
Abstract
Background:
The objective of this multicenter, prospective observational study was to determine the factors related to patency rates after construction of vascular access (VA) and the first percutaneous transluminal angioplasty (PTA).
Methods:
The 24-month primary and secondary patency rates after construction of a radiocephalic arteriovenous fistula (RC-AVF) and arteriovenous graft (AVG) were evaluated using the Kaplan–Meier method and log-rank test. The 12-month post-PTA patency rate was also investigated. A Cox proportional hazard model was used to identify clinical parameters associated with the primary patency rate and the post-PTA patency rate.
Results:
A total of 611 patients were enrolled in the study. The primary patency rate after VA construction was lower in hemodialysis (HD) patients with an AVG than in those with an AVF. Aging (hazard ratio [HR], 1.02 per 1 year; p < 0.001), female sex (HR, 1.41; p = 0.03), diabetes mellitus (HR, 1.37; p = 0.03), low serum albumin (HR, 0.76 per 1-g/dL decrease; p = 0.02), and use of an erythropoietin-stimulating agent (HR, 1.62; p = 0.02) were risk factors for VA problems. The post-PTA patency rate was associated with aging (HR, 1.02; p < 0.001), diabetes mellitus (HR, 1.49; p = 0.02), polycystic kidney disease (HR, 2.14; p = 0.01), temporary catheter use for initiation of HD (HR, 1.60; p = 0.02), and period from VA construction to use (HR, 0.99; p = 0.04).
Conclusion:
Although a poor patency rate is commonly associated with advanced age and diabetes, different risk factors affect patency between VA construction and the first PTA.
Introduction
The number of patients undergoing dialysis has been increasing worldwide each year and is considered a global health concern. 1 In Japan, the number of patients undergoing dialysis reached 339,841 at the end of 2018, with the majority of these patients receiving hemodialysis (HD). 2 HD patients are known to suffer from various complications such as cardiovascular disease (CVD) and infections.3,4 The most frequent complication in HD patients is vascular access (VA) problems, including stenosis, thrombosis, aneurysm, and infection.5,6 In fact, the medical expenses for VA-related complications is estimated at JPY 10,953,310,000/year. 7 Therefore, recognition of risk factors for VA failure is needed not only to improve the quality of life of patients undergoing HD but also to reduce medical expenditure.
Several types of VA, including arteriovenous fistula (AVF), arteriovenous graft (AVG), superficial arterialization, and long-term indwelling catheters, are currently used in the clinical setting. According to several observational studies, radiocephalic-AVF (RC-AVF) is associated with fewer VA-related complications,8,9 a higher patency rate, and a better lifetime prognoses than the other types of VA. 10 These findings led to “the fistula-first policy,” which states that RC-AVF should be the first VA technique considered for the forearm.11,12 Recently, with the increasing numbers of patients with advanced age and diabetes mellitus (DM) it has become difficult in some cases to perform surgery to construct a RC-AVF. 13 In such patients, an AVG is constructed prior to the RC-AVF,14,15 raising the possibility that this clinical background may result in a higher patency rate of the RC-AVF. However, the actual effects of the VA types and background factors on the patency rate remain unclear.
Among the VA problems, venous stenosis is reportedly the most common cause of VA dysfunction,16,17 with guidelines recommending percutaneous transluminal angioplasty (PTA) as the first-line therapy. 18 However, previous studies have shown that the 12-month post-PTA patency rate is approximately 50%,19,20 and therefore repeated PTA is required to maintain VA. Physiological findings, such as those obtained by auscultation and palpation, have been used in the clinical setting for screening of VA stenosis. 21 Recently, to determine the need for PTA, ultrasound examination has been performed to evaluate not only morphological changes but also VA function in patients who may have a stenosis. 18 Therefore, the current status of the post-PTA patency rate and the risk factors for restenosis need to be determined by a large registry study.
The current multicenter, prospective, observational study enrolled 611 patients who had started HD and investigated the primary and secondary patency rates after construction of a RC-AVF and AVG. The clinical factors that affected the primary and the post-PTA patency rates were also determined. In addition, the study examined the post-PTA patency rate and the clinical factors that contributed to the development of restenosis.
Materials and methods
Patient population
Of the patients who started HD between 1 April, 2012 and 31 March, 2018 at 19 facilities in Hiroshima (Supplemental Table 1), we enrolled those who underwent construction of a RC-AVF or AVG to start maintenance HD and followed them until the end of December 2018. Patients with either a brachiocephalic AVF, long-term indwelling catheter, or superficial arterialization and those who had died or been transferred to another facility within 3 months after starting HD were excluded from enrollment. Because the study investigated the patency rate after VA construction for starting HD, patients who underwent PTA prior to starting HD were also excluded. Similarly, because the patency rate in cases with a history of AVF construction before an AVG may not be a precise assessment of patency of the graft, patients who underwent AVG construction for maturation failure prior to starting dialysis were also excluded. We provided the study information on a poster and gave the patients the opportunity to withdraw from the study. The ethics committee of Hiroshima University Hospital approved the study protocol (approval number: H-457) and the study was performed in accordance with the Declaration of Helsinki.
