
Abstract
Extracorporeal membrane oxygenation (ECMO) is required for patients with refractory cardiac or respiratory failure. Inadequate securement of ECMO cannulae may lead to adverse events, ranging from line kinking to catastrophic accidents, such as air entrainment into the circuit or massive bleeding. Furthermore, the micro-motion of the cannulae at the entry site might increase the risk of local infections. Since 2015, we implemented a written protocol for management of ECMO cannulae and tubing, which specifically includes the securement of each cannula with three sutureless devices. The aim of the present study was to retrospectively assess cannulae micro-motion and the rate of bleeding events at the insertion site. Secondarily we aimed to evaluate the impact of prone positioning maneuvers during ECMO on these events. We performed a single-centre retrospective analysis of prospectively collected data on nursing care of ECMO cannulae. We included adult patients treated with veno-venous (V-V) or veno-arterial (V-A) ECMO between 2015 and 2018 in our general intensive care unit. The distance between the insertion site and the end of the wire-wound part of the cannula was recorded daily. Variations of this distance (defined as “cannula micro-motion”) were recorded. Forty-five ECMO consecutive adult patients (40 V-V and 5 V-A) were included. No accidental cannula dislodgement was recorded. Median daily “cannula micro-motion” was 0.0 (−0.5 to 0.2) cm, without any significant difference between ECMO configuration, cannula type, and insertion site. Twelve patients (26%) presented at least one bleeding episode at cannula insertion site, none of which required surgical intervention. In the subgroup of patients who underwent prone positioning, no difference in cannulae micro-motion was recorded. An ECMO nursing protocol for cannulae management providing sutureless devices for cannula and tubing securement allows safe line stabilization, with the potential to reduce complications related to ECMO vascular access.
Introduction
Extracorporeal membrane oxygenation (ECMO) provides cardiac or respiratory support to critically ill patients when maximal conventional support fails.1–4
Ensuring the vascular access is a fundamental of ECMO management.5,6 Adverse events related to ECMO circuit or components have been described in the Extracorporeal Life Support Organization (ELSO) registry. 9 Serious complications include partial or complete cannula dislodgement with resultant loss of ECMO blood flow, air entrainment, and/or catastrophic bleeding.3,7 Effective securement of cannulae and ECMO tubing to a surface, such as the patient’s limb, is mandatory to prevent line movement, kinking, or dislodgement.
Inadequate anchorage of the cannulae might also lead to an increased risk of infection, as cannula micro-motion may facilitate the entry of skin-borne organisms from the insertion site to the bloodstream, as it is described with smaller intravascular catheters.8,9 Cannula-associated infections are described in up to 10% of ECMO patients and represent a diagnostic challenge because of the difficulty of obtaining samples for cultures.10,11 Despite the universal acceptance of the importance of ECMO cannula securement, there are currently few data on best practice for the effective dressing and securement of ECMO cannulae.
The main objective of this study was to retrospective analyze data related to nursing management of cannulae in patients undergoing ECMO support in a general intensive care unit, with an emphasis on cannulae micro-movement at the insertion site. Secondary aim was to investigate the incidence of bleeding from ECMO cannula sites and to verify if the application of prone position in ECMO patients could be a risk factor for cannula dislodgment.
Methods
Study design and setting
We performed a single-centre retrospective study in the General Intensive Care Unit (ICU) of the University Teaching Hospital San Gerardo (Monza, Italy). This study was a secondary analysis of the ConnECMO study, which was approved by the local Ethics Committee (Comitato Etico Monza e Brianza, ref 1695). We included all consecutive adult patients, admitted to our ICU from January 2015 to December 2018, who were treated with veno-venous (V-V) ECMO or veno-arterial (V-A) ECMO support.
ECMO management
For V-V ECMO, femoro-femoral and femoro-jugular approaches are usually preferred, whereas femoro-femoral configuration is used in V-A ECMO. All the cannulations are performed percutaneously by intensivists, using real-time ultrasound and a classical or modified Seldinger technique. 12 After ECMO implantation, a suture point is secured at the end of the wire-wound part of the cannula.
