
Abstract
Background:
This retrospective study investigates the efficacy and safety of the novel Celt ACD® vascular closure device (VCD) following antegrade and retrograde common femoral artery (CFA) punctures for the treatment of peripheral artery disease in a challenging patient collective (e.g. calcifications, obesity, and anticoagulation).
Methods:
A total of 208 VCDs (i.e. 100 antegrade and 108 retrograde) were deployed between October 2019 and December 2020 in a tertiary referral interventional radiology department. Fifty-two devices were undersized in relation to the introducer sheath (up to 2 Fr). Technical success and VCD related complications were evaluated in the immediate post procedure period and the following 24 h clinically. In 68% of cases, additional duplex ultrasound was performed prior to discharge.
Results:
The overall technical success rate was 97%. Technical failures following antegrade approach were due to a too acute access angle (⩾60°), rendering it impossible to pass the applicator tip through the sheath lumen. A subgroup analysis of technical success pinpoints severe calcification as another key limiting factor in VCD use (p = 0.004). Comparing equally sized with undersized device selection (p = 0.196), direction of approach (p = 0.265), and body mass index (p = 0.184) proved to be insignificant. Five (2%, 5/208) major complications occurred: Four antegrade (i.e. one false aneurysm, one vessel laceration with retroperitoneal hemorrhage, two device migrations; 4%, 4/100) and one following retrograde access (i.e. >6 cm hematoma, 1%, 1/108)). Complications were successfully managed with manual compression or interventional procedures.
Conclusions:
The novel clip-based VCD proved to be effective with a low VCD related complication rate.
Keywords
Introduction
The need for achieving immediate hemostasis and definitive closure of a femoral puncture site encouraged the development of a variety of vascular closure devices (VCDs) since the 1990s. VCDs offer an effective alternative to manual compression (MC) and prolonged bed rest.1–3
To date, previously published pre- and postmarked studies evaluated the use of the novel Celt ACD® VCD (Vasorum Ltd., Dublin, Ireland) following retrograde punctures for interventional cardiology procedures.4–6 As a key element of up-to-date treatment of peripheral artery disease (PAD), the number of antegrade peripheral vascular interventions increases constantly. Complex peripheral artery obstructions above or below the knee require vascular access via an antegrade route to successfully restore blood flow to the affected limb for limb salvage, pain relief, and improved wound healing. As considerable advantages exist, antegrade puncture is more challenging (i.e. vessel branching anatomy, angulation) and accompanied by a higher rate of access site complications.7,8 Consequently, every measure, which minimizes access site complications, is welcome and the use of VCDs is growing.9,10 In contrast, the currently available data about antegrade VCD use reflects the increasingly complex clinical scenarios only to a limited extend (e.g. calcifications, scarring, obesity, and anticoagulation).1,6–8,11
Therefore, the aim of our study was to assess the efficacy and safety of the novel VCD following antegrade common femoral artery (CFA) punctures. In addition, we investigated the efficacy of the novel VCD following retrograde punctures with larger access diameters as previously published.4,6 Furthermore, we assessed the option of undersizing the VCD in relation to the introducer sheath up to 2 French (Fr) in order to potentially expand the field of application toward punctures as large as 9 Fr.4,6
Methods
Study design
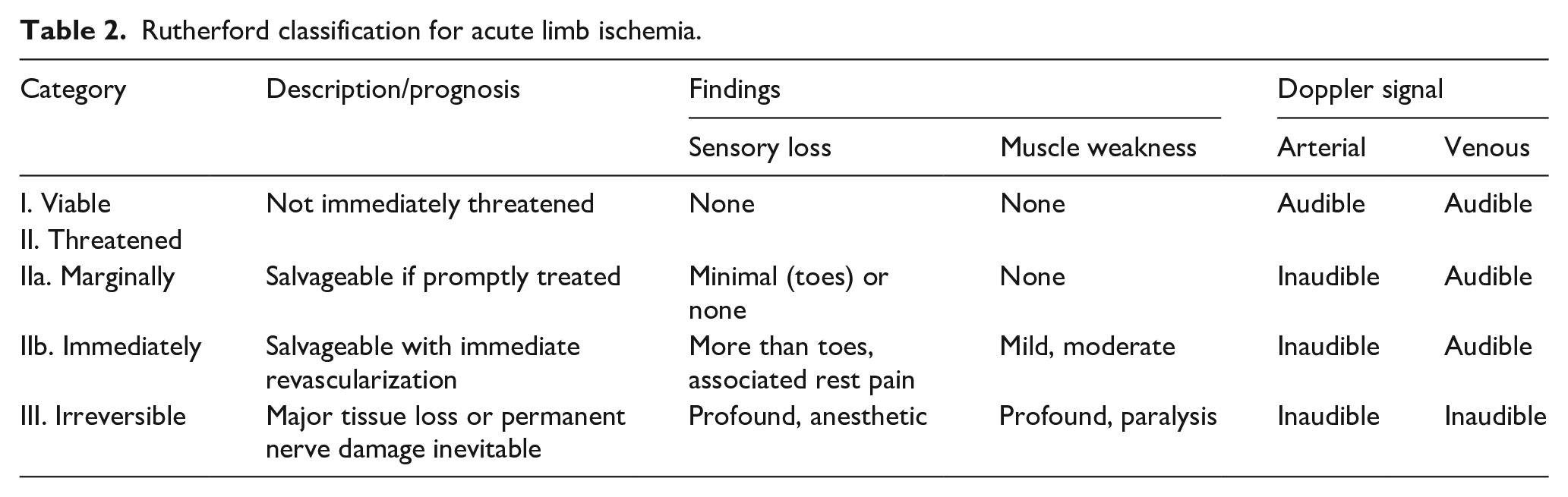
This non-randomized single center post-market study retrospectively evaluates the efficacy and safety of Celt ACD® VCD in our tertiary referral interventional radiology department from October 2019 to December 2020. We included adult patients between 30 and 94 years of age, scheduled to undergo an interventional peripheral vascular procedure via CFA. Prerequisite for inclusion was a CFA diameter of at least 5 mm (determined by computed tomography or ultrasound). Sixteen patients presented with acute limb ischemia (Rutherford I–IIB). About 136 patients suffered from chronic limb ischemia (Rutherford 2–6). Fifty-six patients underwent endovascular treatment of abdominal vascular disease. Prior to the interventional procedure, patients provided informed, written consent.
