
Abstract
Background:
Little is known about the changes in hemodynamic parameters during arteriovenous (AV) access maturation using duplex ultrasound according to radiocephalic fistula (RCF), brachiocephalic fistula (BCF), and AV graft (AVG) in incident hemodialysis (HD) patient. The objective of this study was to evaluate changes and differences in brachial artery flow rate (BAFR) and related parameters affecting maturation by duplex ultrasound in incident HD patients according to access type.
Methods:
This study was an observational study conducted from March 2019 to October 2020. During the study period, 109 incident patients underwent new AV access creation, of which 100 were included in the study. The duplex ultrasound was performed on the day prior to access creation, further, day 1, 2 weeks, and 4 weeks later after access creation in incident HD patients.
Results:
Among all the patients, 38 (38%) received BCF, while 26 (26%) underwent RCF. Of the patients with AVG, 18 (50%) had a forearm loop AVG. The overall mean age was 62.2 ± 13.8 years (range, 32–89). The BAFR increased about 6.9 times in the RCF, 17.4 times in the BCF, and 19.5 times in the AVG at day 1. The median BAFR measured on day 1 was 580.4 mL/min for RC, 1029.0 mL/min for BC, and 1133.0 mL/min for AVG. Relative to the values measured in week 4, the BAFR on day 1 was 69.5% in RCF, 90.6% in BCF, and 93.9% in AVG. The acceleration decreased most significantly on day 1(p < 0.05). The acceleration time increased significantly on day 1 (p < 0.05) and beyond during maturation in the RCF and BCF. The BAFR of the RCF had a significantly negative correlation with the pulsatility index. The BAFR of the BCF showed a significantly positive correlation with the systolic and diastolic blood pressure but negatively correlated with pulse rate. The BAFR of the AVG showed a significant positive correlation with the diameter of the outflow vein.
Conclusions:
There were differences in the clinical and duplex parameters during maturation according to access type. The most dramatic changes of duplex parameters were on the day after AV access creation regardless of AV access types. Though RCF had a lower BAFR rate compared to BCF and AVG, it already had a sufficient BAFR required for adequate HD treatment the day after creation. The BAFR of BCF was not different from that of AVG.
Introduction
A functionally stable and sustainable arteriovenous (AV) access is an indispensable requirement for hemodialysis (HD) patients. However, 20%–60% of newly created arteriovenous fistulas (AVF) fail to mature for HD. 1 As such, studies on the immaturity of AVF have been actively conducted. Malovrh 2 showed that duplex ultrasound may provide useful data on preoperative morphological and functional characteristics of the vessels used for AVF creation. In addition, in several small, single-center studies, postoperative ultrasound measurements have been used to predict the clinical maturation of AVF using AV access blood flow measured in varying locations of the radial or brachial artery, or in the outflow vein. 3 However, it was difficult to compare these studies because the AV access flow measurement sites were not uniform. For this reason, we measured the AV access flow using the brachial artery during the maturation processes and evaluated the changes in the measured duplex ultrasound parameters. In addition, in AV graft (AVG), the rate of maturation failure is relatively low, so there are few ultrasound studies on its maturity. We evaluated the changes in the duplex parameters during AV access maturation and compared the differences between the hemodynamic changes related to duplex ultrasound of AVF and AVG in incident HD patients.
Materials and methods
Study design
We conducted a single-center, observational study to compare the changes in the duplex ultrasound parameters during the maturation process between AVF and AVG. We enrolled incident patients aged over 18 years receiving HD at Hallym University Dongtan Sacred Heart Hospital, Dongtan, Korea and had a newly created AVF or AVG for initial permanent AV access between March 2019 and October 2020. Patients with arrhythmia were excluded. The study protocol was approved by the Institutional Review Board of Hallym University Dongtan Sacred Heart Hospital (2020-10-006-001). There were no changes in methods after the study had commenced.
