
Abstract
Introduction:
Radial artery cannulation (RAC) is a common procedure in Intensive Care Units (ICU); radial catheters for ICU patients require increased durability to collect blood samples and to guarantee continuous hemodynamic monitoring. Failure in catheter functionality needs catheter replacement, impacting on staff workload, costs, and patient safety and discomfort.
Methods:
prospective non-randomised cohort study on adult ICU patients describing intensivists and critical care nurses’ approach in radial artery catheterization.
Results:
A sample of 103 radial artery cannulations was observed. Catheterization was performed blind in 71 patients (68.9%) and with ultrasound guidance (USG) in 32 (31.1%); majority of blind inserted RAC were at a distance between 0 and 3.9 cm from wrist joint (77.5%) while catheters inserted from 4 to 10 cm were mainly positioned with USG (84.4%). Radial catheters inserted with USG at a distance of 4 to 10 cm from wrist joint had an in-situ time double than those inserted blind (8.2 ± 7.5 vs 4.8 ± 7.3, p < 0.038).
Conclusions:
As recommended by current evidence and guidelines, USG represents a valuable support during arterial catheterization and is recommended in adult patients with clinical signs of shock, obese, swelling, and in the paediatric population. RAC in the forearm proximally, at a distance of at least 4 cm from wrist, could increase catheter durability and functionality for ICU patients. USG for cannulation in this forearm area is mandatory because of the deeper course of the radial artery.
Keywords
Introduction
Radial artery cannulation (RAC) is a common procedure in Intensive Care Units (ICU) for patients requiring frequent blood gas samples, continuous pressure monitoring, and pulse contour waveform analysis for haemodynamic monitoring. Reported arterial catheter use in United States ICU is 49.2% for patients undergoing mechanical ventilation and 51.7% for patients requiring vasopressors.1–3 Radial artery is usually the most accessed site for cannulation due to a series of advantages and a reduced frequency of associated complications, mostly related to distal ischemia. 4 An adequate collateral flow to the hand is guaranteed by the superficial and deep palmar arches joining radial and ulnar arteries in the distal forearm. A complete superficial palmar arch is reported to be present in between 43% and 97% of patients hands while complete deep palmar arch in 90% to 95%. 5 In a sample of 327 patients, radial artery diameter was significantly larger than the ulnar artery (2.45 vs 2.3 mm, p 0.0001) in 87% of arms. 5 Female population presents smaller diameter vessels. 6 Traditional blind cannulation technique by anatomical landmarks and pulse palpation has an estimated first-attempt success rate lower than 70%. 7 Radial artery catheterization may be difficult in patients with obesity, atherosclerosis or haematoma due to previous arterial punctures; weak pulse and low systolic blood pressure correlate with a reduction in success rate.8,9 Unsuccessful attempts increase the risks of haematoma formation, arterial spasm, intimal dissection, and radial nerve injury as well as patient pain and discomfort.10–12
Ultrasound guidance (USG) represents an effective support to increase efficacy in both venous and arterial cannulation. Ultrasound-guided radial artery catheterization is reported to be particularly helpful in critical patients with shock, severe hypotension, and poorly palpable pulse, as well as in paediatric patients.13,14 As suggested by White et al., there is actually sufficient evidence to consider ultrasound guidance as a best practice for radial artery cannulation. 15
Unlike arterial catheters placed in the operating room and usually necessary only for the time dedicated to surgery and post-anaesthesia recovery, arterial catheters for ICU patients require a durability of several days to ensure that blood samples can be taken and to guarantee safe and continuous pressure and hemodynamic monitoring.
Despite consistent literature reporting the advantages of USG for radial artery catheterization and on the other hand evaluating clinical complications related to cannulation procedure, factors related to increased effective catheter durability and functionality have not been well investigated. Failure in catheter functionality, resulting in a pressure waveform dampening with consequent altered or impossible interpretation of parameters and need for catheter replacement, impacting on nursing and medical staff workload, costs and patient discomfort as well, has been traditionally studied evaluating the solution used to maintain patency, flushing the lumen of tubing and catheter, and other related aspects such as flushing infusion speed and pressure applied. A systematic review published by Cochrane in 2014 suggests that a flush of 3 mL/h of normal saline solution is as effective as heparinized solutions in maintaining patency and functionality of arterial catheters. 16
Patient spontaneous wrist movements could be associated with an increased risk of radial artery catheter malfunctioning, dressing removal, and infections. 17
This research is addressed to describe the advantages of USG for RAC in critical patients admitted in ICU and the increased duration of catheters inserted distally from wrist joint.