Nursing protocol for ECMO cannula management
Cannulation sites are routinely examined to rule out signs of infection or bleeding. Maintenance of the ECMO cannula is performed in adherence to our ICU protocol and policy as follows:
- Disinfection of the cannula insertion site is performed with disposable sticks of Chlorhexidine Gluconate (CHG) 2% in 70% isopropyl alcohol (IPA).8,9
- A transparent semipermeable dressing with 2% CHG (Tegaderm CHG, 3M—USA) is the standard of care if no bleeding at the cannula entry site. Routine cannula dressing changes follow the most recent guidelines to prevent bloodstream infection.8,9 Transparent dressing changes are scheduled every 7 days or sooner in case of loss of dressing adherence or soiling.
- Every ECMO cannula is secured using a suture-less device (GRIP-LOK 3300MWA–Vygon, France or WingGuard®, Centurion, USA) in three different points for (venous or arterial) femoral cannulae. The cannula and the tubing are maintained along the leg axis. When a cannula is placed in the internal jugular vein, it’s fixed to the patient’s head with a bandage (see Figures 1 and 2). In addition, the ECMO tubing is fixed with two sutureless devices on the shoulder and on the chest. The change of these sutureless devices is scheduled every 7 days or sooner if they lose their adhesive power.
- Thin hydrocolloid dressing (Duoderm extrathin 9200, Convatec—UK) is applied on the skin in contact with the ECMO tubing to prevent pressure ulcer. 13
- The distance between the insertion site and the end of the wire-wound is recorded every morning by the ICU nurse, to allow recognition of any cannula movement (Figure 3)
- Thigh and leg circumference are measured daily to early detect hematoma formation below the insertion site and/or obstruction to venous return from the distal leg (Figure 4).

Care of femoral cannulae in veno-venous V-V ECMO. The figure shows medication and fixation of the ECMO cannulae and tubing along the leg axis.

Care of jugular cannula in V-V ECMO. Medication and fixation of the ECMO cannulae and tubing along the head, shoulder, and chest are displayed.
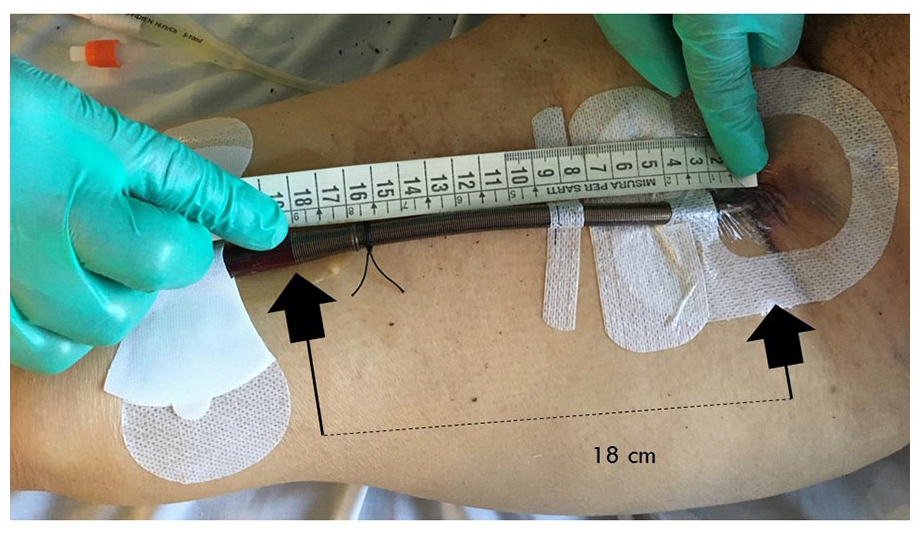
Measurement of distance between the insertion site and the end of the wire-wound to monitor cannula micro-motion.
