
Abstract
Objective:
To evaluate the validity of laboratory tests for blood sampling from a peripherally inserted central catheter.
Methods:
A total of 22 patients diagnosed with head and neck cancers were enrolled. In total, 101 paired blood samples were taken both via venipuncture and peripherally inserted central catheter for hematology and biochemistry testing. Paired t tests and linear correlation analysis were used to evaluate the results. Blood sampling–related pain was recorded by visual analogue scales and numerical rating scales. Infusion occlusion, hemolysis, and catheter-related blood stream infection were also recorded.
Results:
The peripherally inserted central catheter–associated test results were slightly lower than those with venipuncture. Some parameters differed more than others. However, the degree of difference was less than 5% for every pair. There was a high correlation between the test results with two methods of blood sampling with the representative equation approximately being “y = x.” According to visual analogue scales and numerical rating scale analysis, the pain degree with peripherally inserted central catheter was significantly lower than that of the venipuncture (p < 0.001). No case of infusion occlusion, catheter-related blood stream infection was reported with both methods. Hemolysis rate in blood samples from peripherally inserted central catheter (1/101) was much lower than that seen with venipuncture (11/101) with significant difference (p = 0.0056).
Conclusion:
Blood sampling via peripherally inserted central catheter and venipuncture showed equivalent reliability in laboratory testing. Compared with venipuncture, blood sampling via peripherally inserted central catheter causes less pain and is safer. Blood sampling via peripherally inserted central catheter is strongly recommended for clinical use.
Introduction
A peripherally inserted central catheter (PICC) is a type of central vascular access device. Unlike peripheral venous catheter (PVC), which is placed in a superficial vein of a short length on the hand or arm, PICC is inserted into a relatively large vein, mainly the basilic vein or brachial veins. Thus, PICC can be used for intravenous delivery of total parenteral nutrition (TPN), chemotherapy, antibiotics, or other medications.1–3
Patients with PICC usually receive a long time period treatment during which blood sampling is inevitably frequently performed. Blood sampling via venipuncture is invasive and painful, and thus, if frequently used, it might cause bruising, hematoma, infections, vasovagal reactions, anxiety, and in rare cases, peripheral nerve injury.4,5 It also exposes nurses to the risk of an accidental needle stick. Furthermore, it is also challenging for nurse to perform a venipuncture when the vessel condition is poor, especially for obese patients or who had chemotherapy.6,7
Theoretically, PICC can be an alternative to venipuncture for blood sampling. Compared to venipuncture, there are several advantages in favor of PICC, that is, painless intervention and no need for repeated invasive procedures, low risk of needle stick, and process simplicity. Easier blood aspiration should also be an advantage for PICC in normal circumstances, although formation of fibrin sheath which forms one-way valves in the catheter tip may make the aspiration difficult or even impossible. A fibrin sheath may occur after placement of a PICC, and if extensive, fluid flow may be decreased causing partial or complete occlusion.8–10 Nevertheless, fibrin sheath related to blood sampling from catheters was rarely mentioned.11–15 However, more adequate and reliable evidence to confirm the accuracy and safety of the blood sampling from PICC is needed. Hambleton et al. conducted a prospective, cross-sectional research on laboratory test results comparing venipuncture and peripheral catheter. They reported peripheral catheter to be a reliable collection method for hematology, biochemistry, and coagulation assessments. 11 This research, however, did not provide significant evidence regarding the type of venous catheter (PVC or PICC), as it was not considered. Tourniquet was used for every patient in this study to facilitate the identification of a viable vein, which was not necessary for centrally inserted central catheter (CICC) or PICC.12–14 Furthermore, common complications of PICC were not evaluated except for hemolysis.
We conducted a prospective, self-controlled study to accurately evaluate the validity of laboratory tests when using PICC for blood sampling collection.
Methods
Eligible patients
The study protocol was approved by the ethics board of The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, China. This prospective study enrolled 22 eligible patients. All patients were diagnosed with head and neck cancers by Otolaryngology & Head and Neck Department or the Radiotherapy Department. PICC was successfully placed in all patients (C.R. Bard, Inc., New Providence, NJ, USA) and they underwent neoadjuvant chemotherapy with the regime of Docetaxel-Cisplatin-5′-Fluorouracil (TPF).
The enrollment period lasted from May 2017 to May 2019. Patients who refused to undergo blood sampling via PICC or had a high performance status (PS) (>2) were excluded. Patient’s PS is an important part of cancer care and treatment. We used Zubrod scale to evaluate patient’s PS. The scale recommends the following: normal activity is 0, symptomatic and ambulatory and cares for self is 1, ambulatory > 50% of time and occasional assistance is 2, ambulatory ⩽ 50% of time of nursing care needed is 3, and bedridden is 4. 16 We excluded the patients with a high PS because it was not convenient for them to do PICC maintenance in outpatient department. Informed consent was obtained from every patient.
