
Abstract
Background:
On February 21 2020, in Schiavonia Hospital occurred the first death by COVID-19 in Italy and since this date SARS-CoV-2 caused more than 100,000 deaths in our country. Our hospital was immediately closed and re-opened after 15 days as a reference Covid Hospital. Among services involved in a process of destruction and rebirth there was also the Vascular Access Team.
Methods:
We analyzed our Vascular Access Team activity comparing data from the first month (March) in which basically it did not work and data from the following month (April) in which we began to re-build the Team adapting it to the new reality.
Results:
In all patients admitted to Intensive Care Unit a Centrally Inserted Central Catheter multilumen was placed, but in March only 5.5% of patients admitted to Medicine-Sub-intensive Unit had a catheter different from the short peripheral cannula while in April it was possible to guarantee a more suitable catheter 31.7% of patients admitted to Medicine-Sub-intensive Unit (p < 0.000). In April, compared to March, a significant higher number of Midline were implanted in Medicine-Sub-intensive Unit (36/139 vs 12/238 p < 0.000) where also a higher number of Centrally Inserted Central Catheter and Femoral Inserted Central Catheter were implanted (8/139 vs 1/238 p = 0.003). This change allowed us to implant more vascular accesses in Medicine-Sub-intensive Unit favoring Midline with a longer average duration. Only one patient with Midline developed a catheter vein thrombosis, and in only one patient the device was removed for suspected infection.
Conclusions:
The experience we gained will allow us to be more prepared in the future and our experience has highlighted that a structured Vascular Access Team is necessary to respond adequately to COVID-19 patients’ needs, to ensure the effectiveness of the maneuver, to reduce complications and to avoid the waste of resources, always working in safe condition.
Introduction
In the most of Italian hospitals the arrival of COVID-19 was a “tsunami” leading to an initial phase of confusion and “crash” followed by a second phase of re-organization based on new priorities. The pandemic wave hit every department and every clinical unit and Vascular Access Team (VAT) have not been an exception. 1
On February 21 2020, in Schiavonia Hospital occurred the first death by COVID-19 in Italy and since this date SARS-CoV-2 caused more than 100,000 deaths in our country. 2 Our hospital was immediately closed to the public, all patients and all staff were screened, wards and facilities were completely re-organized to re-open after 15 days as a Covid Hospital where patients from all the province of Padua could been referred. 3
Among services involved in a process of destruction and rebirth there was also the VAT, a young reality that was made up 3 years ago, a few months after the inauguration of this new spoke hospital able to accommodate 430 beds. Our multidisciplinary medical and nursing team has been responsible for the insertion of short, medium and long-term venous catheters for hospitalized patients, guests of care health residences, patients with program of chemotherapy or dialysis. The activity was working on 4 days a week and was able to perform more than 800 catheters in 2019.
In the first month after COVID-19 “tsunami” the VAT was substantially inactive because the nursing staff was diverted full-time to clinical activities in the various Covid units and the anesthesiologists were involved full time in the multiplication of resuscitation beds 4 ; only later the Team tried to rebuild itself to deal with the new situation that required, probably even more than in pre-Covid phase, the need to provide each patient with the most appropriate vascular access with the lowest possible risks both for patients and healtcare-workers. 5
In order to rationally address the new COVID era, the publication of a GAVeCeLT document was an important guide for the re-organization of the Team’s activity. 6
Objective
PRIMARY GOAL:
– To analyze the VAT activity in Schiavonia Hospital after the “tsunami” of the first case of death for COVID-19 in Italy, comparing data from the first month (March) in which basically the Team could not be able to perform normal activity and data from the following month (April) in which we began to re-build the Team.
SECONDARY GOALS:
– to evaluate the clinical characteristics of patients who had a vascular catheter inserted in the 2 months analyzed.
– to evaluate the characteristics, indications, and complications of catheters implanted.
Methods
We retrospectively compared the data of vascular accesses during the first month (catastrophic period) with the data during the second month (re-organization period).
The “catastrophic period” corresponds to the month of March 2020 where VAT nurses where reassigned to care activities in intensive care unit, sub-intensive unit or medicine, and VAT anesthesiologists were full-time employed in intensive care unit where a difficult reorganization led original 12 beds up to 50 beds of intensive care.
The “re-organization period” corresponds to the month of April 2020 when both the reduction of hospitalized patients and the ability to manage the emergency, together with the publication of GAVeCeLT and SIAARTI recommendations6,7 helped us to re-organize the activity of the Team and reschedule the insertion of the devices.
