
Abstract
Background:
Proper securement of central venous catheters plays an important role in onco-hematological pediatric patients. A new subcutaneously anchored securement device has been recently introduced in the clinical practice, and it has been extensively used in children.
Method:
In our study, we have retrospectively investigated the safety and the effectiveness of such device, reviewing the experience of three Italian pediatric oncological units. We have considered only tunneled catheters (cuffed or non-cuffed) inserted in children with malignancy; all types of tunneled central catheters were included in the analysis (both centrally and peripherally inserted) as long as they were secured with a subcutaneously anchored device. We investigated the incidence of dislodgment and of other catheter-related complications, with special attention to local adverse effects potentially related to the securement device.
Results:
We collected data from 311 tunneled catheters of different caliber: 80.4% were centrally inserted central catheters (CICC), 15.4% were peripherally inserted (PICC), and 4.2% were femorally inserted. Approximately half of the catheters (51%) were non-cuffed. Incidence of dislodgment was very low (2.6%) and the incidence of local pain or inflammation potentially related to the securement device was minimal (1.9%). Catheter related bacteremias were below 1 episode/1000 catheter days. No symptomatic catheter related thrombosis was reported. There was no significant difference in complications comparing cuffed versus non-cuffed catheters, or CICCs versus PICCs, or hematologic tumors versus solid tumors.
Conclusion:
In our retrospective analysis of a vast population of oncological pediatric patients with tunneled central catheters, the subcutaneously anchored securement device was tolerated very well, and it was highly effective in preventing dislodgment, both in cuffed and non-cuffed catheters.
Keywords
Introduction
Central venous access devices (CVADs) are essential tools in the management of onco-hematological pediatric patients, providing an atraumatic and durable venous access for blood sampling and for administration of intravenous drugs, blood components, and parenteral nutrition.
The most relevant potential complications of CVADs are infection (local or systemic), mechanical complications (dislodgment, rupture, or malfunction), and catheter-related venous thrombosis. The most severe complication of pediatric CVADs is catheter-related bacteremia, which may occur frequently (up to 4.5/1000 catheter days) 1 ; mechanical complications are also quite frequent (1.7/1000 catheter days) 1 ; the actual incidence of catheter-related thrombosis is not easily quantified.
Interestingly, some of these complications may be related to the inappropriate securement of the catheter to the skin: in fact, in/out movements of the catheter at the exit site may facilitate bacterial contamination of the exit site, as well as venous thrombosis and/or catheter dislodgement. Though, such movements can be completely abolished by using a specific device for subcutaneously anchored securement (SAS), introduced in the clinical practice a few years ago; this device consists in a small nitinol anchor placed just below the skin, inside the subcutaneous tissue, securing the catheter for the whole duration of its use. A recent consensus document 2 has discussed the evidence about the safety and effectiveness of such device.
Clinical studies have demonstrated the safety and efficacy of SAS in reducing the risk of dislodgement both in adult and in pediatric patients,3–5 as well as the good compliance of patients and the easiness of management by the nursing staff 6 ; a recent study has also suggested a beneficial effect of SAS on the risk of infection. 7
The Infusion Nurses Society’s Infusion Nursing Standards of Practice 8 (INS 2021) address catheter stabilization as an important component of clinical practice, promoting consistent practice among all clinicians and describing the criteria for the management of SAS.
This type of securement has been successfully introduced in Italy since 2015, and it has been widely used in children. The aim of our study is to report the clinical experience of three Italian hospitals in the use of SAS in pediatric oncological patients.
Methods
We retrospectively analyzed data of children treated for onco-hematological diseases—from January 2016 to December 2018—in three units of pediatric oncology, at the “Bambino Gesù” Pediatric Hospital in Rome, at the “Pausilipon” Pediatric Hospital in Naples, and at the “A. Gemelli” University Hospital in Rome. Approval of the study was granted by the institutional review board at each investigational site.
We reviewed the charts of children suffering from oncological or hematological diseases, who required the insertion of any external CVAD for short term, medium-term, or long-term venous access, as long as the device had been secured by SAS.
We collected all demographic characteristics and all available data about CVAD insertions and removal procedures. According to the local hospital policies, all catheters were power injectable, open-ended, non-valved, in polyurethane; we considered only tunneled catheters, either cuffed or non-cuffed.
The SAS device (SecurAcath, Interrad Medical) was always placed and removed by specifically trained clinicians.