Sample collecting procedure
Altogether 101 paired blood samples were collected. To collect one pair of samples, the nurse would initially collect the blood sample via venipuncture of median cubital vein of the upper limb without PICC using BD Vacutainer® venous blood collection portfolio (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), including blood collection tube, needle, holder, and tourniquet. The second step was the blood sample via PICC. Infusion through PICC was halted prior to blood sample collection. The hub was then cleaned or disinfected by rubbing alcohol and 2 mL blood was discarded from the catheter, using a syringe without needle. A new syringe without needle was used to draw blood sample out of the catheter. The sample was then injected into vacutainer. Upon completing the blood sampling process, the catheter was flushed and locked with 10 mL of 0.9% saline solution before the infusion was continued. If there was no infusion at the point of blood sampling, the process was the same except flushing and locking instead of continuation.
One pair of samples was retrieved by the same nurse by venipuncture first and then PICC immediately.
Laboratory tests
All blood samples were sent to laboratory test department for hematology and biochemistry testing. Hematology tests were conducted with automatic blood cell analyzer (Beckman Coulter, Inc., Carlsbad, CA, USA), while biochemistry was performed using an automatic chemistry analyzer (Architect C16000; Abbott Laboratories, Abbott Park, IL, USA).
Pain associated with blood sampling
Pain intensity score was recorded using the visual analogue scales (VAS) and numerical rating scales (NRS).17,18