We collected and compared data of patients in which a venous access other than short peripheral cannula (peripheral venous line <6 cm long, PIV) was inserted during the period March—April 2020. This retrospective observational study was conducted in accordance with the Declaration of Helsinki and our Institutional Review Board provided approval; because of emergency it was not possible to obtain a specific consent from each included patient.
All venous accesses were positioned bedside by ultrasound guidance, as recommended by all international guidelines.8,9 We used peripheral venous line 6–15 cm long called mini-midline, peripheral venous line >15 cm long called Midline, Peripherally Inserted Central Catheters (PICC), Centrally Inserted Central Catheters (CICC), and Femorally Inserted Central Catheters (FICC). The insertion was performed by the operator following the Centers for Disease Control (CDC) recommendations for vascular access 10 : hand hygiene before the maneuver, skin antisepsis with 2% chlorhexidine in 70% isopropyl alcohol, nonsterile surgical mask, non-sterile cap, sterile gloves, waterproof sterile gown, wide sterile field on the patient, sterile probe cover of appropriate length around the ultrasound probe. In COVID-19 patients the CDC recommend the use of the surgical mask for the patient (if not intubated) and personal protective equipment (PPE) for contact protection (double glove, full suit, goggles, or face shield, footwear) for the operator. 11 All operators wore a double mask (masks with protective filter type FFP2 or FFP3 + a surgical mask) considering the high risk of aerosol in the environment. 12 All mini-midline, Midline and PICC were performed in respect of specific bundle of secure implant (Es: ISP protocol). 13 Only with PICC Subcutaneously anchored securement devices (SecurAcathTM Interrad Medical, Inc) was used while other catheters were fixated with sutureless devices.
The following patients’ parameters were analyzed: number of patients admitted to different Covid wards (Intensive Care Unit—ICU or Medicine-Sub-intensive Unit—M-SU), patients’ comorbidity (obesity, hypertension, diabetes, cognitive impairment, presence of pulmonary thromboembolism at the admission), therapy against COVID-19, biochemical parameters (worst values during hospitalization of: lymphocytopenia, D-Dimero, PCR, creatinine, lactic acid), and outcome (died, discharged, still hospitalized).
