
Abstract
Background:
Cannulation of the radial artery can be extremely challenging in infants. Scale ultrasound can provide accurate arterial location and guidance for operators. We hypothesized that scale ultrasound helps increase the initial success rate of radial artery cannulation in this population.
Method:
Seventy-six infants aged 0–3 months who needed arterial puncture after general anesthesia were randomly divided into two groups (1:1 ratio): the scale ultrasound group and the traditional ultrasound group. The primary endpoints were the success rate of the first attempt and the total success rate of arterial cannulation. The secondary endpoints were the time during arterial puncture and the incidence of vascular complications.
Results:
The success rate of the first attempt and the total success rate of arterial cannulation were 92.1% (35/38) versus 50% (19/38) and 100% (38/38) versus 86.8% (33/38) in the scale ultrasound and traditional ultrasound group (p < 0.005), respectively. The median time to ultrasound location, needle entry into the radial artery, and successful cannulation in the scale ultrasound group were significantly shorter than those in the traditional ultrasound group: 10 (8.0, 17.2) s, 15 (11.7, 20) s, and 65 (53.8, 78.5) s vs 30 (26.5, 43.5) s, 35 (23, 51) s, and 224.5 (123.5, 356) s (p < 0.001), respectively. The incidence of hematoma was higher in the traditional group (p < 0.005).
Conclusions:
Scale ultrasound-guided radial arterial cannulation can significantly improved initial success rate and overall success rate, shorten puncture time in infant, compared with that achieved with the use of traditional ultrasound guidance.
Introduction
Radial artery cannulation is a common and important procedure performed in the operating room, emergency room, and intensive care unit to continuously monitor invasive arterial pressure and analyze arterial blood to guide the treatment of electrolyte disturbance and shock. 1 When large fluid shifts or blood losses are expected and frequent blood sampling is anticipated in the perioperative period, the radial artery is the most common site for arterial puncture because of its low complication rate.2–4 Ultrasound guidance has become widespread for radial artery cannulation because it can increase the success rate, decrease the total procedural time, and decrease the incidence of cannulation complications.5–11 However, arterial puncture in infants is particularly difficult due to low blood pressure, small arterial diameter, and weak pulses. Even with ultrasound guidance, arterial cannulation in children can be challenging. 12 The success rate of puncture and the total procedural time with the ultrasound-guided technique are largely dependent on the experience and skill of the ultrasound operator. This may be attributable to the lack of an accurate correlation between the location of the artery on the ultrasound screen and the location of the artery on the ultrasound probe, which limits the advantages of ultrasound-guided radial artery cannulation. We adopted a new technique involving a corresponding scale that was marked both on the ultrasonic probe and the ultrasonic screen. We hypothesized that an accurate correlation between the location of the artery on the scale ultrasound screen and the scale ultrasound probe can provide an accurate arterial location and improved guidance for the operator, thereby increasing the success rate of radial artery puncture and shortening puncture time in infants. The primary endpoints were the success rate of the first attempt and the total success rate of arterial cannulation. The secondary endpoints were the time of ultrasound location, the time of the needle entering the radial artery, and the time of successful cannulation, times of the arterial puncture and the incidence of vascular complications.
Material and methods
Ethics
This study was approved by the Institutional Review Board of Children’s Hospital of Chongqing Medical University, Chongqing City, China (Chairperson Professor Zhongyi-Lu, Ethical Committee N° #287/2019) on 10 January 2020. The trial was registered prior to patient enrollment at chictr.org.cn (ChiCTR2000029353, Principal investigator: Fei Yang, Date of registration: 26 January 2020). Written informed consent was obtained from parents or guardians for research participation. The study started in May 2020 and ended in December 2020.
Confirming the scale on the ultrasonic probe and ultrasonic screen
To confirm the suitability of the ultrasonic probe and ultrasonic screen for infants under the age of 3 months, we measured the inner diameters of 140 radial arteries in infants ranging from 0 to 3 months. The mean inner diameter of the arteries was 1.61 ± 0.34 mm, the mean age was 20 ± 14.5 days, and the mean weight was 3.6 ± 1.39 kg. Based on our statistical results, the inner diameters of the radial and ulnar arteries reported in other literature, 14 and our pre-experiment, we confirmed the scale on the ultrasonic probe as follows (Figure 1): the total length of the scale on the ultrasonic probe was 2 cm, each scale was spaced 2 mm apart, the midpoint of the ultrasonic probe was the zero point, and the scale lines were evenly distributed to the left and right sides in the direction of ultrasonic probe length detection. The left side was marked as −5, −4, −3, −2, and −1; the midpoint of the ultrasonic probe was marked 0; and the right side was marked as 1, 2, 3, 4, and 5. The length, style, direction, and spacing of the scale on the ultrasonic screen correspond to the ultrasonic probe, and the actual distance between the two scales on the ultrasonic screen was determined by the actual magnification of the ultrasound. Ultrasound with scale on the ultrasonic probe and screen was defined as the scale ultrasound. In our study, the ultrasound device (GE venue40; GE, Boston, Massachusetts, USA) with a linear transducer (5–13 MHz), a vascular puncture mode and a depth of 2 cm was applied to localize the radial artery. So this is a constant set up, it didn’t need re-created for each patient unless you change the mode and depth.