Safety monitoring
Infusion occlusion, blood sample hemolysis, and catheter-related infection were monitored. Infusion occlusion was defined by slowing down of the dropping speed or complete stoppage due to occlusion of catheter. Hemolysis was determined by laboratory technician. If the color of blood plasma or serum was red after centrifugation, the sample was determined as showing “hemolysis.” Catheter-related infection was defined by the presence of clinical manifestations of infection and the evidence of colonization of the catheter tip by bacteria, mycobacteria, or fungi.
Statistical analysis
The paired continuous data were summarized as the mean ± standard deviation and analyzed using the paired Student’s t test as well as linear correlation analysis. Categorical data were analyzed using the chi-square test. A p value of <0.05 was considered statistically significant. For linear correlation analysis, R2 > 0.8 was considered as high correlation; 0.5 < R2 < 0.8 was considered as moderate correlation; 0.3 < R2 < 0.5 was considered as low correlation; and R2 < 0.3 was considered as no correlation. All statistical analyses were performed using Graphpad Prism 8 (Graphpad Software Corp., San Diego, CA, USA).
Results
Eligible patients’ characteristics
A total of 22 patients were included in the study. All patients were male. The average age was 61.9 ± 3.51 years. The average duration of PICC indwelling time was 83.7 ± 8.4 days. The average number of blood drawing for patients was 16.9 ± 3.0 times. All patients suffered from head and neck cancers. Patients’ characteristics are listed in Table 1.
The characteristics of enrolled patients.