We recorded all catheter complications that had been reported by the staff: catheter-related blood stream infection (CRBSI) (diagnosis established by paired cultures from the catheter and from the peripheral blood, according to the delayed time to positivity method); catheter-related symptomatic thrombosis (CRT) (diagnosis based on ultrasound exam, performed only in presence of signs or symptoms suggestive for venous thrombosis); dislodgment (defined as catheter movement of at least 2 cm from the original position at the exit site); catheter malfunction (defined as irreversible lumen occlusion or persistent/irreversible withdrawal occlusion); local inflammation (pain and/or redness of the exit site without secretions and with negative skin culture); exit site infection (pain and redness of the exit site plus evidence of local secretions and/or positive skin culture). We also recorded the any reported pain at SAS removal or any local discomfort clinically ascribed to the presence of the SAS. The possibility of pain at SAS placement was not considered, since all maneuvers of CVAD insertion were carried out in general anesthesia or in light sedation with local anesthesia.
This retrospective study was carried out according the STROBE checklist for retrospective cohort studies.
The statistical analysis was performed by Prism 8th version. Differences in complication rate were assessed by Fisher’s exact test.
Results
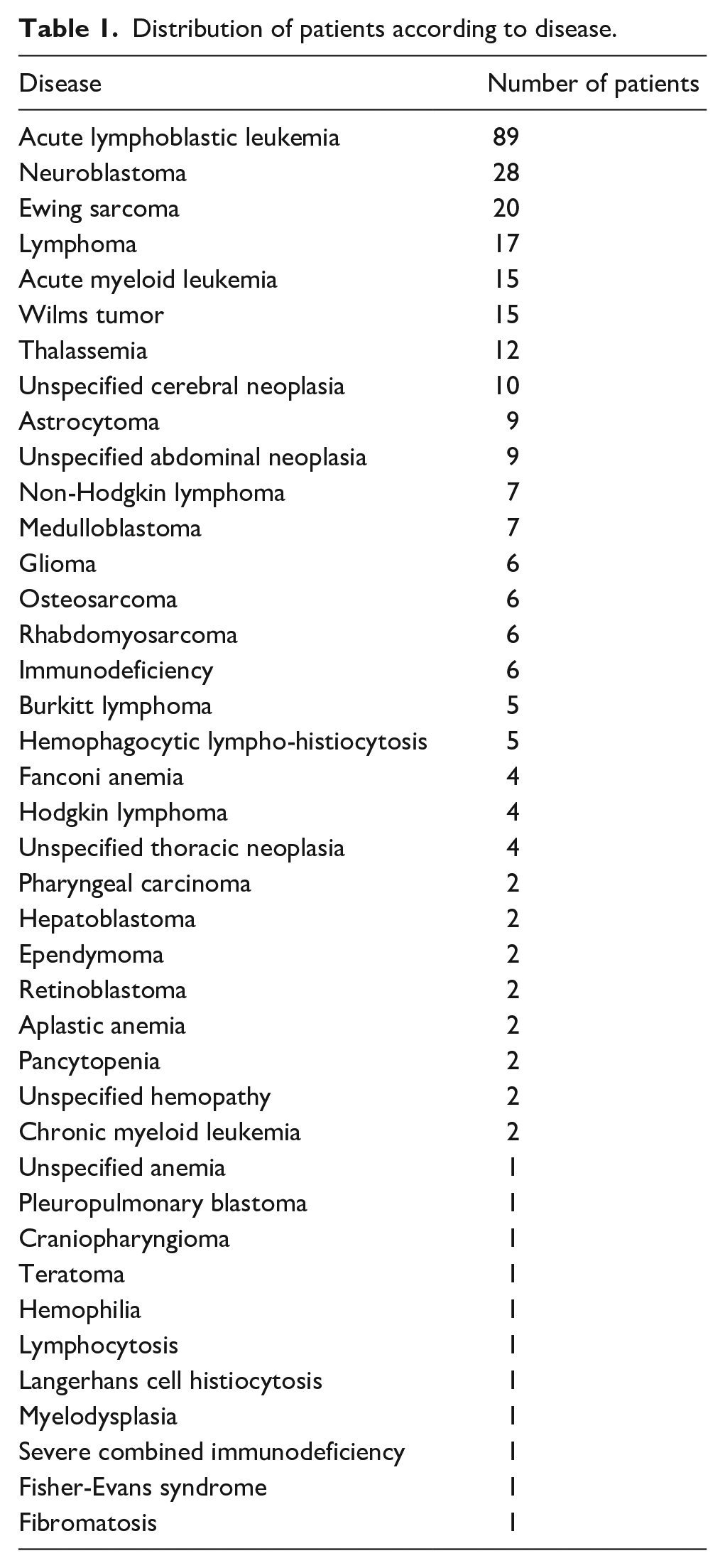
We collected data from the charts of 311 children. The median age at the time of CVAD insertion was 5 years (range 0–20 years); 175 patients (56.3%) were male and 136 (43.7%) were female, affected by various oncological and hematological diseases, as shown in Table 1.
