
Abstract
Background:
Central venous catheter dysfunction may be associated with intraluminal clots, drug precipitates and lipid residues or extra luminal causes such as fibroblastic sleeve, tip malposition, pinch-off syndrome and venous thrombosis at the tip of central venous catheter. Failure to restore patency after addressing these causes, empirical treatment with thrombolytic agents should be considered. Urokinase is used widely as a thrombolytic agent but very few outcome studies have been published.
Methods:
A multicentre group conducted a prospective audit of management of central venous catheter dysfunction after exclusion of common causes using in centre standardised doses of urokinase from September 2017 to February 2018 in haematology and oncology units. Data of catheter blood flow were collected anonymously following administration of 5000- to 25,000-IU urokinase in dysfunctional central venous catheter.
Results:
A total of 117 patients were recruited from eight centres, 54 females and 63 males, median age was 60 (46–68). In total, 53% presented as partial withdrawal occlusion and 47% total occlusion. In partial withdrawal occlusion, patency was restored in 80% of interventions, in 82% of interventions using push lock and in 76% using dwell lock. In total occlusion, patency was restored in 88% of the interventions. The central venous catheter clearance rate was dose dependent; patency was restored in 83% of central venous catheter with 5000 IU, 89% with 10,000 IU and 92% with high dose of 25,000 IU. No adverse events were recorded.
Conclusion:
In this study, treatment of dysfunctional central venous catheter using standardised urokinase doses was safe and effective in restoring patency when no other mechanical causes could account for central venous catheter dysfunction.
Keywords
Introduction
In oncology and haematology, setting central venous catheter (CVC) is defined as any intravenous catheters mainly used for parenteral nutrition, administration of blood products or drugs and blood sampling. The use of CVC may be complicated by unintended adverse clinical events. These can be systemic and life-threatening events such as thrombosis and infection. 1 CVC dysfunction may be defined as (a) the inability to administer treatments due to total occlusive (TO) or (b) persistent withdrawal occlusion (PWO). 2 CVC dysfunction may be secondary to intraluminal causes such as clots, drug precipitates and lipid residues 3 or due to extra luminal causes such as fibroblastic sleeve, tip malposition, pinch-off syndrome, kinking of the catheter and venous thrombosis at the tip of the catheter. 4 This may limit the efficacy of the treatment, limit the longevity of the CVC and lead to a potentially life-threatening situation where the essential therapy cannot be provided.
Timely simple investigation at the time CVC dysfunction is observed can rapidly lead to proper diagnosis of the nature of obstruction. For example, progressive obstruction to flow in a patient on parenteral nutrition is often due to accumulation of lipid residue or rapid occlusion of a lumen may be due to drug precipitates when two non-compatible drugs are used simultaneously or catheter kink or catheter tip malposition. In the initial treatment of CVC dysfunction, non-pharmacological interventions such as ‘saline push’ should only be done once drug precipitates or lipid residues and catheter kink are excluded as causes of CVC dysfunction. 5 Failure to restore patency after addressing the above causes, empirical treatment with thrombolytic agents is essential if venous thrombosis at the tip of CVC or intraluminal clots are suspected as the cause of CVC dysfunction. 4
Despite the role of CVC dysfunction in negative patient outcomes of morbidity and poor quality of life, there is lack of evidence-based practice guidance for diagnosis and management of CVC dysfunction. A multicentre focus group was formed to address this issue and offer guidance in the management of CVC dysfunction focusing on the role of thrombolytic agents in the management of CVC dysfunction using standardised urokinase dose regimens. 2 Urokinase is one of the most widely used thrombolytic agents for CVC occlusions in the United Kingdom; however, there is wide variation in urokinase dose regimens. In total, 5000–25,000 IU 6 of urokinase is used for push or dwell catheter locks in most oncology and haematology centres.