Study design
The study was a multicenter, prospective, observational design. The patients’ baseline blood parameters were measured immediately before the start of dialysis on the day of initiation of dialysis. CVDs included cerebrovascular disease, ischemic heart disease, and peripheral arterial disease. Valvular disease was defined as more than moderate valvular disease. Maturation failure was defined as the requirement for VA repair because of insufficient blood flow before starting HD. Patients with maturation failure underwent surgical reconstruction and were followed up regarding the VA used for the start of HD. The need for PTA was judged in accordance with the 2011 update Japanese Society for Dialysis Therapy Guidelines of Vascular Access Construction and Repair for Chronic Hemodialysis, 18 and PTA was performed at each facility. Briefly, the indication for PTA was a stenosis rate of ⩾50%, with stenosis leading to abnormal physical findings, such as low blood flow, aneurysm formation, elevated venous pressure, abnormally high blood urea nitrogen concentration or increased recirculation rate, and an unpredictable low dialysis volume. Primary patency was defined as the period from VA construction to PTA or surgical revision within 24 months, while secondary patency was defined as the period from VA construction to the date of VA abandonment. The post-PTA patency rate was defined as the period from the first PTA to the next PTA or surgical revision within 12 months. The observation periods were determined according to the reported 24-month primary patency rates of the AVF and AVG between 34% to 51% and 13% to 20%, respectively,19,22–24 the 24-month secondary patency rates of the AVF and AVG between 54% to 64% and 33% to 48%, respectively,22,24,25 and the 12-month post-PTA patency rates of the AVF approximately 50%.19,20,26 The respective patency rates were investigated in the RC-AVF and AVG groups.
Statistical analysis
The study parameters were analyzed using the Shapiro–Wilk test to confirm whether or not they had a normal distribution. Normally distributed data were expressed as mean ± standard deviation and variables with a parametric distribution as median (25th–75th percentile). The 24-month primary patency rates of RC-AVF and AVG were compared by the Kaplan–Meier method and the log-rank test. Similarly, the 24-month secondary patency rate after VA construction and the 12-month post-PTA patency rates were compared between VA types using the Kaplan–Meier method and the log-rank test. A Cox proportional hazard analysis was performed to identify the variables associated with each patency rate. First, a univariate regression analysis was performed for the parameters shown in Table 1 and those with a p value of < 0.1 were then included in a multivariate analysis. Statistical significance was set at the level of p < 0.05. The analyses were performed using SPSS software version 25.0 (IBM Corp., Armonk, NY, USA).
Characteristics of patients with or without a need for PTA or surgical reconstruction.
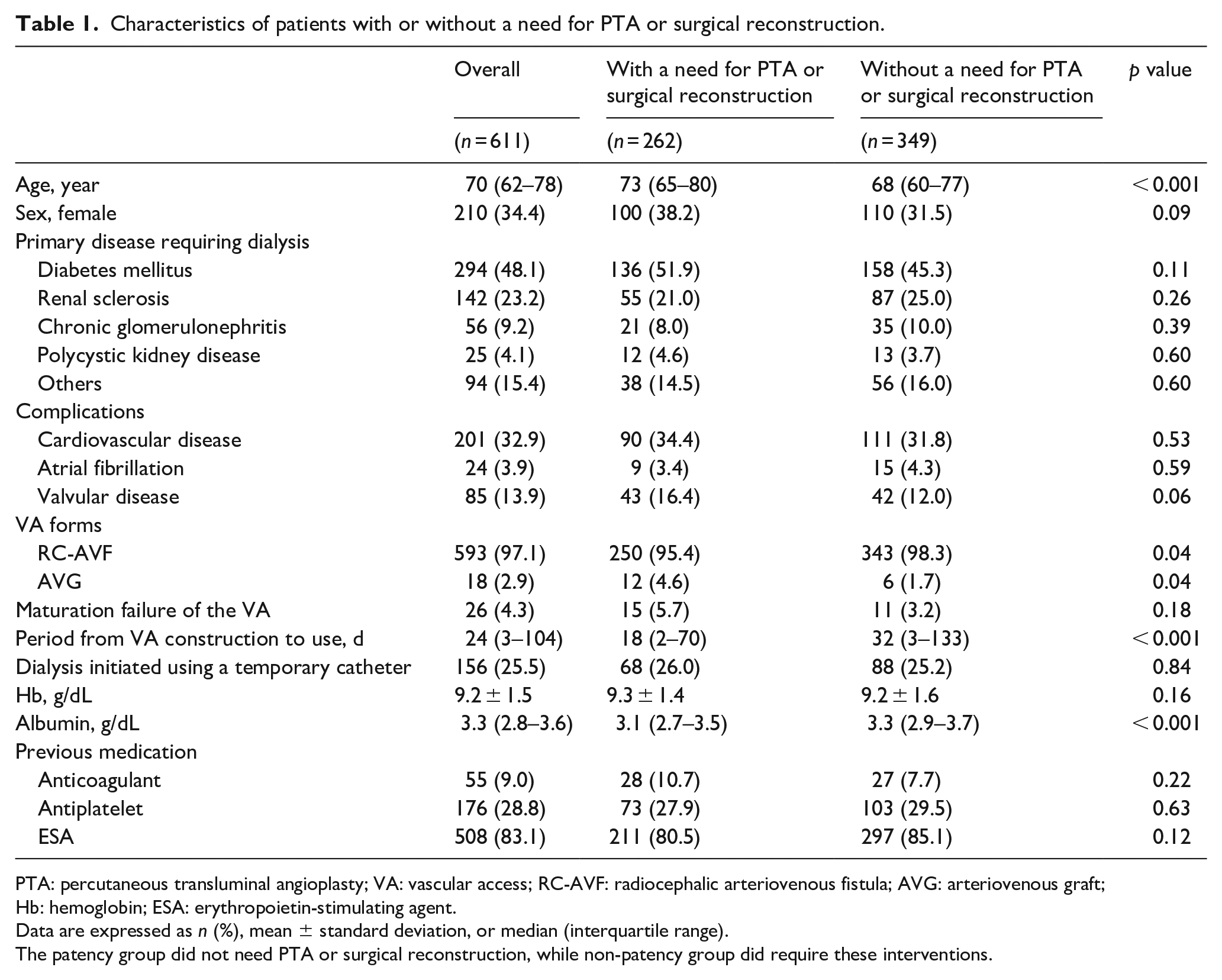
PTA: percutaneous transluminal angioplasty; VA: vascular access; RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft; Hb: hemoglobin; ESA: erythropoietin-stimulating agent.