Objectives
The main objective of this study is to analyse some variables (blind or USG technique usage, distance from wrist <4 cm or >4–10 cm) commonly applied during different individual approaches of intensivists and critical care nurses (CCN) in performing radial artery cannulation in ICU patients and their possible correlation to a longer and effective radial artery catheter functionality.
Methods
Design and setting
This paper reports a prospective non-randomised cohort study conducted in a general/surgical ICU with 9 beds and a general/trauma ICU with 10 beds at a tertiary hospital in Bologna, Italy, between May and December 2015.
Population and sample
A convenience sample of critical patients admitted in ICU requiring arterial line placement and over 18 years old was included. Catheters were inserted with Seldinger technique, using maximal barrier precautions; all catheters were 20 gauges in calibre and 8 cm in length. Ultrasound guided catheterizations were performed using a MyLab™ One ultrasound system equipped with a 13-4 MHz linear probe (Esaote, Genova, Italy). Catheterization of brachial or femoral arteries was excluded from analysis. This study is limited to radial artery catheterization in ICU patients, excluding cannulations performed for angiography and Percutaneous Coronary Interventions (PCI) because catheter differs in models, sizes, and in site duration, usually inferior to 24 h.
Variables and data collection
Primary objective of this research is to evaluate USG utilization and efficacy during RAC by intensivists and CCN and to detect if the insertion site of the catheter more proximal or distal from the wrist joint could have any impact on its duration. Secondary variables are related to catheters’ fixation technique, need for multiple daily dressings, and infectious complications.
Intensivists and CCN were free to perform radial artery cannulation according to their habits. During the manoeuvre, insertion technique (blind vs USG) and catheter insertion distance from wrist joint, measured by a paper ruler (Figure 1), were observed and recorded by one colleague or self-reported. Daily catheters variables (catheter functionality, need for repeated dressings) were assessed and reported by the nurses in charge. Systolic pressure was recorded after successful cannulation, connection of the arterial line to the ICU monitoring system and the transducer correctly zeroed. Follow-up was considered completed at catheter removal, for catheter not working or no longer required, ICU discharge, or patient’s death. Differences in time to successful cannulation between blind and USG techniques has not been considered a key variable because we considered success at first attempt and reduction of complications as a priority goal. All variables were collected in a specifically developed data collection form and subsequently transcribed into an electronic spreadsheet (Excel, version Office Professional 2016®, Microsoft Corporation™, Redmond, Washington, USA).
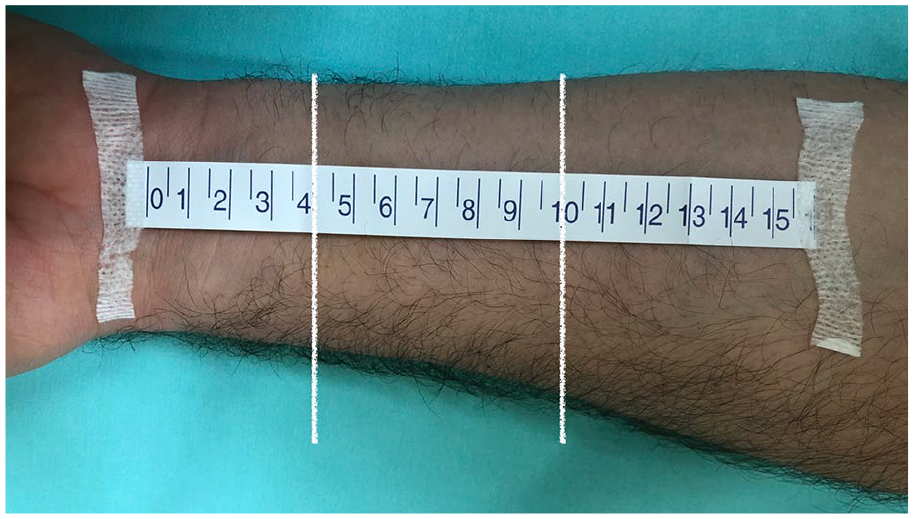
Distances in the forearm (0–4 cm and 4–10 cm).