The mean body mass index (BMI) was 24. Eighty (38%) patients were overweight (BMI 25–29.9). Twenty-five (12%) patients were obese (BMI 30–34.9) and eight (4%) patients were extremely obese (BMI ⩾35). Patients with abdominal fat aprons, covering the inguinal region, were prepared for the procedure by taping overhanging aprons proximally. Thirty-two percent of patients were diabetic. About 84% received treatment for hypertension and more than 60% had impaired renal function (i.e. glomerular filtration rate (GFR) less than 89 mL/min/1.73 m2).
Eighty-two percent of patients received long-term antithrombotic therapy for cardiovascular disease. Among these patients, 70% were under antiplatelet treatment with a single agent (aspirin, clopidogrel, or ticagrelor), 8% had dual antiplatelet therapy, and 22% were on anticoagulants (58% direct factor Xa inhibitors, 3% direct thrombin inhibitor, 39% vitamin K antagonists). Five percent of these patients received a dual combination therapy consisting of antiplatelet drug and anticoagulation.
In 74% of interventions, we administered unfractionated heparin (e.g. 5000 International Units) without protamine reversal.
Preprocedural evaluation of the access site with computed tomography (conducted for procedure planning) or duplex ultrasound revealed in more than 65% of patients moderate (25%–50% circumference) to severe (>50% circumference) vessel wall calcification. 12 Antegrade femoral access sites showed in 27% none to mild (<25% circumference), in 35% moderate and in 38% severe vessel wall calcification. Retrograde femoral access sites had in 41% none to mild, in 35% moderate, and in 24% severe vessel wall calcification. Sixteen patients had severe inguinal scarring after previously performed surgical procedures including open surgical endarterectomy and bypass surgery.
Three operators (interventional radiologists with 25, 2, and 1 year post certification experience), who previously had been trained by a company representative, deployed 208 VCDs (5–7 Fr) in 195 consecutive patients under sterile conditions and local anesthesia according to the instructions for use. 13 The operators have experience with other VCDs, including suture based and clip based active approximators as well as sealant based passive approximators: Operator 1 (Angio-Seal® and FemoSeal® (Terumo, Tokyo, Japan), Perclose Proglide® and StarClose SE® (Abbott Vascular, USA), Exoseal® (Cardinal Health, Dublin, Ireland)), Operator 2 (StarClose SE® (Abbott Vascular, USA)), and Operator 3 (StarClose SE® (Abbott Vascular, USA), MynxGrip® (Cardinal Health, Dublin, Ireland)).
About 131 male and 77 female patients with a mean age of 71 (±11) years received closure of the access site with the novel VCD. In 13 patients, more than one device was used, on both femoral sides as well as on the same femoral side at consecutive time-points. One hundred VCDs were deployed following antegrade and 108 following retrograde CFA punctures.
For establishing antegrade access, we applied ultrasound to guide the initial puncture in the majority of cases. The introducer sheath sizes ranged from 5 to 8 Fr in the antegrade group (Radifocus® Introducer II Standard sheath; sheath length 10 cm, Terumo, Tokyo). In 66 cases, sheath and device were equally sized (i.e. 23 × 5 Fr/5 Fr, 41 × 6 Fr/6 Fr, 2 × 7 Fr/7 Fr). In 34 cases, we used a smaller VCD size in relation to the sheath size (i.e. 22 × 6 Fr/5 Fr, 2 × 7 Fr/6 Fr, 10 × 8 Fr/7 Fr).
For establishing retrograde access, we used sheath sizes from 5 to 9 Fr. In 90 cases, sheath and device were equally sized (i.e. 43 × 5 Fr/5 Fr, 15 × 6 Fr/6 Fr, 32 × 7 Fr/7 Fr). In 18 cases, we undersized the device in relation to the sheath (i.e. 1 × 7 Fr/5 Fr, 1 × 7 Fr/6 Fr, 9 × 8 Fr/7 Fr, 7 × 9 Fr/7 Fr).
Two main aspects induced us to assess the option of undersizing: First, following antegrade and retrograde accesses, we intended to check, whether we can safely close accesses of up to 8 or 9 Fr with a 7 Fr device. To date, the novel VCD is available in 5–7 Fr. However, we need accesses of 8–9 Fr in our daily routine (e.g. in cases of acute limb ischemia, in which manual femoropopliteal thrombus aspiration with an 8 Fr aspiration catheter is indicated, or in cases of aortoiliac covered stent or stent graft insertions requiring sheath sizes of up to 9 Fr). In other words, the diameter of a 7 Fr VCD clip measures 5 mm and the outer diameter of a 9 Fr sheath is approximately 3 mm. Therefore, we aimed to assess, whether a safety rim of 2 mm width in the relation of clip-to-sheath-diameter is sufficient for definite puncture site closure.
