
Abstract
Background:
Placement of central venous access devices is a clinical procedure associated with some risk of adverse events and with a relevant cost. Careful choice of the device, appropriate insertion technique, and proper management of the device are well-known strategies commonly adopted to achieve an optimal clinical result. However, the environment where the procedure takes place may have an impact on the overall outcome in terms of safety and cost-effectiveness.
Methods:
We carried out a retrospective analysis on pediatric patients scheduled for a major neurosurgical operation, who required a central venous access device in the perioperative period. We divided the patients in two groups: in group A the central venous access device was inserted in the operating room, while in group B the central venous access device was inserted in the sedation room of our Pediatric Intensive Care Unit. We compared the two groups in terms of safety and cost-effectiveness.
Results:
We analyzed 47 central venous access devices in 42 children. There were no insertion-related complications. Only one catheter-related bloodstream infection was recorded, in group A. However, the costs related to central venous access device insertion were quite different: €330–€540 in group A versus €105–€135 in group B.
Conclusion:
In the pediatric patient candidate to a major neurosurgical operation, preoperative insertion of the central venous access device in the sedation room rather than in the operating room is less expensive and equally safe.
Introduction
Central venous access devices (CVADs) are defined as venous catheters whose tip is located in the superior vena cava, in the right atrium, or in the inferior vena cava. They are essential part of the critical and oncologic care, especially in those children who need multiple infusion therapies, fluid replacement, parenteral nutrition, frequent blood sampling, or hemodynamic monitoring. 1
The insertion of a CVAD is a procedure potentially associated with early and late adverse events (including pneumothorax, accidental injury to arteries or nerve, arrhythmias, catheter-related infection, etc.) and relevant costs. 2,3 Careful choice of the device, appropriate insertion technique, and proper management of the device are well-known strategies commonly adopted to achieve an optimal clinical result. 4
Ultrasound-guided puncture and cannulation of the deep veins is currently considered mandatory, not only in adult patients but also in pediatrics, by all international guidelines and evidence-based recommendations. 5,6 During CVAD insertion, ultrasound is also of great value for the pre-procedural ultrasound examination (so to choose the most adequate vein and a catheter of appropriate caliber), for assessing the correct position of the tip, and for real-time diagnosis of potential insertion-related complications (hematomas, pneumothorax, etc.). According to the current international recommendations, tip location of the central catheter should be preferably verified during the procedure, by intracavitary electrocardiography (IC-ECG) 7,8 and/or by trans-thoracic echocardiography. 5
While short-medium term venous access devices such as non-tunneled CICCs (centrally inserted central catheters), PICCs (peripherally inserted central catheters), and midline catheters are usually inserted at bedside, long-term devices (tunneled CICCs, tunneled PICCs, ports) are preferably inserted in dedicated environments, such as procedure rooms, sedation rooms, operating rooms, or radiological suites. Infection prevention appears to be related to the adoption of the currently recommended strategies of antisepsis (a proper policy of hand hygiene, use of maximal barrier precautions and of 2% chlorhexidine in alcohol),7 rather than to the type of environment. On the other hand, the special needs of the pediatric patient may often require a dedicated environment equipped not only for the insertion maneuver (ultrasound device and ECG monitor) but also for a proper sedation/anesthesia management.
The current international guidelines on central venous access recommend to avoid fluoroscopy whenever possible 7 and to adopt methods of tip location such as IC-ECG and TTE, which are safer, more accurate, and less expensive than radiological methods. Thus, the use of the radiological suite is not justified any longer. Therefore, when sedation and/or anesthesia are required, we must choose between a simple, low-cost procedure room or a high-cost, fully equipped operating theater.
In accordance with the growing concerns about the economic costs of healthcare, it is important to optimize the cost-effectiveness of such procedures, with the aim to guarantee the best possible healthcare practices but favoring those that save resources. In this regard, we must take into account both the cost of the procedure itself and the cost of potential adverse events; the former includes not only the devices, the equipment, and the human resources, but also the costs related to the environment in which the procedure takes place.
Methods
We designed this retrospective, monocentric study with the aim of comparing the procedures of CVAD insertion in two different hospital environments: (a) the standard operating room and (b) the sedation room of our Pediatric Intensive Care Unit (PICU). We reviewed the CVAD insertions of all children candidate to major neurosurgical operation; only CVAD placed prior to surgery were considered. The procedures were evaluated in terms of cost-effectiveness (resources) and safety (periprocedural adverse events).
