
Abstract
Background:
Arteriovenous access failure is most often due to the development of neointimal hyperplastic stenoses. Balloon angioplasty remains standard of care for endovascular treatment of stenoses obstructing blood flow in hemodialysis fistulas and grafts. Scoring balloon technologies have been developed to disrupt the atheromatous plaque and have shown to be safe and effective for treating stenosis in the hemodialysis access circuit. However, improvement in patency has yet to be established.
Methods:
This prospective, single-arm study included 50 patients with stenosed hemodialysis fistula/grafts treated with the AngioSculpt® scoring balloon (Philips) and followed for 6 months. The primary endpoint was target lesion primary patency at 2 and 6 months defined as freedom from re-intervention.
Results:
Treatment with the scoring balloon resulted in a reduction in stenosis from 78% ± 13.36% to 7.2% ± 7.57% (mean ± standard deviation). Scoring balloon inflation pressures averaged 11.4 atm; no slippage/dissections occurred. After 2 months, 10% of patients required re-intervention. At 6 months, 19% of patients required re-intervention. The 6-month freedom from re-intervention rate was higher for patients with stenosed fistulas (83.3%) compared to patients with stenosed grafts (71.4%). Six-month patency rates were highest for patients with no or one previous intervention (91.6% and 90.0%, respectively); patients with two to five preceding interventions had a 6-month patency rate of 80%, and those with more than five previous interventions had a 50% 6-month patency rate.
Conclusion:
Results from this pilot study suggest that the AngioSculpt scoring balloon may be a viable treatment option for stenosed arteriovenous fistula/graft access.
Keywords
Introduction
By 2008, more than 341,000 patients in the United States were undergoing hemodialysis for the treatment of their end-stage renal disease (ESRD). 1 All arteriovenous (AV) access circuits, whether native vein or prosthetic graft, will inevitably fail due to the development of neointimal hyperplastic stenoses. These smooth muscle cell lesions obstruct blood flow and thereby decrease the efficiency of hemodialysis and increase the risk of access thrombosis.
AV fistula/graft stenosis is the most frequent complication and affects morbidity and mortality in dialysis patients. 2 Typically, multiple interventions are required to maintain patency, and the cost of treating a patient who has failure of a hemodialysis access graft is significantly higher (US $62,000 per patient-year) than the cost of treating a patient who does not have access failure.1,3 Consequently, hemodialysis access maintenance contributes significantly to the financial healthcare burden of ESRD. 4 Total cost-reducing treatment options that can restore blood flow for longer periods of time are desirable.
Percutaneous transluminal angioplasty (PTA) is the most commonly used intervention for access stenosis management. Studies have reported 6-month patency rates around 50% to 60% after angioplasty.5,6 In addition, repeated angioplasty procedures are often necessary to maintain function and preserve patency.7,8 The availability of ultra-high-pressure balloons has improved technical success, but there have been reports of delayed elastic recoil vessel wall.9,10 Despite decades of clinical research, an effective, long-lasting treatment for neointimal hyperplastic stenoses remains elusive.
The development of PTA scoring balloon catheters may advance the treatment of AV access stenosis. AngioSculpt® (Philips, Colorado Springs, CO, USA) is a unique angioplasty balloon with three rectangular scoring wires that spiral around the longitudinal axis of a semi-compliant balloon. The innovative catheter design promotes focal concentrations of dilating force that reduce slippage and aid in luminal expansion. In addition, the lesion scoring “effect” may lead to less elastic recoil, reducing the need for stents to maintain luminal gain.
The effectiveness and safety of PTA scoring balloons have been established for peripheral vascular stenosis of the infrapopliteal and femoropopliteal arteries.11–13 Data are, however, more limited for the use of scoring balloons to treat AV access stenosis. A recent case series (n = 16) examined the treatment of resistant and recurrent vascular access stenosis with PTA scoring balloons. 14 The authors reported fully enlarged vessels by expanding at a maximum pressure of 14 atm in all cases, without any complications. Intradialytic venous pressures decreased from 181.8 ± 39.2 to 150.5 ± 39.3 mm Hg (p < 0.0001). The case series represents the first evidence that the scoring balloon could successfully and safely treat hemodialysis patients with resistant and recurrent vascular access stenosis. Further studies that assess procedural success, safety, and efficacy may help support the treatment of AV access stenosis with PTA scoring balloons.