Study population
During the study period, 109 incident patients underwent new AV access creation; 100 of which were included in the study. Seven patients were excluded from the study, of which three had atrial fibrillation, three could not obtain ultrasound measurements, and one patient had severe steal syndrome. In addition, there were two primary failures. One patient underwent access ligation due to the rupture of the outflow vein several days after the operation, and the other had a reoperation due to acute thrombosis the next day after the operation, but eventually, the AV access could not be salvaged.
AV access maturation
Primary failure of AVF or AVG was defined as failure to mature adequately for HD or occurrence of access thrombosis. 4 AV access maturation was defined as successful use with two needles over three consecutive sessions in patients with AVF or AVG by a mean dialysis machine blood pump speed of >200–250 mL/min.
Duplex ultrasound evaluation
Patients who chose to undergo HD treatment were subjected to standardized preoperative mapping and postoperative AV access evaluations using duplex ultrasound, which were performed on day 1, week 2 and week 4. The ultrasound schedule was determined based on the Kidney Disease Outcomes Quality Initiatives guidelines that recommend evaluating surgical complications within 2 weeks and confirming the AV access maturity within 4–6 weeks after surgery. 1 The internal diameters of the arteries and veins were determined. Specifically, the diameter of the vein was measured at the AV anastomosis site before surgery and at 5 cm away from the anastomosis after access creation. On the other hand, using the recommended method of the time-averaged velocity integral of the mean velocity (TAVM), the brachial artery flow rate (BAFR) were measured in the brachial artery, at least 5 cm proximal to the anastomosis or above the elbow. 5 Peak systolic velocity (PSV), end diastolic velocity (EDV), TAVM, pulsatility index (PI), resistive index (RI), acceleration, and acceleration time (AT) were calculated using the Doppler spectrum used for AV access flow measurement in the brachial artery.6,7 RI was calculated by dividing the difference between the PSV and EDV by the PSV. Acceleration index was the slope of the systolic upstroke and AT was the time from the start of systole to peak systole. 8 All measurements were taken three times, and the average values were used. An experienced specialist performed all ultrasound examinations using a GE Logiq P7 (GE Electric Medical Systems, Milwaukee, WI) machine with a 12–15-MHz linear transducer for the B-mode examination and a 5.0–6.3-MHz linear transducer for the Doppler evaluation.
Surgical technique
In the case of RCF and BCF, a length of about 3 cm of the vein was dissected from the surrounding tissue and then divided at the distal end. The end of the vein was anastomosed to the side of the artery using a 7-0 polypropylene suture (Ethicon, Somerville, NJ, USA). For AVG, a straight 6-mm polytetrafluoroethylene (Advanta VXT, Atrium Medical Company, USA) was used. We used brachial artery for arterial anastomosis, and basilic or axillary vein for venous anastomosis in AVG. We created forearm brachio-basilic loop graft or upper-arm brachio-axillary straight graft creation using straight graft. AVG is first anastomosed to the vein using 6-0 polypropylene by end-to-end method, then placed in the arterial side, and then anastomosed to artery by end-to-side method. All AV access creation was performed by one experienced cardiovascular surgeon.
Statistical analysis
The postoperative ultrasonographic parameters before and after AV access creation were compared using the following methods. Patients were divided into three groups according to AV access types: the RCF, BCF, and AVG groups. Differences between the groups were examined for statistical significance using analysis of variance (ANOVA). Continuous variables were expressed as means ± standard deviations, while categorical variables were expressed as numbers and percentages. Continuous variables were compared using Student’s t-test, and categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. The relationships between the clinical and Doppler ultrasound parameters were determined using Pearson’s correlation analysis. Repeated measures ANOVA was used to test the values with multiple measurements. Multivariate analysis was used when Mauchly’s test of sphericity was not satisfactory. Results were considered significant when p was <0.05 (two-tailed). All statistical analyses were performed using SPSS, version 21.0 (SPSS, Inc., Chicago, IL, USA).