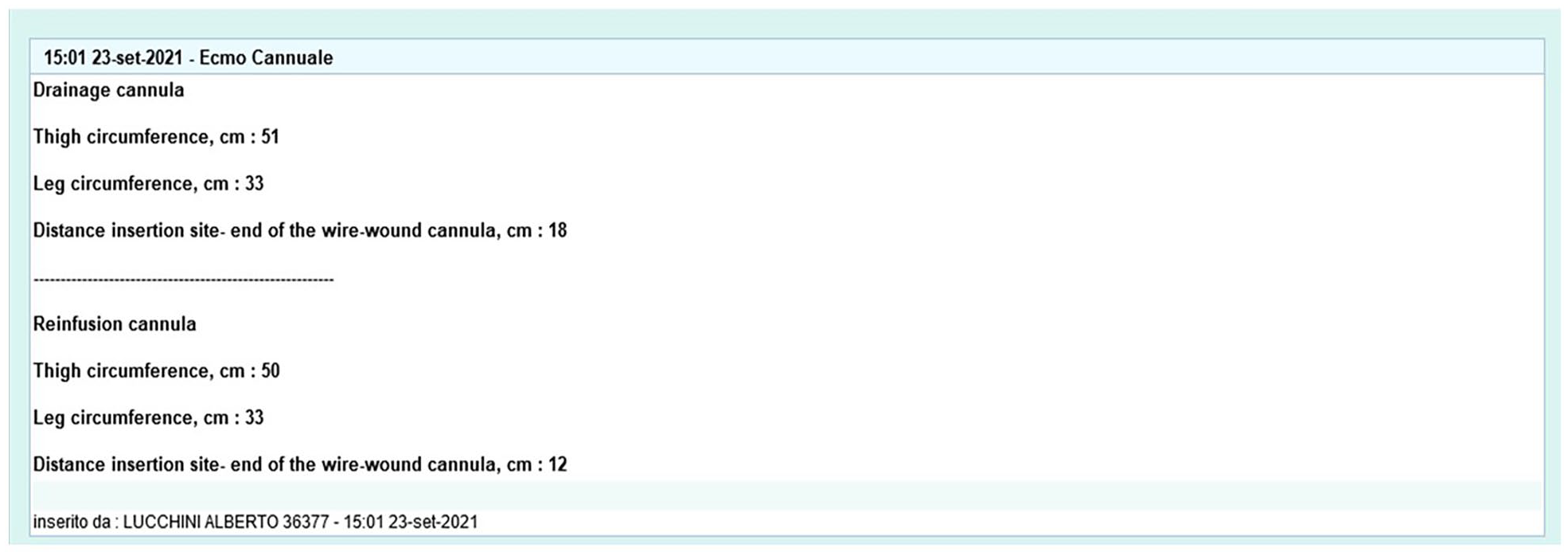
“Nursing card” used for daily cannula monitoring.
Data collection
We retrospectively collected data from the “ECMO cannula nursing” form, a section of our electronic health record (Innovian SUITE® patient management system, Drager Medical GmbH, Lubeck, Germany) which was created to prospectively collect this information. Every day, the ICU nurse used this form to record (for both ECMO cannulae) the distance between the insertion site and the end of the wire-wound, thigh and leg circumference, bleeding episodes, ECMO blood flow, activated clotting time (ACT), International Normalized Ratio (INR), activated Partial Thromboplastin Ratio (aPTT), platelet (PLT) count, and unfractionated heparin dose.
We defined as “cannula micro-motion” the absolute difference between the cannula’s reference distance (insertion site—end of the wire-wound) and the daily measurement of this parameter reported by ICU nurse. A positive value indicates that the cannula has moved outward from the patient, whereas a negative value means that the cannula has advanced through the entry site.
Statistical analysis
Continuous variables were expressed as median (interquartile range). Categorical variables were expressed as count (proportion). Difference in continuous variables between the patient groups (V-A vs V-V group and PP vs supine group) was explored by Mann-Whitney U test. Difference among categorical variables between the two groups was tested using the Chi Square test. Statistical significance was considered in the presence of a p-value < 0.05 (two-tailed). Spearman’s correlation analysis was utilized, and p-value < 0.01 (two-tailed) was considered significant. Statistical analysis was performed using SPSS 24.0 (IBM, Armonk, NY), and Microsoft Excel for Mac 2017, version 15.32 (Microsoft Corporation, Redmond, WA).
Results
During the study period 45 patient with ECMO were analyzed, for a total of 570 ECMO days. Characteristics of the study population are provided in Table 1.
General characteristics of all enrolled patients.