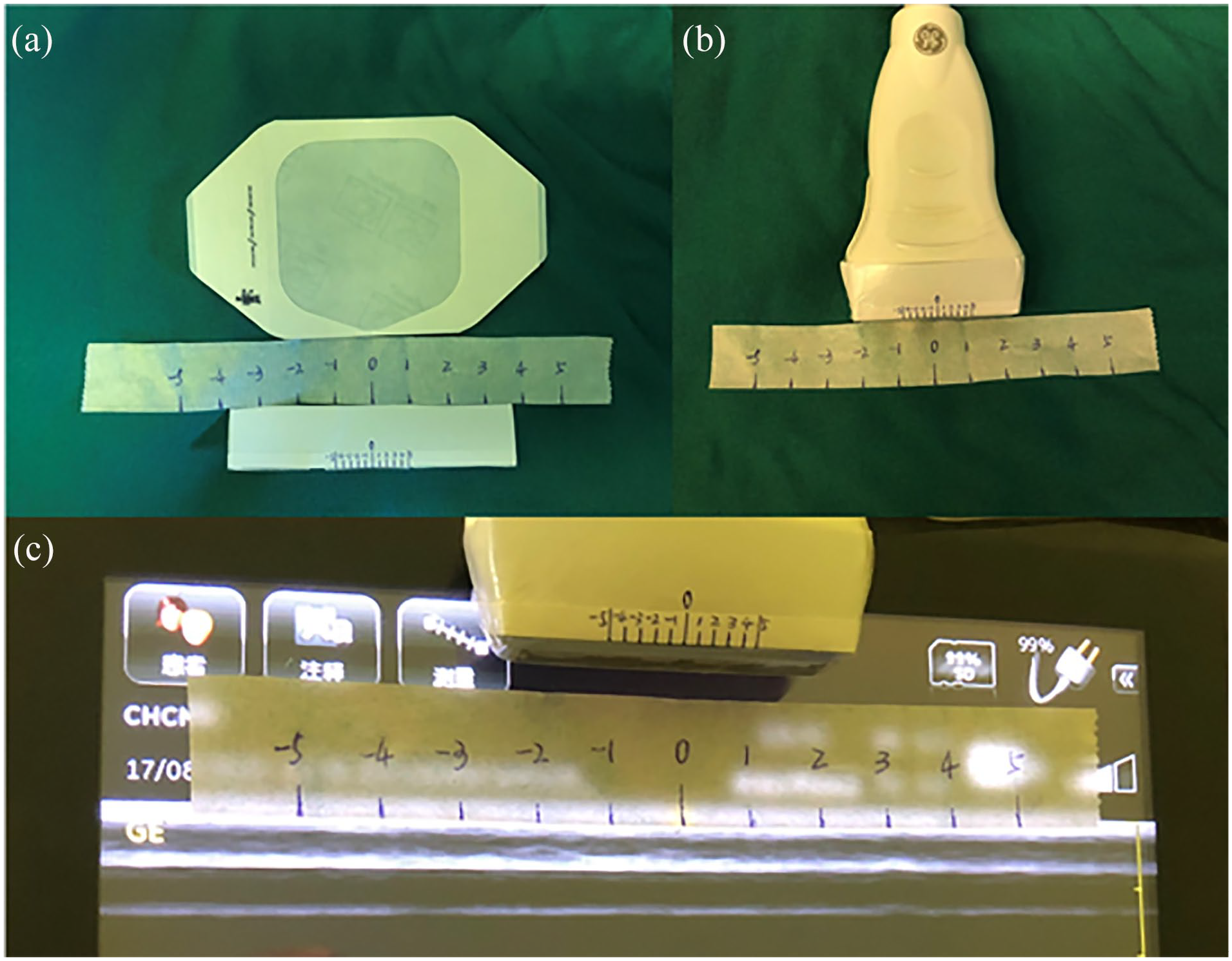
The total length of the scale on the ultrasonic probe was 2 cm, each scale is spaced 2mm apart, the midpoint of the ultrasonic probe is the zero point, and the scale lines are evenly distributed to the left and right sides in the direction of ultrasonic probe length detection. The left side is marked as -5, -4, -3, -2, -1, the midpoint of the ultrasonic probe marked 0, and the right side is marked as 1, 2, 3, 4, 5.The length, style, direction and spacing of the scale on the ultrasonic screen correspond to the ultrasonic probe, and the actual distance between the two scales on the ultrasonic screen is determined by the actual magnification of the ultrasound: (a) The scale on the ultrasonic probe and ultrasonic screen, and the sterile 3M membrane, (b) The scaleas added on the ultrasound probe. Sterile 3M membrane was used to cover the ultrasound probe, (c) the scale on the ultrasonic screen correspond to the ultrasonic probe.