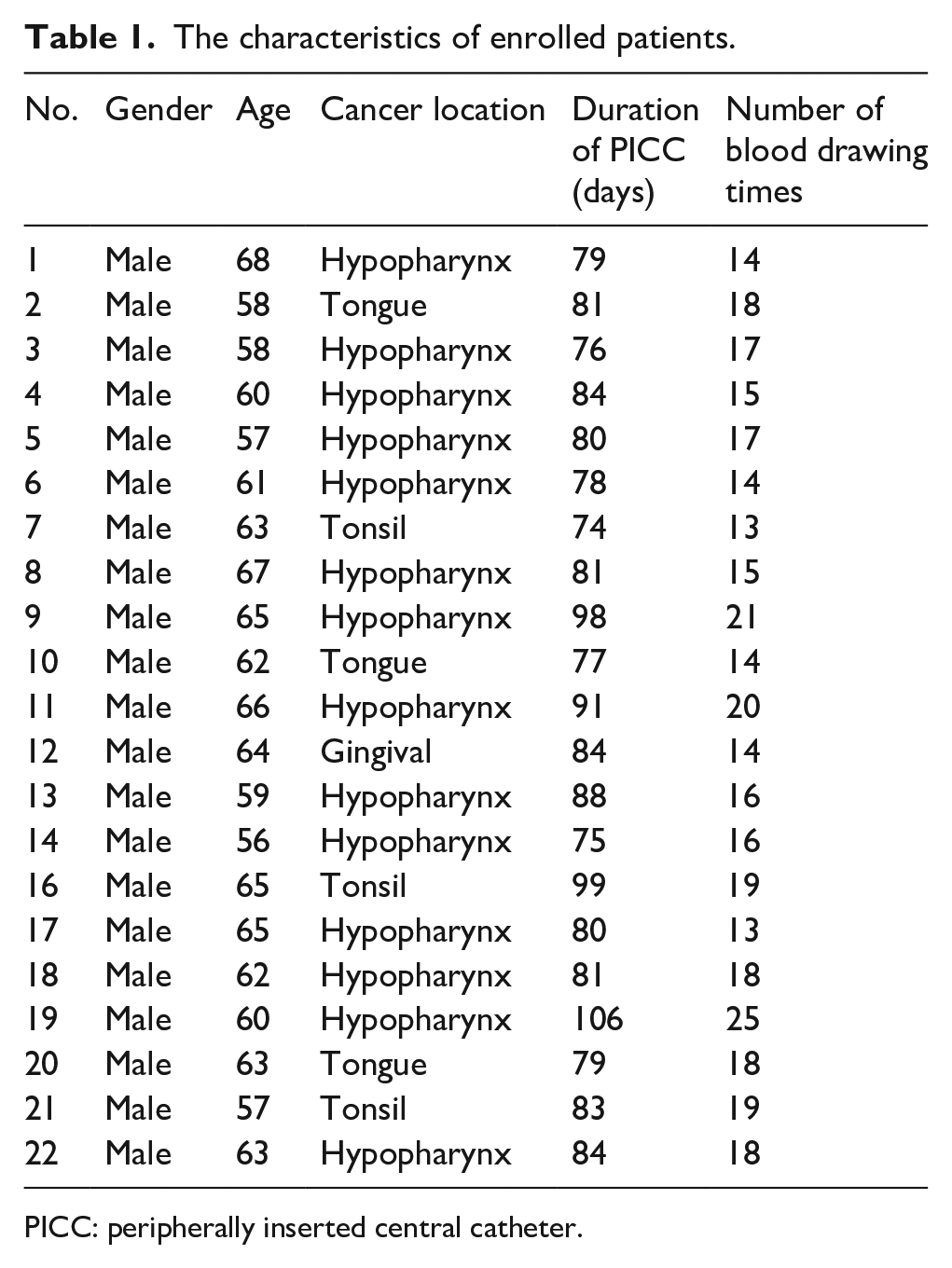
PICC: peripherally inserted central catheter.
Difference between venipuncture and PICC-associated laboratory test results
Three parameters in hematology including white blood count (WBC), hemoglobin (Hb), and platelet count (PLT) as well as six parameters in biochemistry including osmotic pressure (OS), sodium (Na), potassium (K), glucose (GLU), serum creatinine (SCr), and C-reactive protein (CRP) levels were examined and recorded for all samples.
Each parameter was divided into two subgroups: “infusion” (blood sampling during infusion) and “not infusion” (blood sampling without infusion).
The test results of PICC were slightly lower than that with venipuncture for almost all parameters except in WBC-infusion group, some showing significant difference. Degree of difference was less than 5% for every pair. The data regarding averages and the degree of difference are shown in Figures 1 and 2.
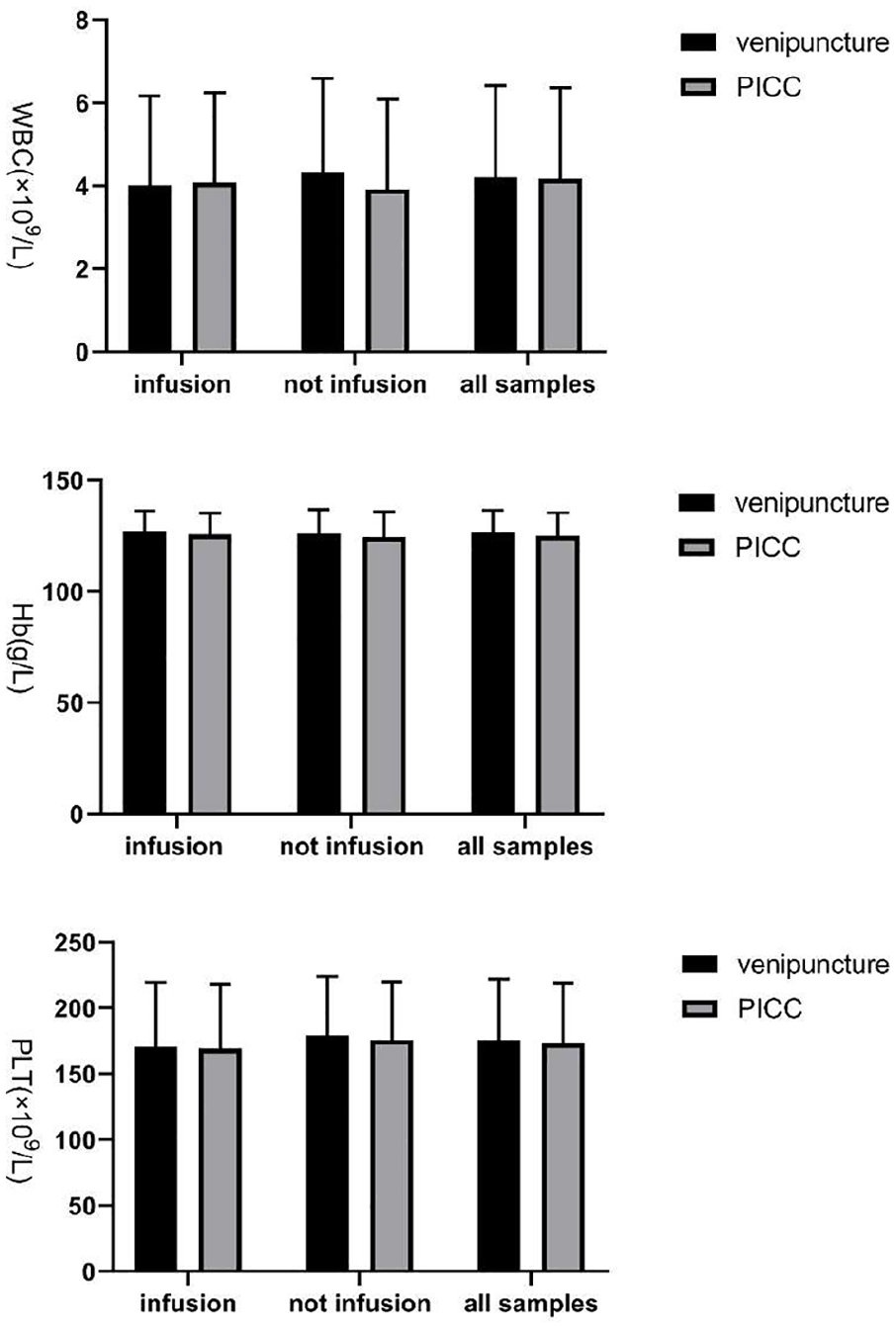
Hematology test results. All parameters are divided into two groups according to infusion or not at the time of blood sampling. Except for the “WBC-infusion” group, the test results of PICC are a little lower than the venipuncture ones, with some groups of statistical significance. The degree of difference between the two methods was quite limited (less than 5%). WBC: white blood count.
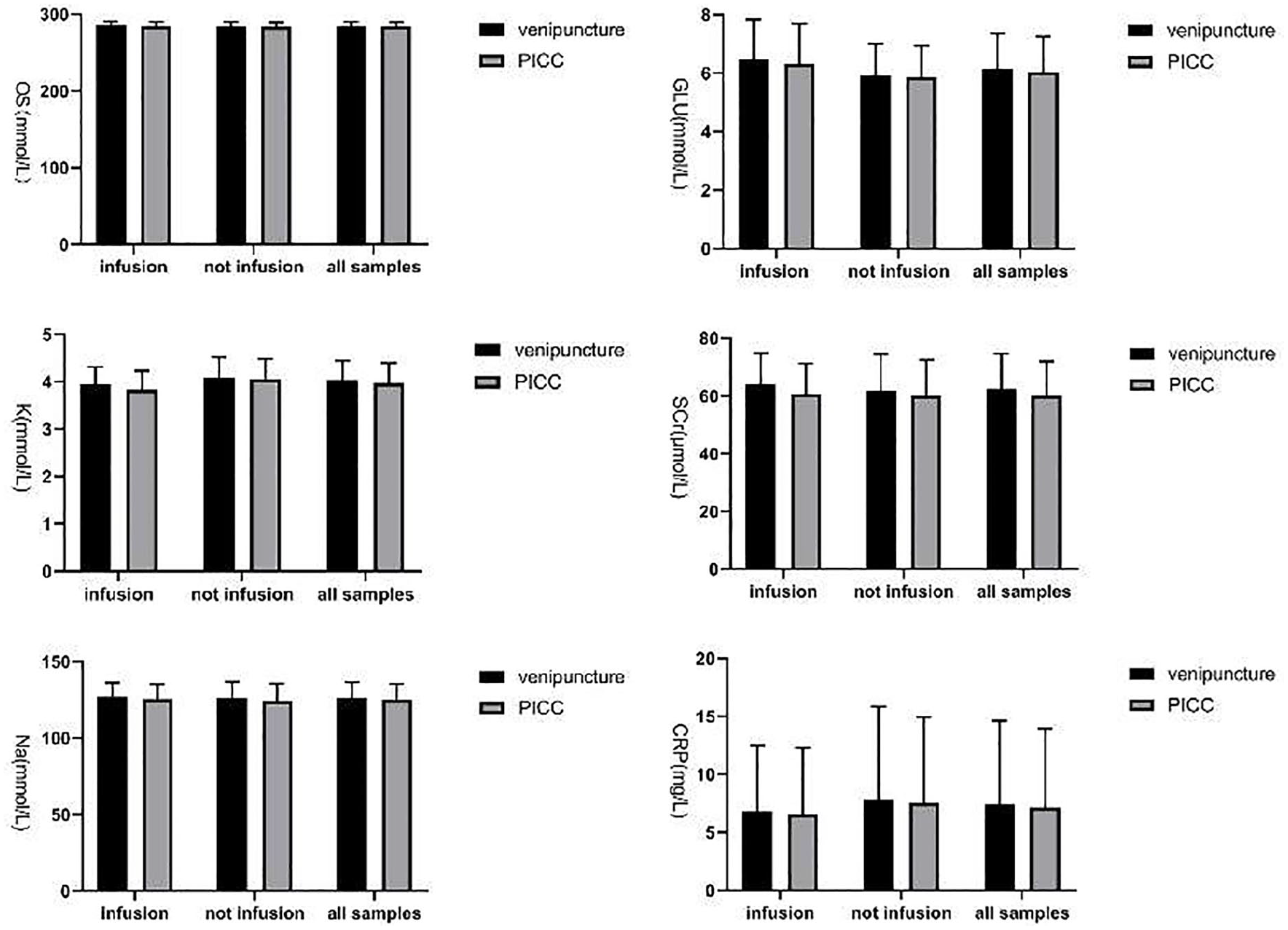
Biochemistry test results. The test results of PICC group were a little lower than venipuncture group with some groups statistically significant. The degree of difference between the two methods was quite limited (less than 5%).