Distribution of patients according to disease.
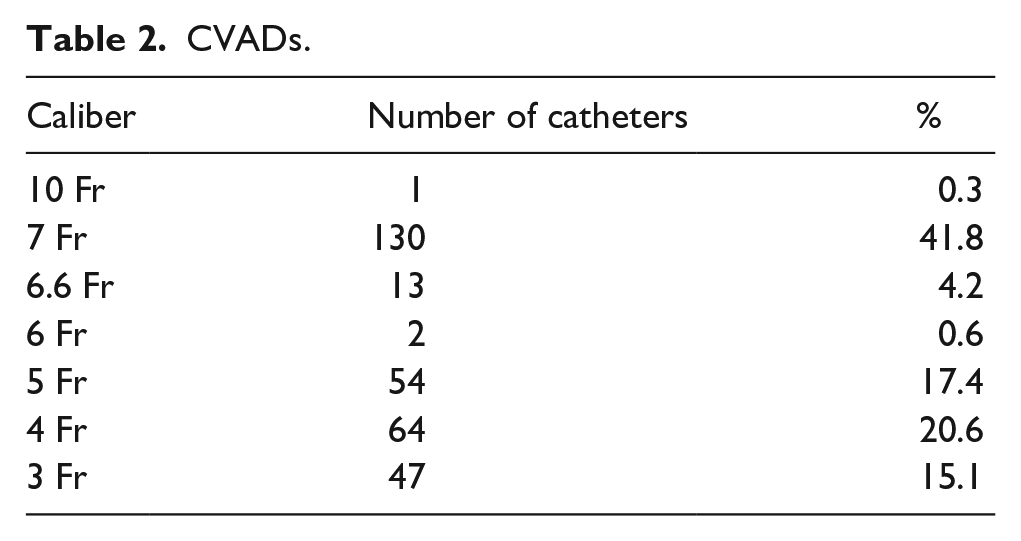
Only tunneled external CVADs were considered: 250 (80.4%) centrally inserted central catheters (CICC), 48 (15.4%) peripherally inserted central catheters (PICC), and 13 (4.2%) femorally inserted central catheters (FICC). The caliber of the catheters, chosen on the basis of the required treatment and of the vein size, is shown in Table 2: 187 (60.1%) were double lumen and 124 (39.9%) were single lumen; 160 (51.4%) catheters were tunneled, but non-cuffed.
CVADs.
Only 6 catheters (1.9%) were inserted by surgical cut-down, as the majority of insertions (98.1%) were performed by percutaneous ultrasound-guided venipuncture, as recommended by current guidelines. CVAD insertion was performed by specifically trained clinicians, according to the insertion bundle of the local hospital policies. CVAD maintenance was consistent with the hospital policies, which included—for all three centers—the same main strategies: dressing change every 7 days, skin antisepsis with 2% chlorhexidine in alcohol, protection of the exit site with semipermeable transparent membranes, use of neutral displacement needle-free connectors, flush, and lock with saline only.
The range of duration of the central lines was 0.1–113 weeks (median: 24.9 weeks), with a total number of 43,464 catheter days; the median duration was higher for cuffed catheters (31 weeks; range 0.6–113 weeks) than for non-cuffed ones (14.7 weeks; range 0.1–66.1 weeks).
Six catheters were still in place at the time of data collection (June 2019).
We reported 59 cases (18.9%) of catheter-related complications, described in Table 3. The overall rate of complications was 1.35/1000 CVAD days. The incidence of CRBSI was 0.97/1000 CVAD days.
Complications.
