
Abstract
Dialysis access steal syndrome is a well-recognised complication, affecting 1%–8% of all patients who undergo arteriovenous fistula formation particularly those that are brachial based. We present a case of ongoing steal syndrome following a DRIL procedure via retrograde flow in the ulnar artery. This was managed via a hybrid procedure and the use of an Amplatzer plug. This case demonstrates a novel use for the Amplatzer occlusion device, it is also a reminder that failure to occlude the vessel close to the fistula anastomosis can result in continued steal despite a functioning DRIL bypass.
Keywords
Introduction
Dialysis access steal syndrome (DASS) is a well-recognised complication, affecting 1%–8% of all patients who undergo arteriovenous fistula (AVF) formation particularly those that are brachial based.1,2 Patients can present acutely (<24 h), sub-acutely (<30 days) or chronically (>30 days) with a variety of symptoms that are consistent with inadequate perfusion. 3 These include pain, pallor, coldness, reduced or absent peripheral pulses, paraesthesia, paralysis, and in severe cases, tissue loss.
Diagnosis of DASS is based on history and clinical examination consistent with distal ischaemia in the limb of the dialysis fistula. Non-invasive tests such as plethysmography, Doppler ultrasonography and digital pulse oximetry have all been used to confirm the diagnosis. 4 Nerve conduction studies or catheter angiograms can be used if the diagnosis is equivocal.
Medical treatment options for DASS includes initiation of anti-platelet therapy, withholding anti-hypertensives and increasing dry weight. 5 Surgical treatment options include fistula ligation, banding/reduction, revision using distal inflow (RUDI), distal revascularisation with interval ligation (DRIL) and proximilisation of arterial inflow. 6 DRIL is often described as the preferred surgical technique as it reliably improves ischaemic symptoms whilst preserving a patent fistula.7,8
We present a case of DASS following formation of a brachiocephalic fistula which continued after a modified DRIL procedure.
Case description
A right brachiocephalic fistula was created for a 58-year-old woman with end-stage renal failure secondary to diabetic nephropathy and the patient was discharged home on the same day with no evidence of acute steal syndrome or ischaemic monomelic neuropathy (IMN).
One week later she re-presented with pain and paraesthesia in her right hand; this had been present since discharge but was progressively getting worse. On examination, she was found to be febrile but otherwise systemically well with sats 96% on room air, heart rate 89 and normotensive at 130/60. The fistula had a thrill but her hand was cold and neither the radial nor ulnar pulse could be palpated. The surgical wound was superficially infected. Management options including ligation were discussed with the patient who was currently dialysing through a right sided permacath as her previous left sided fistula had failed. She was keen to explore all surgical and salvage options and proceeded with a DRIL procedure.
As she arrived during the midst of the COVID-19 pandemic and had a febrile episode she had to be screened and isolate pending results. Her definitive surgical management was delayed for 24 h until had a negative swab result as it wasn’t deemed to be life or limb saving. DRIL is our preferred procedure for steal from (non-high flow) brachial based fistulas and it is our normal practice to anastomose to, and ligate, the brachial artery distal to the fistula anastomosis. In this case, to avoid contamination of the fresh surgical sites from the infected wound, the distal anastomosis using the left GSV as a conduit was made to the radial artery which was then ligated proximally. Post-surgery the patient’s symptoms improved and she was discharged home 3 days’ later.
Unfortunately, she returned a week later with recurrent symptoms and ultrasound showed the DRIL bypass to be functioning well with antegrade flow in the radial artery but retrograde flow in the ulnar.
Due to the recent surgery and infection in the fistula wound, it was decided to perform an endovascular occlusion of the brachial artery to ‘complete’ the DRIL procedure. As perfusion to the hand was then going to be dependent on radial supply only, an endovascular approach also allowed confirmation of an intact palmar arch.