Data are expressed as n (%), mean ± standard deviation, or median (interquartile range).
The patency group did not need PTA or surgical reconstruction, while non-patency group did require these interventions.
Results
Patients
The baseline characteristics of the patients with or without a need for PTA or surgical reconstruction are shown in Table 1. A total of 611 patients were enrolled in the study and the number of patients who started HD and underwent maintenance HD at each facility are shown in Supplemental Table 1. The variables that were significantly different between the groups were age (p < 0.001), RC-AVF (p = 0.04), AVG (p = 0.04), period from VA construction to use (p < 0.001), and serum albumin level (p < 0.001). The characteristics of the patients with or without restenosis after PTA are summarized in Table 2. Significant differences between these two groups were observed for the incidence of polycystic kidney disease (PKD) as the primary disease (p = 0.02), other disease as the primary disease (p = 0.001), and temporary catheter use for the initiation of HD (p = 0.02).
Characteristics of patients with or without restenosis after PTA.
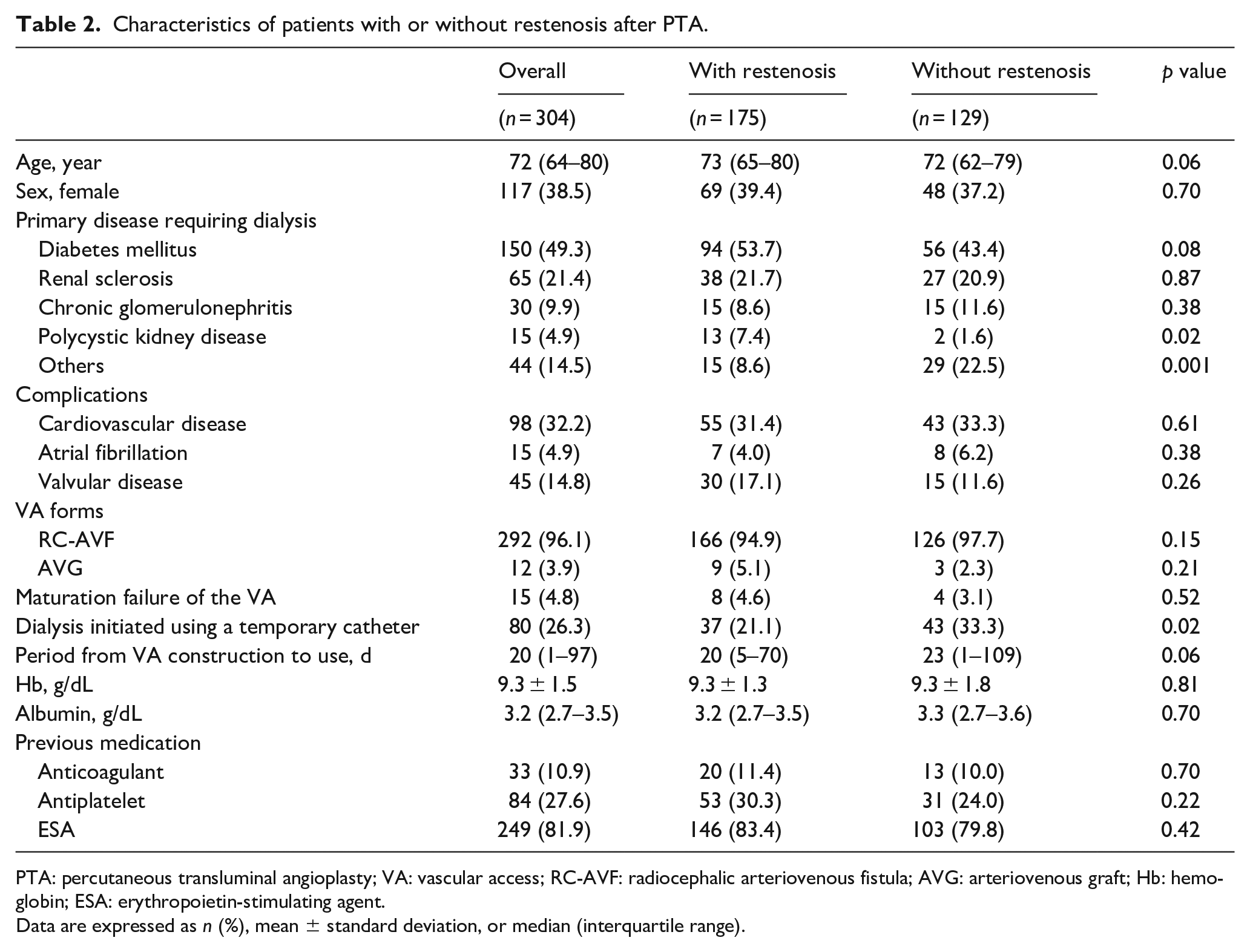
PTA: percutaneous transluminal angioplasty; VA: vascular access; RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft; Hb: hemoglobin; ESA: erythropoietin-stimulating agent.