The patients were divided in two groups: group A included CVAD inserted in the operating theater, immediately before neurosurgery; group B included CVAD inserted in the sedation room of the PICU, within the 24 h before neurosurgery.
We recorded the following data: type of sedation/anesthesia and drugs administered; technique of CVAD insertion; method of tip location; type of catheter securement; length of the procedure; early and late adverse events; length of stay in PICU; total length of hospital stay.
Catheter-related bloodstream infections (CRBSI) were defined as an infection whose source is the catheter, as determined by the technique of delayed time to positivity, in accordance with the Centers for Disease Control and Prevention (CDC) criteria. 9
Group A
In patients who had the CVAD insertion in the operating room, general anesthesia was consistently adopted (tracheal intubation with oxygen/sevoflurane anesthesia, plus maintenance with sevoflurane and remifentanil in continuous infusion). Before the scheduled neurosurgical procedure, the CVAD was inserted by ultrasound guidance, most frequently by a short axis, out of plane approach to the internal jugular vein, using an ultrasound device (MicroMaxx, SonoSite) with a hockey stick 26 mm linear transducer at high frequency (10–13 MHz). All CVADs were non-tunneled CICCs inserted by direct Seldinger technique (“catheter over guidewire”), secured using a skin-adhesive sutureless device and covered with a semipermeable transparent dressing. Tip location was verified by a post-procedural chest x-ray, taken at the end of the surgical operation.
Group B
Patients who had CVAD insertion in the sedation room of the PICU were accompanied by their parents, who were allowed to stay at the patient’s side until an appropriately deep sedation state was achieved. In all patients, we induced a state of deep sedation with spontaneous breathing, using an oxygen/sevoflurane mixture and/or intravenous drugs such as ketamine, propofol, midazolam, or fentanyl, as needed. 10 No tracheal intubation was performed in this group. The CVAD was inserted by ultrasound guidance, using the same type of ultrasound device described for group A. In most cases, the preferred technique was a long axis, in plane approach to the brachio-cephalic vein. The CICCs were inserted using the modified Seldinger technique (“catheter through introducer”) and tunneled to the infraclavicular area. All CICCs were in polyurethane, non-cuffed, and power injectable. The correct tip location was verified during the procedure, by IC-ECG and/or TTE. The catheter was secured by a subcutaneously anchored sutureless device, 11 and the exit site was covered with a semipermeable transparent dressing.
For an evaluation of the cost-efficacy of the procedure, we computed the costs attributable to the preparation of each setting, considering the personnel involved in the procedure and the material and devices utilized. In evaluating the safety of the procedures, we considered the incidence of periprocedural complications and of late catheter-related complications. Our primary outcome was the demonstration of a better cost-efficacy profile of the procedure conducted in the sedation room as compared with the operating room. Secondary outcomes were the incidence of periprocedural adverse events, the length of stay in the PICU, and the total length of hospital stay.
This retrospective study was approved by the Ethical Committee of our Institution and the parents of the children involved signed an informed consent.
Statistical analysis
To assess the statistically significant differences between the outcomes in the two groups, we used a Mann–Whitney test at a statistical significance value of 0.05. The values were expressed as mean ± standard deviation (SD). The median value was used for selected parameters.
Results
Out of our records from April 2015 until February 2018, we considered 42 children who underwent a major neurosurgical procedure requiring preoperative insertion of a CVAD: 27 patients were male (64.3%) and 15 were female (35.7%). Some of the patients underwent more than one CVAD insertion, so that the total number of insertions was 47. The patient’s age at the time of the procedure ranged from 3 months to 20 years (mean age = 70 ± 63.8 months). In 38 cases (80.9%), neurosurgery was required for removal of a cerebral tumor while in 9 cases (19.1%) for correction of craniostenosis. In 25 cases (53.2%), the CVAD was inserted in the operating room (group A), while in 22 cases (46.8%) in the sedation room of the PICU (group B). The clinical characteristics of each group are reported in Table 1. Two patients of group B had two different neurosurgical operations and a CVAD was inserted before each surgery.
Clinical characteristics of the patients.