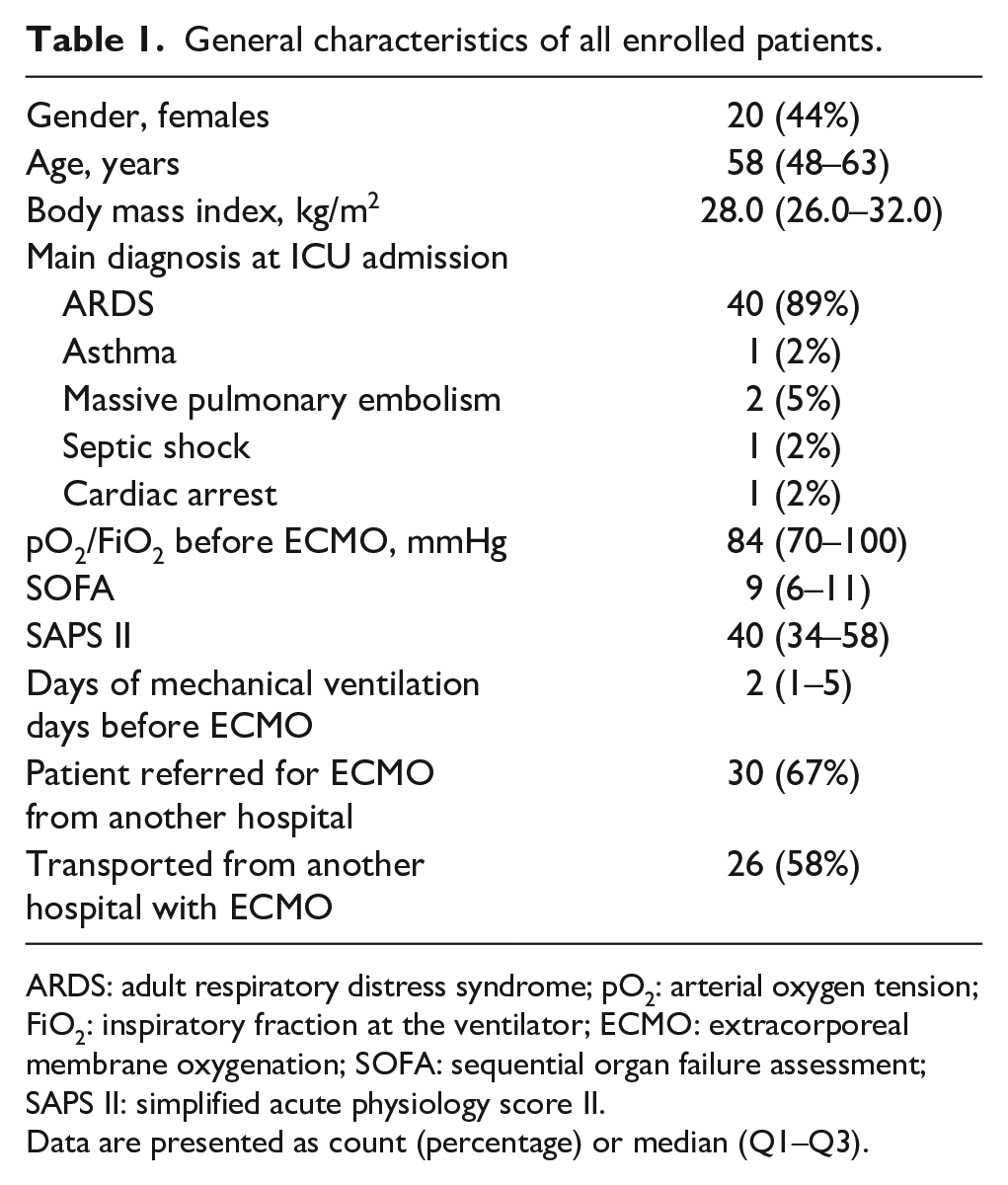
ARDS: adult respiratory distress syndrome; pO2: arterial oxygen tension; FiO2: inspiratory fraction at the ventilator; ECMO: extracorporeal membrane oxygenation; SOFA: sequential organ failure assessment; SAPS II: simplified acute physiology score II.
Data are presented as count (percentage) or median (Q1–Q3).