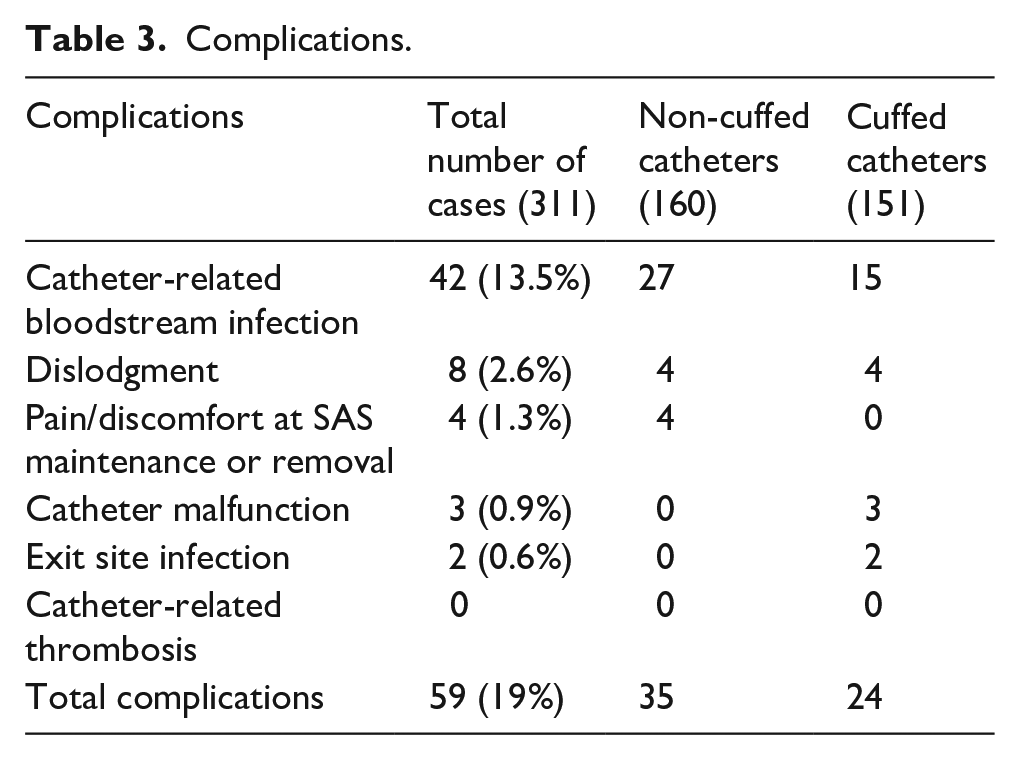
Comparing cuffed and non-cuffed catheters, no significant difference was found in terms of non-infective complications (OR 1.204; p 0.8051) or CRBSIs (OR 0.543; p 0.096).
Also, there was no significant difference between CICCs and PICCs in terms of total complications (OR 0.5546; p 0.3017) and of CRBSIs (OR 1.468; p > 0.999).
Comparing 177 children with hematological diseases (56.9% of total cases) and 134 (43.1%) with solid tumors, we found no significant difference in terms of complication rate (OR 1.345; p 0.3813) and CRBSIs (OR 1.011; p > 0.999)
Discussion
CVADs are widely accepted as necessary in the management of children with hematologic and oncological malignancies, in spite of the potential risk of associated complications (infection, thrombosis, dislodgement, etc.) that may determine unscheduled removal of the device, delayed in the delivery of chemotherapy, prolonged hospital stay, increased healthcare cost and—in some unfortunate situations—increased morbidity and mortality. 9
The incidence of catheter-related complications may be significantly affected by the appropriateness of catheter securement, 6 and the overall effectiveness of SAS in the pediatric population is currently suggested only by few clinical studies.2,3,5,10
Some studies have reported the effectiveness of SAS in reducing the risk of dislodgment in children and neonates, in both tunneled and non-tunneled, cuffed and non-cuffed CVADs5,10; however, in oncological patients, other factors like neutropenia, 11 thrombocytopenia, and corticosteroid therapy 12 may increase the incidence of unscheduled catheter removal.
Our retrospective, multicenter study was designed to collect information on performance and safety of SAS in pediatric patients suffering from hematological or oncological diseases.
Many precious studies have shown that sutureless securement is effective in reducing catheter complications by 45%–72%, especially catheter-related infections.13,14 Cesaro et al. 1 described an overall rate of complications of 6.2/1000 catheter days in children with cuffed central catheters secured by sutures, while Yamamoto et al. 15 reported an incidence rate of 0.7/1000 catheter days in patients using sutureless device with skin adhesion. The introduction of the subcutaneously anchored sutureless securement will be probably associated with even less risk of complications if compared to skin-adhesive sutureless securement, as suggested by our complication rate (1.35/1000 catheter days), better than any previously report in pediatric literature.