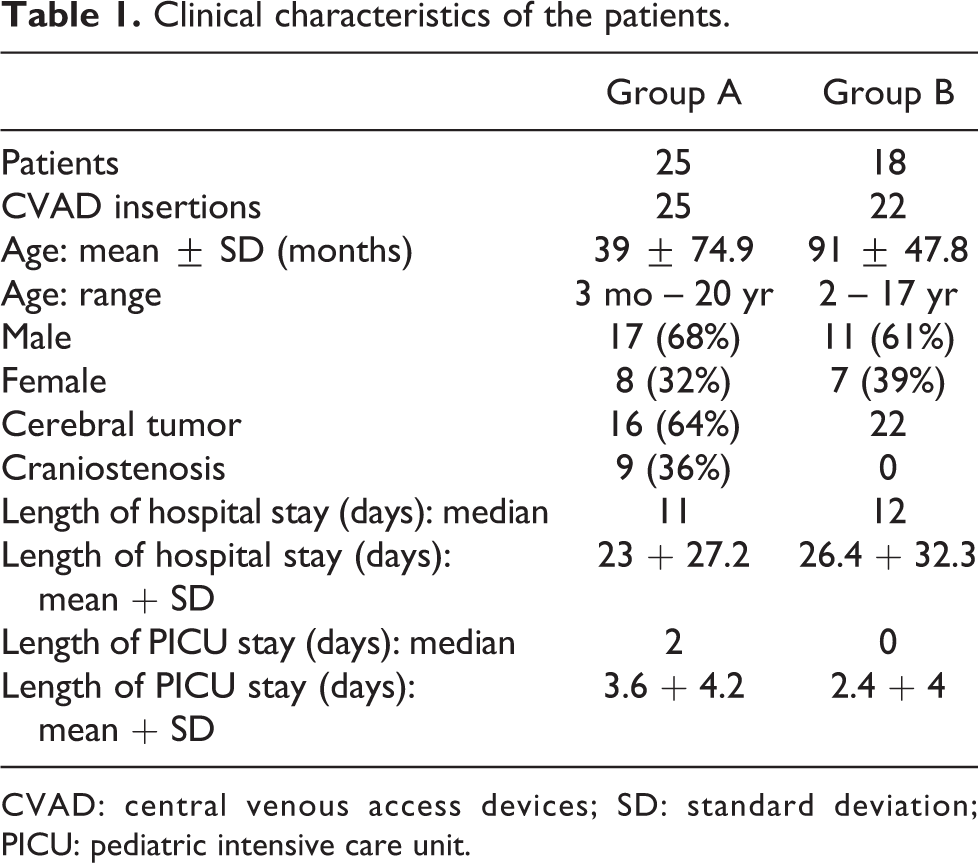
CVAD: central venous access devices; SD: standard deviation; PICU: pediatric intensive care unit.
The overall duration of the procedure was 30–50 min in group A and 30–75 min in group B.
No immediate or early catheter-related complication occurred. As regards late complications, one patient in group A had one episode of CRBSI; in one patient of group A and in one of group B, accidental dislodgment of the CVAD occurred in the post-operative period, and a new CVAD was inserted in the sedation room of the PICU. No infection of the exit site was reported. No symptomatic catheter-related thrombosis occurred.
The overall cost of CVAD insertion in the operating room ranged between €330 and €540; this was computed considering the total cost of the occupation of the operating theater (€600/h), inclusive of the staff, plus the cost of the CVADs and other material required for the procedure (ranging between €30 and €40).
The overall cost of CVAD insertion in PICU ranged between €105 and €135; this includes the cost of the CVAD (€51–€81) and of other material required for the procedure (insertion pack, €24; subcutaneously anchored securement, €30; etc.). The cost of the sedation room and of the PICU staff was not considered in this analysis, as it was not an expense related to the procedure but to the overall maintenance of the activity of the PICU.
Discussion
The scientific literature analyzing CVAD insertion in terms of cost-efficacy is very scarce, and it is generally focused on prevention of catheter-related infections, 12 –14 on the cost-effectiveness of antibiotic-coated catheters, 15 –17 or on the cost benefit of assigning CVAD insertion to nurses rather than to the medical staff. 18 Very few studies have addressed the issue of the most convenient environment for invasive procedures. In two recent clinical studies, 19,20 the elective removal of long-term CVADs in low-cost dedicated environments was as safe as the removal in operating room, but it was more cost-effective.
In our retrospective analysis, we found that CVAD insertion in the sedation room of our PICU (group B) was much less expensive than in the operating room (group A), being associated with an average cost reduction of about 72.4%. This difference is obviously related to the high cost of maintaining the operating theater in activity, a cost of approximately €600/h in our hospital (and probably slighter lower or higher, but similar, in other centers).