Second, in antegrade VCD use we decided to undersize the device in order to facilitate the applicator passage through the sheath lumen in borderline antegrade access angles (50°–60°) as proposed by the manufacturer.
Table 1 presents the patients and procedures’ baseline characteristics. Tables 2 and 3 provide the Rutherford classification for acute and chronic limb ischemia. 14
Patient and procedure characteristics.

Rutherford classification for acute limb ischemia.
Rutherford classification for chronic limb ischemia.

AP: ankle pressure; PVR: pulse volume recording; TM: trans metatarsal; TP: toe pressure.
Device description and deployment technique
The novel VCD is a double clip-based active approximator (available sizes 5–7 Fr). It consists of a MRI-compatible, biocompatible stainless steel implant, delivered by a single use, disposable unit. The star-shaped implant is composed of a distal half, deployed on the endoluminal side, and a proximal half, deployed on the adventitial portion of the vascular wall. A short, cylindrical peduncle connects both wings within the arterial wall. The operator inserts the clip applicator directly through a commercially available introducer sheath. The sheath length has to be confined to a maximum of 15 cm. Therefore, in cases of retrograde access routes, requiring long braided sheaths (e.g. Destination, sheath length 45 cm, Terumo, Tokyo, Japan), a sheath-exchange has to be performed prior to VCD use. To engage clip applicator and sheath, the front end of the applicator handle is latched with the sheath valve. In deployment step 1, the operator turns the end of the VCD handle in a clockwise direction until the distal handle part pops back under formation of a short gap and the endoluminal wing opens. Before proceeding to the next step, the system has to be withdrawn vertically from the patient until the distal wing closely abuts the inner vessel wall. For step 2, the distal handle grip is rotated counter-clockwise while the operator maintains upward tension. After the gap between the two handle parts has increased again, the proximal wing is formed at the adventitial portion of the vessel wall. In a third, final step the operator presses the ejection lever down toward the distal handle part and the implant is released. This sequence takes approximately 60 s to complete (Figure 1).4,13
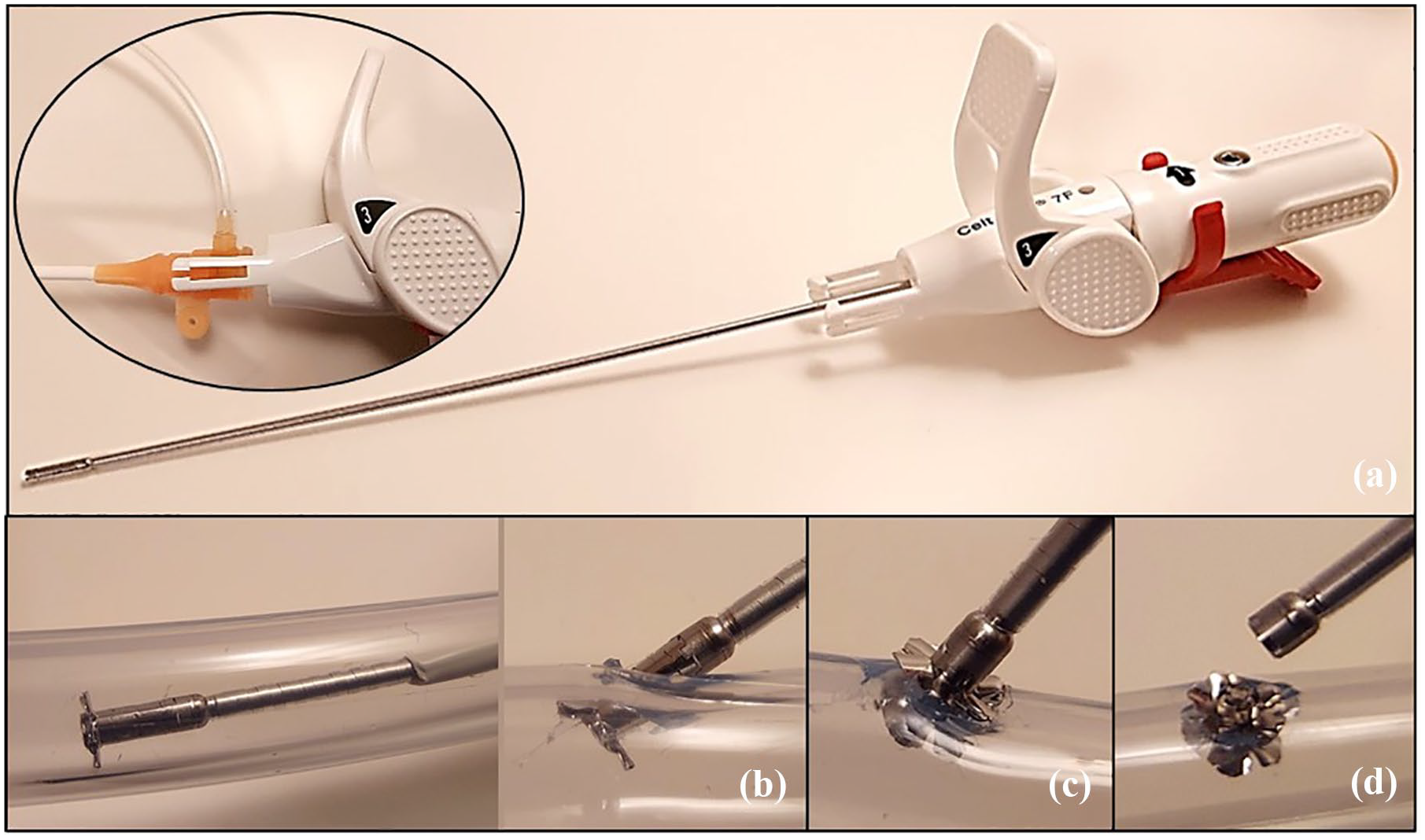
Celt ACD® vascular closure device (7 Fr) and clip applicator engaged with sheath-valve highlighted in inset (a). Deployment steps 1 to 3 (b–d).