Data are expressed as n (%), mean ± standard deviation, or median (interquartile range).
Primary patency after VA construction
The 24-month primary patency rates after VA construction in the two groups were compared using the Kaplan–Meier method and log-rank test (Figure 1(a)). After initiation of HD, 262 of the 611 patients (42.9%) required PTA or surgical reconstruction within 24 months. The Kaplan–Meier curve revealed that the primary patency rate in the RC-AVF group was better than that in the AVG group (54.5% and 25.1%, respectively; p = 0.01). The sites of stenosis are shown in Supplemental Table 2. The most frequent position in the RC-AVF group was anastomosis (39.2%), with juxta-anastomosis (26.0%) being the second most frequent. In the AVG group, most stenoses were observed at the venous-side anastomosis of the graft (60.0%).
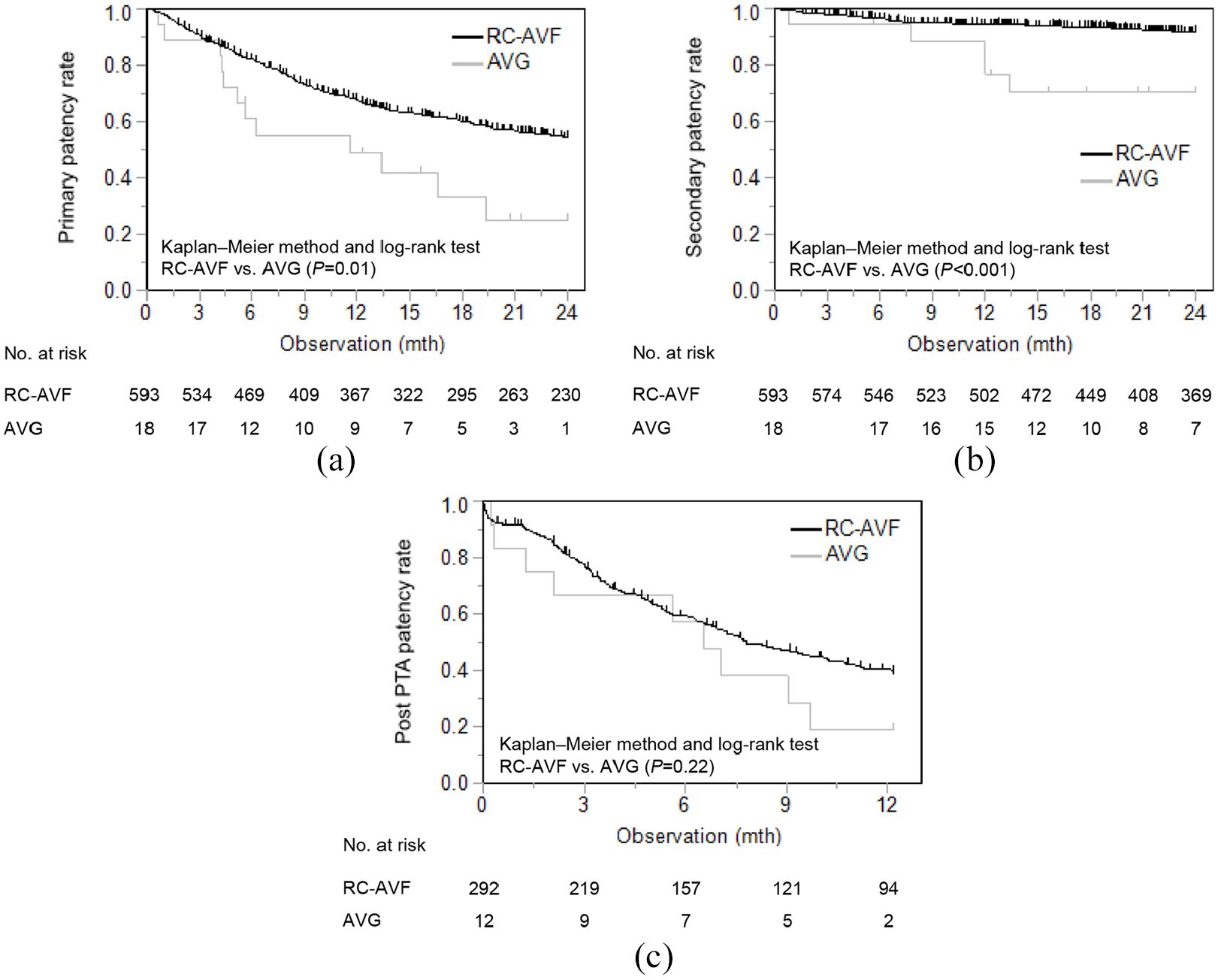
Comparison of patency rates after VA construction and PTA in the RC-AVF and AVG groups. VA: vascular access; PTA: percutaneous transluminal angioplasty; RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft. (a) Comparison of 24-month primary patency rates between RC-AVF and AVG. Comparison between the two groups was carried out using the Kaplan–Meier method and log-rank test. The black line indicates the RC-AVF group and the gray line indicates the AVG group. There was a significant difference between the RC-AVF and AVG groups (p = 0.001). RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft. (b) Comparison of 24-month secondary patency rates between RC-AVF and AVG. The black line indicates the RC-AVF group and the gray line indicates the AVG group. There was a significant difference between the RC-AVF and AVG groups (p < 0.001). RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft. (c) Comparison of 12-month post-PTA patency rate among RC-AVF and AVG. The black line indicates the RC-AVF group and the gray line indicates the AVG group. There was no significant difference between the two groups. PTA: percutaneous transluminal angioplasty; RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft. The numbers at the bottom of the figure indicate the number of patients with maintained patency for all part figures.