The results obtained with venipuncture and PICC were highly related to each other
As done for the difference analysis, subgroup analysis according to infusion was also performed along with a correlation analysis. There was a considerably strong linear correlation between every pair of values. The representative equation was almost “y = x.” The correlation degree of “K” groups and “OS” groups was slightly lower. The R2 of “K-total,” “K-infusion,” “K-not infusion,” “OS-total,” “OS-infusion,” and “OS-not infusion” was all between 0.7 and 0.8, while R2 of all the other parameters was well over 0.8. The correlation of all groups is shown in Figures 3–5.
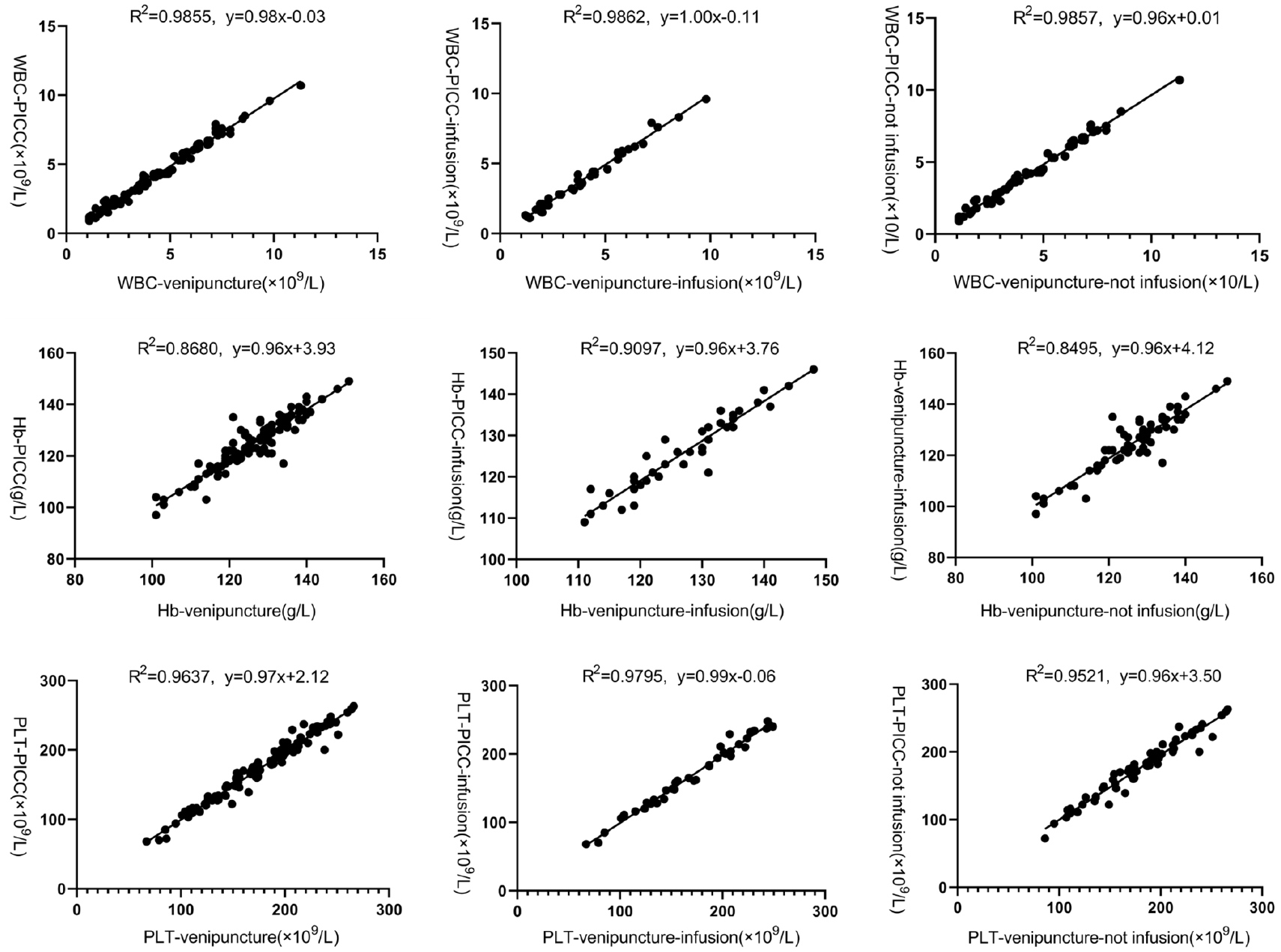
Linear correlation of hematology test results between venipuncture and PICC. There was a high linear correlation between the two methods with the linear equation almost “y = x.”