Statistical analysis
Continuous data are presented as mean ± standard deviation; categorical variables are presented as number and proportion. Comparisons between groups were made using a two-tails Student’s t-test for continuous variables or Chi-square for categories; Mann–Whitney U-test were used to compare the effective duration of catheters. Statistical analysis was performed using GNU PSPP software, Version 2018-11-09 (Free Software Foundation). Statistical significance was defined as p .05.
Protection of human participants
This study was in accordance with the Declaration of Helsinki and its later amendments or comparable ethical standards. Data collection and treatment have been approved local Ethical Committee (CE AVEC N° 357-2020-OSS-AUSLBO). A substitute declaration of informed consent has been submitted and approved by the Institutional Ethical Committee. Data is processed anonymously and aggregated.
Results
A convenience sample of 103 radial artery cannulations was observed between May and December 2015. Catheterization was performed using blind technique in 71 patients (68.9%) and with ultrasound guidance in 32 (31.1%). USG was used as a rescue technique after failed blind cannulation in four patients. Intensivists used blind technique in 58 of 71 patients (81.7%) and USG in five patients (15.6%), three of them after unsuccessful blind cannulation. CCN used blind technique in 13 of 71 patients (18.3%) and USG in 27 of 32 (84.4%). Patient characteristics are shown in Table 1.
Patient details.
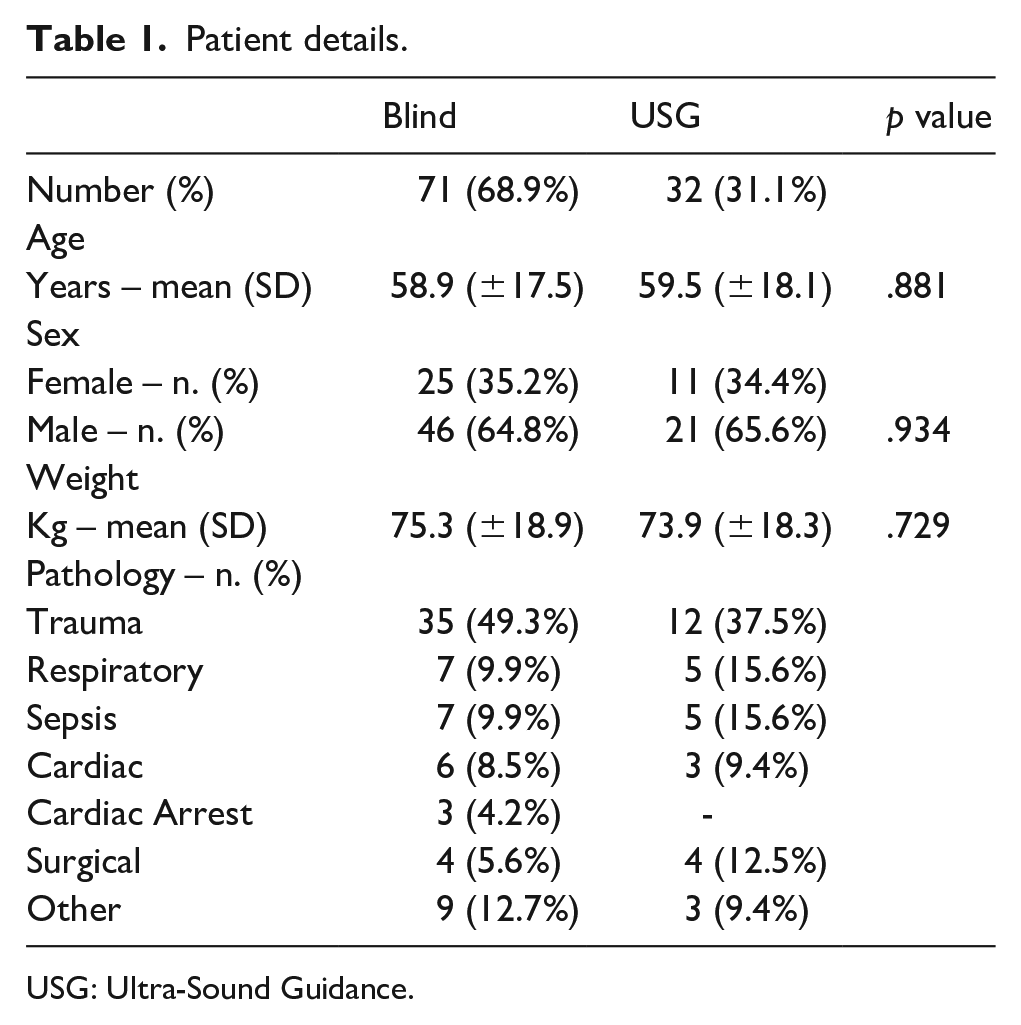
USG: Ultra-Sound Guidance.