Thus, the current study sought to assess the safety and efficacy of a PTA scoring balloon for restoring AV fistula/graft access and to examine patency through 6 months post-procedure.
Methods
Patients and study design
In this prospective, single-arm pilot study, 50 patients were recruited at the Dialysis Access Institute (Orangeburg, SC, USA), from May 2016 through June 2016, and treated with the AngioSculpt® scoring balloon (Philips, formerly Spectranetics) to restore AV fistula/graft function.
Inclusion criteria
Patients were included:
If they had dysfunctional or thrombosed hemodialysis fistula or graft and >50% stenosis;
Patients with single lesions of any length;
Willing to consent to participation in the study.
Exclusion criteria
Patients with a life expectancy shorter than 6 months.
Eligible patients were screened for inclusion/exclusion and enrolled prior to the procedure.
Procedure
Under fluoroscopic observation, a guidewire was passed into the graft or fistula, followed by catheter placement over the guidewire to confirm the stenotic lesion. The target treatment site was verified by angiography and intravascular ultrasound (IVUS) to be in the true lumen. The appropriate size of the scoring balloon was based on the diagnostic findings. The scoring balloon catheter preparation, transit to target lesion, and inflation time were all according to the manufacturer’s instructions. The AngioSculpt scoring balloon was used without any pre-dilation. If necessary, post-scoring balloon dilation was performed using a high-pressure (non-compliant) balloon (Dorado and/or Conquest).
Endpoints
The primary efficacy endpoint was target lesion primary patency at 2 and 6 months defined as freedom from re-intervention based upon clinical assessment of function.
The safety endpoint was freedom from major device, procedure, and treatment site–related adverse events through 30 days post-procedure.
Data collection and analysis
Data on patient and procedure characteristics as well as follow-up data were collected at Dialysis Access Institute. The study, including the protocol and informed consent form, was approved by the institutional review board (Regional Med Ctr of Orangeburg and Calhoun Counties), and all patients provided written informed consent. This study was performed in accordance with the ethical principles originating from the Declaration of Helsinki and current Good Clinical Practice (GCP) guidelines and in compliance with the Code of Federal Regulations (CFR), 21 CFR 312.
Standard digital angiography was used to assess percent stenosis. Adverse events were assessed immediately post-procedure and at 1 month post-procedure. Primary and secondary patency rates were assessed at scheduled visits 2 and 6 months post-procedure at a clinical visit in which digital angiography was performed.
Data were analyzed via GraphPad Prism 7. Differences in pre- and post-procedure stenosis rates were subject to the Wilcoxon matched-pairs signed rank test. Patient characteristics were analyzed for sex-specific differences using the nonparametric Mann–Whitney or Fisher’s exact test as, respectively, stated in the “Results” section. A p value below 0.05 was considered significant.
Results
Patient characteristics
A total of 50 patients were enrolled: 23 were male and 27 were female. A majority of patients were African American (85.7%) and had a history of hypertension (96.0%). See Table 1 for patient characteristics. The average duration of fistula in use was 2.5 ± 2.1 years. Mean lesion length was 4.56 ± 1.0 mm. Female patients in this cohort were significantly older than included males. However, there were no significant sex-related differences for comorbidities, ethnicity, or lesion length. Of included patients, 42% had undergone two or more previous intervention prior to study enrollment, and 20% had undergone more than five preceding interventions. Most patients (72%) had an AV fistula hemodialysis access, while 28% were treated for a stenosed graft. Among the patients with fistulas, most had a brachiocephalic access (41.7%), followed by basilic vein transpositions (BVTs), radiocephalic fistulas (13.9%), and brachiobasilic fistulas (11.1%), while for five patients in the fistula group (13.9%), no further subclassification was documented. The majority of patients had outflow lesions (40%) or cephalic arch stenosis (24%). See Table 1 for a full listing of lesion locations.
Patient and lesion characteristics.