Clinical factors associated with the primary patency rate after VA construction
A Cox proportional hazard model was used to assess the association between clinical factors and the primary patency rate after VA construction. The presence of valvular disease, maturation failure of the VA, and RC-AVF were selected as candidate confounding variables from the univariate analysis, although no significant association for these three parameters was observed in the multivariate analysis (p = 0.16, p = 0.39, and p = 0.52, respectively). In patients with maturation failure of the VA, surgical reconstruction was performed via an anastomosis to the central side in 27 cases and creation of an AVF in the contralateral arm in 1 case (Supplemental Table 3). Aging (hazard ratio [HR], 1.02 per 1 year; p < 0.001), female sex (HR, 1.41; p = 0.03), DM (HR, 1.37; p = 0.03), serum albumin level (HR, 0.76 per 1-g/dL decrease; p = 0.02), and use of an erythropoietin-stimulating agent (ESA) (HR, 1.62; p = 0.02) were associated with the primary patency rate (Table 3).
Clinical factors associated with the 24-month primary patency rate.
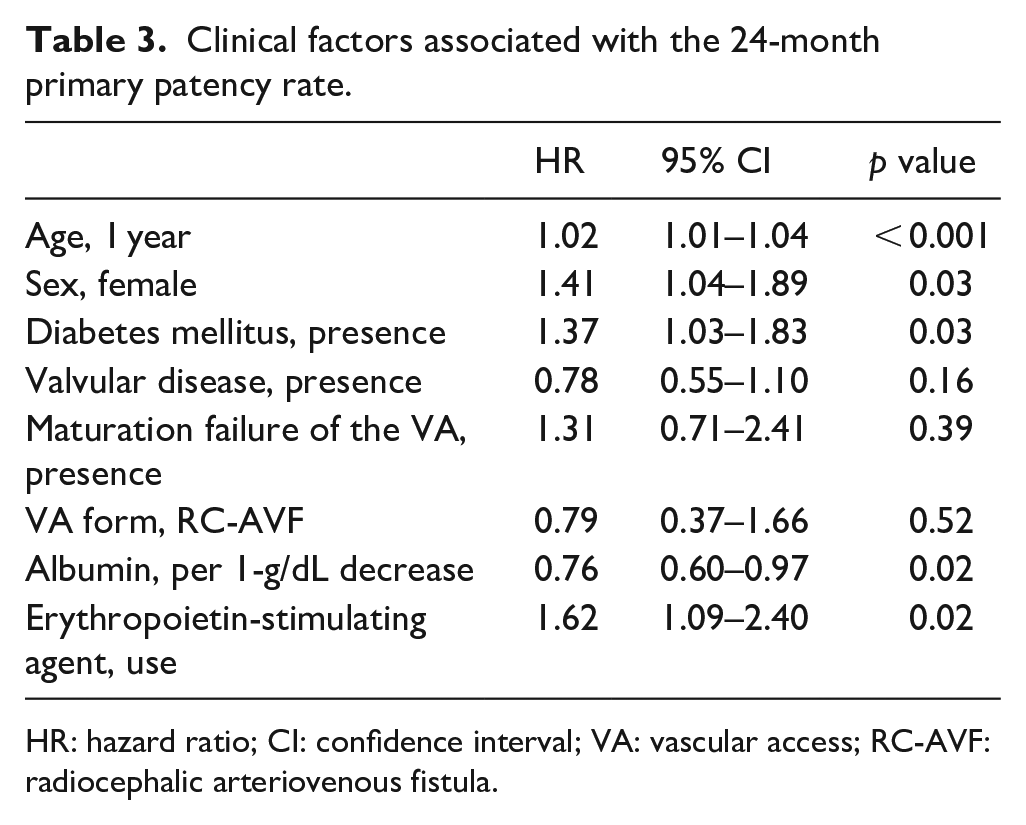
HR: hazard ratio; CI: confidence interval; VA: vascular access; RC-AVF: radiocephalic arteriovenous fistula.