Results
Baseline characteristics of the population according to access type
Among all the patients, 64 (64%) received AVF, of which 26 (40.6%) underwent RCF. BCF (59.4%) was formed just below the elbow crease. Thirty-six (36%) patients underwent AVG creation. Of the patients with AVG, 18 (50%) had a forearm brachio-basilic loop AVG. The remaining 18 patients received the upper arm brachio-axillary straight graft.
The study subjects were grouped by access type; RCF, BCF, and AVG groups. The overall mean age was 62.2 ± 13.8 years (range, 32–89); the mean age of patients with AVG was notably higher compared to the AVF group. There were 37 female patients (37%), with the RCF group having the least number of females (Table 1). Of the total patients, 66 (66%) had diabetes mellitus, and 90 (90%) had hypertension. At the time of access creation, 59 (59%) patients were undergoing HD using a tunneled cuffed catheter. There was no difference in the ratio of patients undergoing HD treatment via catheter among the groups. Body mass index, body surface area, diastolic blood pressure, and pulse rate were significantly higher in the RCF group (p < 0.05). Systolic blood pressure was not significantly different among the groups. Diameter, flow rate, and TAVM of the brachial artery were significantly higher in the RCF group (p < 0.05). Furthermore, the diameter of the anastomosing artery was the smallest in the RCF group (p < 0.001). Meanwhile, there was no significant difference between the diameters of the BCF and AVG (p > 0.05). There was no significant difference in the size of the anastomosing vein between the RCF and BCF, but the size of the anastomosing vein was significantly larger in the AVG. The serum levels of hemoglobin and albumin did not significantly differ according to access type (p > 0.05).