In addition, we studied the following parameters related to placed catheters: type of catheter, setting (ICU or M-SU), end point of the infusion administered, operator that performed the procedure, length of stay of the device, causes of removal.
Results
The ratio of vascular access placements to hospitalized patients significantly changed between March and April. In all patients admitted to ICU (both in March and April) a CICC multilumen (four lumen) was placed, but in March only 5.5% of patients admitted to M-SU had a catheter different from the short peripheral cannula while in April it was possible to guarantee a catheter different from a short peripheral cannula in 31.7% of patients admitted to M-SU (p < 0.000) (Table 1). In March we were able to place only mini-midline (No. 12); in April also Midline (No. 31) and CICC/FICC (No. 8) were inserted ensuring safer and longer-lasting vascular access. Overall, in April we placed more vascular catheters (No. 44) in M-SU than in March (No. 13).
Request of vascular devi for patients admitted to Schiavonia Hospital.
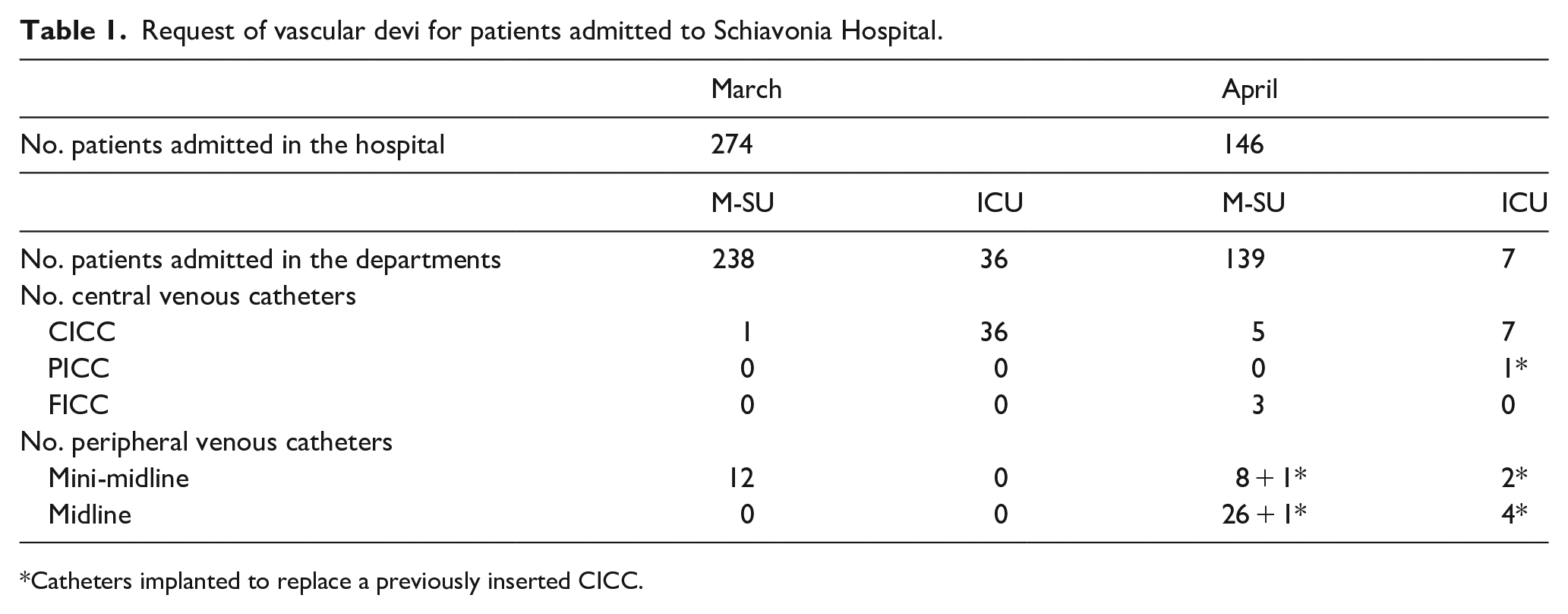
Catheters implanted to replace a previously inserted CICC.
Three out of the 36 (8.3%) CICCs placed in March were removed due to the presence of infectious complications (No. 3 CRBSI): none of these CICCs was replaced with other devices during this period. In April only two CICCs were removed for infectious complications (No. 2 CRBSI) and nine CICCs (five inserted in April + four inserted in March) have been removed and replaced with other devices (Midline and PICC) to ensure a vascular access with lower risk of infection before the admission in other wards.
Moving to the comparison of patients in which a vascular catheter was implanted in March and April (Table 2), we observed that the majority of patients admitted to ICU during both analyzed periods were male (M/F:29/14) while in M-SU there were more female patients (M/F:22/29) (p = 0.032). The average age of patients in ICU was higher compared to M-SU in both March (p = 0.013) and April (p = 0.008).
Description of patients who have been placed a vascular catheter.
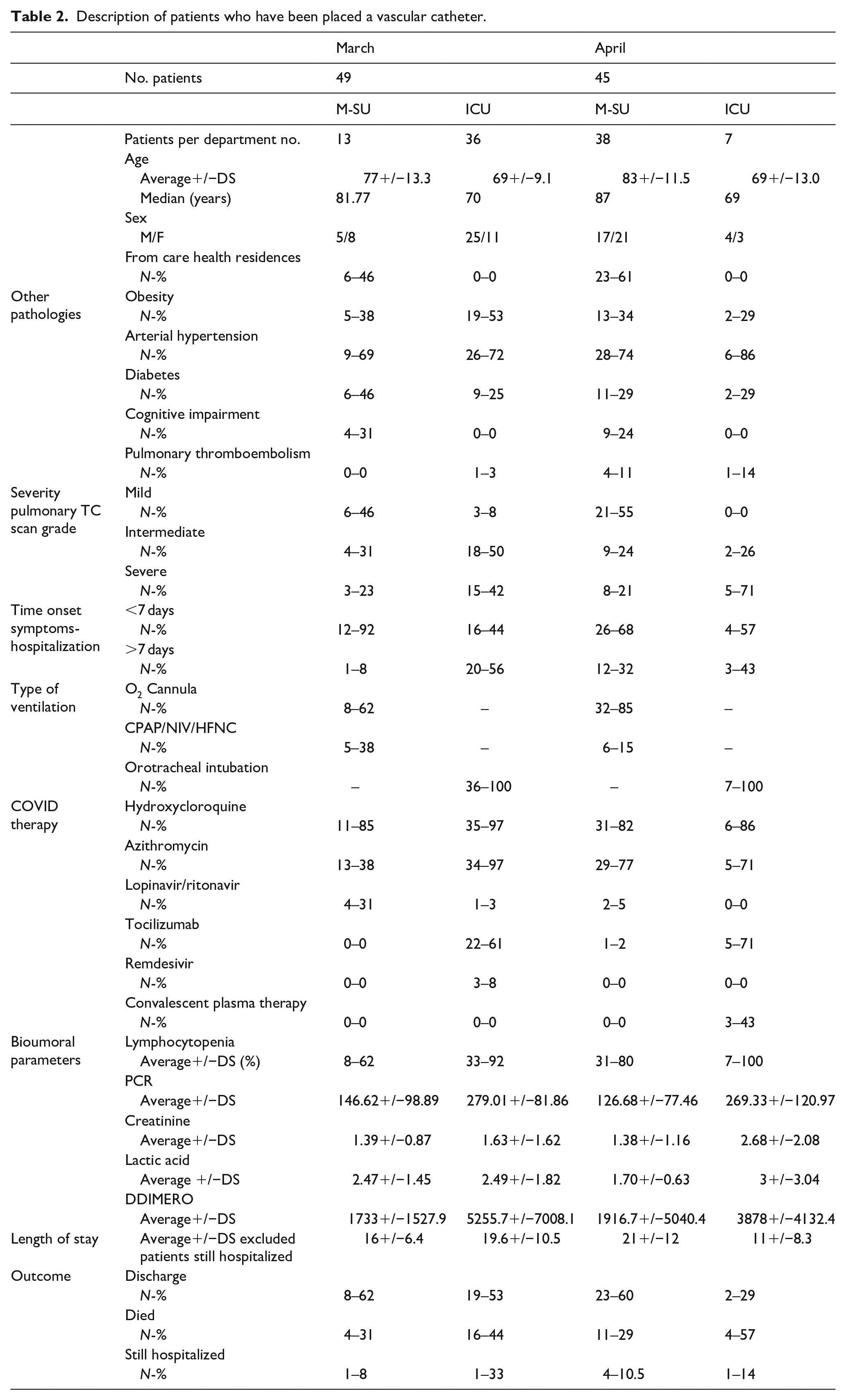
Around half of the patients admitted to M-SU in both March (6/13) and April (23/38) came from nursing homes (p ns).
Most of the patients admitted had at least one comorbidity:
– 53% of patients admitted to ICU in March were obese versus 38% of patients admitted in other wards but no statistical significance was observed (p = 0.575); this percentage was around 30% in both units in April.
– High blood pressure was registered in more than 70% of patients regardless of ward.
– Many M-SU patients suffered from cognitive impairment.
– Severe pneumonia at CT scan was present in 46.5% of patients in ICU versus 21.5% in M-SU (p = 0.019).
In both March and April, in patients admitted to ICU we observed a longer time between then onset of symptoms and hospitalization than in those admitted to M-SU and this difference was statistically significant in March. (March >7 days 8% vs 56% p = 0.008, April >7 days 32% vs 43% p = 0.670).
All patients were provided with oxygen therapy, in non-critical patients predominantly through nasal straws, less frequently CPAP/NIV, or HFNC.
While hydroxychloroquine was used in almost all patients, azithromycin was initially reserved for ICU patients, while in April it was administered also in M-SU.
The lopinavir/ritonavir was only administered in the first period and was then abandoned. Tocilizumab has been used almost exclusively in ICU patients. Convalescent plasma was used in ICU patients only in April, when 43% of patients received this therapy.
Analysis of bioumoral parameters showed that PCR values were higher in ICU patients compared to M-SU patients both in March (279.01 (DS 81.86) vs 146.62 (DS 98.89) p = 0.000) and in April (269.33 (DS 120.97) vs 126.68 (DS 77.46) p = 0.000). No significant differences were observed for creatinine and lactic acid values. DD values were higher in ICU patients both in March and in April but with a statistical significance only in March (5255.72 vs 1733 p = 0.008), not in April (3878 vs 1916.73 p = 0.375).
The average days of hospitalization were similar in different wards in March while in April we observed statistically significant lower days of hospitalization in ICU compared to M-SU (p = 0.048).
More than 60% of patients in M-SU were discharged, while the % of those who died in ICU remained stable in the 2 months and averaged 46.5%.
Analysis of data on vascular catheters showed that in April, compared to March, a significant higher number of Midline were implanted in M-SU (36/139 vs 12/238 p < 0.000) where also a higher number of CICC and FICC were implanted (8/139 vs 1/238 p = 0.003). (Table 3)
Description of implanted catheters.