After releasing the implant and removing of sheath and applicator, we manually held pressure for up to 1 min at the access site to ensure hemostasis. In order to guarantee the correct position of the metallic implant, we acquired a fluoroscopic image of the inguinal region. Moreover, we clinically ascertained immediate effectiveness and safety data. Subsequently, we applied a sterile pressure dressing and asked the patient to keep bed rest until the next morning. For further evaluation of access site complications, all patients underwent clinical surveillance for at least 24 h by the referring vascular surgeon. Additionally, we assessed 140 (67%) access sites after 24 h with duplex ultrasound (Figure 2).
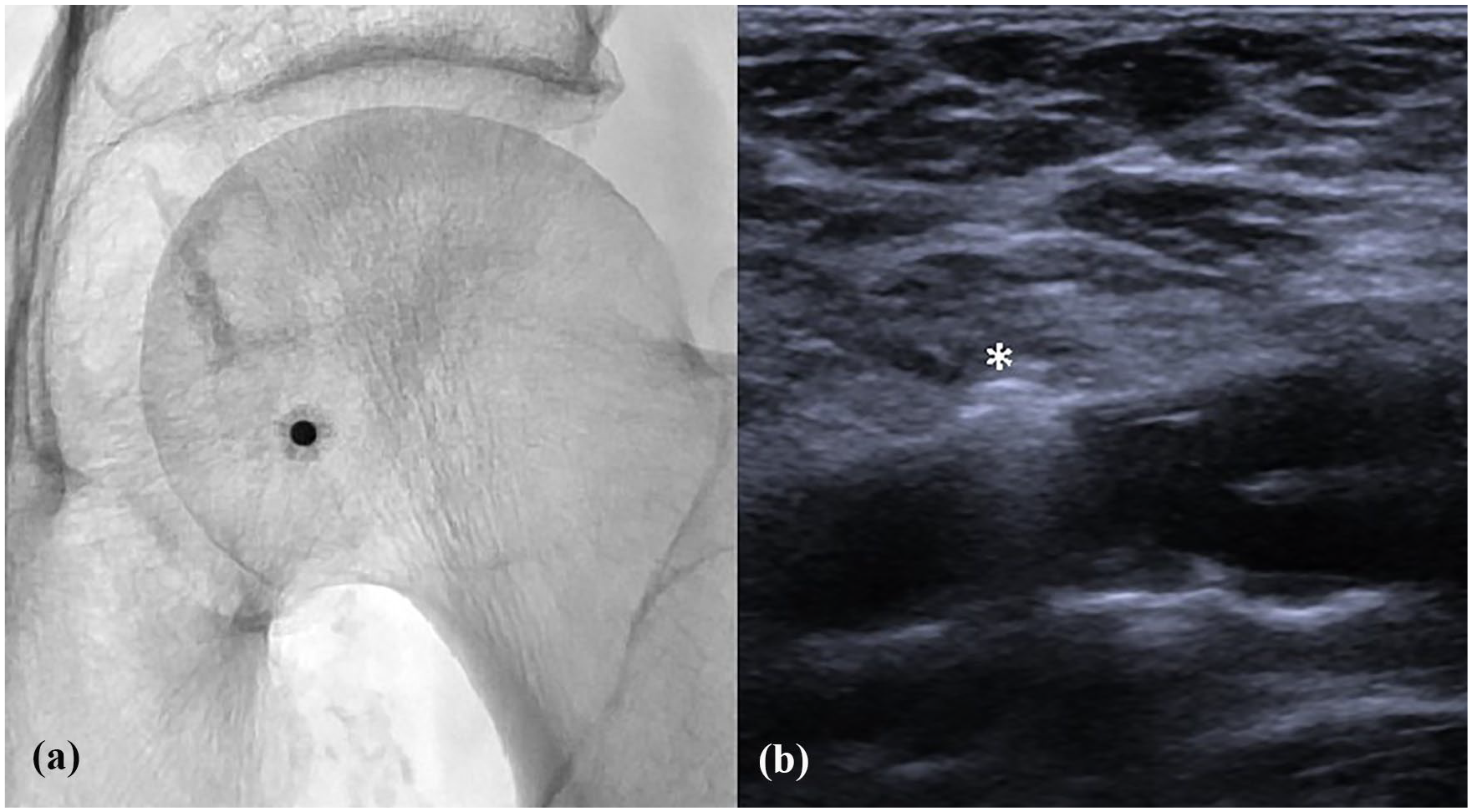
Fluoroscopy-image (a) and ultrasound image (b) of a correctly deployed device (white asterisk).
Endpoint definition
The efficacy end-point of the study was technical success. Technical success was defined as unimpeded VCD deployment and hemostasis in less than 2 min. As safety endpoint, we designated persistent hemostasis during the hospital stay and freedom from major complications. Complications following VCD use were classified according to the reporting standards of the Society of Interventional Radiology. 15
Statistical analysis
We performed statistical analysis with a dedicated software (RStudio 1.2.5033, The R Foundation for Statistical Computing, Wien, Austria). Continuous variables are represented as mean ± standard deviation (SD) for normally distributed variables or medians with ranges for non-normally distributed variables, categorical variables as absolute values and percentages. With regard to assessment of normality, the Anderson-Darling test was used rejecting the hypothesis of normality when the p-value was less or equal to 0.05. Group differences were assessed with the unpaired Student’s t-test for normally distributed variables, Mann-Whitney U-test for non-parametric or non-normally distributed variables and Fisher’s exact test for categorial data. We considered a p-value less than 0.05 statistically significant.