Methodology
A prospective multicentre audit of current practice of the use of thrombolytic agents was carried out from September 2017 to March 2018 recording and reporting on dose regimen practice from individual participating centres in oncology and haematology in the United Kingdom. Methodology for a standardised approach has previously been proposed by a national multidisciplinary focus group which comprised relevant clinical stakeholders and included doctors, nurse consultants and clinical nurse specialists in IV therapy and oncology. 2 Urokinase dose regimens were standardised within each centre and not across all facilities. Approval from audit/ governance committees and registration of this audit was obtained from respective institutional review boards prior to data collection. Once approval was granted, patients’ consent to take part in the audit was not required, all data were collected anonymously as previous outlined in PASSPORT 1. 7 The urokinase used in this study ((Syner-KINASE®) was distributed by Syner-Med (Pharmaceutical Products) Ltd, Purley, South London, United Kingdom. Patients without non-thrombotic causes of CVC dysfunction were included in this study. In intervention 1, urokinase was administered as shown in Box 1. A total of 25,000 IU of urokinase was not commonly used in routine practice. Any patients with known history of contraindications to urokinase use were excluded from the study.
If Intervention 1 was unsuccessful the options for Intervention 2 were (a) same dose of urokinase was repeated and administered as Push or Dwell Lock or (b) the dose of urokinase was titrated up and administered as Push or Dwell Lock. In some units, urokinase Dwell Lock was left overnight (prolonged dwell) and therapy was planned for the next day.
If CVC dysfunction persisted, the decision for further administration of urokinase and/or CVC removal or replacement was based on local (in centre) protocols. Discrepancies or incompleteness of data were highlighted and discussed at individual centre level. All anonymised data were pooled and analysed by individuals blinded to and not participating in data collection. Individual patient and access device demographic data were collected at time of first thrombolytic intervention as well as any potential significant influencing factors as identified by the focus group. Separate repeating forms were populated for recording of subsequent thrombolytic interventions or any adverse events related to the use of urokinase. Categorical variables were reported as percentages and frequencies. Patient and CVC demographics, thrombolytic interventions and adverse events were recorded.
Results
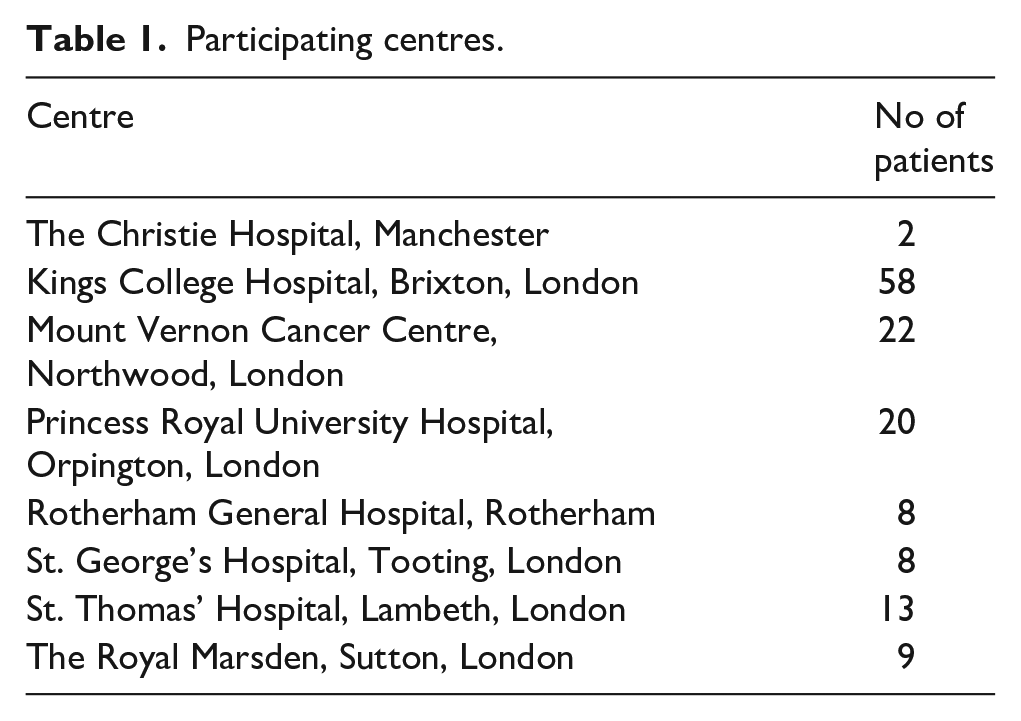
Eight oncology and haematology centres took part in the audit (Tables 1 and 2). The number and timing of interventions are shown in Figure 1. Most patients underwent one intervention (Table 3) with only 24 needing two or more interventions. The majority of patients who had second intervention had it on the same day (eight patients) or on the next day (five patients).