USG increased successful catheter insertion at first attempt, particularly in patients with systolic blood pressure lower than 90 mmHg (90% USG vs 44.5% blind). The majority of blind inserted RAC were at a distance between 0 and 3.9 cm from wrist joint (77.5% blind vs 22.5% USG) while catheters inserted from 4 to 10 cm were mainly positioned with ultrasound guidance (84.4%). Critical care nurses inserted 8 RAC in the area 0 to 3.9 cm (3 USG) and 31 in the area 4 to 10 cm (22 USG). Radial catheters inserted with USG at a distance of 4 to 10 cm from wrist joint had an in-situ duration almost double compared to blind inserted catheters. Differences in techniques, distances and catheter duration between the two distance groups are reported in Table 2.
Success rate and catheter duration.
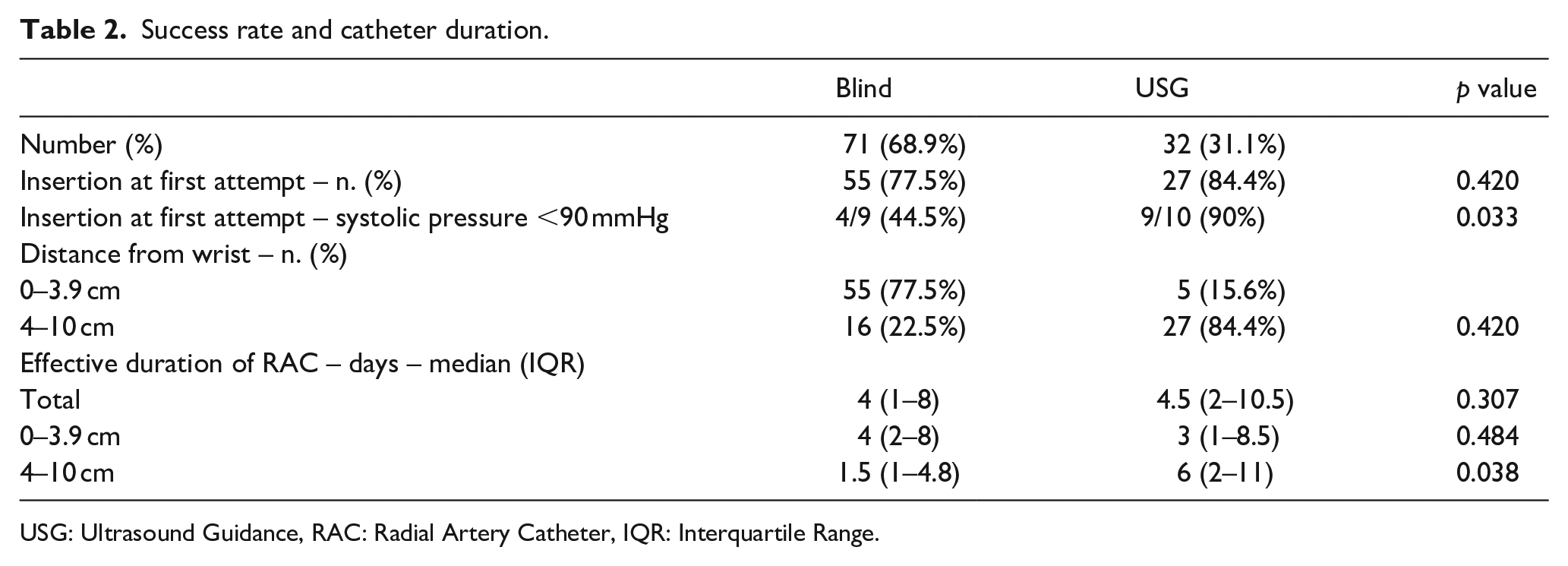
USG: Ultrasound Guidance, RAC: Radial Artery Catheter, IQR: Interquartile Range.