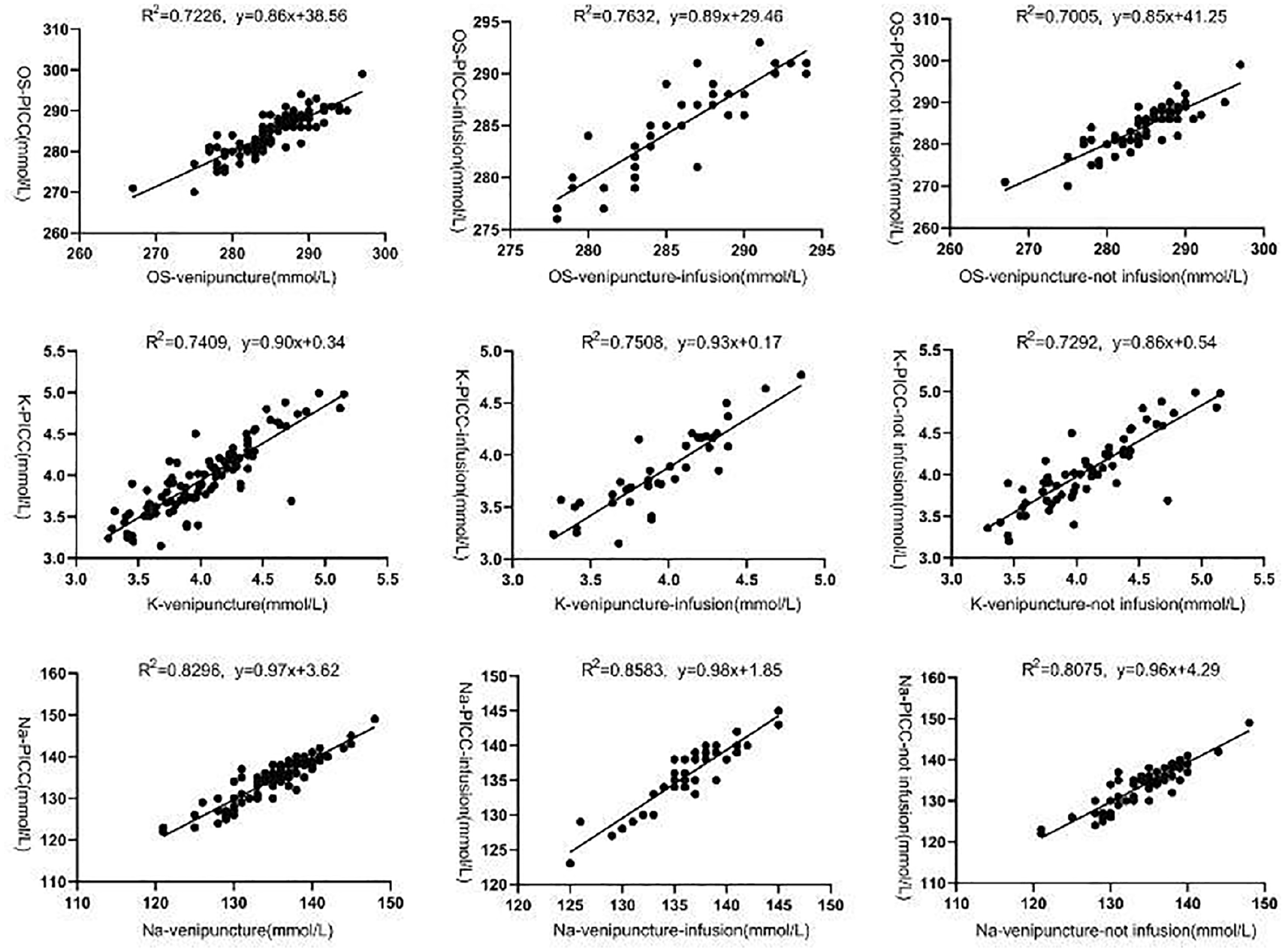
Linear correlation of partial biochemistry test results between venipuncture and PICC. There was a medium linear correlation for “OS” and “K” while high linear correlation for “Na” between the two methods. The linear equation is almost “y = x” for all lines. OS: osmotic pressure; K: potassium; Na: sodium.