Forty patients underwent V-V ECMO and five patients V-A ECMO. ARDS was the primary diagnosis in all V-V ECMO patients, while the most frequent indication for V-A ECMO was pulmonary embolism (40%). More than a half of patients were retrieved by our mobile team after ECMO cannulation outside hour hospital. Median ECMO duration was 11 (5–16) days. Twenty-one patient underwent prone position during V-V ECMO (Prone group), whereas the remaining 19 were managed in the supine position (Supine group). Thirty patients (67%) were discharged alive from ICU. Data from the “ECMO cannula nursing” form were available for all the 570 ECMO days. No accidental cannulae dislodgement was recorded.
Global data about cannula management, daily recorded by nurses, are provided in Table 2.
Cannula insertion site, characteristics, monitoring, and micro-motion.
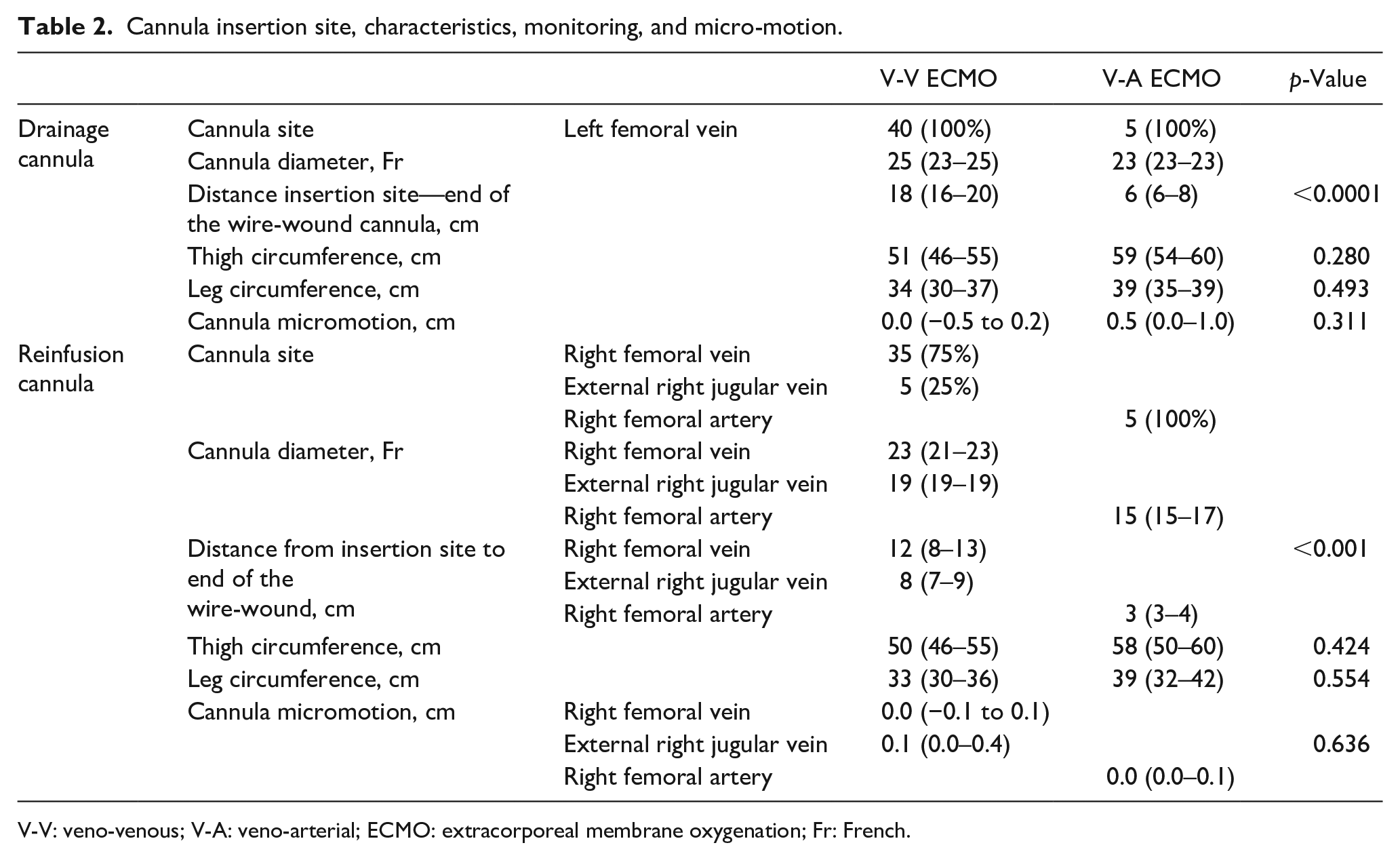
V-V: veno-venous; V-A: veno-arterial; ECMO: extracorporeal membrane oxygenation; Fr: French.