Catheters were fixed with sutureless securement devices in 60 patients (58.3%) and with sutures in the other 43 patients (41.7%). Need to perform more than one dressing per day was reported in 11 RAC (10.7%), all in the area 0 to 3.9 cm; catheters inserted from 4 to 10 cm did not require supplemental dressings. Only one catheter, inserted with blind technique in the 0 to 4 cm area, showed clinical signs of local infection and was subsequently removed; no signs of infections were reported in the other groups (USG and 4–10 cm area). Prevalence of infections signs in the whole population was 0.97%.
Discussion
Data from the current research agree with literature findings about the advantages of USG for RAC. USG showed a higher success rate rather than blind insertion (84.4% vs 77.5%), particularly in patients with hypotension and shock (90% vs 44.5%).
While in the last years USG was increasingly used for central venous catheterization and despite the availability of an ultrasound machine in each of our two ICU, USG for RAC was poorly used by intensivists. One of the possible reasons for not using USG for RAC may be the belief that USG is more time consuming than blind technique. Other issues to consider may be represented by the lack of a guideline or a mandatory statement at the time of the study, or by the shortage of clear evidence on the advantages of USG for RAC, considered a rescue technique after failed blind attempts. 10 The increased use of USG by CCN is likely to be due to an ultrasound vascular access training course attended in the previous months. Even if the course was addressed to venous accesses, nurses gradually acquired skills and confidence in the use of ultrasound also for radial artery cannulation, with a clear improvement in clinical practice.
Other findings show that RAC inserted at a distance of 0 to 4 cm from wrist crease have a shorter in situ duration than those inserted over 4 cm. Catheters inserted in the wrist joint area also required more dressing a day, increasing the risk for bleeding, infections, accidental removal, and affecting nursing staff workload. The deeper course of radial artery in the tract comprised between 4 and 10 cm from wrist joint presents a linear but deeper course (Figure 2 and 3). Catheters inserted in this area have a longer duration but requires USG cannulation because of the deeper course of the vessel. The higher percentage of RAC inserted by CCN are in the area 4 to 10 cm probably because nurses are aware of the advantages of this area and the risks related to wrist joint patient movements.
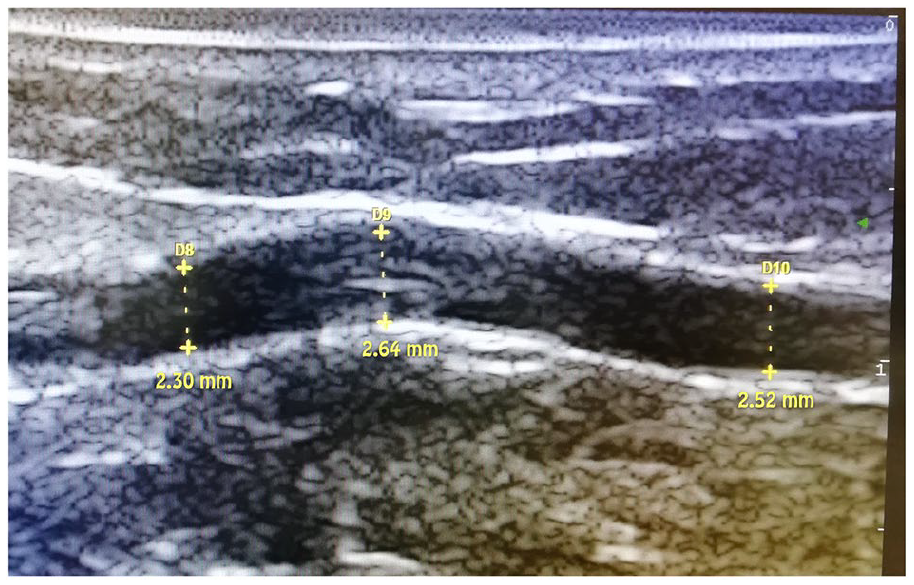
Ultrasound view of radial artery in the area 0 to 4 cm from wrist joint.