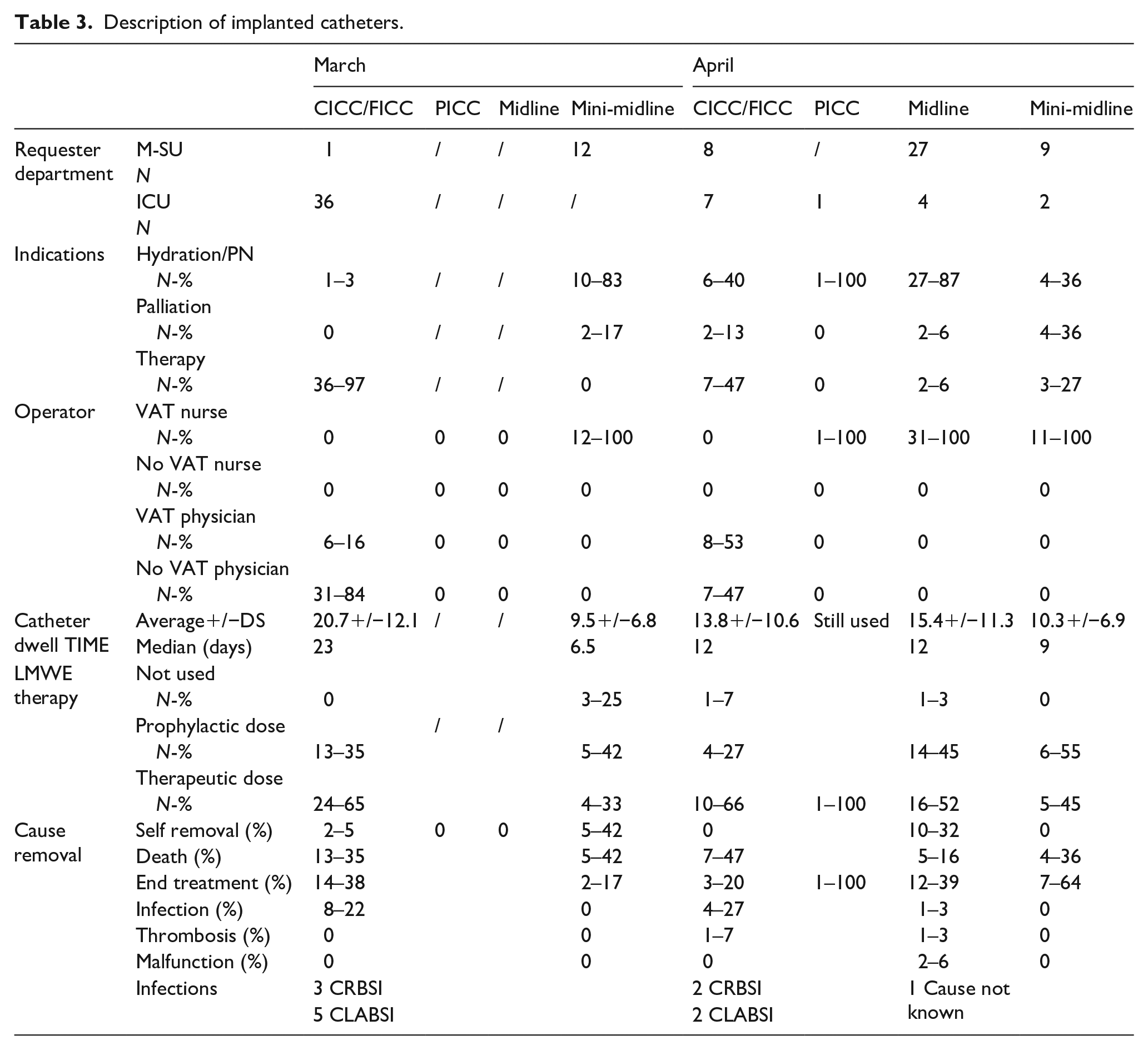
A PICC was also inserted in ICU in April against 0 in March.
CICCs have been positioned mostly for drug therapy while other catheters, especially mini-midline and Midline for hydration and parenteral nutrition in both periods: 87% of CICCs were placed in the right inner jugular vein while 41% of Midline/mini-midline were placed in the right basilica vein and 37% in the right brachial vein.
In March only 16% of CICCs were inserted by a VAT anesthetist while this percentage was 53% in April. (p = 0.017)
All peripheral accesses were placed by a VAT nurse both in March and in April but in March they were able to guarantee only a little number of mini-midline (No. 12) while in April they were able to implant a significantly higher number of peripheral accesses (43 vs 12 p < 0.000) with greater variety and better appropriateness (31 Midline, 11 mini-midline and 1 PICC).