Sample size calculation
The sample size of this study was calculated by our preliminary experiment. Based on our preliminary experiment, the first-attempt success of radial artery cannulation in the traditional ultrasound group and scale ultrasound group was 60% versus 90%. Therefore, we wanted to improve the first-attempt success of radial artery cannulation from 60% to 90%, considering the rate of withdrawal (15%), and the final sample size was identified as 38 for each group.
Arterial catheterization procedure
Infants scheduled for elective surgical procedures who required continuous arterial pressure monitoring were enrolled in this study between May and December 2020 at the Children’s Hospital of Chongqing, China. The inclusion criteria were as follows: age range of 0–3 months and American Society of Anaesthesiologists (ASA) grades I to IV. The exclusion criteria were as follows: arterial puncture received within 1 month before the commencement of the trial, an abnormal Allen’s test, shock, and erosions near the radial artery puncture in the skin. Patients were randomly assigned to the scale ultrasound group or the traditional ultrasound group using a computer-generated random number (1:1 ratio). Group allocation was enclosed in sealed envelopes. At the time of enrolment, the research assistant opened the envelopes, and the researchers enrolled the patient. All patients were enrolled by the researchers, and data were recorded by residents who were blinded to the group allocation. A flow diagram shows the patient selection process (Figure 2).
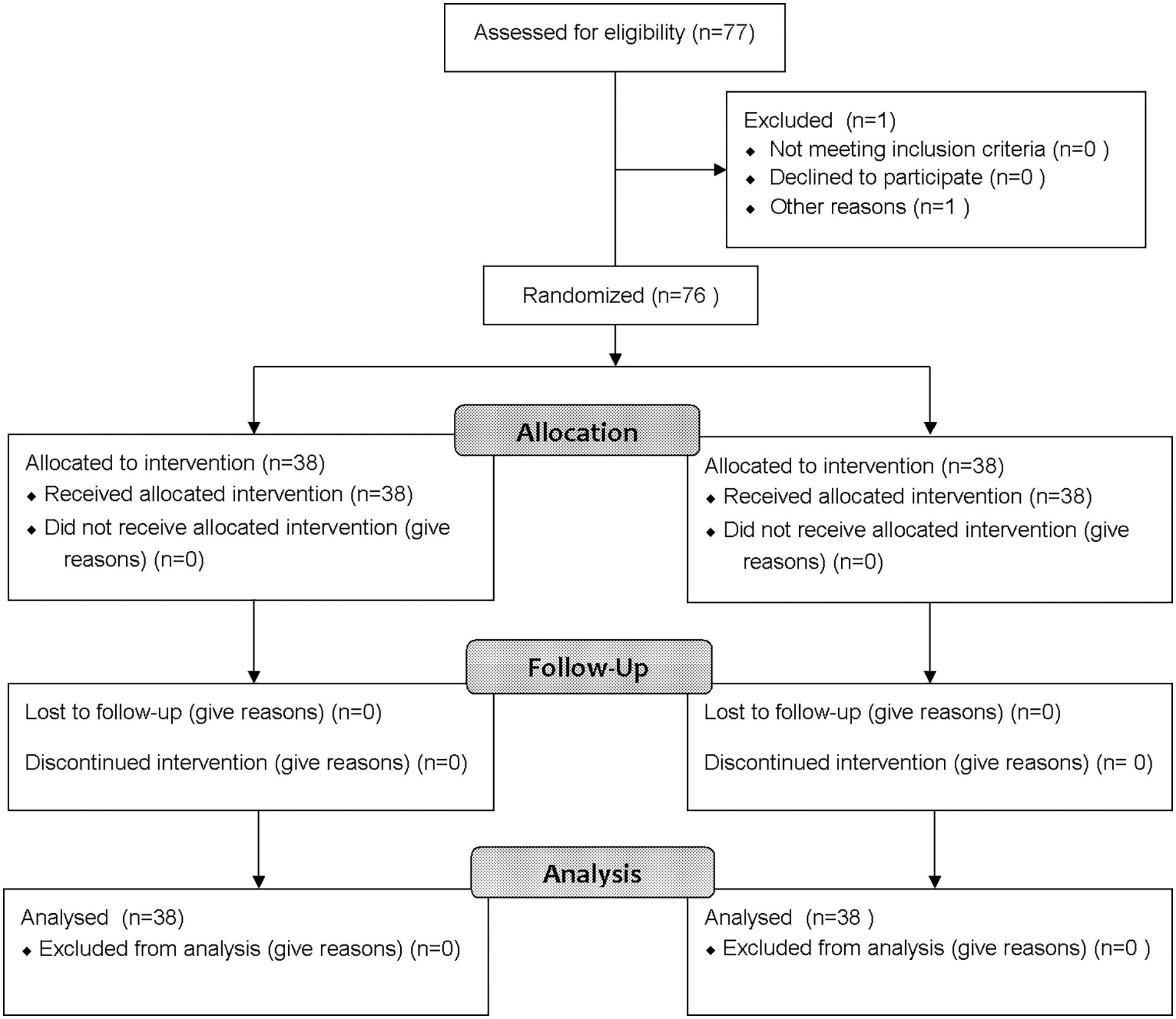
Study flow chart.