Baseline characteristics of the population according to access type.
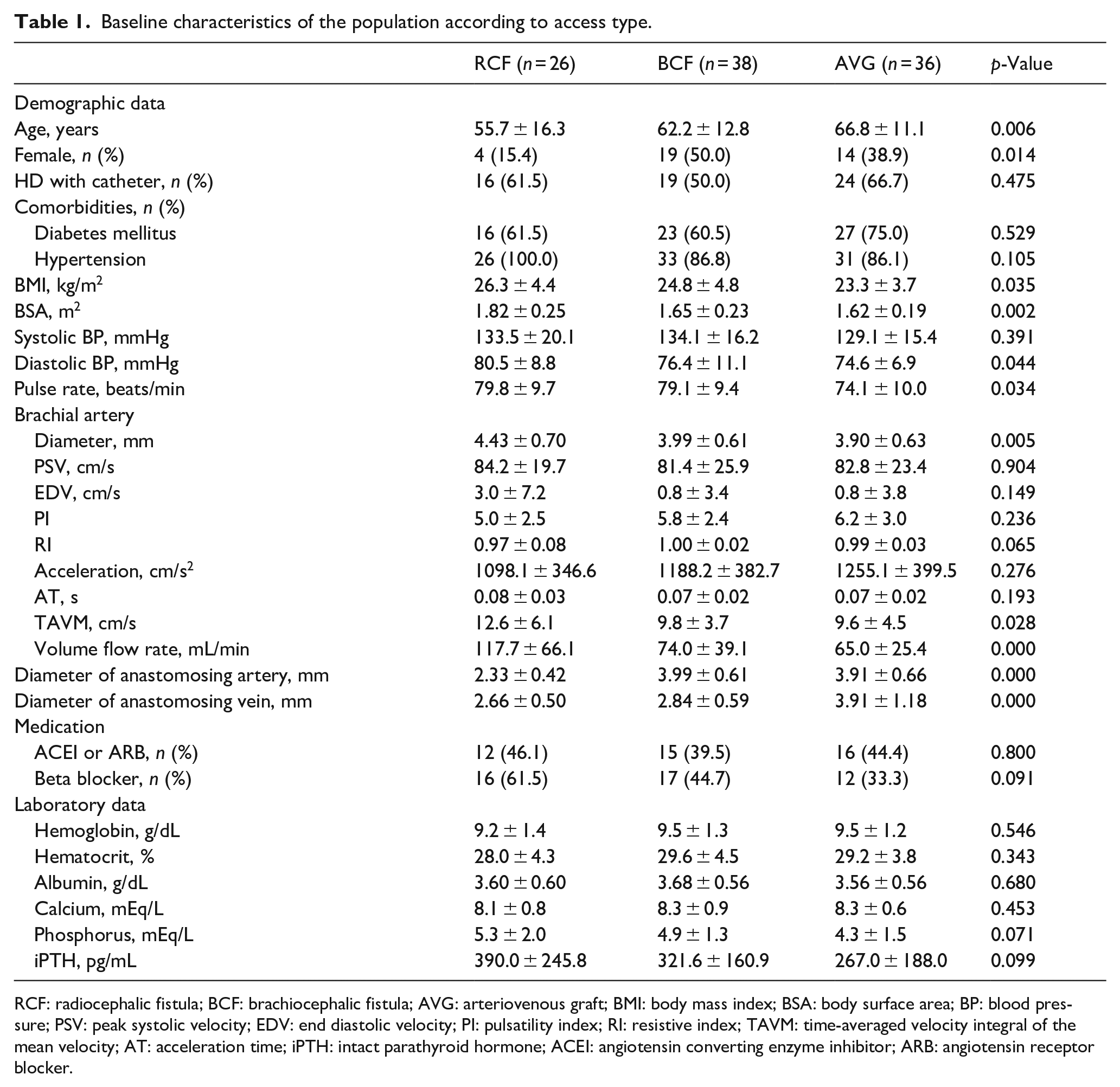
RCF: radiocephalic fistula; BCF: brachiocephalic fistula; AVG: arteriovenous graft; BMI: body mass index; BSA: body surface area; BP: blood pressure; PSV: peak systolic velocity; EDV: end diastolic velocity; PI: pulsatility index; RI: resistive index; TAVM: time-averaged velocity integral of the mean velocity; AT: acceleration time; iPTH: intact parathyroid hormone; ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker.
Changes in blood flow rate, diameter, RI, and TAVM of the brachial artery during maturation according to AV access types
On day 1, the overall BAFR increased by 15.3 ± 9.4 times compared to the preoperative period. Specifically, the BAFR in RCF, BCF, and AVG groups increased by 6.9 ± 4.5, 17.4 ± 10.5, and 19.5 ± 6.7 times, respectively (Figure 1(a)) compared to the preoperative period. Relative to the values measured in week 4, the BAFR on day 1 was 69.5% in RCF, 90.6% in BCF, and 93.9% in AVG. The BCF and AVG groups had a significantly higher BAFR compared to the RCF group (p < 0.05), but there was no difference in the BAFR between the BCF and AVG groups during maturation (p = 0.910). The median BAFR measured on day 1 was 580.4 mL/min for RC, 1029.0 mL/min for BC, and 1133.0 mL/min for AVG. The mean BAFR at day 1 of the patients with RCF that failed to mature was 369.3 mL/min. This was significantly lower than the average value of 660.5 mL/min in the patients with successful maturation (p = 0.028).