Results
Efficacy
The overall technical success rate was 97%. Five antegrade VCD deployments failed due to malfunction of the delivery system, composed of sheath and clip applicator. The combination of a too acute antegrade vascular access angle (>60°), causing sheath kinking at the level of the vascular access point, and the configuration of the applicator tip, contributed to technical failure in these cases. At the level of the vascular access point, the applicator tip scraped the posterior sheath-wall, rendering it impossible to pass the applicator through the sheath lumen. In four of these cases, the undeployed VCD was safely removed and the access site was closed by MC and bed rest.
However, in one case profound damage to the sheath occurred by slitting the posterior sheath-wall, leading to a short segment vessel wall laceration with bleeding. In this case, the access site was unintentionally high at the level of the inguinal ligament. Subsequently, the patient developed hemodynamic compromise due to retroperitoneal hemorrhage. Since the patient was not suitable for general anesthesia, we immediately excluded the lacerated vessel segment with covered stent implantation in crossover technique. Due to the flatter access angle, we did not observe this type of failure in retrograde approaches.
In patients presenting with severe inguinal scarring, only one technical failure appeared following retrograde CFA puncture with persistent oozing within 5 min after releasing of the device (Figure 3).
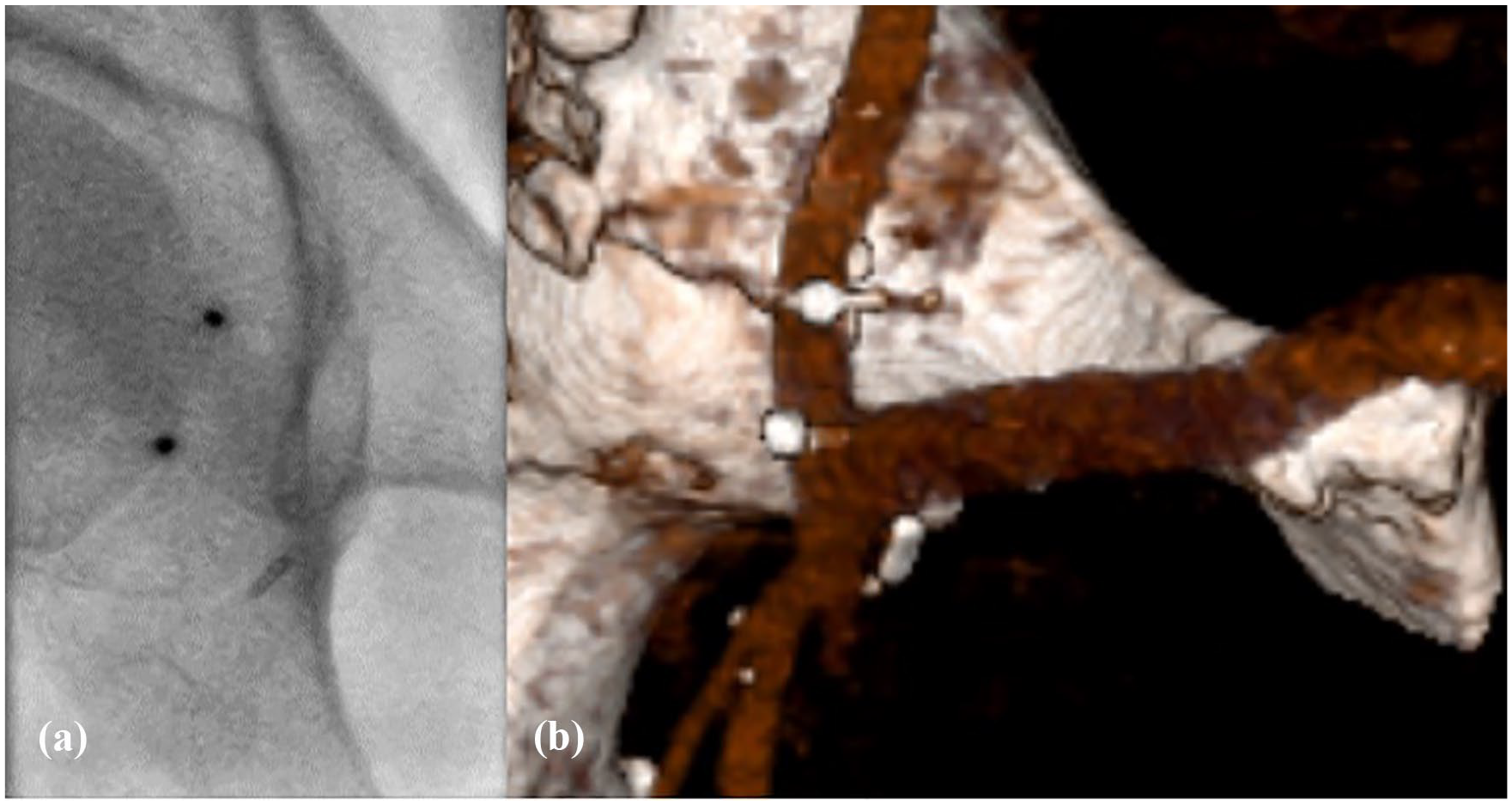
Fluoroscopy-image (a) and corresponding computed tomography-image in volume rendering technique (b) of two correctly deployed devices in a patient with femorofemoral crossover bypass graft and inguinal scarring.