Participating centres.
Baseline characteristics.
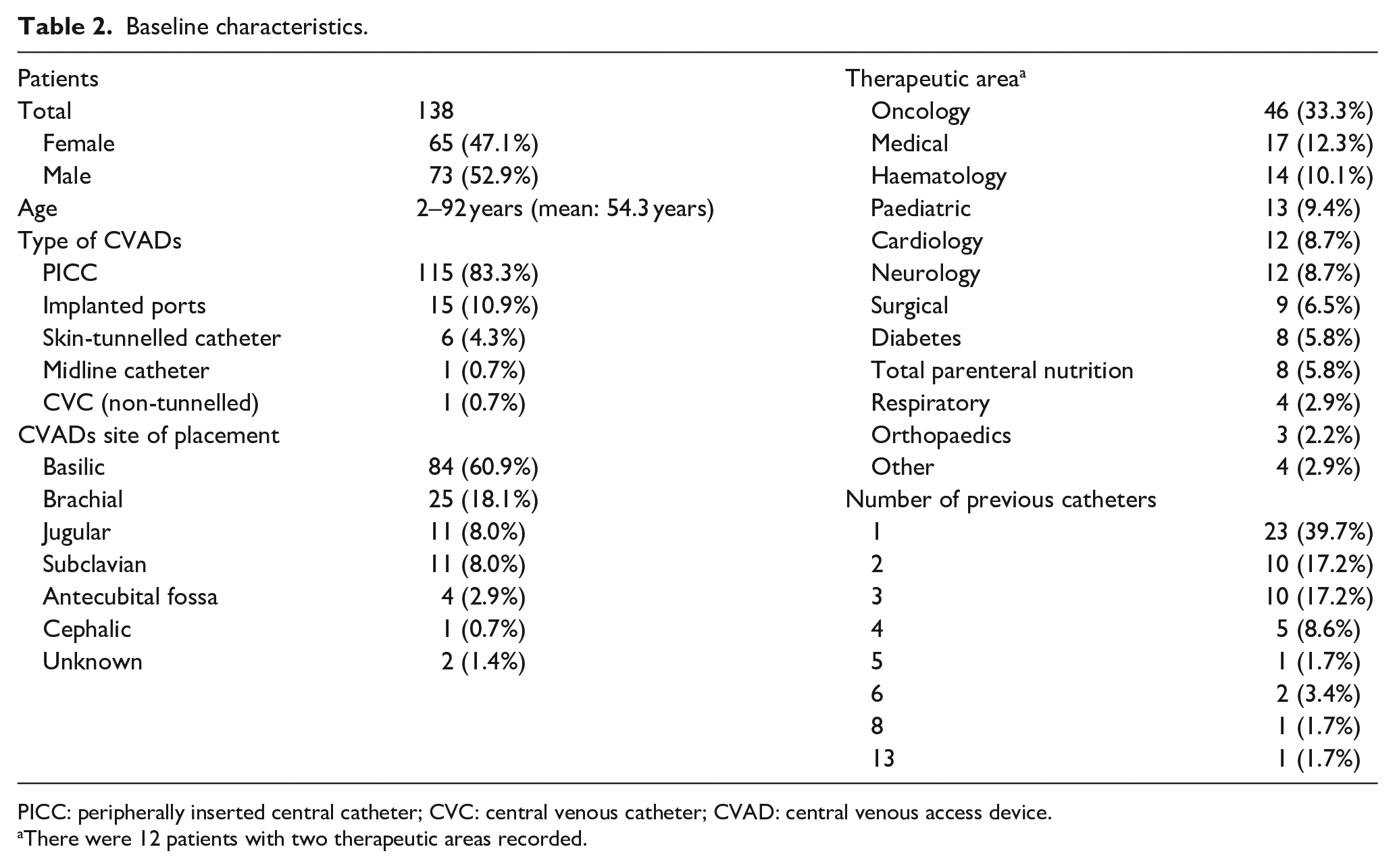
PICC: peripherally inserted central catheter; CVC: central venous catheter; CVAD: central venous access device.
There were 12 patients with two therapeutic areas recorded.
Outcomes of thrombolysis with urokinase.