Secondary patency after VA construction
The 24-month secondary patency rate after VA construction is shown in Figure 1(b). Reconstructive surgery was required in 50 of the 611 patients (8.2%) within 24 months after starting HD. The patency rate in the RC-AVF group was higher than that in the AVG group (91.6% and 70.3%, respectively; p < 0.001). The reasons for the reduction in the secondary patency rate are shown in Table 4. The most frequent reason for surgical reconstruction was stenosis in all groups. The cases that required surgical reconstruction were those in which PTA did not effectively improve VA function. These included cases in which restenosis occurred within a short period after PTA, and cases of stenosis which were resistant to PTA.
Reasons for surgical reconstruction of VA.
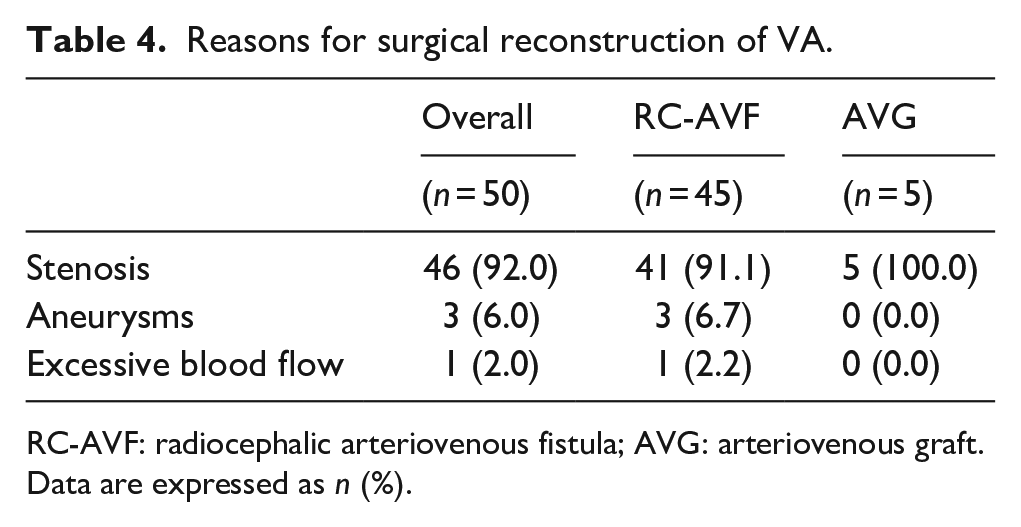
RC-AVF: radiocephalic arteriovenous fistula; AVG: arteriovenous graft.
Data are expressed as n (%).
Post-PTA patency rate
Of the 304 patients who underwent PTA after starting HD, 286 completed the follow-up, with restenosis observed in 175 of the 286 patients (61.2%) during the period of observation (Figure 1(c)). A total of 33 patients were censored due to hospital transfer (seven patients), death (10 patients), observation period < 12 months (15 patients), and taken off dialysis (one patient). There was no significant difference in the patency rates after PTA between the two groups. Multivariate regression analyses showed that the following clinical factors were associated with the 12-month post-PTA patency rate: aging (HR, 1.02; p < 0.001), DM (HR, 1.49; p = 0.02), PKD (HR, 2.14; p = 0.01), temporary catheter use for initiation of HD (HR, 1.60; p = 0.02), and the period from VA construction to use (HR, 0.99; p = 0.04) (Table 5). Supplemental Table 4 shows the characteristics of the PKD patients with or without restenosis after PTA. Age (p = 0.04) and hemoglobin (Hb) level (p = 0.002) were significantly different in the two groups.
Multivariate regression analyses of factors associated with the 12-month post-PTA patency rate.
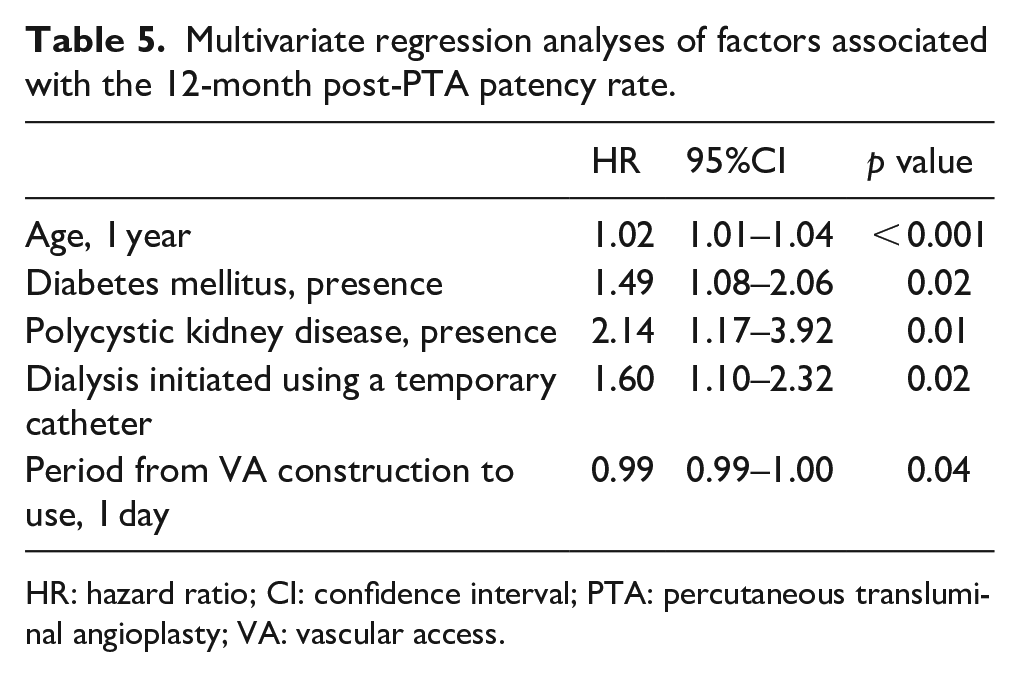
HR: hazard ratio; CI: confidence interval; PTA: percutaneous transluminal angioplasty; VA: vascular access.