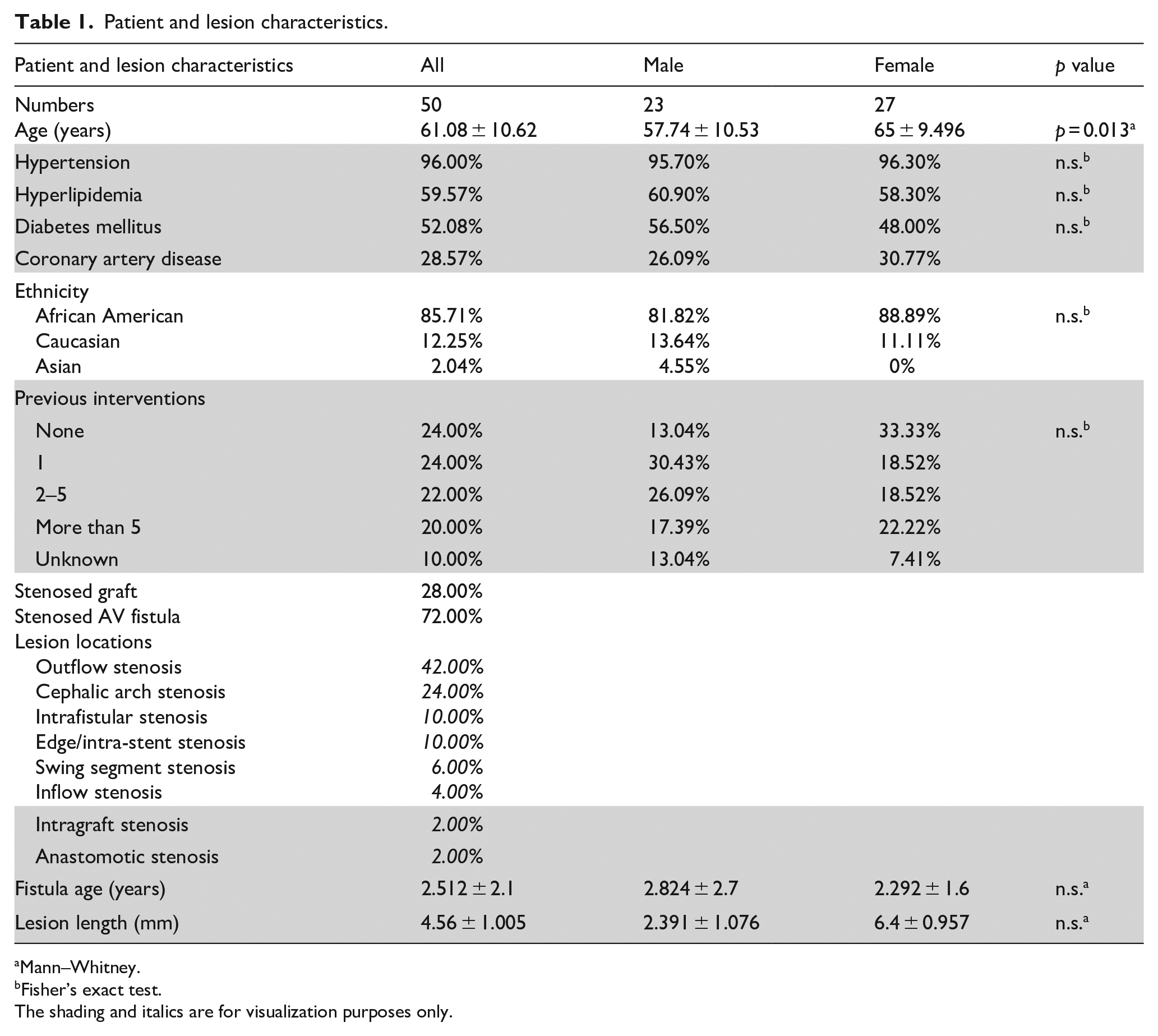
Mann–Whitney.
Fisher’s exact test.
The shading and italics are for visualization purposes only.
Procedural characteristics
Procedural characteristics are described in Table 2. The average inflation pressure was 11.4 ± 1.6 atm. There was no slippage or dissections. Nine patients (18%) received additional treatment with high-pressure (non-compliant) balloons.
Procedural characteristics.

Wilcoxon’s matched-pairs signed rank.
The shading is for visualization purposes only.