As regards the main goal of securement, in our experience SAS was highly effective, since we recorded only eight cases (2.6%) of catheter dislodgement, with a rate of 0.18/1000 catheter days, less than previously reported in literature. 6
SAS was used for different size of catheters and both CICCs, PICCs, and FICCs, as already reported in other studies. 5 We successfully adopted SAS for both centrally and peripherally inserted central catheters, ranging from 3 to 10 Fr, with no difference in terms of clinical effectiveness in reducing the risk of dislodgment.
Our experience was focused on only tunneled catheters, both cuffed and non-cuffed.
SAS have a significant role in tunneled-cuffed catheters, where accidental dislodgement may be caused by two different mechanisms: incomplete adhesion of the Dacron cuff to the subcutaneous tunnel tissue in the early weeks after CVAD positioning, and/or excessive physical activity of the child. Most dislocations of cuffed CVAD occur within 2 months after insertion; younger age is the only significant factor associated with unscheduled CVAD removal. 1 These findings suggest that more effectively securing the CVAD to the subcutaneous tissue by SAS may reduce significantly the premature loss of cuffed CVAD, especially in young children.2,11 In our study the rate of dislodgment was similar in cuffed and non-cuffed catheters, suggesting that the cuff may play a less important role in securement of tunneled CVADs if compared to SAS, as already suggested by other authors. 11
The risk of exit site complications (bleeding, inflammation, infection) potentially caused by the SAS device is apparently very low. 2 Some evidence suggests that the local placement of cyanoacrylate glue may avoid bleeding/oozing and protect the exit site from bacterial contamination16,17; though, this practice is not yet universally adopted, and it was used only in one of the three hospitals included in our study.
In most patients in this study, no complication potentially related to SAS was reported; this good performance is probably also explained by the fact that the device was managed by properly trained clinicians. In fact, many authors have described that management of SAS is easy and safe only if practiced by specifically trained healthcare professionals.3–5 In these studies, no relevant pain at insertion, management, or removal had been reported.3,5
Our retrospective review confirms that SAS is well tolerated in children and even in newborns: we found only four reports (1.3%) of pain/discomfort at entry-site, all of them requiring removal of the SAS, but not removal of the CVAD.
Not surprisingly, we had no case of allergic reaction to the device. The concern about the possible allergy to the nitinol anchor in patients with nickel hypersensitivity is not supported by the literature. No case of allergy to nitinol (compound of nickel and titanium) has been reported, and no cross-sensitivity between nickel and nitinol is known.
As regards CRBSI and CRT, the incidence of such complications was very low in our series, and we cannot infer whether the subcutaneous anchorage had any role in this regard.
Finally, our study showed that tunneled CICCs and tunneled PICCs have the same expected rate of complications in oncologic pediatric patients, confirming that the incidence of infection, thrombosis, and dislodgment are mainly related to the adoption of appropriate specific strategies of prevention during insertion and maintenance, rather than to the choice of a centrally inserted versus peripherally inserted device.
The limitations of our study are the following:
- Being a retrospective, non-controlled cohort study, there was no direct comparison between SAS with the traditional skin-adhesive sutureless device in terms of safety, effectiveness, and cost-effectiveness; this issue would require a proper randomized prospective trial.
- Also, being a retrospective study, it is possible that some minor discomfort or minimal complications of SAS had not been reported.
- Last but not least, all clinicians operating in our three hospitals (nurses and physicians) were specifically trained in the management of SAS; it is possible that the same device, in untrained hands, might be associated with poorer outcomes.
In conclusion, the analysis of the data of our retrospective study—carried out in a vast pediatric population of oncological patients, with both hematologic and solid tumors—shows (a) that SAS was very effective as securement of tunneled central catheters, since the incidence of dislodgment was very low (2.6%), regardless of the presence of a cuff; (b) that the securement device was very well tolerated by all patients, since local complications potentially related to the presence of the SAS, such as local pain or inflammation/infection of the exit site, were very rare (2.25%); (c) that the adoption of this securement was not associated with any increased risk of CRBSI (extremely low in our experience: <1 episode/1000 CVAD days) or of symptomatic CRT (no case reported in our series).
The low CRBSI is probably explained by the proper adoption of strategies of infection prevention in our three hospitals. The absence of any reported case of symptomatic CRT may be also explained by the adoption of strategies for prevention of thrombosis (appropriate catheter/vein ratio, ultrasound guided venipuncture, proper central location of the tip).
Further prospective, controlled studies are warranted, so to ascertain whether the very low risk of infection and thrombosis might have been partially ascribed also to the use of this new securement device.
Footnotes
Author contributions
Alessandro Crocoli and Cristina Martucci equally contributed to the realization of this study and the draft of this manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.