Device undersizing in relation to the introducer sheath proved to be effective as well. In 52 deployments, we used undersized devices up to 2 Fr and no technical failure occurred, both in antegrade and in retrograde approaches.
In the subgroup comparison of technical success, there was no significant difference comparing equally sized and undersized device selection (p = 0.196) and different directions of approach (p = 0.265). Moreover, technical success did not differ in terms of sheath size (p = 0.533), arterial closure device size (p = 0.992), and the patients’ BMI (25.6 ± 2.7 vs 23.9 ± 8.0; p = 0.184). However, in patients with severe calcifications of the CFA, technical failures occurred significantly more often (p = 0.004).
Safety
In total, five major complications due to VCD use occurred, resulting in an overall major complication rate of 2%. We detected four (4%, 4/100) major complications following antegrade CFA puncture (as mentioned above, one was directly associated with technical failure due to sheath kinking) and one (1%, 1/108) following retrograde CFA puncture. Complications were successfully treated with MC or endovascular intervention.
In two cases following antegrade puncture, device migration into the superficial femoral artery (SFA) occurred after initially unimpeded VCD deployment. In one case, we detected the dislodgement immediately after deployment via fluoroscopy. Delayed device migration, 5 weeks after VCD use, was evident in the second case. This patient was clinically apparent with signs of worsening claudication. We detected the migrated implant fluoroscopically. In both cases, we introduced an Amplatz Goose Neck™ Snare (Medtronic, Santa Monica, CA) through an 8 Fr introducer sheath and retrieved the normally formed implant by snare maneuver (Figure 4).
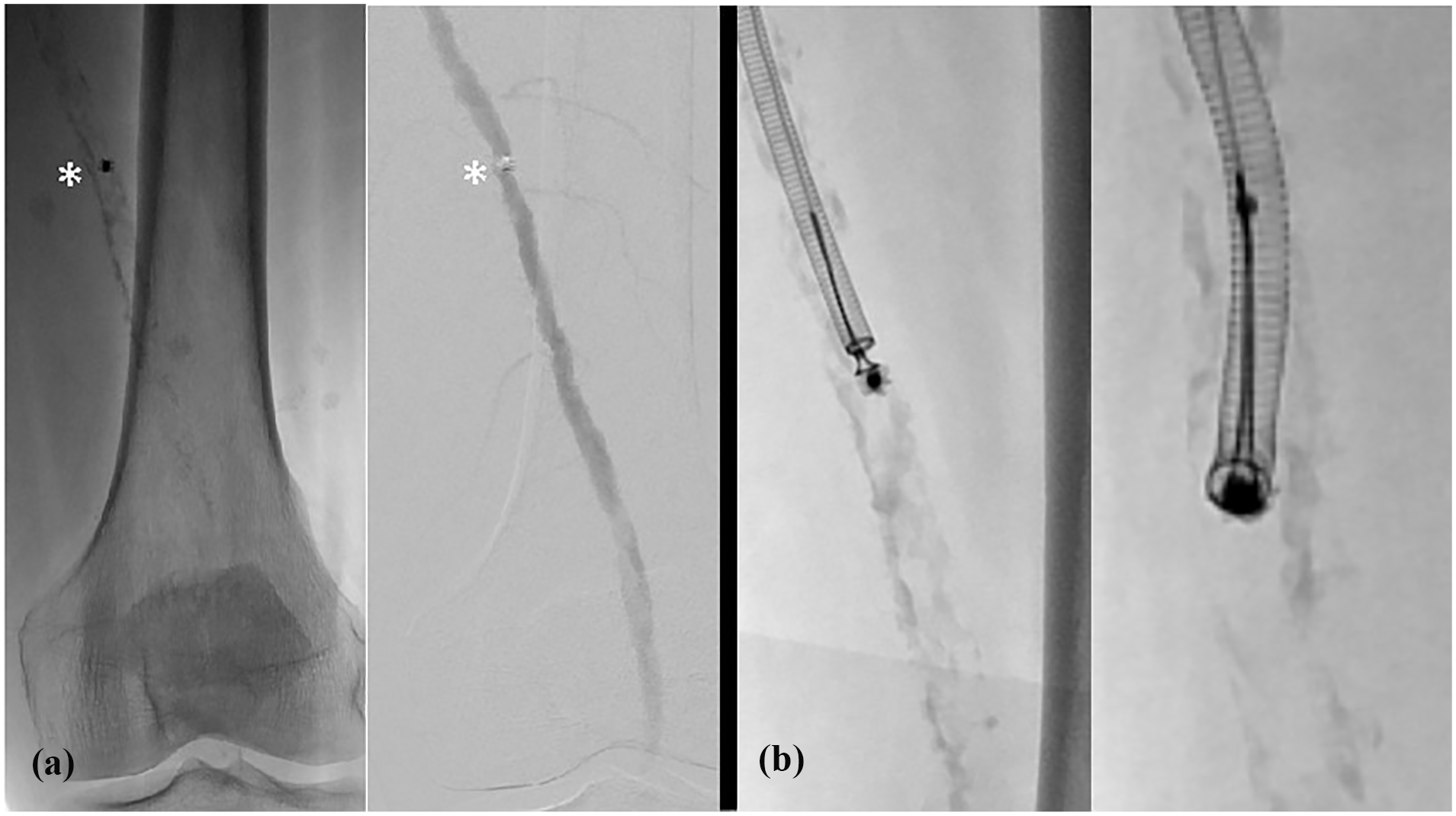
Post procedural worsening of claudication. Fluoroscopy- and Digital subtraction angiography (DSA)-images with delayed implant migration (white asterisk) to the severely calcified SFA (a). Successful fluoroscopy-guided snare retrieval maneuver (b).