Blood pressure, electrocardiogram, and peripheral oxygen saturation were monitored in the operating room. After general anaesthesia was induced, radial artery cannulation was performed. Radial artery catheterization was performed by residents who had experience with at least 50 cases of arterial puncture. The left hand for radial artery puncture was preferred.
The wrist was padded up with a small roll, and the palm of the hand was taped to keep the hand positioned in dorsiflexion. Aseptic preparation of the skin was performed around the insertion site. The aseptic preparation included disinfecting the insertion site with povidone iodine solution and wrapping the ultrasonic probe with disposable sterile covers, sterile gloves, and operating towels. An ultrasound device (GE venue40; GE, Boston, Massachusetts, USA) with a linear transducer (5–13 MHz) and a depth of 2 cm was applied to localize the radial artery. A standard 22-gauge catheter (BRAUN Company, Melsungen, Germany) percutaneously punctured the radial artery using the short-axis, out-of-plane procedure. Patients in the traditional ultrasound group underwent conventional ultrasound-guided radial artery puncture, whereas radial artery puncture was guided by scale ultrasound in the scale ultrasound group. The probe with scale was adjusted such that the radial artery was positioned between any two scales on the ultrasound image (Figure 3(a1), the radial artery is positioned on the ultrasound screen between scale 0 and 1). Subsequently, we chose the position on the ultrasonic probe corresponding to the ultrasonic screen as the arterial puncture point (Figure 3(a2), the arterial puncture point was positioned between scale 0 and 1 on the ultrasonic probe). Between the two scales on the probe, the needle was inserted into the skin at an angle of 30°–45°. Because the scale ultrasound screen and the scale ultrasound probe can provide an accurate arterial location and improved guidance for the operator, we can easily find the location of the needle tip, which was directed toward the arterial lumen when the needle entered the subcutaneous region. Then, the probe was moved proximally 2–3 mm to the radial artery again. According to the scale on the ultrasound screen and the probe, we could easily determine the position and direction of the radial artery (Figure 3(b1) and (b2), the arterial was positioned between scale 0 and 1, closer to scale 0). After adjusting the direction of the tip of the needle and inserting the needle into the radial artery (Figure 3(c1) and (c2)), the needle appeared as a hyperechoic dot on the screen and could be distinguished from the nearby tissue. According to the scale on the ultrasound screen and the probe, adjusting the angle and direction of the incoming needle made the needle come forward to the center of the radial artery. While keeping the needle immobile, the probe was moved proximally a few millimeters until the image of the needle tip disappeared, the radial artery was repositioned according to the scale on the ultrasound image, and the needle was inserted toward the corresponding scale on the ultrasound probe until the image of its tip reappeared. This procedure was repeated until the needle was inserted fully into the radial artery (Figure 3(d1) and (d2)). Then, the stylet was removed, and a pressure sensor was connected to monitor blood pressure.