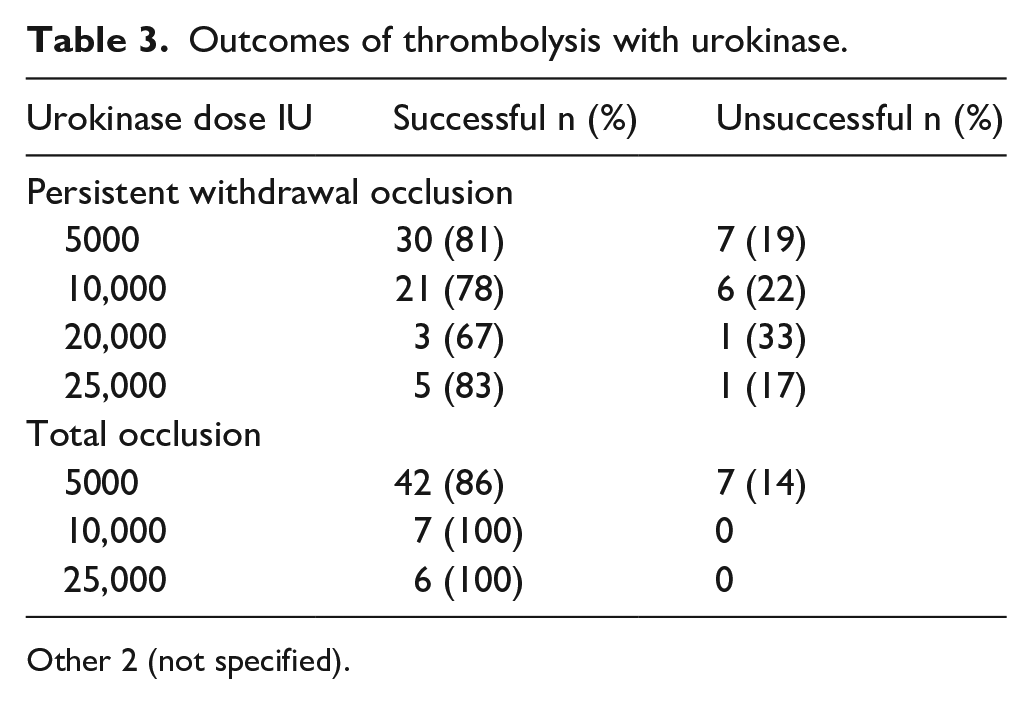
Other 2 (not specified).
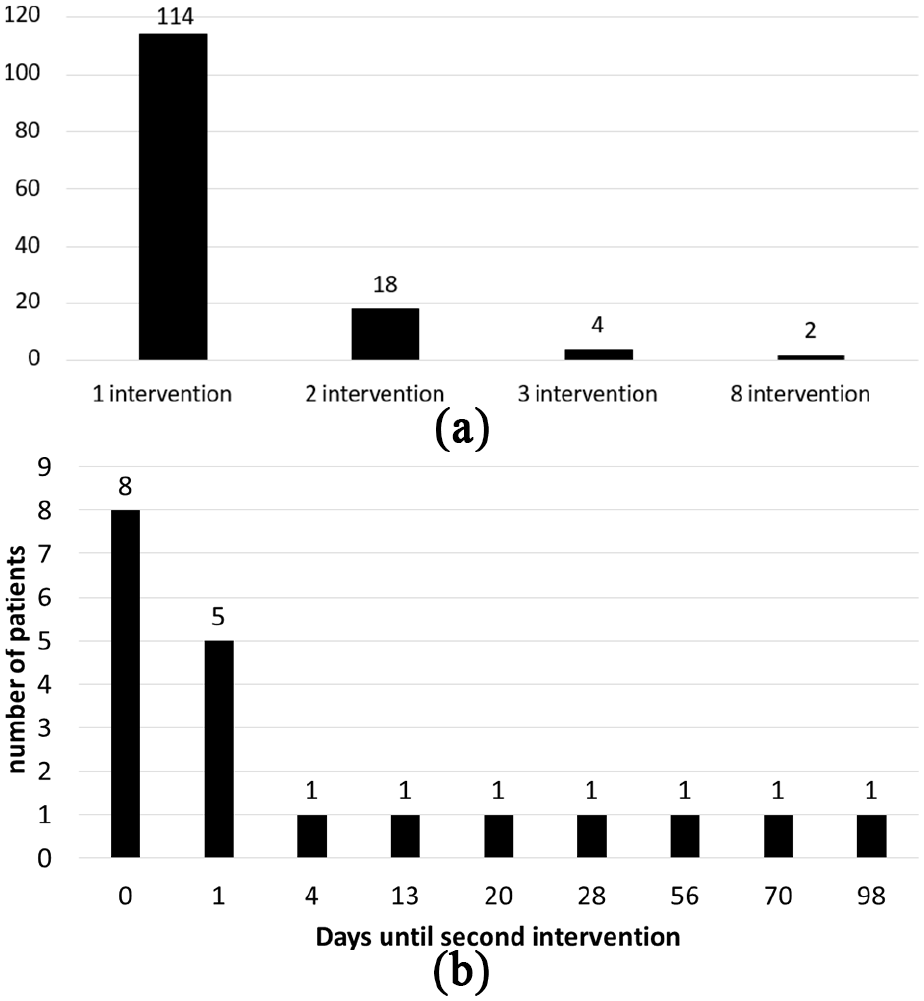
(a) Number of patients with intervention and repeat interventions and (b) days between first and second intervention.