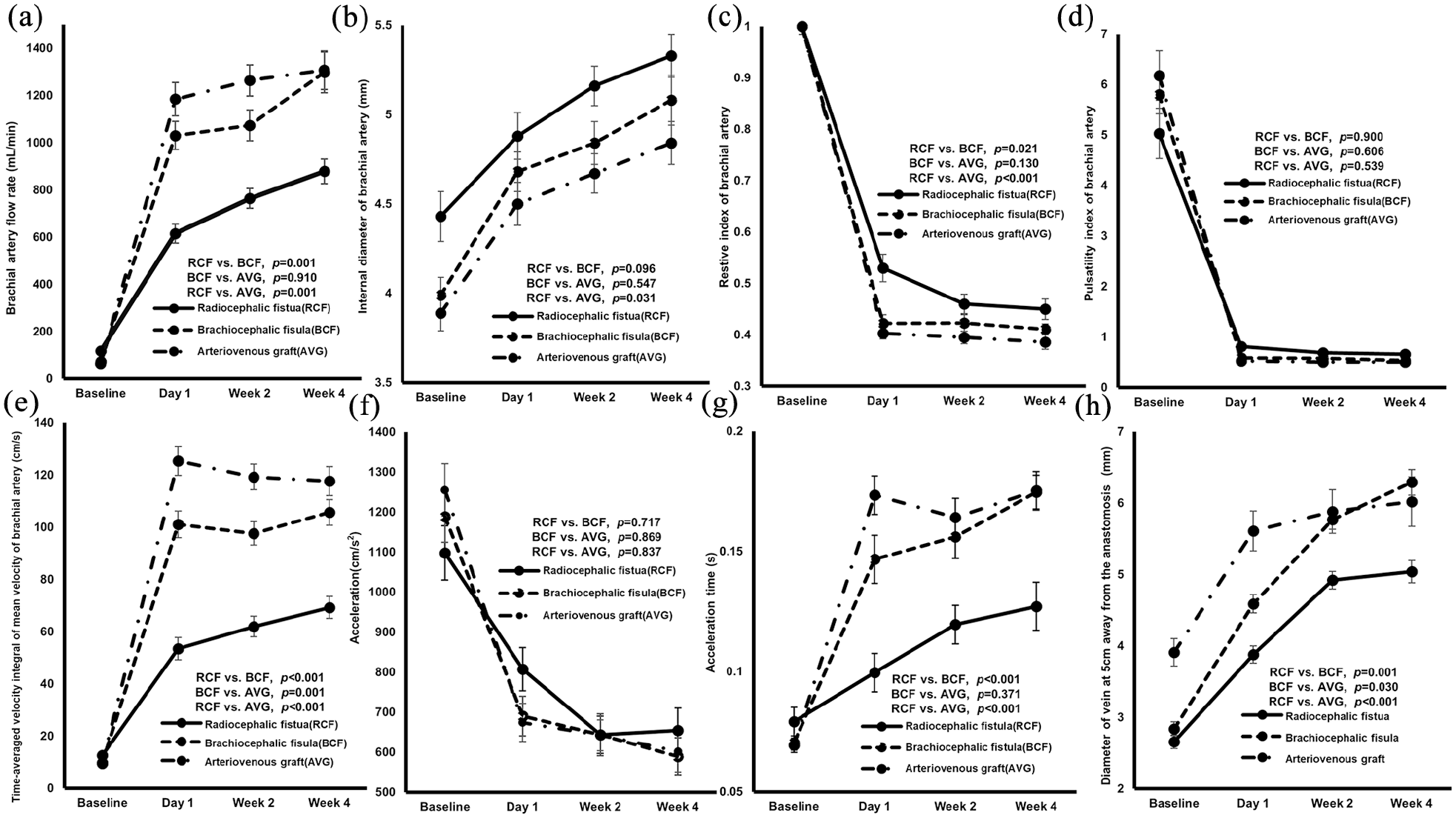
Changes in duplex ultrasound parameters measured in the brachial artery during maturation according to arteriovenous access type. (a) changes in brachial artery flow rate, (b) changes in brachial artery diameter, (c) changes of resistive index, (d) changes of pulsatility index, (e) changes of time-averaged velocity integral of the mean velocity, (f) changes of acceleration, (g) changes of acceleration time, and (h) changes of diameter of vein at 5 cm away from the anastomosis.