Median daily “cannula micro-motion” was 0.0 (−0.5 to 0.2) cm, without any significant difference between ECMO configuration, cannula type, and insertion site. In patients who underwent femoro-femoral V-V ECMO (drainage cannula in left femoral vein and reinfusion cannula in right femoral vein) we found a correlation between patient’s height and distance between the insertion site and the end of the wire-wound drainage cannula (Spearman’s correlation coefficient: −0.283 (p < 0.001) for drainage cannula, −0.572 (p < 0.001) for reinfusion cannula).
Median ECMO blood flow was 3.4 (2.9–3.9) l/min. Heparin total daily dose was 23,500 (14,900–30,200) International Units, resulting in an ACT of 170 (158–188) s and an aPTT ratio of 1.37 (1.16–1.69). Median INR was 1.1 (1.0–1.3) and platelet count 144,000 (93,800–198,000)/mm3. A total of 12 patients (26%) presented at least one bleeding episode at cannula insertion site, requiring renewal of the dressing before the planned 7 days. None of these episodes required surgical intervention.
During the study period, 21 (53%) patients on V-V ECMO were placed in prone position (PP) for at least one cycle. ECMO configuration was femoro-femoral in 19 of these patients. No significant differences in daily “cannula micro-motion” of drainage cannula were observed in patients who underwent prone positioning compared to controls managed in the supine position. Micro-motion of the drainage cannula was −0.1 (−0.5 to 0.1) cm in the Prone group versus 0.0 (−0.1 to 0.2) cm in the Supine group (p = 0.135). “Cannula micro-motion” was 0.1 (−0.1 to 0.5) cm for Prone patients versus 0.0 (−0.3 to 0.3) cm in the Supine group (p = 0.535) for femoral reinfusion cannulae, and 0.0 (0.0–0.0) cm versus 0.1 (0.1–0.5) cm (p = 0.750) for jugular reinfusion cannulae, respectively.
Discussion
In this retrospective cohort study, the application of a written nursing protocol for the management of vascular access for ECMO allowed safe line stabilization. No cannula dislodgement was recorded, and cannulae micro-motion was negligible, also in patients who underwent prone positioning during ECMO. Furthermore, we recorded a low rate of reversible bleeding episodes at the insertion site.
To our knowledge, this is the first “in vivo” study that analyzed the impact of a predefined protocol to manage dressing and securement of ECMO cannulae to prevent adverse events (cannula dislodgement, “cannula micro-motion,” and bleeding). Despite the universal acceptance of the importance of ECMO cannula securement, there are currently no data on best practice for the effective dressing and securement of ECMO cannulae and circuit. ELSO recommendations suggest covering ECMO cannula sites with transparent dressings to protect from extrinsic contamination.3,14 Use of CHG 2% and IPA 70% for disinfection of ECMO cannula entry site is derived from consensus guidelines applicable to smaller intravascular devices, even there is not ECMO-specific guidelines.8,9 Standard tapes, adhesive bandages, or sutureless devices may be employed to secure ECMO cannulae and tubings. 15 Our centre implemented the use of sutureless securement devices for ECMO cannulae and tubing since 2003. These devices are simple and quick to apply, can remain in place for several days and avoid skin suturing, which might cause bleeding and incidental perforation of ECMO cannulae. Furthermore, they allow ICU nurses to simply readjust ECMO tubing as needed. Our policy provides for the use of a suture point at the end of the metal spiral of the cannula combined with the use of three sutureless systems (the first positioned near the cannula-circuit connection, the second one on the thigh, and third one on the leg). Bull et al. 15 reported that a sutureless securement device or adhesive fabric tape/bandage were used by 16% and 10% of the centres involved in an international survey, respectively. Twenty-six percent of the centers were reported to use more than two points of fixation, 48% routinely used two fixation points along femoral line, whereas a minor fraction of centers (21%) used only one. 15