In group A, the procedure of CVAD insertion was usually shorter, mainly because no intra-procedural method of tip location—IC-ECG or TTE—was adopted; on the other hand, in this group tip location was performed after surgery, taking a post-procedural chest x-ray, which was obviously associated with a further cost in terms of time and money. Another factor which might explain the longer procedure time in group B is the consistent choice of tunneling the CICCs; though, this maneuver was felt to be highly desirable, so to guarantee a better protection from the risk of bacterial contamination via the extraluminal route. 21 –23
In terms of safety, there were no significant differences between group A and group B. The performance of the procedure in the sedation room was not associated with any increased risk of insertion-related complications, which were absent in both groups. This makes sense, since the main strategy for avoiding puncture-related complications (pneumothorax, accidental arterial injury, etc.) is ultrasound guidance, which was adopted consistently in both groups.
In terms of infection risk, the only CRBSI occurred in group A. This is consistent with the widespread notion that infection prevention is mainly based to the adoption of a strict policy of hand hygiene, on the use of 2% chlorhexidine in 70% alcohol for skin antisepsis, and on the adoption of maximal barrier precautions (mask, beret, sterile gloves, sterile gown, vast sterile field and long sterile cover for the ultrasound probe): such strategies were consistently adopted in both groups. In our experience, insertion of a CVAD in a low-cost sedation room rather than in the operating theater did not increase the risk of infection; on the contrary, the only episode of CRBSI occurred in a patient of group B.
Length of stay of the device, as well as its use (chemotherapy vs intraoperative monitoring or intravenous therapy) did not influence outcome of the device in term of complication rate.
As regards the length of hospital stay and of PICU stay, there was a wide statistical dispersion of these variables among the patients in both groups, as shown by the high standard deviation. This variability is mainly explained by the presence of patients who needed a long hospitalization due to the need of further surgery or for other complications. In only one case, the extended hospital stay could be attributed to a CRBSI.
In conclusion, the preoperative insertion of the CVAD in PICU was as safe as the “last minute” insertion in operating room, but more cost-effective.
Furthermore, in our experience the performance of the procedure in PICU had some collateral advantages: The environment of the sedation room favored the adoption of the best current strategies for reducing complications: minimal invasiveness of the sedation/anesthesia techniques; intra-procedural tip location by IC-ECG and/or TTE for avoiding the risk of malpositions; tunneling of the catheter, for reducing the risk of extraluminal contamination; securement by subcutaneously anchored devices, for reducing the risk of dislodgment. In the sedation room, the procedure could be carried out with no hurry, taking time for an accurate preoperative ultrasound scan of the venous patrimony of the patient, and for the other ultrasound-based maneuvers (immediate post-puncture control of the pleura, so to exclude pneumothorax; immediate control of the puncture site, so to rule out hematomas; tip navigation, so to assess the correct direction of the guidewire and of the catheter; tip location by TTE, using a micro-convex probe or a sectorial probe). The tip location methods adopted in the sedation room (IC-ECG and TTE, potentially feasible but logistically more challenging in the operating room) are known to be more accurate and less expensive than post-procedural chest x-ray, and they avoid the exposure of children to radiation.8,
24
Finally, the sedation room is compatible with an environment built around the child’s needs (colors, toys, adequate temperature, the presence of the parents soon before the sedation); this implies numerous psychological benefits for the patient and his parents which cannot be adequately described in economic terms.
25
The main limitations of our study derive from the limited number of patients that, although it allowed us to identify the undoubtable economic advantage of the sedation room, was not sufficient to adequately weigh the overall incidence of complications of the procedure.
Moreover, as in all retrospective studies, the homogeneity between the two groups was not optimal: there was a significant imbalance regarding the ages of the patients: in group A we had nine patients less than 1 year old. In addition, all the patients who had surgery for craniostenosis were all in group A. There is ground for suggesting a prospective randomized study in the future, so as to assess potential differences in complications between the two strategies.
Conclusions
In a retrospective analysis of 47 CVAD insertions in 42 children scheduled for a major neurosurgical operation, we found that the insertion of the device in a sedation room rather than in the operating room was associated with a relevant reduction in costs, with no difference in terms of immediate, early, or late complications. The benefits of this innovative approach include an easier periprocedural management of the patient, less radiation exposure, and more comfortable and welcoming environment for the child and his parents.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.