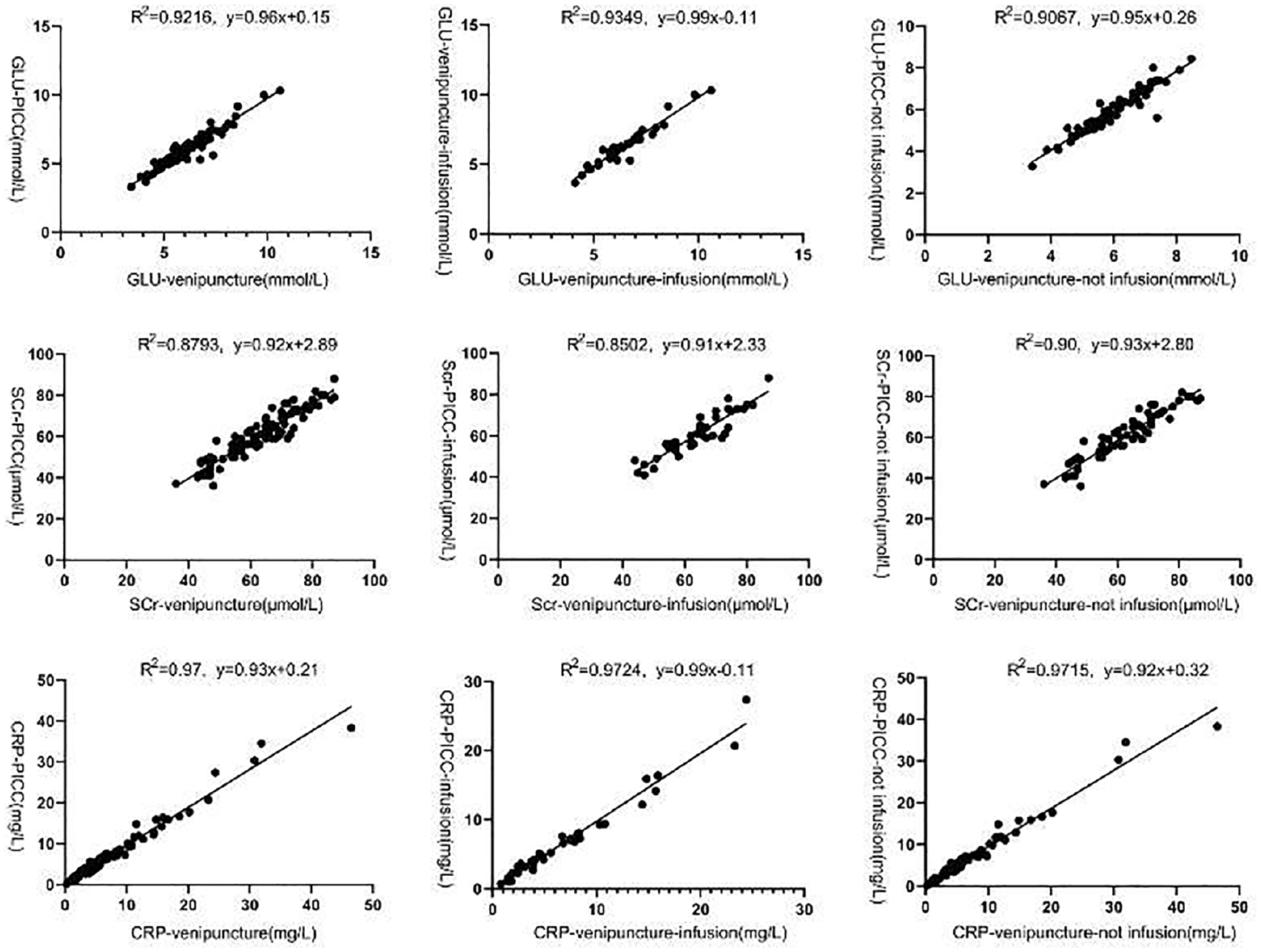
Linear correlation of partial biochemistry test results between venipuncture and PICC. There is a high linear correlation for all parameters between the two methods. The equation is almost “y = x” for all lines.
The degree of pain with PICC was much lower than that with venipuncture
According to VAS and NRS analyses, the pain degree with PICC was significantly lower than that with venipuncture (p < 0.001) (Figure 6).
