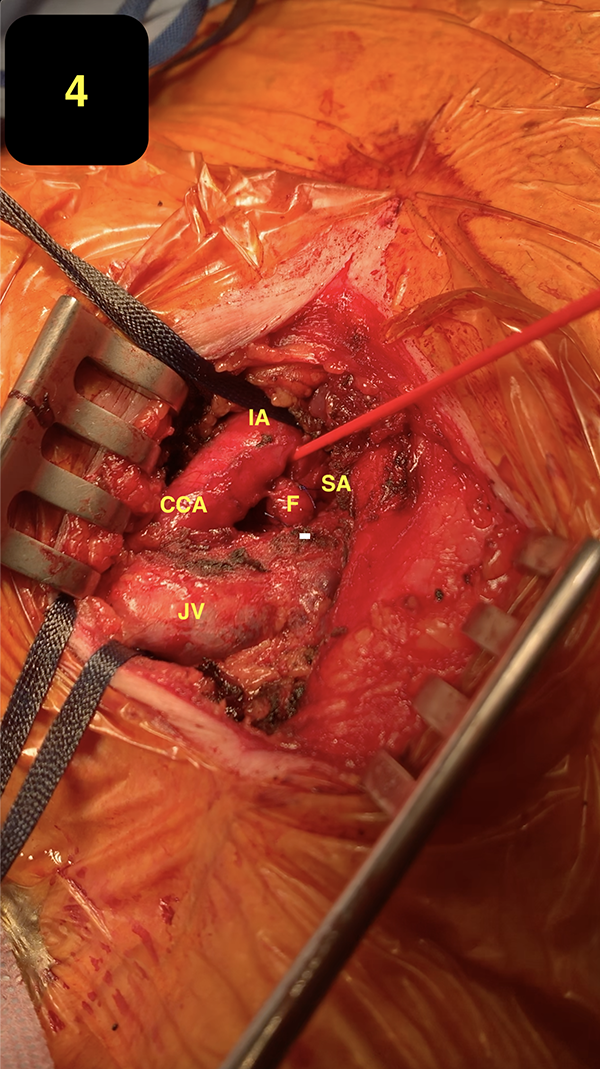
Operative view showing the innominate artery (IA), the common carotid artery (CCA), the subclavian artery (SA), the jugular vein (JV), and the fistula (F).
Discussion
Internal jugular vein catheterization is a frequently performed procedure that provides central venous access before major surgical procedures. Iatrogenic arteriovenous in this region are uncommon but may occur as a consequence of central catheter placement especially if puncture is not ultrasound guided and is blindly done using surface musculoskeletal landmarks.1,2 Of note, even in cases of ultrasound-guided placement when care is not taken for careful visualization of the needle tip during puncture, these complications may also arise. Other complications include hematoma, pseudo-aneurysm formation, active bleeding with hemorrhagic shock, and compressive manifestations, notably airway compression. These complications occur especially in case of hemostasis disorders, anticoagulant treatment, difficulty in inserting the catheter (multiple venipunctures and arterial puncture), short neck, obesity, inexperienced operator, and emergency setting.3 –5
Meticulous preoperative imaging and rigorous surgical technique is required for uneventful repair of such lesions. Two therapeutic attitudes are possible: surgical treatment and endovascular techniques (such as covered stents, vascular closure devices, tract embolization, and balloon tamponade). Surgical treatment is the more challenging option as access to deep structures requires extensive dissection of the vascular and nerve pedicles and is not always easy in a fibrotic area, with a high risk of bleeding given the multitude of high flow vessels. Endovascular treatment is considered to be the first-choice treatment because it is minimally invasive, it reduces blood loss, shortens the length of hospital stay, can be performed under local anesthesia, and does not require a potentially difficult surgical dissection. In addition, these patients are often fragile with multiple medical comorbidities and contraindication for anesthesia.
In our patient, careful preoperative imaging gave us two very important elements—first, the localization of the fistula at the origin of the subclavian artery excluded endovascular treatment, and second, surgical control of the innominate artery was possible without the need for sternotomy—even though the patient was prepped for it in case of intraoperative bleeding.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.