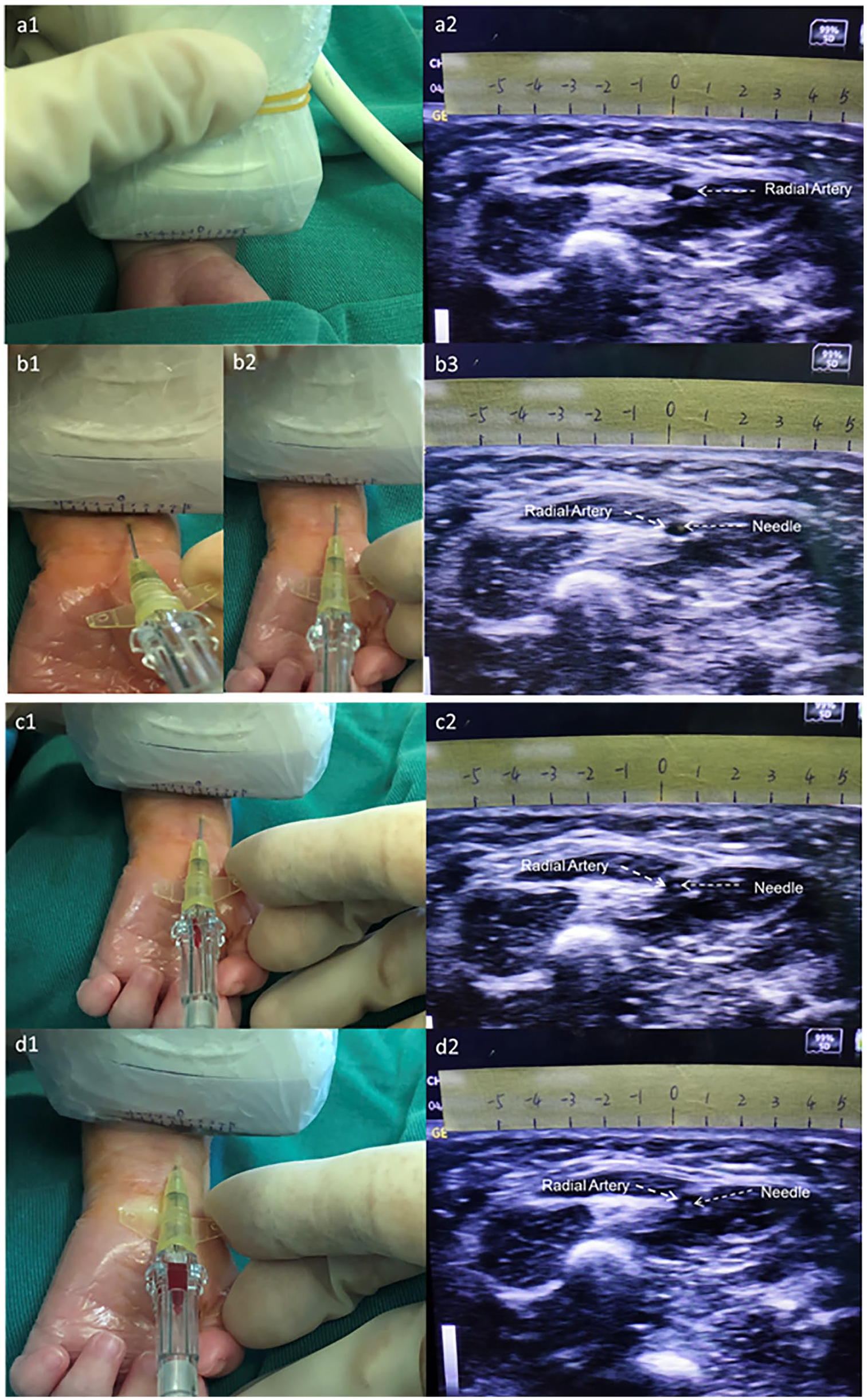
Puncture steps and corresponding ultrasound images: (a1) Ultrasonic probe with a sterile cover and sterile coupling agent is placed in the short axis above the distal end of the selected radial artery, moving the probe the radial artery was positioned between any two scales on the ultrasound image, (a2) Ultrasonic images corresponding to a1 (the radial artery was positioned between 0 to 1 on the ultrasonic screen), (b1) chose the position on the ultrasonic probe corresponding to the ultrasonic screen as the arterial puncture point.( the arterial puncture point was positioned between 0 to 1 on the ultrasonic probe), (b2) the probe was moved proximally 2–3 mm, according to the scale on the ultrasound screen and the probe we can easily determine the position and direction of the radial artery, (b3) Ultrasonic images corresponding to b2, (c1) The needle entered into the radial artery. c2, Ultrasonic images corresponding to c1, (d1) the needle was inserted fully into the radial artery, (d2) Ultrasonic images corresponding to d1.
Data acquisition
The patient’s general condition was recorded by residents who were blinded to the group allocation, including the patient’s age, weight, sex, ASA physical status, heart rate, mean arterial pressure, depth from the skin to the radial artery, and inner diameter of the radial artery. The primary endpoints were the success rate of the first attempt and the total success rate of arterial cannulation. The secondary endpoints were the time of ultrasound location, the time of the needle entering the radial artery, and the time of successful cannulation, times of the arterial puncture and the incidence of vascular complications. Successful puncture was defined as the arterial waveform being verified after arterial cannulation. Puncture failure was defined as more than three attempts to achieve cannulation of the radial artery or any attempts requiring more than 10 min. The time of ultrasound location was defined as the time from the placement of the ultrasound probe on the skin to the insertion of the needle into the skin. The time of the needle entering the radial artery was defined as the time the skin was punctured by the needle to the time the needle entered the radial artery. The time of successful cannulation was defined as the time between when the needle was inserted into the skin and the time the arterial waveform could be verified after arterial cannulation. Complications were recorded, including bleeding and hematoma formation. Ultrasound was used to monitor hematoma formation after puncture.