The diameter of the brachial artery markedly increased by 11.3% in RC, 17.0% in BC, and 16.3% in AVG on day 1, after which it increased significantly within 4 weeks (p < 0.001, Figure 1B). In the case of RCF, the internal diameter of the radial artery increased by 31.6 ± 22.9% on day 1 and by 58.4% during maturation (p < 0.001). As shown in Figure 1(c), the RI had the most notable decline on day 1 among all the access types, with the RCF group seeing a continuous decline until week 4. Similarly, the PI most markedly decreased on day 1 in all the groups. After day 1, there was no significant difference according to access type (Figure 1(d)). In the RCF group, the mean PI value on day 1 of the patients who showed maturation failure was 1.47, which was significantly higher than that of the maturation group (0.69; p < 0.001).
TAVM showed the most substantial increase on day 1 in all the groups, but only the RCF group showed a statistically significant increase in maturation (p = 0.001) (Figure 1(e)). The acceleration decreased most significantly on day 1 (p < 0.05, Figure 1(f)) and beyond, except in the RCF group. However, there were no significant differences among the groups. The AT increased significantly on day 1 (p < 0.05, Figure 1(g)) and beyond during maturation in the RCF and BCF groups.
The cephalic vein diameter significantly increased with a mean of 4.3 ± 0.8 mm on day 1 in the AVF group (p = 0.001, Figure 1(h)). In week 2, the cephalic vein diameter was 97.2% (4.9 ± 0.6 mm) and 95.9% (5.7 ± 0.8 mm) in the RCF and BCF groups, respectively, in comparison to the values in week 4.
Analysis of correlation between BAFR measured on day 1 according to AV access type and variables measured on preoperation and day 1
The BAFR of the RCF group had a significantly negative correlation with the PI measured on day 1 (r = −0.476, p = 0.016). There were no significant correlations with the other variables (Table 2). On the other hand, the BAFR of the BCF group showed a significantly positive correlation with the systolic and diastolic blood pressure, diameter, TAVM, and AT of the brachial artery, but negatively correlated with pulse rate before AV creation. The BAFR of the AVG group showed a significant positive correlation with the diameter of the vein 5 cm away from the anastomosis as measured on day 1 (r = 0.442, p = 0.012).
Analysis of correlation between BAFR measured on day 1 according to access type and variables measured on preoperation and day 1.
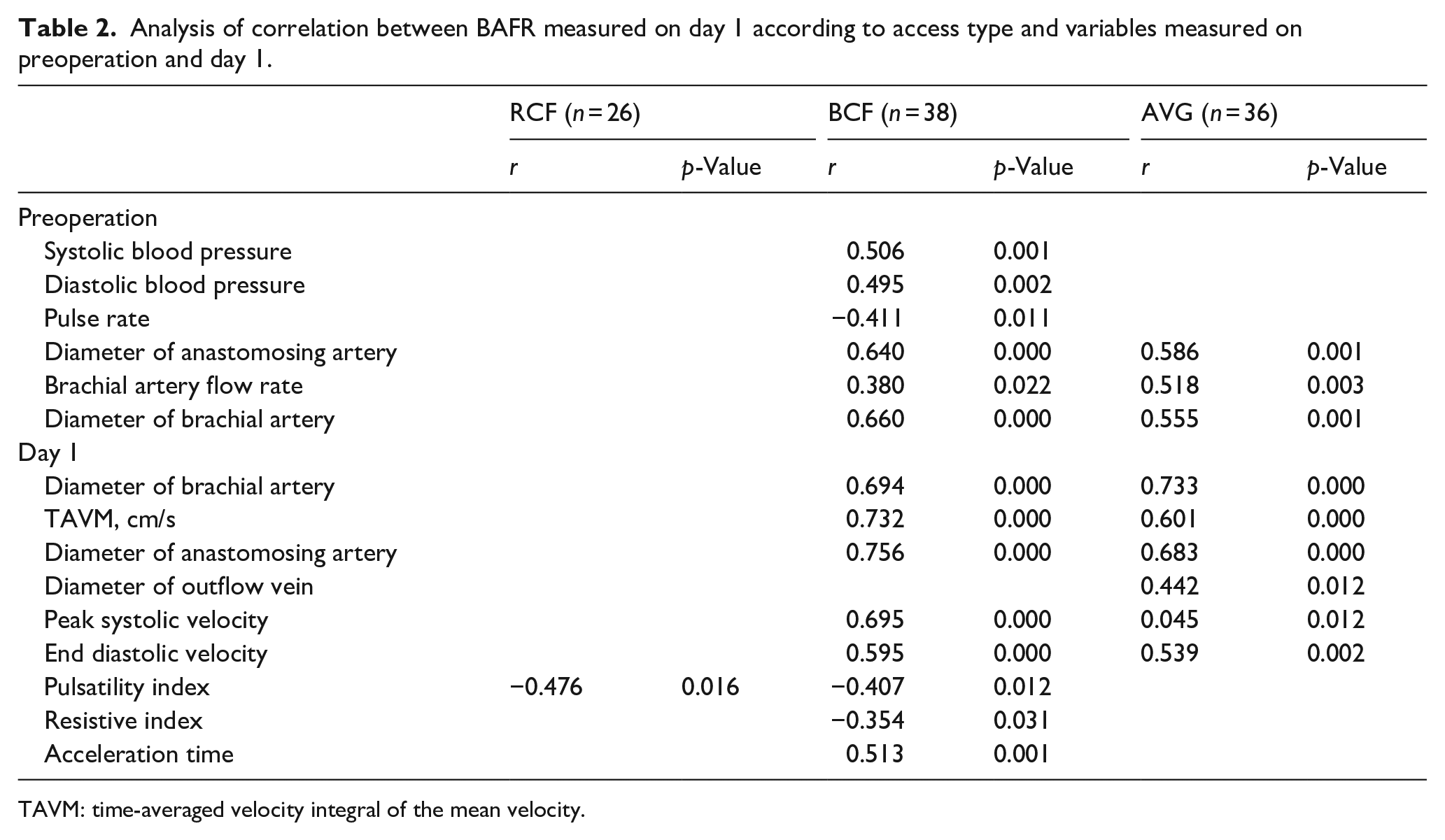