Discussion
This multicenter prospective observational study used a log-rank test that showed RC-AVF exhibited better 24-month primary and secondary patency rates than AVG in patients who started HD. However, a Cox proportional hazard model demonstrated that aging, female sex, DM, low serum albumin, and use of ESA were associated with poor primary patency after VA construction, although the VA form was not associated with poor primary patency. In contrast, the log-rank test showed that the 12-month post-PTA patency rates were not significantly different between the two VA forms. In the Cox proportional hazard model aging, DM, PKD, initiation of HD with the use of a temporary catheter, and a shorter period from VA construction to use were associated with poor patency after the first PTA. These findings suggest that with the exception of aging and DM, different risk factors contribute to the incidence of VA problems after surgical construction of VA and restenosis after PTA.
The median age of the patients in this study was 70 years and about half were undergoing HD because of DM. These values are similar to the data of the Japanese Society for Dialysis Therapy in 2018 in which the patients’ median age was 69.99 years and 42.3% of patients had started dialysis due to DM. 2 These findings indicate that our data reflect the current background of Japanese patients who start HD. In addition, we showed that the respective 24-month primary and secondary patency rates of RC-AVF after VA construction were 54.5% and 91.6%, whereas those of AVG were 25.1% and 70.3%. Previous studies from other countries have shown that the 24-month primary patency rates of AVF and AVG were 34% to 51% and 13% to 20%,19,22–24 and that the 24-month secondary patency rates of AVF and AVG were 54% to 64% and 33% to 48%, respectively.22,24,25 Therefore, the 24-month primary and secondary patency rates after VA construction in Japan are better than those in other countries. One possible reason for this is that Japanese patients undergo HD with lower blood flow, 27 which may enable the VA to be used for longer periods.
Our study showed that the patency rates after VA construction between the two VA forms was not significantly different in the multivariate analysis, but did show a significant difference in the log-rank test. With respect to the post-PTA patency rate, although RC-AVF appeared to result in a better patency rate than that of AVG, the difference was not statistically significant in either the log-rank test or Cox proportional hazard model. A previous study reported that AVF exhibited a better patency rate after both VA construction and PTA than AVG.19,22–25,28 Notably, another study showed that the patency rate of AVF did not differ from that of AVG in advanced-age patients undergoing HD, especially those aged > 65 years. 29 In the present study, the median age of the patients was 70 years, suggesting that rather than the VA form, the background of the patients may be more strongly associated with the patency rate.
We demonstrated that aging, female sex, DM, low serum albumin, and the use of ESA are risk factors for a reduction in the primary patency rate after VA construction. Of these risk factors, aging, DM, and low serum albumin may indicate the poor general condition of the patients. Regarding the effect of sex on VA patency, females reportedly have a smaller vascular diameter than that of males, thereby potentially increasing VA problems. 30 In addition, it has been reported that ESA is associated with thrombosis and VA problems. 31 In previous studies, aging, DM, a higher body mass index, smoking status, higher total cholesterol level, lower protein intake, peripheral artery disease, and taking antiplatelet agents were risk factors for VA dysfunction.32–35 Taken together these results indicate that VA patency might be improved if modifiable risk factors identified in the present study are well controlled.
The current study also showed that in addition to aging and DM, the presence of PKD, the use of a temporary catheter, and the period from VA construction to use were associated with the 12-month post-PTA patency rate. Given that aging and DM were also associated significantly with the 24-month patency after VA construction, we assume a common pathway may exist that results in the progression of both dysfunction after VA construction and restenosis after PTA. Previous studies have reported that atherosclerosis is commonly associated with a decline in patency rates after both VA construction and PTA. 36 It is well recognized that the development of atherosclerosis is accelerated with aging and the presence of DM, suggesting that advanced atherosclerosis may contribute to poor patency rates after VA construction and PTA in elderly patients and those with DM. The use of a temporary catheter and the short period from VA construction to use suggests that patients need to start HD urgently. These patients may exhibit an acute decline in kidney function due to various reasons, such as sepsis, critical illness, circulatory shock, and nephrotoxic drugs, 37 which may contribute to a decrease in the 12-month post-PTA patency rate.