Data analysis
Minitab 18.0 (Minitab Inc., USA) was used for statistical analysis. Descriptive statistics of normally distributed variables were calculated using counts and means ± SD. Descriptive statistics of nonnormally distributed variables were calculated using the median with the interquartile range. Normality of the data was evaluated by the Anderson–Darling test. If the data exhibited a normal distribution, a two-tailed Student’s t-test was used to measure the difference between groups; otherwise, a nonparametric test was used. The chi-square test was used for other categorical data, such as sex and ASA status. Fisher’s exact test was used to determine the successful puncture rate and the incidence of adverse reactions, and the differences in incidence and associated 95% CI were calculated. Statistical significance was defined as a p-value less than 0.05.
Result
Demographic characteristics
A total of 76 patients were enrolled in the randomized study between May and December 2020 (77 patients was assessed for eligibility, one case was ruled out due to surgical reasons). There were 38 patients in the scale ultrasound group and the traditional ultrasound group. The patients’ baseline characteristics are shown in Table 1. There were no differences in the age, weight, sex, ASA physical status, heart rate, mean arterial pressure, depth from the skin to the radial artery, or inner diameter of the radial artery of the patients (Table 1).
Basic characteristics of all patients enrolled in the study.
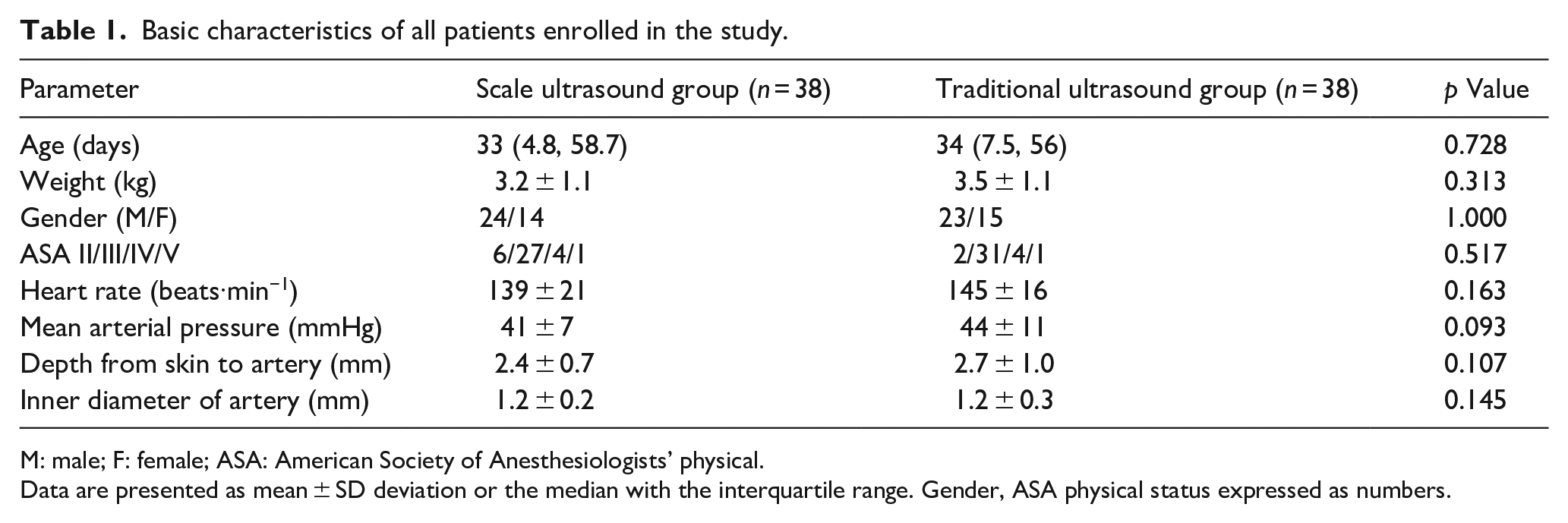
M: male; F: female; ASA: American Society of Anesthesiologists’ physical.
Data are presented as mean ± SD deviation or the median with the interquartile range. Gender, ASA physical status expressed as numbers.