Commercial sutureless devices were tested in a recent study. 16 These devices were reported to be significantly “stronger” than the standard method using adhesive bandage. For this reason, as per our protocol, we use (three) sutureless securement devices to minimize the risk of cannula displacement or removal. Furthermore, the fixing of ECMO tubing along the limbs aims to minimize any impact of patient movements on ECMO drainage and, consequently, on ECMO blood flow. 17 The overall “cannula micro-motion” in the enrolled patients was few millimeters, both for the drainage and reinfusion cannula. The distance between insertion site and the end of the wire-wound cannula (cm) of drainage cannulae was different for V-V and V-A ECMO, 18 (17–20) versus 6 (6–8) cm respectively. This was an expected result, as in V-V ECMO the drainage cannula usually ends in the inferior vena cava, while in V-A ECMO the tip of the drainage cannula is placed in the right atrium. 14 Especially for the multi-stage drainage cannula, a stable fixation is a crucial key-point, as a partial withdrawal of the cannula from the entry site could determinate rapidly entrain air through side holes. In the femoro-femoral V-V ECMO configuration, the distance between the tip of the drainage and the reinfusion cannulae oscillates between 5 and 10 cm. The position of the cannulae within the vena cava is crucial, due to the possibility of blood recirculation, which greatly reduces the oxygenation performance of the V-V ECMO system.14,17 The reinfusion cannulae used in our study were placed in 35 (75%) patients in the right femoral, 5 (25%) in the right internal jugular, and 5 in the femoral artery. Although the cannulae used for the three sites differ in length, the “micro-motion” was substantially similar and close to zero for all sites. It is important to underline how the daily measurement of the extra-vascular part of the cannulae could help inexperienced ICU nurses in increasing the “visual” experience in controlling the ECMO cannulae. To our knowledge, this parameter has not been described in any previous study.
In our results the “cannula micro-motion” was negligible also in patients who underwent prone positioning during ECMO, a rescue (and therapeutic) maneuver for patients who remain hypoxemic despite V-V ECMO support.13,18,19 Recently, a multicentric study led by our research group showed that the application of prone positioning in patients with ARDS on V-V ECMO improves oxygenation and may be associated with a reduction of hospital mortality. 20 However, to ensure a potential benefit of prone positioning during ECMO, the adoption of a meticulous protocol for the management and securement of ECMO cannulae is mandatory.
Finally, it is crucial to underline that ECMO patients exhibit considerable risks of bleeding due to the required systemic anticoagulant therapy. Bleeding may occur from the cannula site, especially when patients’ position is changed. Twenty-six percent of patients experienced at least one episode of bleeding from the ECMO cannula entry site, which required the replacement of the dressing, but relevant bleeding episodes requiring surgical intervention did not occur. This incidence was similar to the one reported by the ELSO register. 7
Study limitations
Our study has however several limitations. First, it was retrospective in its design, therefore our findings must be confirmed by prospective studies. Second, the study population was small. Third, we did not investigate the use of medical-grade skin glue (cyanoacrylate), which may play a role in this setting. 21 We did not collect data about cannula-related infection. We plan to edit the cannula nursing form to prospectively record any eventual sign of local infection.
Conclusions
Cannula-related complications, as accidental removal, cannula micro-motion and bleeding, are frequently described in patients supported by ECMO. For these patients, daily cannulae and circuit management, can be safely performed by nurses if a written protocol was established. When managed by an experienced critical care nurse, the sutureless device for cannula and tubing securement provides an optimal overall strategy for line stabilization, with the potential to reduce ECMO line-associated complications. The very low incidence of complications observed in our patients confirms the feasibility and safety of our method. Further investigation is warranted to define the most effective methods for ECMO cannulae securement.
Footnotes
Authors’ note
The present study was performed at the General Intensive Care Unit, Emergency Department and Intensive Care, San Gerardo Hospital—ASST Monza, Via Pergolesi 33—Monza, Milan-Bicocca University—Italy.
Author contributions
AL, SE, RR, GF, and MG: conception and design of the study, manuscript writing, and final approval. AL, DP, MaGr, LG, LC, AC, and MG: data collection and analysis. AL and MG: statistical analysis. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.