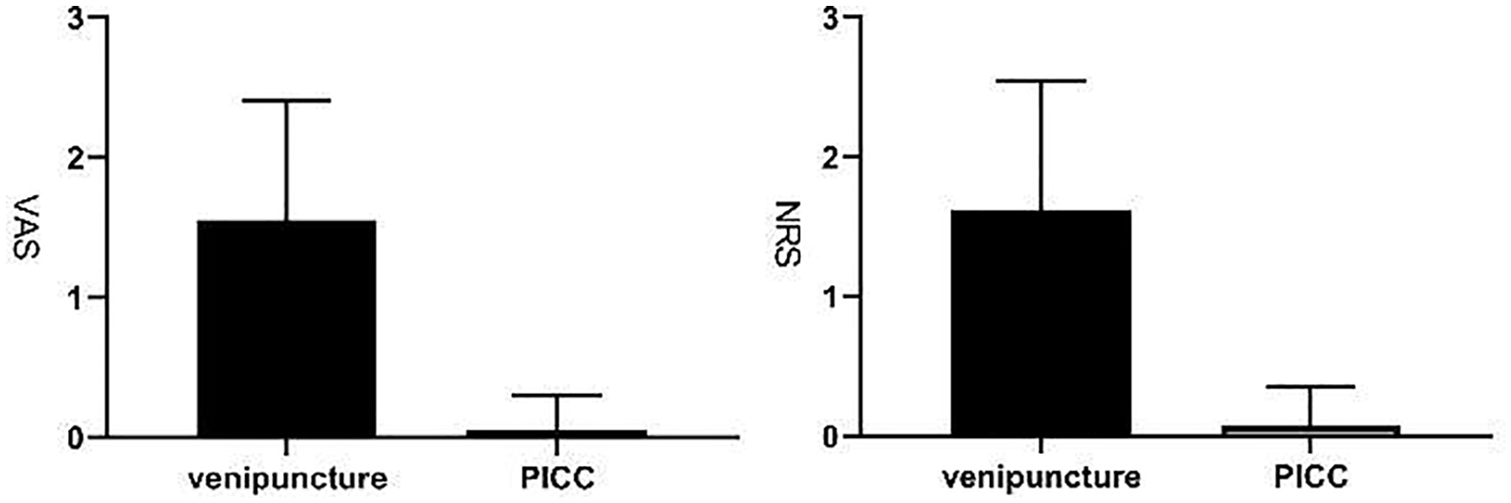
The pain degree of the two methods of blood sampling using the VAS and NRS scales. VAS: visual analogue scale; NRS: numerical rating scale.
Blood sampling from PICC was safe
There was no case of infusion occlusion or catheter related infection in the PICC sample collection among the 22 patients. Hemolysis rate in blood samples from PICC (1/101) was much lower than that with venipuncture (11/101) with significant difference (p = 0.0056).
Discussion
In our study, we thoroughly evaluate blood sampling via PICC, considering two main aspects: accuracy and safety. We also evaluate the pain level experienced by patients.
For accuracy, both paired t test and linear correlation analysis were conducted. T test results showed that almost all PICC-associated data were slightly lower than that with venipuncture. The difference was not more than 5%, and considering the regular measurement error, a slight difference is acceptable. Difference in some groups, although slight, was statistically significant (p = 0.01–0.05), while in the other groups it was not. The reason for the PICC-associated data being slight lower remains unknown. It could be speculated that the blood drawn from PICC was diluted by the residual liquid in the catheter. However, as the difference was slight and did not affect the accuracy, it might not be necessary to speculate about the reason.
Furthermore, linear correlation analysis was also conducted. If the test results are slightly affected by venipuncture or PICC, a high linear correlation must be noted between them (R2 > 0.8), and the equation of the line should be almost “y = x.” As expected, a high correlation between venipuncture and PICC was confirmed for WBC count and Hb, PLT, Na, GLU, SCr, and CRP levels, with all of having R2 > 0.8 and a representative equation of approximately “y = x.” The results demonstrate the equivalence of the two methods of blood sampling with respect to the validity of the laboratory test results. However, R2 in the “K” and “OS” groups was slightly lower than 0.8, although comparable (0.7409 and 0.7226, respectively); the slope of the lines based on the equation for these values was 0.9001 and 0.8623, respectively. We did not consider that the exception seen for “K” and “OS” could become a negation of the equivalence of the two methods. The reason for “K” being an exception was that compared to other parameters, it was difficult to test “K” accurately. The “K” concentration in extracellular fluid was quite low and any slight hemolysis, which cannot be completely avoided in blood sampling, would lead to leakage of intracellular “K” resulting in relatively large measurement errors. 19 For “OS,” the dispersion degree in both groups was too small, and thus, any slight measurement error between the paired data could be enlarged. The coefficient of variation (CV) in “OS-venipuncture” and “OS-PICC” was only 1.72% and 1.75%, respectively, which were lowest among those for all parameters.
Combining the results of paired t tests and linear correlation analysis, we can conclude that the two methods of blood sampling are equivalent in terms of the accuracy of laboratory results.
We further compared the pain degree and safety between the two methods. Blood sampling by PICC caused much less pain as expected. There was no difference in the incidence of infusion occlusion and catheter-related infection between the two methods, while the incidence of hemolysis in PICC group was significantly less than in the venipuncture group. This finding suggested that blood sampling via venipuncture caused more physical damage to cells than PICC and an easy explanation for it can be proposed. The width of PICC is large enough for easy pumping and pushing in contrast to that with venipuncture, wherein both a sharp, narrow needle and repeated attempts in patients with poor vascular condition may lead to hemolysis.20–22 Vascular condition is known to become poorer after infusion of cytotoxic drugs such as chemotherapeutic drugs. 6
In conclusion, our study proved that blood sample collection from PICC is safe and effective, and thus, is strongly recommended for clinical use.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Second Affiliated Hospital Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, China (ethical number: IR2019002001).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported in part by grants from the Department of Health and Family Planning Commission of Zhejiang Province (2017KY380 and 2017KY407).