There is evidence from a previous study of an association between poor patency after PTA and PKD. 38 In this regard, another earlier study suggested that higher Hb levels, aneurysmal dilatation, endothelial dysfunction, carotid intima-media thickness, arterial stiffness, oxidative stress, inflammation, and hypertension may contribute to the decline of post-PTA patency in PKD patients. 39 In the present study, the Hb level and amount of ESA administered did not differ between patients with and without PKD (data not shown). In contrast, the Hb level in PKD patients with restenosis after PTA was significantly lower than that in patients without restenosis. A previous study reported that anemia predicts poor renal prognosis in PKD, 40 raising the possibility that anemia may reflect the severity of PKD. Accordingly, anemia may predict the incidence of restenosis after PTA in HD patients with PKD. Regarding inflammation and hypertension, we did not observe a significant difference in C-reactive protein levels or blood pressure between patients with or without restenosis. Another study also showed that patients with PKD had a narrow and atypical running direction of the cephalic vein. 41 Although the precise mechanism that accounts for the lower patency rate after PTA in patients with PKD cannot be clarified by a clinical study, it should be recognized that these patients are at risk of developing restenosis after PTA.
Interestingly, the present data demonstrated that a significant number of patients classified as having “other primary diseases” did not develop restenosis after PTA. This suggests that in contrast to DM and PKD, these patients have better PTA patency, although 94 patients another primary disease that included more than 20 diseases. Notably, 50 patients had an “unknown disease,” with the number of these patients almost equal to that of patients requiring HD due to chronic glomerulonephritis. Previous studies have reported that exposure to poison, alcohol consumption, and kidney injury developing in childhood are possible causes for chronic kidney disease (CKD) of unknown etiologies. 42 Additionally, although the transition from acute kidney injury (AKI) to CKD is currently well-recognized as a major cause of end-stage kidney disease, 43 renal dysfunction after AKI may be considered as an unknown etiology for initiation of HD. In any case, unknown primary disease was diagnosed when a physician did not identify an obvious systematic disease that had caused kidney dysfunction, and therefore the post-PTA patency rate may be better in HD patients who start HD due to CKD of unknown etiology.
Our data showed that stenosis accounted for 92.0% of VA problems. Previous studies have also shown that stenosis is the most common reason for VA dysfunction,16,17 and that PTA plays an important role in the treatment of VA stenosis.44,45 Pathologically, VA stenosis is characterized by neointimal hyperplasia, which is a common feature of both restenosis after VA construction and PTA.46–48 Various stimuli, such as uremia, wall shear stress caused by increased blood flow and pressure, hypoxia, and inflammation, are implicated in this process after VA construction, while balloon dilation-induced vascular injury is the main cause of restenosis after PTA.46,49 These findings suggest that the presence or absence of procedure-induced stimulation may cause differences in the risk factors that influence the patency rates after VA construction and that after PTA.
The main strengths of this study were its multicenter, prospective design, large number of clinical samples, and inclusion of only patients who had started HD. However, the study also had some limitations. First, because of the “AVF-first policy,” the imbalances in the number and characteristics of patients in the groups should be taken into account. Second, the skill of the clinicians performing the VA constructions may have influenced the choice of VA form as well as the patency rate, while operator bias may have also occurred in the selection of PTA. Third, the study protocol did not standardize aspects of the PTA procedure, such as balloon selection, dilatation pressure, and inflation time. Finally, although we excluded patients who died within 3 months after starting HD, some patients might have been in a poor general condition. Despite these limitations we contend that the resulting data reflect the actual clinical practice of VA management.
In summary, we performed an observational study to clarify the factors related to VA patency in patients who started HD and showed a significant difference between the 24-month patency rates of RC-AVF and AVG after VA construction. A Cox proportional hazard model showed that aging, female sex, DM, low serum albumin, and use of ESA were clinical factors associated with a reduction in primary patency. Conversely, the 12-month post-PTA patency rates were not significantly different between the two VA forms. Interestingly, aging and DM were both associated with the patency rate after VA construction and PTA, although other factors, such as the presence of PKD, HD induction with the use of a temporary catheter, and a shorter period from VA construction to use, were different from the risk factors after VA construction. These findings suggest that older patients and those with DM are more likely to experience VA problems after both VA construction and PTA and that different risk factors should be taken into account when managing patients undergoing HD after VA construction and PTA. Understanding the risk factors that contribute to VA problems may lead to better surveillance and focused care in high-risk patients, resulting in more effective management of VA.
Supplemental Material
Supplemental_Table_1-4 – Supplemental material for Different risk factors are associated with vascular access patency after construction and percutaneous transluminal angioplasty in patients starting hemodialysis
Supplemental material, Supplemental_Table_1-4 for Different risk factors are associated with vascular access patency after construction and percutaneous transluminal angioplasty in patients starting hemodialysis by Mahoko Yoshida, Shigehiro Doi, Ayumu Nakashima, Yasufumi Kyuden, Toru Kawai, Koichiro Kawaoka, Shunsuke Takahashi, Toshinori Ueno, Yoshiko Nishizawa and Takao Masaki in The Journal of Vascular Access
Footnotes
Acknowledgements
Clinical Trial Protocol number: University Hospital Medical Information Network (UMIN) UMIN000007655. Approval number of the ethics committee of Hiroshima University Hospital: H-457.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.