Following retrograde VCD use, one secondary hemorrhage with hematoma of >6 cm diameter occurred. We controlled the bleeding by adjusting of the pressure dressing and advising of prolonged bed rest for 24 h.
In 98% of undersized deployments, we attained freedom from major complications. In the retrograde group, we did not observe any major complication following undersized VCD use. In antegrade undersized group, one major complication was identified. An 87 year old patient with severely calcified arteries, who required fully anticoagulation, developed a false aneurysm following an 8 Fr antegrade CFA puncture, which was closed with a 7 Fr VCD. Since the pseudoaneurysm persisted following conservative treatment (i.e. pressure dressing and bed rest for 24 h) and the patient was not suitable for general anesthesia, we successfully excluded the pseudoaneurysm with ultrasound-guided percutaneous thrombin injection (Figure 5).
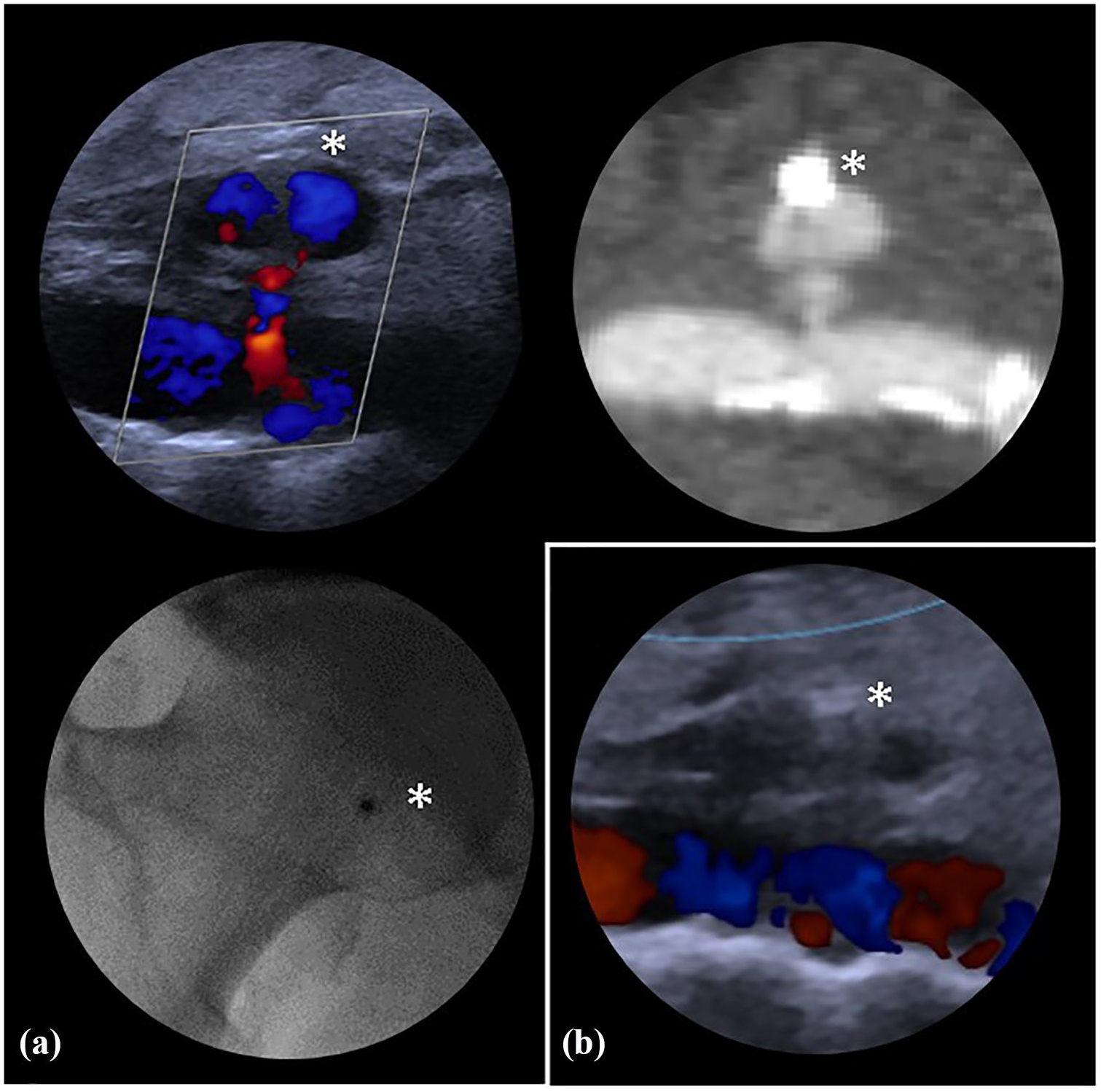
Duplex ultrasound, contrast enhanced computed tomography and fluoroscopy images showing a false aneurysm at the CFA access site. The implant (white asterisk) has shifted off the artery wall, abutting the boundary of the false aneurysm (a). Duplex ultrasound image confirming exclusion of the pseudoaneurysm following thrombin injection (b).
The clinical surveillance and the acquired ultrasound studies, detected no further major VCD related complications. At the access site, patients developed none or less than 5 cm ecchymosis, which resolved without intervention. Small hematomas mainly occurred during the procedure and were not necessarily associated with VCD use. Neither thrombosis, nor AVF occurred. There was no evidence of infection or new-onset neuropathy.