Outcomes
Immediately following treatment, a significant decrease in percent stenosis was recorded, from a mean of 78% at baseline to 7.2% (p < 0.0001). After treatment, 40% of patients displayed no visual remaining stenosis, 52% had 10% or less residual stenosis, and 8% showed 20% to 40% residual stenosis. There were no sex-related differences; average pre-procedure stenosis was 78.9% in men and 77.2% in women; and average post-procedure residual stenosis was 5.7% in men and 8.5% in women. See Figure 1 for an overview patient characteristics and initial, post-procedure outcome. In addition, we found no correlation between pre-procedure stenosis rates (Spearman rs = 0.113, p = 0.43) or initial lesion length (Spearman rs = 0.2272, p = 0.12) compared with post-treatment stenosis, indicating that achieved results were likely independent of stenosis severity.
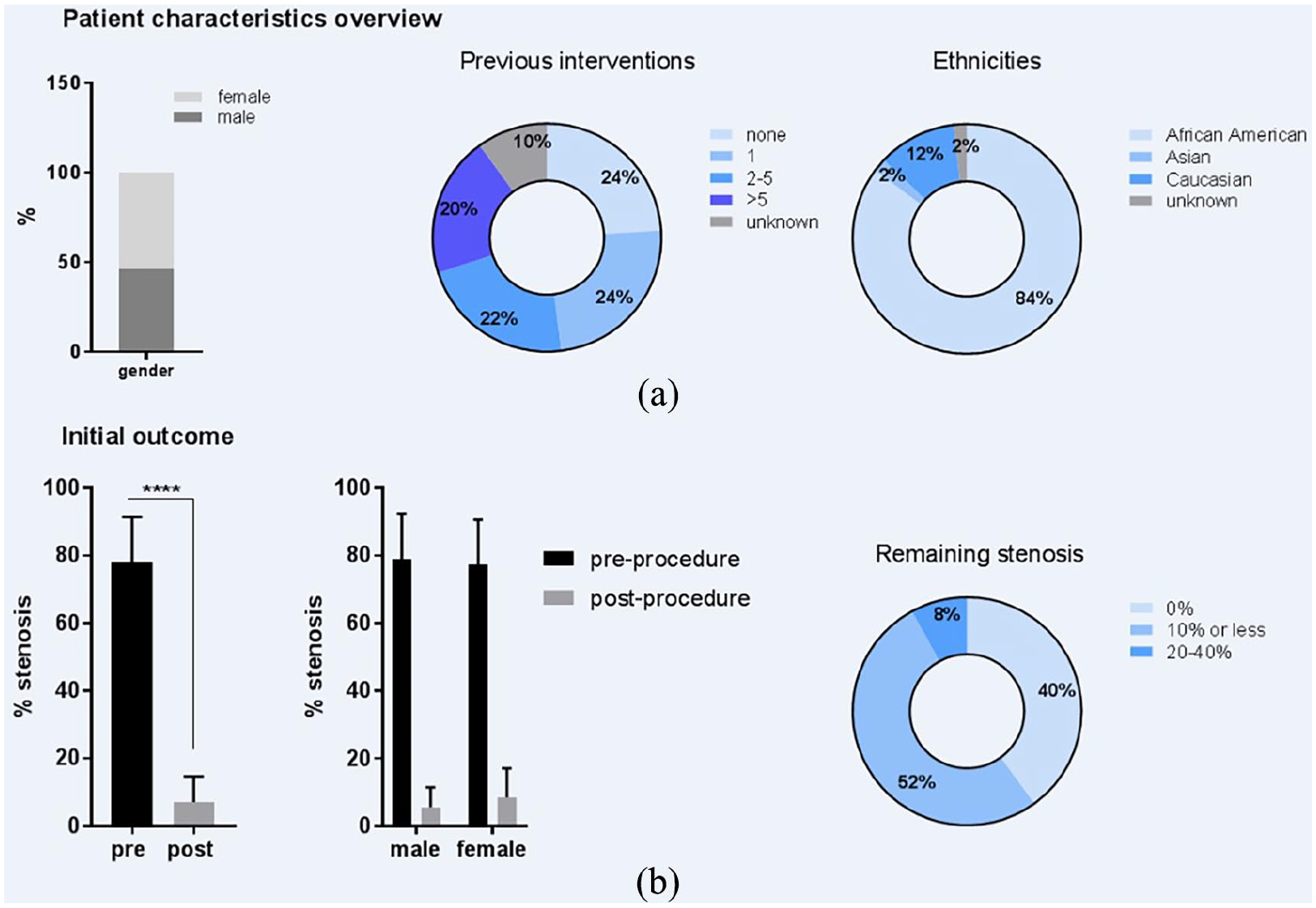
Patient characteristics and initial outcomes: (a) patient characteristics: male:female ratio, percentage of previous interventions, and ethnic background; and (b) initial outcomes: pre- and post-intervention stenosis (%), pre- and post-intervention stenosis (%) by sex, and residual stenosis (%). ****p < 0.0001.