Primary endpoints
The success rate of the first attempt and the total success rate of arterial cannulation were 92.1% (35/38) and 100% (38/38) in the scale ultrasound group and 50% (19/38) and 86.8% (33/38) in the traditional ultrasound group (p < 0.005), respectively (Table 2). In the traditional ultrasound group, five patients experienced failure. One of them was a 31-day-old premature boy with a weight of 3.7 kg who was hospitalized due to intestinal obstruction and who was to undergo an exploratory laparotomy. The inner diameter of her radial artery was 0.9 mm, and the depth from the skin to the radial artery was 1.1 mm. The puncture time for this boy was more than 10 min, and two puncture attempts were required. Another patient was a 53-day-old boy with a weight of 5.5 kg who was hospitalized due to retroperitoneal tumour and who was to undergo an exploratory laparotomy. The inner diameter of her radial artery was 1.2 mm, and the depth from the skin to the radial artery was 2.5 mm. The puncture time for this boy was more than 10 min, and three puncture attempts were required. The other patients were 8-, 30- and 73-day-old boys, with weights of 4.2, 3.5, and 4 kg; inner diameters of the radial artery of 1.5, 1.2, and 1.7 mm; and depths from the skin to the radial artery of 4.7, 2.5, and 4.2 mm, respectively. Four attempts to cannulate the radial artery were made before succeeding in each patient.
Comparison of success rate of cannula insertion, location time, puncture time, arterial puncture times and complications between the two groups.
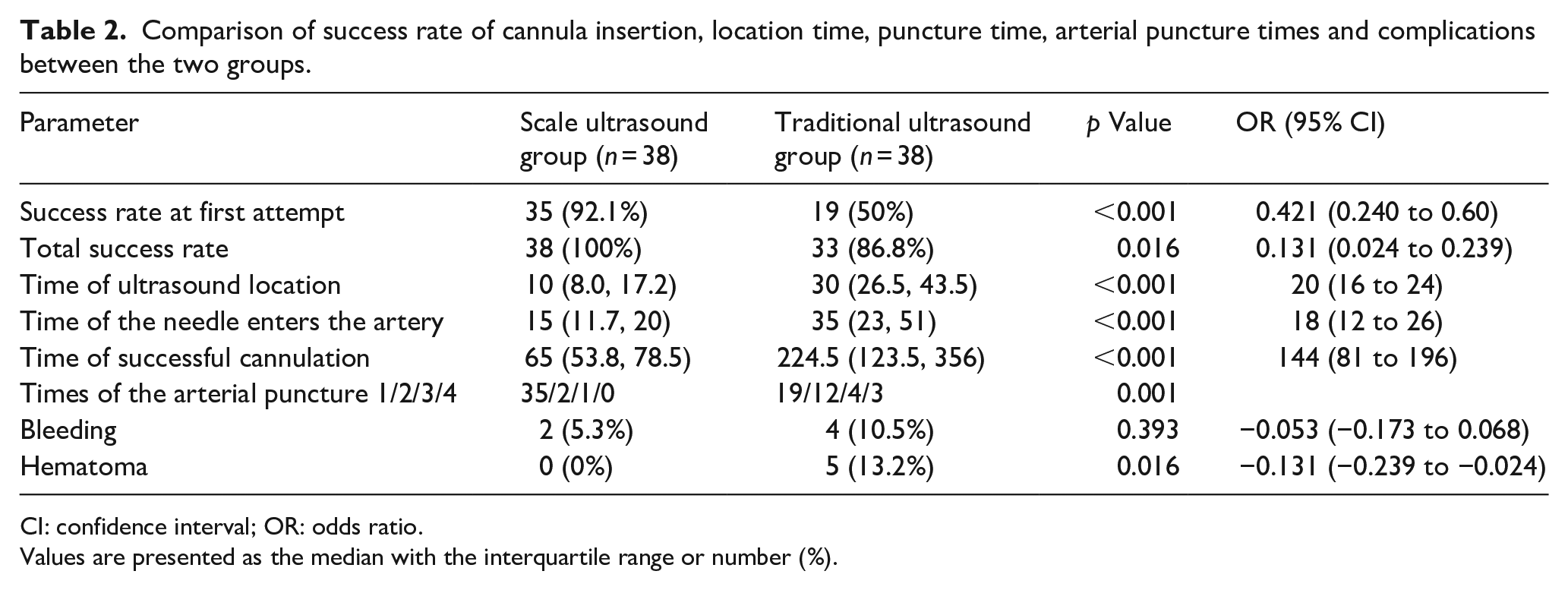
CI: confidence interval; OR: odds ratio.
Values are presented as the median with the interquartile range or number (%).
Secondary endpoints
The median time of ultrasound location, needle entry into the radial artery and successful cannulation in the scale ultrasound group were significantly shorter than those in the traditional ultrasound group: 10 (8.0, 17.2) s, 15 (11.7, 20) s and 65 (53.8, 78.5) s versus 30 (26.5, 43.5) s, 35 (23, 51) s, and 224.5 (123.5, 356) s (p < 0.001, Table 2), respectively. The times of the arterial puncture in the scale ultrasound group was significantly lower than that in the traditional ultrasound group (p = 0.001; Table 2).
The incidence of hematoma was higher in the traditional group (0 of 38 (0%) vs 5 of 38 (13.2%), p = 0.016; Table 2). There was no significant between-group difference in the incidence of bleeding (2 of 38 (5.3%) in the scale ultrasound group vs 4 of 38 (10.5%) in the traditional group, p = 0.393; Table 2).