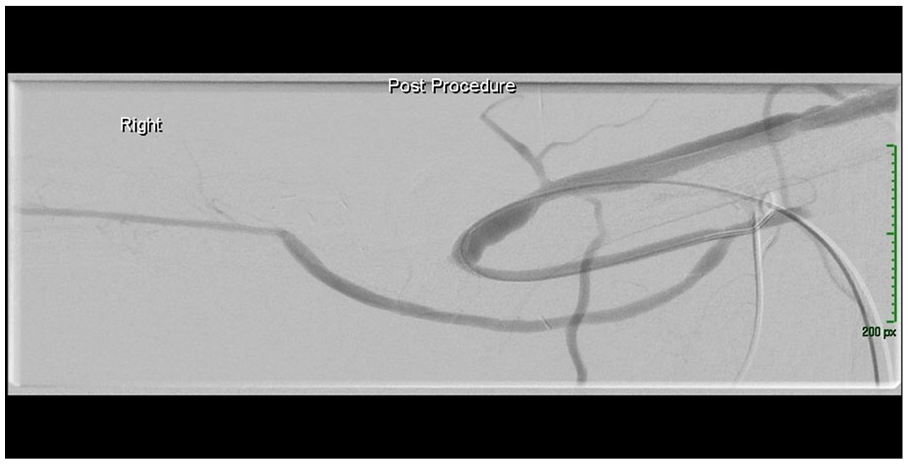
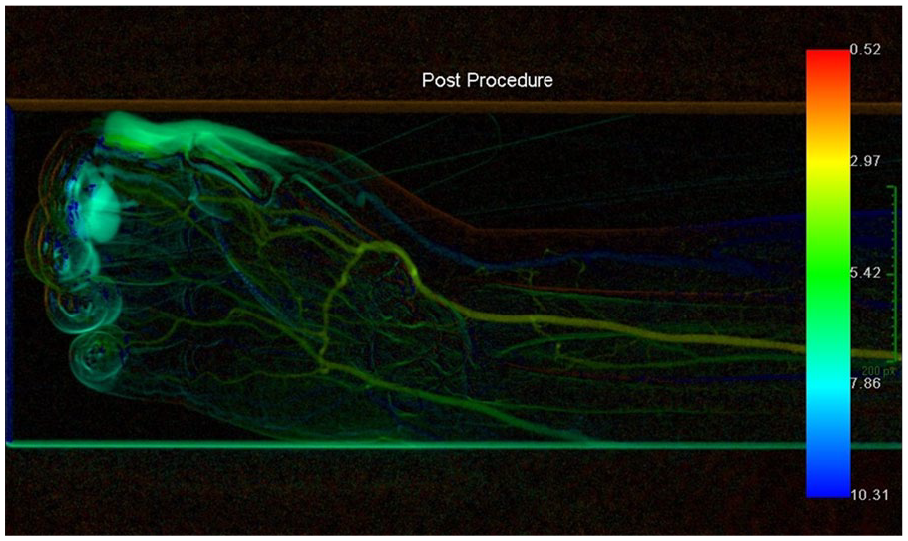
Under local anaesthetic the fistula was accessed under ultrasound guidance, a 7-Fr sheath inserted and a catheter placed in the brachial artery proximal to the DRIL anastomosis. Pre-intervention angiography demonstrated a patent DRIL bypass, a ligated radial artery and a patent distal radial artery in continuity with a complete palmar arch. It also showed rapid retrograde flow in the ulnar artery consistent with ongoing DASS (Figures 1 and 2) which was then confirmed using perfusion angiography (Figure 3).
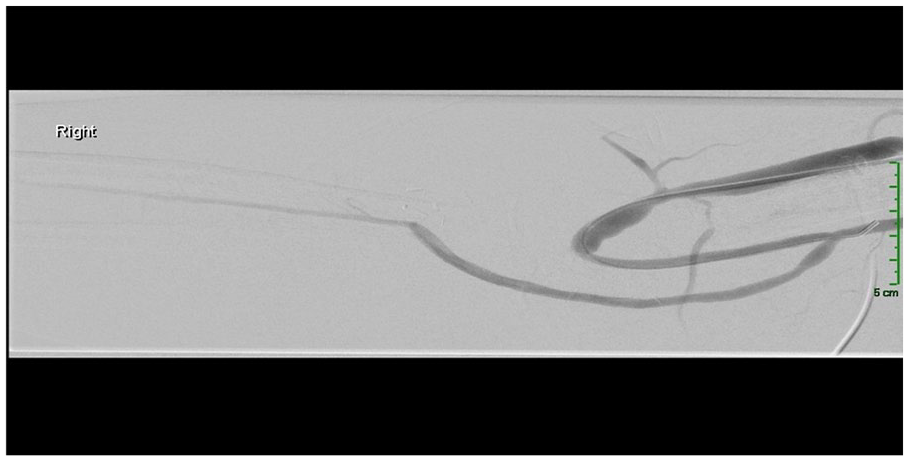
Pre-intervention digital subtraction angiography – contrast can be seen to flow down a patent bypass graft created during the DRIL procedure.
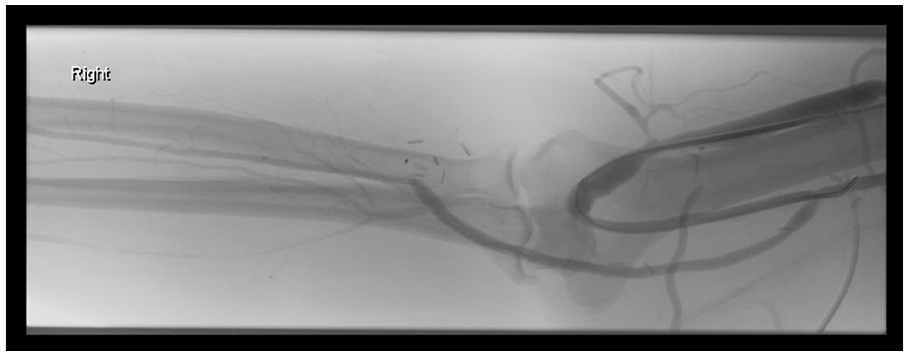
Faint ghosting of brachial artery seen in image below via the ulnar artery.