Regarding patency (primary efficacy endpoint), the percentage of patients remaining free from re-intervention was high: 90% at month 2 and 80.9% at month 6 post-procedure (see Figure 2). Furthermore, re-interventions occurred more frequently for newly developed lesions not present at the time of the initial study procedure (54% of re-interventions occurred for new lesions).
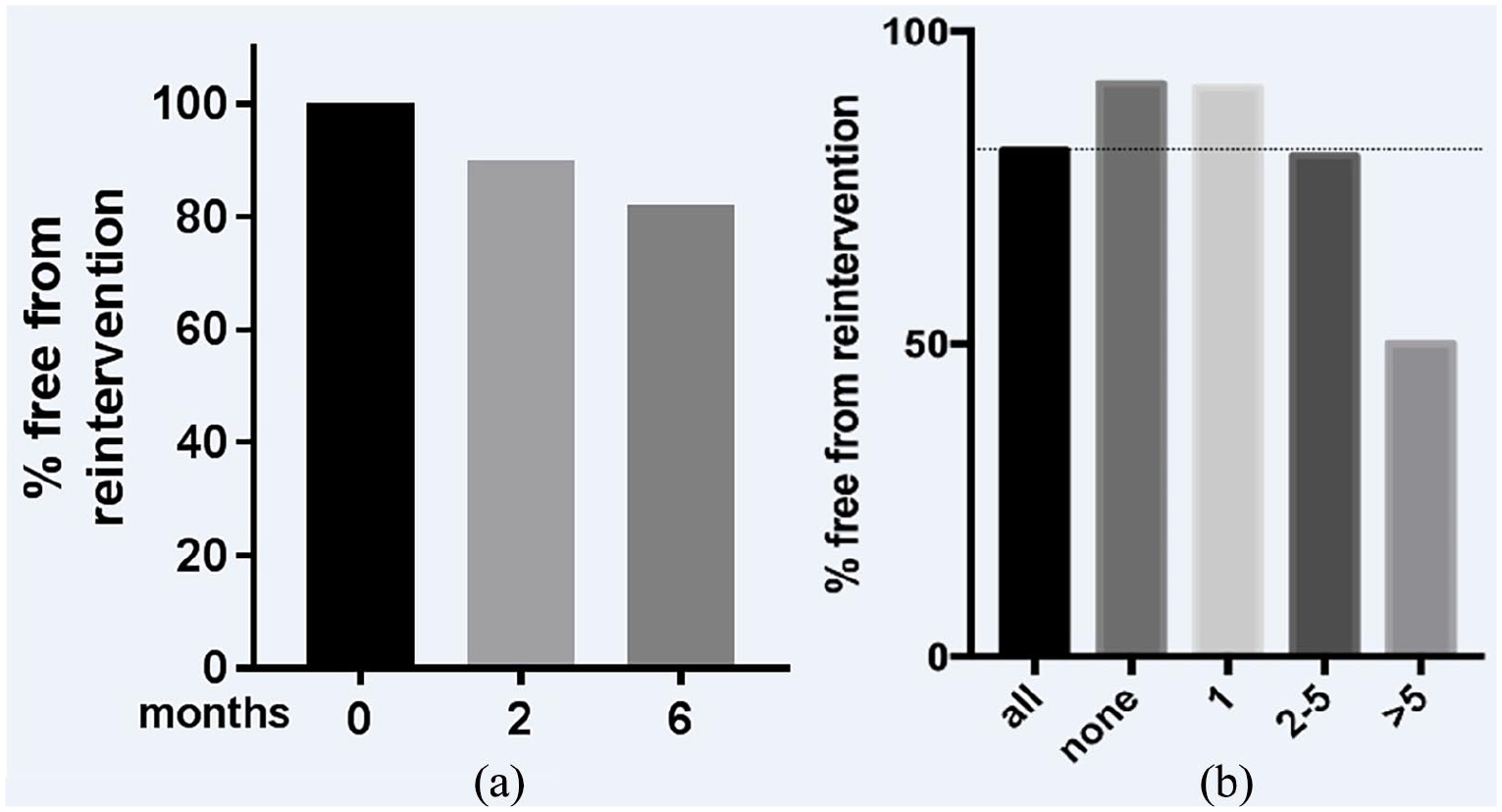
Percentage of patients free from re-intervention of total enrolled (N = 50): (a) at 0, 2, and 6 months after treatment, and (b) sub-grouping of the 6-month data according to the number of previous interventions.