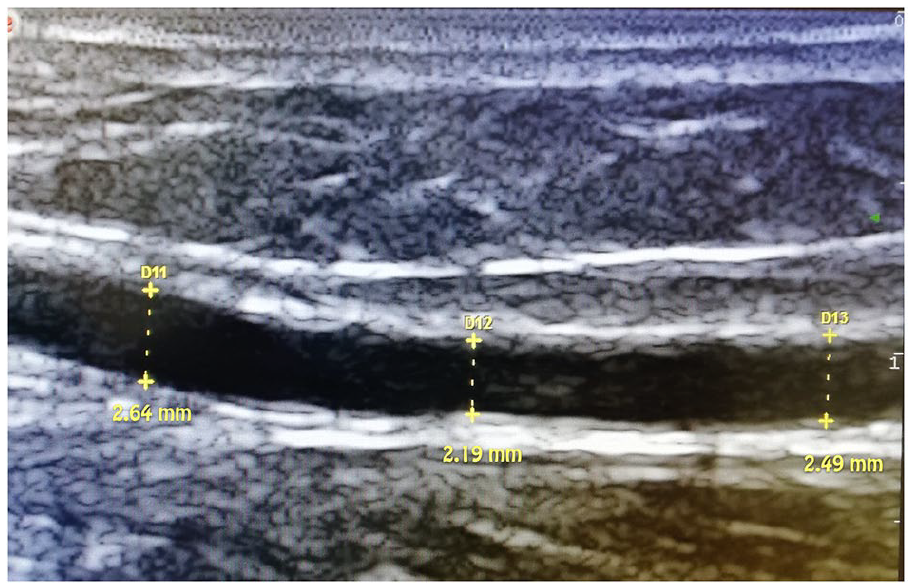
Ultrasound view of radial artery over 4 cm from wrist joint.
First-attempt success rate of blind radial artery catheterization is reported with a range from 13.8% to 68.6% in the adult and paediatric population. 7 Martin and colleagues report a 78% success rate within three puncture attempts in subjects with a palpable radial pulse. 8 Hypotension and weak radial pulse were correlated with success rates lower than 75%.8,11 Anatomic landmarks can be unreliable in locating the radial artery in up to 30% of cases and particularly in patients with severe hypotension, swelling, obesity, and atherosclerosis.5,18 Ultrasound guidance, actually considered a standard of care for central venous catheterization in adults and paediatric patients, has showed its efficacy also during arterial cannulation. While older literature and guidelines recommended USG as a rescue technique after failed blind attempts, recent guidelines are starting to consider USG as first choice technique.10,19 Even if studies and meta-analyses express controversial results on time reduction advantages in adult patients, USG radial catheterization can increase the percentage of first-attempt successful radial cannulation, reducing the number of attempts and limiting pain for patients, particularly in shock patients.7,20–23 USG arterial cannulation is recommended during peri-operative elective procedures in hypotensive, hypovolaemic and haemodynamically unstable adult patients and as a routine procedure in the paediatric population. 24 Other advantages of real-time 2 dimensional USG are represented by a reduction in haematomas formation and direct damage to radial nerve or other anatomical structures.25,26 A lower number of attempts may also be related in a reduction of catheter-related infections. 27 In-situ catheter duration is considered an important risk factor for infective complications, similar to short-term central venous catheters, with a reported incidence of 1.75% for catheter-related local infection and 0.45% for bloodstream infection (BSI). 28 The incidence of colonization of arterial catheters is lower with chlorhexidine skin preparation, as recommended by current guidelines, adequate and stable dressing and when they are positioned in ICU rather than emergency room or operating room. 25 Unlike arterial catheters used during surgery, usually removed at recovery from anaesthesia, radial artery catheterization for ICU patients requires a series of measures to ensure a longer and effective life of catheters, to ensure blood sampling, and to guarantee pressure and haemodynamic monitoring, especially when vasoactive drugs are administered. Radial catheters inserted too close to wrist joint are exposed to the risk of stress and tractions, particularly when patients present spontaneous or non-finalistic flexion movements and when physical restraints are applied to wrists. Mizukoshi et al studied the relation between radial artery height and wrist extension angle and found that excessive extension of the wrist joint angle (>60º) reduces arterial size. 29 Their study was designed to find an optimal wrist position for radial artery cannulation and they evaluated wrist joint extension but not flexion, a typical spontaneous wrist movement for ICU patients. USG allows catheter insertion above the transverse crease of the wrist, with a tract of 2.5–3.5 cm in the subcutaneous tissues before entering the radial artery, and this could play an important role in fixing the catheter and reducing the risk for infection. 23 We can hypothesize that wrist flexion movements, as well as high extension angles, could result in a reduction of radial artery calibre and blood flow, increasing the risk for thrombosis when a catheter is placed. Wrist joint movements can lead to catheter movement, irritation of arterial intima, bleeding, and haematoma formation. Bleeding of the catheter insertion site affects dressing adherence, increasing the risk for accidental removal and colonization. A similar mechanism can be found in the Red Zone, the distal zone of the arm near the elbow joint, described by Dawson in the PICC Zone Insertion Method™ for peripherally inserted central venous catheters. 30 The reduction of complications and the improvement in catheter duration and functionality suggests that a sort of Green Zone should be considered even in the forearm, inserting arterial catheters at a distance superior to 4 cm from the wrist joint. The deeper course of the radial artery in this forearm area requires USG for cannulation to ensure success and reduction of complications.