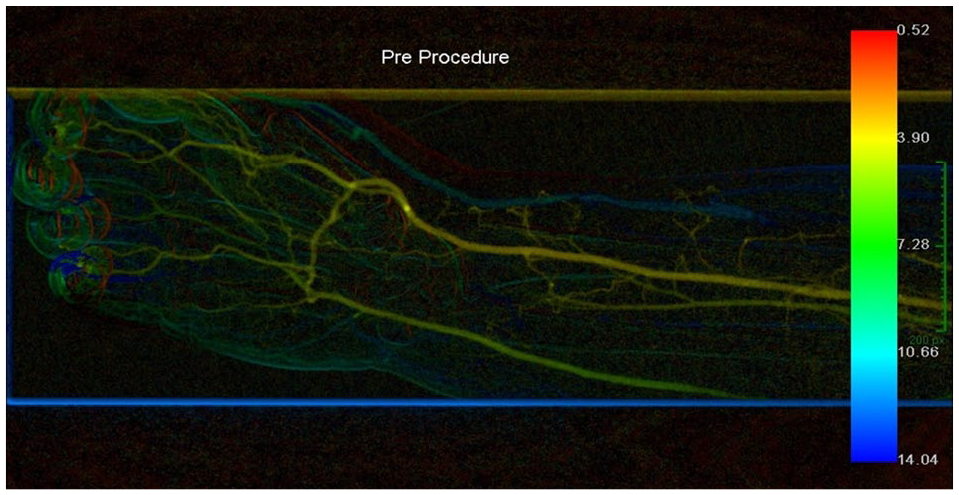
Pre-intervention perfusion angiography – there is restricted flow into the palmar arch and digital vessels.
An 8 mm Amplatzer Vascular II Plug (supplier in Australia) was then deployed in the brachial artery distal to the fistula anastomosis (Figure 4). Post-intervention angiography confirmed occlusion of the brachial artery, continued, but significantly reduced retrograde flow in the ulnar artery (Figure 5) and a significant improvement in perfusion angiography (Figure 6). Post-procedure the patient became pain free and experienced significant improvement in her neurological symptoms.
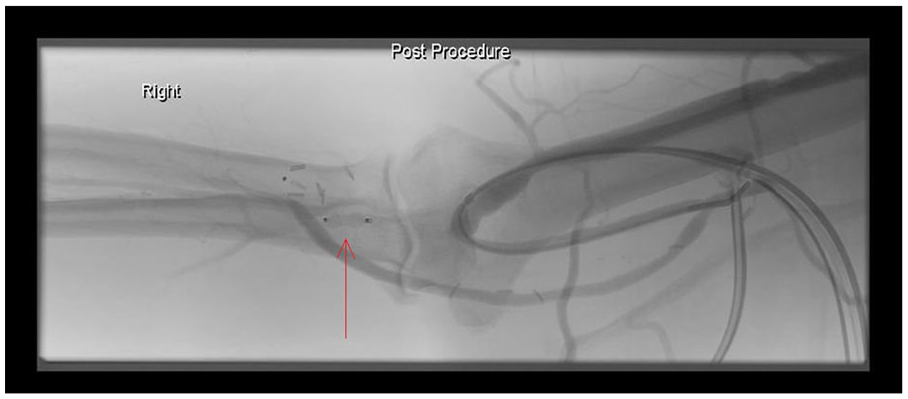
Post deployment of Amplatz plug in brachial artery with maintained flow in the DRIL.
Post-intervention digital subtraction angiography – contrast can still be seen to flow through the patent bypass but has now been abolished in the ulnar artery.
Post-intervention perfusion angiography – perfusion of the hand can be seen to have significantly improved particularly in the thumb, index and middle fingers which is where our patient described her most severe symptoms.
Conclusions
As well as a novel use for the Amplatzer occlusion device, this case is a reminder that failure to occlude the vessel close to the fistula anastomosis can result in continued steal despite a functioning DRIL bypass. It also highlights the potential for using both conventional and perfusion angiography 11 when performing procedures for DASS.
Given the success of the majority of access procedures including DRIL when performed with the usual technique, routine use of hybrid techniques is difficult to justify. However, other commonly performed procedures for DASS, particularly banding/reduction, are less reliable and outcomes could potentially be improved by the use of intraoperative perfusion angiography. In addition, some access formation procedures such as femoral vein transposition, are associated with a very high risk of DASS and there is potential for intraoperative perfusion angiography in these cases also.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.