When interventions were examined according to the number of previous treatments, high rates of intervention free status through 6 months were noted for patients with no previous interventions (91.6%) and patients who had one previous intervention (90.0%). Patients with two to five preceding interventions had an intervention free rate of 80% at month 6, and those with more than five previous interventions had the lowest rate of intervention free patients (50%). Lower 6-month freedom from re-intervention rates was noted for patients with grafts (71.4%) versus fistulas (83.3%). Among AV fistula patients, those with radiocephalic access (n = 5) had the highest rate of freedom from intervention (100%), while patients with brachiobasilic fistulas (n = 4) had the lowest (50%). BVT (n = 7) and brachiocephalic access (n = 15) were both slightly above the average rate of 80.9% in our studied cohort with 85.7% and 86.7%, respectively.
No device- or procedure-related complications (safety endpoint) occurred through 30 days post-procedure.
Discussion
This pilot study aimed to assess the AngioSculpt scoring balloon in restoring patency of AV fistula/grafts in ESRD patients. A total of 50 patients with stenosed hemodialysis access were enrolled, and, at 6 months, 19% of patients required re-intervention. The 6-month freedom from re-intervention rate was higher for patients with stenosed fistulas (83.3%) compared to patients with stenosed grafts (71.4%). Furthermore, 6-month patency rates were highest for patients with no previous interventions (91.6%) or one previous intervention (90.0%). Patients with two to five preceding interventions had a 6-month patency rate of 80% at month 6, and those with more than five previous interventions had a 50% 6-month patency rate.
Historically, reported primary patency rates for balloon angioplasty are quite variable. Studies have shown 6-month patency rates around 50%, 6 but some reported far lower and some reported higher rates. Pooling angioplasty results in AV fistula and grafts from 15 publications including 2166 cases showed a primary patency of 62% at 6 months. 5 A recent 2016 report highlighted 6 months AV patency rates for single lesion PTA interventions at 71.4%, while for two or more treated lesions, this number fell to 34.7%. 15 Data on cutting balloons are subject to similar variability for 6 months primary patency rates: 27.7%, 16 47.9%, 17 76%, 18 and even as high as 86% 19 have been described. Regarding drug-coated balloons (DCBs), primary patency rates are generally higher, ranging between 70% and 97%, and randomized controlled trials have shown superiority over standard balloon angioplasty. 20 While no direct comparison can be made to other treatment modalities, the results of our pilot study suggest the rates of 6-month primary patency with AngioSculpt scoring balloon may be similar to or better than rates reported for standard PTA and cutting balloons or DCB. Furthermore, there was zero slippage or dissections along with excellent immediate stenosis reduction.
Nonetheless, before considering AngioSculpt as a first-line treatment option in restoring AV access, additional data are needed. The current study is limited by a small sample size of patients with short lesions (mean: 6.4 mm), the lack of data past 6 months, and the lack of a control group. Future randomized controlled trials are needed to confirm these early results, with a larger, more representative patient sample and longer follow-up period.
Taken together, our results demonstrated an approximately 70% reduction of stenosis and suggest that AngioSculpt can be a viable treatment option to secure durable hemodialysis access through 6 months post-procedure. As mentioned, larger studies are needed to investigate its potential over longer timelines. Such studies might also include the use of a subsequent DCB. Combination therapy approaches could be a promising way to further reduce restenosis, benefiting patients and reducing costs by increasing time between treatments.
Conclusion
Results from this single-center, pilot study suggest that the AngioSculpt scoring balloon may be a viable treatment option for stenosed AV fistula/graft access, but further research from well-controlled, randomized trials is needed.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ross received a grant for this study by the device manufacturer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was an Investigator initiated research study funded by Spectranetics (now part of Philips IGTD).