TAVM: time-averaged velocity integral of the mean velocity.
Discussion
Maturation is a dynamic process in which vascular remodeling is facilitated by the release of nitrous oxide and the breakdown of elastin to permit the enlargement of the draining vein. 9 In addition, AV access creation bypasses resistance vessels in the distal extremity and equilibrates with a low-resistance flow, which eventually increases as a result of the reduced resistance by the access. 10 The flow depends on the pressure gradient and the total resistance in the AV circuit, including the proximal artery, fistula anastomosis, and outflow vein. Flow through the anastomosing artery increases dramatically. Therefore, low increases were associated with failed AVFs.3,11 Lomonte et al. 12 reported that the most dramatic increase in BAFR occurs on postoperative day 1, accounting for approximately 50% of the BAFR in RCF at week 4. Similarly, in the present study, the greatest increases in BAFR were observed on day 1. The BCF and AVG had significantly higher BAFR compared to the RCF, but there was no significant difference in the BAFR between the BCF and AVG during maturation.
The BAFR is calculated from both the diameter and the TAVM of the brachial artery. 5 It is proportional to the fourth power to the vessel radius. 13 Because the flow rate is proportional to the radius, it is greatly affected by the diameter. Therefore, we investigated the variables correlated with the BAFR measured on day 1, according to the AV access type. In RCF, there was a significant negative correlation with the PI value measured on day 1, but there was no correlation with the diameter and the TAVM of the brachial artery. The reason for this is not known exactly, but in this study, it can be estimated that the flow rate was measured in the brachial artery, not in the radial artery. More studies are therefore needed to determine the exact reason. Meanwhile, BCF was positively correlated with the systolic and diastolic blood pressures. In addition, there was a strong positive correlation with the diameter and TAVM, while there was a negative correlation with pulse rate, the PI, and RI of the brachial artery. AVG was significantly correlated with the diameter and TAVM of the brachial artery. In addition, AVG had a significant positive correlation with the diameter of the outflow vein. The process is referred to as “maturation” after access creation, but it can be inferred that this occurs in different manners depending on the type of AV access.