The main types of CVCs used were peripherally inserted central catheters (PICCs) in 83.3% of patients followed by ports, reflecting the current use of CVC in oncology and haematology practice in the United Kingdom. Out of 117 patients, 53% presented as PWO and 47% TO. Overall, treatment was successful for PWO in 80% of interventions (Table 3), in 82% of patients using push lock and 76% using dwell lock.
In TO, the success rate was 89%, urokinase was only instilled in TO using 3-way tap method. In both PWO and TO, some centres left the urokinase overnight (Table 4).
Outcomes when urokinase locks were left overnight (prolonged dwell) or not.
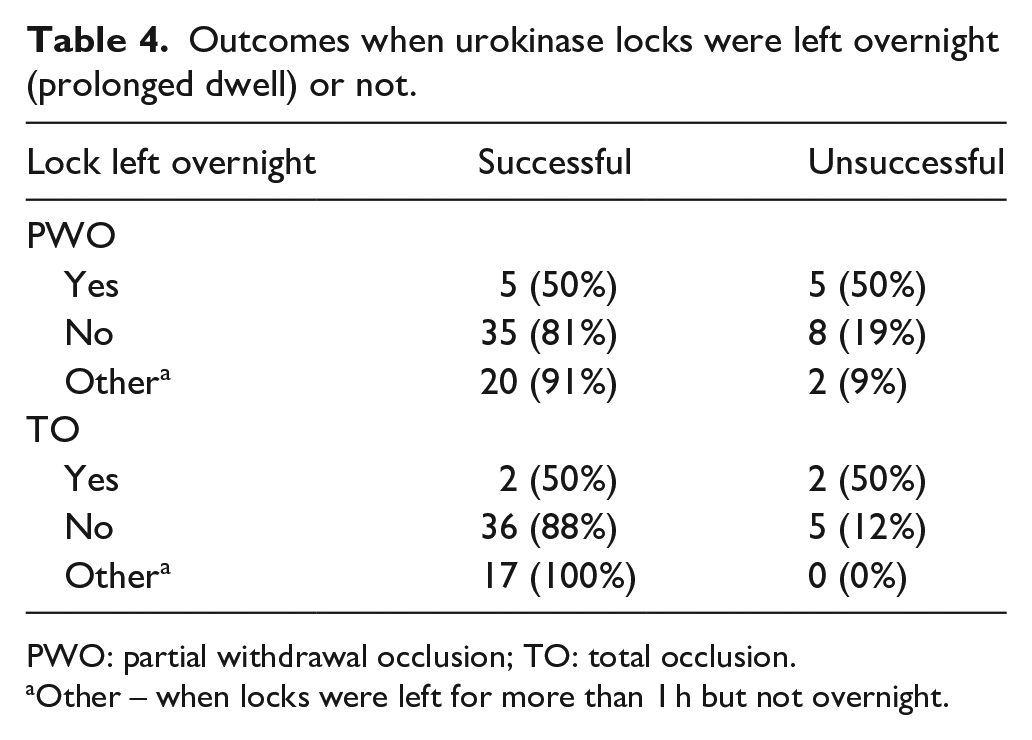
PWO: partial withdrawal occlusion; TO: total occlusion.