Discussion
Arterial puncture in infants is particularly difficult due to low blood pressure, small arterial diameter, and weak pulses. Ultrasound guidance is beneficial to improve the success rate of infant arterial puncture. However it is very difficult to find the needle tip in ultrasound images in infants, which is also a key factor in determining the puncture success rate and puncture time. An accurate correlation between the location of the artery on the scale ultrasound screen and the scale ultrasound probe can provide accurate arterial location and guidance for the operator. In clinical applications, we found that scale ultrasound can help operators find the tip of the needle more quickly and improve the success rate of punctures in infants, at the same time, scale ultrasound does not require additional invasive procedures and does not increase the risk of infant artery puncture. In our study, the success rate of the first attempt and the total success rate of arterial cannulation in the scale group were higher than those in the traditional ultrasound group, and higher than those in other studies.5,6,9,13,14 In our study, the success rate of the first attempt in the traditional ultrasound group was lower the other study. 15 This may be related to the higher difficulty of puncture due to the younger age of the included patients in our study.
In the scale ultrasound group, the time of ultrasound location, the time of the needle entering the radial artery, and the time of successful cannulation were approximately 20, 18, and 144 s shorter, respectively, than in the traditional ultrasound group. Scale ultrasound can improve the efficiency of arterial puncture and shorten the puncture time, which may be related to the rapid positioning and accurate guidance provided by scale ultrasound.
The dynamic needle-tip positioning technique has been shown to significantly improve the clinically relevant aspects of radial artery catheterization.8,11 The first step involves localization of the puncture point for radial artery puncture. Compared with traditional ultrasound, when the ultrasonic probe is placed on the wrist, scale ultrasound can be used to more quickly and accurately locate the projection point on the skin surface of the midpoint of the radial artery, and then quickly determine the puncture point, without repeatedly moving the ultrasonic probe to find the puncture point, similar to traditional ultrasound. The second step involves puncture of the radial artery. Since scale ultrasound has a one-to-one corresponding scale for the direction on the ultrasonic probe and ultrasonic screen, we can easily and conveniently determine the direction of needle-tip puncture according to the position of the needle entering the radial artery after the skin. The final step involves the insertion of the cannula into the radial artery. We recommend that the needle with the catheter be inserted into the radial artery as far as possible under the guidance of ultrasound, and that the needle core be removed; then, the cannula can be inserted into the radial artery. 8 Scale ultrasound helps one properly adjust the angulation of the needle and maintain information on the position of the needle tip in real time. Thus, scale ultrasound can effectively shorten the time of arterial puncture and improve the success rate of the first attempt. Song et al. 12 compared the short-axis/out-of-plane and long-axis/in-plane techniques for ultrasound-guided arterial cannulation in children and found that there was no significant difference in the total time of successful cannulation between the two techniques. Regardless of the type of puncture chosen, long axis or short axis, scale ultrasound is an effective auxiliary for arterial puncture.
For the teaching of arterial puncture in children, beginners who are inexperienced with ultrasound-guided downward arterial puncture often take a long time to find the tips and have a long duration, a low success rate, and an increased risk of patient injury. Scale ultrasound is an effective teaching tool that can help them to find the tip of the needle more quickly and to trace the artery’s ultrasound image more easily. It can not only improve the learning enthusiasm of beginners, but also minimize the risk of patient injury. Therefore, it can also be promoted as a teaching tool.
A limitation of this study was that we did not include children older than 3 months because we believe that children under 3 months of age undergoing artery puncture represent the most difficult form of this procedure. If scale ultrasound is beneficial to patients of this age undergoing arterial puncture, then scale ultrasound should be conducive to patients of other ages undergoing artery puncture; this hypothesis needs further experimental confirmation. Of course, when scale ultrasound is used for arterial puncture for patients of other ages, the scale label might need to change; notably, this study provides a new idea for ultrasound-guided arterial puncture. Additionally, only residents who had performed at least 50 arterial punctures participated in this study. Therefore, we cannot assess how much the success rate was influenced by different levels of expertise.
Conclusions
Thin blood vessels and narrow wrist of infants greatly increase the difficulty of radial arterial cannulation. Scale ultrasound can provide accurate arterial location and guidance for operators, can significantly improved initial success rate and overall success rate, shorten puncture time in infant, decreased incidence of cannulation-related complications, compared with that achieved with the use of traditional ultrasound guidance. It can alleviate the suffering of infant, greatly improve the quality of medical care, and is worthy of wide recommendation.
Footnotes
Acknowledgements
We would like to acknowledge the support of the staff from the Anaesthesia and Gastroenteric neonatal Surgery Department at the Children’s Hospital affiliated with Chongqing Medical University, China, for their cooperation in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.