Discussion
Following retrograde CFA puncture, our study confirmed the previously observed robust efficacy and safety results of Celt ACD®.4–6 In 108, retrograde VCD deployments one technical failure in a heavily scarred groin and one major complication with secondary hemorrhage occurred. Hence, our results are consistent with the previously published data, indicating an overall pooled complication rate in retrograde VCD use in the range of 1%–3%. 7 Our findings provide strong evidence, that the novel double-clip based VCD allows immediate and robust hemostasis with a very low complication rate after retrograde puncture up to 9 Fr. These favorable results were achieved in a challenging patient cohort, suffering from significant comorbidities and severe PAD with a high rate of heavily calcified arteries. In accordance with the literature, technical failure rates of the novel VCD were higher following antegrade punctures (i.e. antegrade 5% (5/100) vs retrograde 0% (0/108)).2,7 However, according to our statistical analysis this difference lacked statistical significance (p = 0.265).
In view of the data, provided in previously published review articles, assessing the use of other currently available VCDs in antegrade approaches, we detected comparable VCD related major complication rates following the use of Celt ACD®. Kennedy et al. reported an overall pooled complication rate in antegrade VCD use of 4.6% (95% CI: 2.7%–6.8%). 7 We achieved these favorable results in a challenging patient collective, which seems to be under-represented in clinical trials. 4 These patients often do not meet the inclusion criteria and receive MC instead of VCD closure. 2
Nevertheless, the novel VCD carries specific challenges. The endoluminally-anchored part of the implant poses the risk of intravascular device migration with luminal obstruction and flow limitation.16–18 Furthermore, the device proved inapplicable in acute vascular access angles between 70° and 90°, occurring in antegrade approaches. Thus, we suggest ultrasound guidance for the initial antegrade puncture, in order to achieve an access angle of less than 50°. In borderline antegrade access angles (50°–60°) device undersizing proved to be one trouble-shooting option. With an undersized device, it was easier to move the applicator safely through the sheath lumen. However, to date, undersizing of the VCD represents an off-label-use. Additional traction on the abdominal fat apron by an assistant was also helpful to lower the likelihood of sheath kinking. If a flat access angle is not achievable, we recommend refraining from antegrade Celt ACD® use.
Moreover, it is advisable to avoid re-access directly adjacent to the former access site, since the laser-cutted slits of the star-shaped implant may cause damage to the introducer sheath. Fluoroscopic guidance prior to re-accessing the CFA is helpful to ensure a distance of approximately 5 mm between the previously implanted device and the newly targeted puncture site.
Caution is required in vessels with eccentric calcified plaques, located shortly distant to the access site. After releasing the intraluminal part in stage 1, it is important to ensure that the distal plate is pulled back until it directly abuts the endoluminal wall. Otherwise, the endoluminal wing may be caught on an eccentric plaque. The operator may incorrectly assume the system being located at the vessel wall and start deployment step 2 and 3. Consequently, the implant may be deployed endoluminally with the risk of luminal obstruction or implant migration. In case of doubt, we recommend to check fluoroscopically, if the base plate abuts the wall at the supposed puncture site.
Furthermore, in terms of calcification, our data pinpoints that severe calcification of the target vessel continues to be a key limiting factor in VCD use. Contrary to BMI, sheath size or VCD size, severe calcifications of the CFA proved to be a significant risk factor for technical failure (p = 0.004).
The majority of technical failures and VCD related complications occurred within the first 46 patients. Thus, comparable to other VCDs, our data emphasize the need for appropriate training and careful patient selection to increase the learning curve in antegrade VCD use. 19
Readers may criticize that we did not focus on common criteria for VCD use, for instance, time to ambulation (TTA) and discharge. Indeed, TTA as well as patient and operator comfort were of minor concern to us. Safety was our main rationale for VCD use. This is due to our complex study population: The majority of our patients were multimorbid, elderly patients, scheduled for interventions for severe chronic PAD or acute limb ischemia with, for example, sensory loss, rest pain, pending compartment syndrome, therapeutic heparinization, nonhealing ulcers or gangrene. Moreover, another subgroup received transarterial chemoembolization for liver cancer with a considerable percentage of patients suffering from post-embolization syndrome (e.g. pain and nausea). Furthermore, we used VCDs to close access sites in emergent interventions (e.g. acute bleeding complications due to hemorrhagic diathesis, trauma, surgery, or diagnostic interventions).
Consequently, our patients found themselves in conditions, in which (1) MC may take too long or may be insufficient and (2) pressure dressings may slip off or not reliably prevent local complications due to restlessness or incompliance. Additionally, regardless of our access site, these patients needed further in-hospital monitoring and treatment and were not able to ambulate immediately after intervention. Accordingly, for our patient collective we suggested a longer bed rest for approximately 12 to 24 h.
Limitations
Our study is limited by a small patient cohort, which is composed of a heterogeneous patient population. Furthermore, our study had a non-randomized, single center design. A long-term follow up was not registered. The groups representing inguinal scarring and device under sizing comprise only a relatively small number of patients. Minor complications resolving spontaneously without intervention or surgery, were not specifically recorded, since they lack clinical relevance. Prospective randomized trials comparing different VCDs are needed to evaluate their efficacy and safety performance especially in antegrade punctures for PAD.
Conclusions
The novel double clip-based VCD proved to be effective in 97% of cases. Our study confirms a low VCD related major complication rate and a robust, quick and easy deployment performance following antegrade and retrograde femoral punctures up to 9 Fr, even in challenging clinical scenarios.
Footnotes
Author’s note
I certify that all authors fulfil the conditions for authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study work was in accordance with the Declaration of Helsinki. Our institutional review board provided approval.