Other – when locks were left for more than 1 h but not overnight.
Doses of 5000, 10,000, 20,000 and 25,000 IU were used to manage PWO and same doses for TO except for 20,000 IU. Thrombolysis success rates noted in 5000-, 10,000- and 25,000-IU doses were high for both types of occlusions. No adverse events were reported throughout the duration of the study.
Discussion
CVC dysfunction may interrupt the delivery of essential intravenous therapies. This prospective study focussed on practice in the United Kingdom in oncology and haematology units in the empirical treatment with urokinase of TO and PWO of CVC when other causes of catheter occlusion such as lipid residue or drug precipitates and catheter kink were excluded. The majority of CVC PWO and TO were resolved on the first intervention either by dwell lock of push lock at doses of 5000, 10,000 or 25,000 IU. The CVC clearance rates were high using either the dwell or push locks. The success rate in PWO was 80% and in TO was 89% which was higher than success rates reported elsewhere. 9 There was no difference in success rates related to venous location of CVC, patients’ previous catheter history or number of previous CVC used per patient.
Due to short half-life, leaving urokinase within the catheter overnight is not recommended 2 ; however, in this study, several centres used this extended dwell regimen when urokinase was left in the catheter overnight until the following day. The overnight (extended) dwell was in fact less successful than shorter dwell regimen (between 30 and 140 min) for managing PWO and 1–7 h for TO. The group speculated that the extended dwell may have been successful in catheter clearance due to the fact that once the urokinase was in contact with the thrombus at the tip of the catheter thrombolysis continued as long as the urokinase did not reach the liver where it could have been metabolised. It was agreed that a separate study was required to verify this speculation.
Following these findings, the best practice protocol suggested by the experts in the form of an algorithm 2 was discussed and updated. The group agreed to implement this new algorithm in the management of CVC dysfunction in their centres. It was agreed that in all cases it was imperative to identify and exclude other causes of CVC dysfunction such as lipid residues or drug precipitates or catheter kinks before the use of thrombolytic agents was considered (Figure 2).
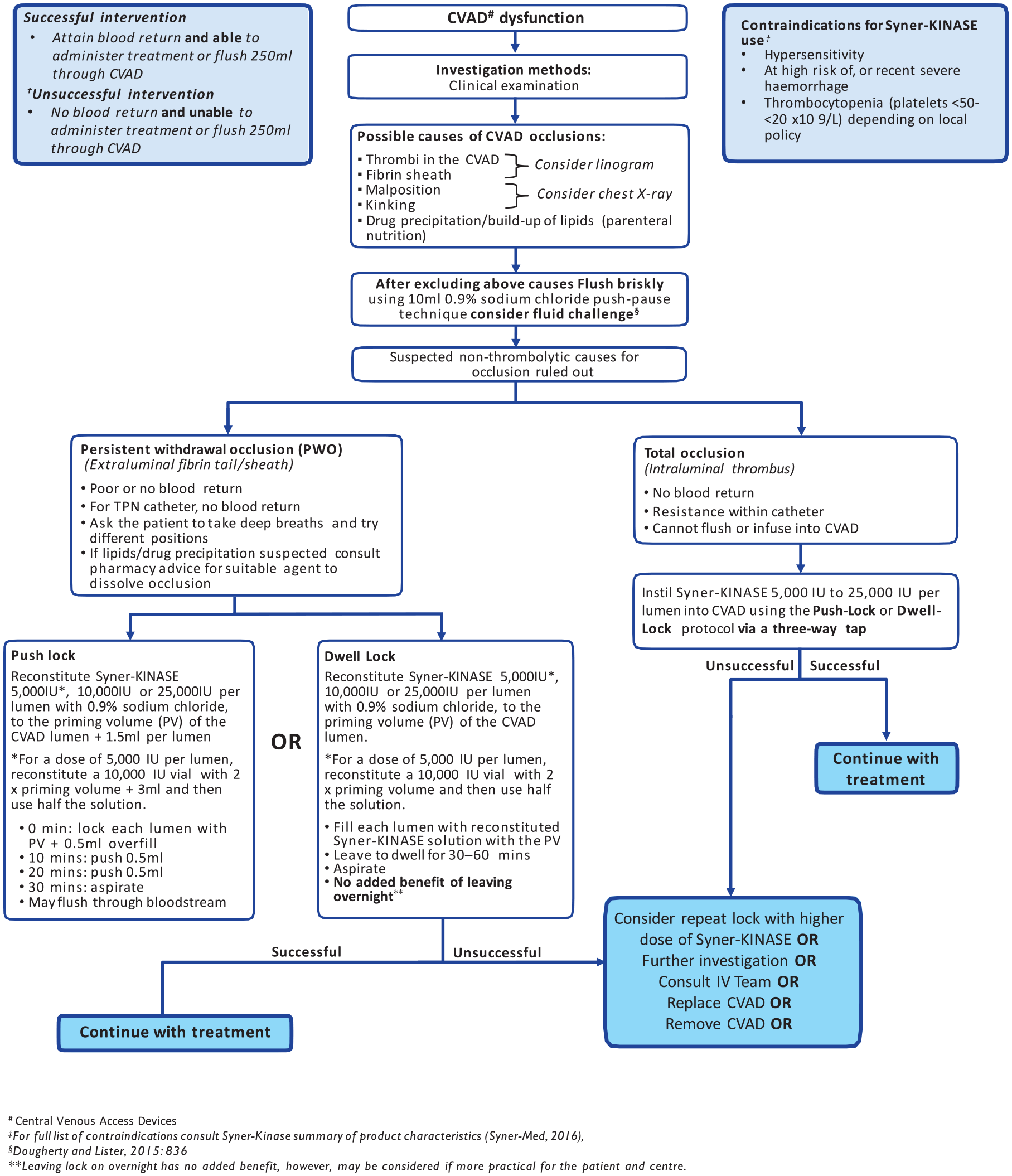