Until now, the clinical implications of acceleration and AT in AV access have not been clearly elucidated. Acceleration most markedly decreased on day 1, with no significant difference until week 4, except for RCF. AT increased significantly on day 1, with RCF and BCF showing significant differences. In addition, The AT measured on day 1 showed a significant positive correlation with BAFR measured at the same time. While the clinical significance of acceleration and AT was not clearly established in this study, the determined trends on these values during maturation may still be helpful to future researchers.
The vein diameter ratios at day 1 and at 4-week were 79.4% (3.9 ± 0.6 mm) and 80.1% (4.6 ± 0.7 mm) for RCF and BCF, respectively. Furthermore, the cephalic vein diameter on week 2 increased by 97.2% (4.9 ± 0.6 mm) in RCF and by 95.9% (5.7 ± 0.8 mm) in BCF, compared to the value measured in week 4. Similarly, Robbin et al. 7 showed that most AVF veins, even in the forearms, reached at least 0.4 cm within 2 weeks. In other words, a successful AV access could have sufficient BAFR for HD treatment even after just a day from creation. However, the diameter of the outflow vein only becomes large enough to be punctured after at least 2 weeks. In clinical practice, cannulating an AVF sooner than 2 weeks after its creation has been associated with a 2-fold increased risk of AVF failure. 7 After 2 weeks, it is crucial to wait for the vein wall thickness and subcutaneous tissue of the cannulation site to become strong enough to withstand the repeated cannulation with HD needles in AVF. Since AVG can also have a sufficient flow rate for HD within a day after access creation, the time required after that is a period for stable regular cannulation due to engraftment of the graft.
Robbin et al. 7 has previously suggested that Doppler ultrasound measurements at 2 weeks after access creation may be of value in identifying earlier the fistulas that are unlikely to mature optimally. Similarly, in this study, the ratios of the BAFR on week 2 to that of week 4 were 86.7% in RCF, 89.9% in BCF, and 98.3% in AVG. In addition, the BAFR and the PI at day 1 in patients with maturation failure were 369.3 mL/min and 1.47, respectively, in this study. Therefore, if the BAFR on the day after access creation is less than 369 mL/min or the PI value is greater than 1.47 in patients with RCF, it would be prudent to immediately find and correct the cause. In the case of BCF, if adequate BAFR cannot be maintained for up to 2 weeks after access creation, it should be corrected through immediate cause evaluation. As for AVG, if sufficient BAFR cannot be maintained the next day after access creation, corrective intervention without delay is necessary. Waiting for several months in anticipation of access maturation should be avoided as it can increase the frequency of complications and unnecessary catheterization in patients with end-stage kidney disease.
This study had several limitations. First, this was a single-center study with a small sample size. Second, an observational study may only provide an associative link but not a causative link; therefore, we cannot rule out the possibility of unmeasured confounding factors that could have influenced the AV access maturation. Third, it would have been more useful if information on the thickness of the outflow vein over time had been identified, but we did not have the equipment to measure the thickness of the vein accurately.
In conclusion, there were differences in the clinical and duplex parameters during maturation according to access type. AV access showed the most dramatic changes in duplex parameters on the day after creation regardless of access type. Though, RCF had a lower BAFR rate compared to BCF and AVG for maturation, but it already had a sufficient BAFR required for adequate HD treatment the day after creation. The BAFR of BCF was not different from that of AVG, but the diameter of the vein used as the outflow vein was larger than that of AVG after 2 weeks. AVG showed no difference in BAFR after 1 day and after 4 weeks. In addition, if a large-scale research will be conducted, it is expected that clear results will be known for access maturation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.