Limitations
The main limit of this study is related to a small number of RAC insertions observed on a convenience sample of patients. The main reason is that the initial design of this study was addressed to observe anaesthetists and CCN during radial artery cannulation, in order to evaluate different approaches and to elaborate a structured training program and a clinical practice protocol. A secondary analysis of collected data allowed to evaluate our hypothesis of an increased duration of radial catheters when positioned at distance >4 cm from wrist joint. Due to the initial design, some potentially relevant factors were not investigated, such as the depth of the artery placed with USG which could have contributed to a better stability of the catheter. Further research is desirable with a specifically designed study, in order to evaluate not only distance from wrist but other elements that could be related to a better functionality and durability of radial artery catheters, such as USG approaches (in-plane vs out-of-plane), arterial depth, catheter angle of insertion or the use of sutureless devices, which may result in a higher catheter angle with respect to the skin plane. Even if data insertion was conducted only by two investigators, it is necessary to take into account risk for transcription bias while transferring data from paper observation into the electronic database.
Conclusion
As recommended by current evidence and guidelines, USG represents a valuable support during arterial catheterization and is recommended in adult patients with clinical signs of shock, obese or swelling, and in the paediatric population. USG can increase success at first attempt and reduce the risk for bleeding, haematomas, and infective complications for ICU patients. Radial artery cannulation at a distance of at least 4 cm from wrist, in an area where arterial calibre, catheter, tubing, and dressing are more stable and less influenced from wrist joint movement, could increase catheter durability and functionality in ICU patients. USG for cannulation in this forearm area should be considered mandatory because of the deeper course of radial artery.
Supplemental Material
STROBE_checklist_v4_combined_PlosMedicine – Supplemental material for Radial artery cannulation in intensive care unit patients: Does distance from wrist joint increase catheter durability and functionality?
Supplemental material, STROBE_checklist_v4_combined_PlosMedicine for Radial artery cannulation in intensive care unit patients: Does distance from wrist joint increase catheter durability and functionality? by Guglielmo Imbriaco, Alessandro Monesi, Aimone Giugni and Nicola Cilloni in The Journal of Vascular Access
Footnotes
Acknowledgements
Authors would like to thank Claudia Casumaro and Michael Guadagno, students of Critical Care Nursing Master course at University of Bologna, who collaborated in the initial phase of this project. We would also like to thank our friends Stefano Bambi, for his support and encouragement, and Ken Richards, for reviewing the final English version.
Authors’ note
The forearm portrayed in Picture 1, 2, and 3 is of one of the authors, Guglielmo Imbrìaco.
Author contributions (CRediT author statement)
Guglielmo Imbriaco: Conceptualization, Investigation, Writing- Original draft preparation, Writing – Review & Editing
Alessandro Monesi: Conceptualization, Investigation, Resources, Data curation, Formal analisys
Aimone Giugni: Data curation, Writing – Review & Editing
Nicola Cilloni: Supervision, Writing – Review & Editing
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study has been approved by local Ethic Committee (CE AVEC N° 357-2020-OSS-AUSLBO). A substitute declaration of informed consent has been submitted and approved by the Institutional Ethical Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.