Consensus evidence-based protocol for the management of partially or totally occluded CVC with Syner-KINASE in oncology and haematology patients.
Literature review
In a literature review, Baskin et al. 9 compared published outcomes of thrombolysis with five thrombolytic agents which showed that the average catheter clearance was 52% with one dose of alteplase, 67%–74% for reteplase, 70% tenecteplase and 60% with recombinant urokinase. The overall clearance rates with second doses were 86% with alteplase, 96% reteplase, 83% with tenecteplase and 73% with recombinant urokinase. Alfimeprase demonstrated rapid catheter clearance with resolution in 40% of subjects within 5 min, 60% within 30 min and 80% within 2 h.
Ouriel et al. 10 compared three agents in an in-vitro model of catheter directed thrombolysis. They used iodine 125 radiolabelled clots that simulated those observed in the venous system which were infused with thrombolytic agents at doses analogous to those used clinically. Perfusion with heparinized, whole human blood was undertaken for 60 min, measuring the efficacy of thrombolysis through serial quantification of radio tracer released into the circuit. Fibrinolytic specificity was determined by following decrements in perfusate fibrinogen concentration. They found that streptokinase was the agent associated with the slowest rate of clot lysis (p = 0.01) versus urokinase and rt-PA. Although urokinase was associated with an intermediate rate of lysis, it appeared to be the agent with the greatest degree of fibrinolytic specificity (p = 0.02) versus streptokinase and versus rt-PA (p = 0.05). There were no differences between rt-PA and urokinase after 30 min (p = 0.05).
Schildler et al. 11 reported the use of urokinase infusion at a dose of 75,000–150,000 U/h for 24–96 h in 18 patients undergoing chemotherapy with or without autologous stem cell rescue developed CVC-related thrombosis. All individuals had a partial or complete resolution of clinical signs and symptoms. Twelve catheters were salvaged and utilised subsequently until no longer required. Six catheters were removed because of poor catheter function or re-thrombosis.
Albisetti 12 published a review of thrombolytic therapy in children; they found that complete and partial resolution rates of thromboembolic events were variable when streptokinase, urokinase and t-PA were administered as infusion. Catheter-directed use resulted in complete and partial resolution rates between 74% and 87.5%. The need to standardise the practice for CVC thrombolytic use in children was highlighted in this review.