The average length of stay of a CICC was significantly shorter in April than in March (13.8 days vs 20.7 days p = 0.061) because the hospitalization in ICU in April was shorter and the CICCs were replaced with other catheters before patients were discharged into the wards to reduce infection risk. The fact that in April VAT nurses placed more Midline than mini-midline allowed a longer average lifespan of peripheral accesses (15.45 days vs 9.5 days, p. 051). 5 out of 12 (42%) mini-midline inserted in March and 10 out of 31 (32%) Midline inserted in April were self-moved by patients.
Despite the well-known hypercoagulative state of COVID-19 in our patients we observed only a few vascular accesses thrombosis in both periods: 1 out of 52 CICC/FICC (1.9%), 1 out of 31 Midline (3.2%), no mini-midline, no PICC. These values could be due to the fact that almost all our patients received low molecular weight heparin treatment at prophylactic (100 UI/kg/24 h) or therapeutic (100 UI/kg/12 h) purposes.
The % of infection of multi-lumen CICCs (CRBSI) placed in the 2 months was 5 episodes/1000 days catheter life. These infections (two from negative gram bacteria: Klebsiella pneumoniae and Enterobacter Aerogenes and three from gram positive bacteria: S. Hominis in one patient, and S. Epidermidis in two patients) resulted in an increase in the length of hospitalization but never led to the patients’ death. Our data are in line with published data showing high infectious risk of multi-lumen catheters14–16 and justify the attitude (implemented in April) of rapidly replacing the CICCs with other catheters that present a lower risk of infection. 17
In our study there were also seven CLABSI (five in March and two in April): of these three were related to Candida spp (in all cases the patient died within a few days) and four related to bacteria (2 gram positive, S. Capitis and S. Epidermidis and 2 of gram negative, A. Baumanii, E. Aerogenes) with only one death.
Discussion
The organization of our Vascular Access Team was dramatically disrupted by the unexpected arrival of the pandemic from SARS-CoV-2 and the destination of our Hospital as a COVID Hospital for the province of Padua.
The reorganization of the hospital wards and the complete allocation of all medical and nursing staff to other clinical care activities related to the COVID-19 emergency has taken resources away from our VAT activity not allowing us to keep faith with the reasoned programing of devices implantation.
However, in April, taking into account the gradual reduction of admissions and supported by the publication of SIAARTI and GAVeCeLT scientific recommendations we were able to proceed to a partial reorganization of the VAT leading to some small but significant improvements in the number and variety of vascular accesses guaranteed and in the “rationality” of the choice of catheter.
Positive aspects of this change included the possibility to implant more vascular accesses in M-SU favoring Midlines with a longer average duration compared to mini-midlines. Midlines were able to be maintained for all the duration of patients hospitalization, proved to be useful both for withdrawals and infusions, and in some patients they allowed supportive therapies to be continued even after discharge. Only one patient with Midline developed a catheter vein thrombosis, and in only one patient the device was removed for suspected infection.
Negative aspects coming out from data analysis include that more than one-third of the peripheral catheters were self-moved by patients. Both advanced age and cognitive impairment as well as the difficulty of ensuring nursing surveillance of devices contributed to this aspect. A larger use of SecurAcath fixed PICC and/or SecurAcath fixed Midline could probably have reduced this problem.
Moreover, we could have been a little more “courageous” in proposing the placement of PICC as first catheter at least in those patients where the need to limit the risks of over-riding bacterial infection could be considered superior to the real need to ensure those multiple and complex pharmacological therapies that led us to the placement of a “routine” multi-lumen CICC in all patients admitted to ICU.
A role for PICC also in ICU, especially in patients with lower intensity of care, was also suggested within the recently proposed “Vascular access approach in COVID (VASCOVID) flow-chart” 18 ; moreover, with the benefit of hindsight and in light of the gained experience, we probably should have replaced CICC more frequently with PICC or Midline, as soon as the clinical conditions appeared more stable. 19
Fortunately, maintaining a high level of concentration, the proper use of protective equipment and the compliance with standardized and shared procedural protocols within the group allowed none of the Team members to become infected.
The experience gained will allow us to be more prepared in the future and our experience has highlighted that a structured VAT is necessary to respond adequately to COVID-19 patients’ needs, to ensure the effectiveness of the maneuver, to reduce complications and to avoid the waste of resources, always working in safe condition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.