Simon et al. 13 carried out a review of urokinase use in the prevention and management of CVC-related complications in paediatric oncology patients. They found that urokinase could be used safely and effectively in CVC with malfunctioning or with intraluminal occlusion using the dose of 5000 IU/mL or as salvage 3-h infusion with 1000 IU/kg/h.
Timsit14 carried out a study to determine the efficacy and safety of urokinase in the management of occluded PICC lines. From 28 PICC lines, 16 were treated with infusion of urokinase, 20,000 IU over 30 min. After urokinase, patency was completely restored in 93.8% (15/16) of PICC lines. No secondary occlusion or complication was noted after urokinase usage.
Recently, da Costa et al. 15 have conducted a systematic review of the interventions used to treat obstructive events in long-term CVCs in cancer patients. They found drugs used to restoration of catheter function were urokinase (53.3%), alteplase (20%), tenecteplase (13.3%), reteplase (6.7%), recombinant urokinase (6.7%) and streptokinase (6.7%). The results of meta-analysis of 14 studies showed an overall restoration rate of 84%. The drug-type meta-analysis demonstrated a success rate of 84%, 92% and 84% for urokinase, alteplase and tenecteplase groups, respectively. The authors stated that only one study reported adverse event possibly related to the drug (r-UK) characterised as minor haemorrhagic events. They concluded that thrombolytic therapy was potentially safe when used in the restoration of catheter patency in cancer patients.
In the absence of unequivocal head-to-head trials comparing thrombolytic agents, prospective validation of clinical algorithms, treatment efficacy and patient outcomes is needed to define best practice and further delineate patient risk stratification strategies. The question remains unanswered whether in oncology and haematology units, higher doses of urokinase rather than repeated low doses should form part of routine practice when first intervention is unsuccessful given that adverse events were not associated with thrombolytic therapies in both PASSPORT 1 7 and in this study.
Limitation of the study
This was a prospective audit rather than a randomised control trial (RCT), and therefore the results may not have occurred without bias. First, the participating centres reported that before recruitment into the study all patients with CVC dysfunction due to non-thrombotic causes had the appropriate treatment for these causes of CVC dysfunction before urokinase was used for thrombolysis. Before thrombolysis was undertaken, there was assumption that the main causes of CVC dysfunction were clots in the catheter or thrombus formation at the tip of the catheter. In the absence of objective measurements of CVC dysfunction such radiological imaging before and after catheter thrombolysis, the true resolution of CVC dysfunction with urokinase in the study could not always be certain. Furthermore, participating centres were not blinded and this may have affected the outcomes of interventions.
Conclusion
Long-term CVC are important for the care of oncology and haematology patients, complications such as CVC dysfunction may seriously interfere with the delivery of lifesaving intravenous therapies. CVC dysfunction is often due to simple causes such as intraluminal drug precipitates or lipid residues or clots and mechanical catheter obstruction. Once these causes are excluded, saline flush (push) should be attempted and if catheter flow is not restored early empirical treatment of CVC dysfunction with thrombolytic agents should be considered. In this study, we have demonstrated that early intervention with urokinase was safe and efficacious at restoring CVC patency, no adverse events were reported even at higher doses not commonly used in routine practice. Randomised controlled studies are required to determine optimal doses, methods of administration, duration of dwell locks and cost effectiveness of urokinase in the thrombolysis of dysfunctional and occluded CVC.
Footnotes
Acknowledgements
PASSPORT 2 link persons from participating centres for all their support with the study and data collection – Loraine Hyde: The Royal Marsden London; Jennifer Caguioa: Kings College Hospital London; Jane Hodson: St Thomas Hospital London; Brian Carey: St Georges Hospital London; Aldwin del Mundo: St Mary Hospital London; Christopher Potter: Southmead Hospital Bristol; Karen Harrold: Mount Vernon Cancer Center Northwood; Helen Summers: Tunbridge Wells Hospital Kent.
Author contributions
M.J.K., chair of steering committee and principal investigator, contributed to study design, data assessment and writing manuscript. L.D., member of steering committee, contributed to data assessment, study design and writing manuscript. A.J. contributed to data assessment and writing manuscript. S.H., investigator, contributed to study design and writing manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors attended an advisory board/panel meeting, supported by Syner-Med (Pharmaceutical Products) Ltd. and were paid an honorarium and travel expenses for their attendance.