
Abstract
Background:
Controversy exists regarding surveillance of arteriovenous fistulas for hemodialysis to increase patency. A significant reduction in volume flow rate (VFR) should lead to diagnostic evaluation and eventually intervention. Several methods are available for VFR measurements, but all of them are associated with low reproducibility. VFR trend analysis is suggested as an improved solution. It is therefore a need to find user-friendly, cost and time-effective modalities. We present a novel Doppler ultrasound device (earlybird) which could bridge this gap. It includes an easy-to-use and light-weight single element transducer.
Methods:
In an experimental and clinical setting, we compared earlybird to duplex ultrasound to assess VFR. In a closed circuit of blood-mimicking fluid, 36 paired calculations of calibrated, duplex ultrasound and earlybird VFR was measured. In addition, 23 paired recordings of duplex ultrasound and earlybird VFR was measured in 16 patients with underarm arteriovenous fistulas. Pearson correlation, intraclass correlation coefficient, root-mean-square and Bland-Altman plots were analyzed.
Results:
Strong correlation (r = 0.991, p < 0.001), and excellent level of agreement (ICC = 0.970 (95% CI 0.932 - 0.985), p < 0.001) between earlybird and the calibrated VFR was found in the experimental setup. This was confirmed in the clinical setting, with a strong correlation (r = 0.781, p < 0.001) and moderate to good level of agreement (ICC = 0.750 (95% CI 0.502–0.885), p < 0.001) between earlybird and duplex ultrasound VFR measured at the arteriovenous fistulas outflow veins. In the Bland-Altman plot-analysis for the experimental setup, we found smaller limits of agreement, a smaller consistent and proportional bias, as well as greater accuracy of earlybird than DUS when compared to the calibrated VFR.
Conclusion:
Earlybird is a feasible tool for VFR measurements and could be a future promising device for easy assessment and surveillance of AVF for hemodialysis.
Keywords
Introduction
Controversy exists over the benefit of surveillance of vascular access.1,2 Some guidelines recommend surveillance of arteriovenous fistulas (AVF) for hemodialysis at regular intervals to improve patency.3–6 The European Society for Vascular Surgery (ESVS) recommend that flow measurements should be performed monthly for arteriovenous grafts and every three-month for fistulas. 3 Access flow surveillance is found beneficial for AV fistulas, but studies have not shown the same benefit for grafts.7–9 The clinical benefit and cost effectiveness of AVF surveillance regimens are a subject of debate.1,3,9–12 Updated guidelines from the European Renal Best Practice (ERBP) and The National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) have found that the available evidence is inconclusive to make a recommendation on AVF surveillance and they do not suggest routine surveillance of grafts.1,12
Several volume flow rate (VFR) quantification modalities are available. Indirect VFR measurements during dialysis with dilution techniques, together with monitoring the venous pressure are routinely used.3,4,9 Direct flow measurements with magnetic resonance imaging has the benefit of providing an anatomic overview but is less available and is regarded as costly. 9 Duplex ultrasound (DUS) is a more available tool for VFR measurement. ESVS guidelines promotes surveillance of AVF with DUS at regular intervals to reduce the risk of AVF-thrombosis. 3 Often the brachial artery is preferred for DUS VFR of the AVF,3,13–15 but the radial artery or the AVF outflow vein could also be used. Ultrasound examinations gives at the same time a functional and anatomic view of the vessels of interest. 9
VFR measurements are known to be sensitive to hemodynamic fluctuations in dialysis patients caused by variations in the hydration level, measurements errors and user-dependency. To cope with low reproducibility, it is proposed to frequently assess VFR and use trend analysis to select patients for further diagnostic evaluation.1,3,12 Research in new technology to facilitate and clarify the role of monitoring and surveillance of vascular access are needed.1,12
Earlybird is a novel ultrasound Doppler monitoring device. A recent published study has shown that the device can detect alterations in blood flow velocities with comparable accuracy as laser Doppler flowmetry and pulsed wave Doppler. 16 Earlybird has the potential to be manufactured as a lightweight, low-cost, and easy-to-use device for blood flow monitoring. The aim of this project was to evaluate whether earlybird could be used to monitor VFR in AVF for hemodialysis and to be a potential future tool for surveillance of vascular access. The feasibility of earlybird for VFR measurements both in an experimental setup and in patients with AVF is investigated.
Material and Methods
Earlybird
Earlybird is an ultrasound Doppler monitoring device, which consists of a single element transducer (Per Kristian Bolstad, University of Southeast Norway), 17 acquisition hardware, and a user interface. The transducer was fixed in a case, that ensured a 63.3° insonation angle to the surface, Figure 1. The nominal frequency is 7.8 MHz, transmitted at a pulse repetition rate of 8 kHz. In-house software, developed in MATLAB (MathWorks® R2018a), recorded multi-gated Doppler signals for later post processing of power-Doppler M-mode and spectrogram. For VFR measurement the earlybird-probe was placed above the simulated vessel of interest or at the proximal part of the AVF outflow vein. The probe was positioned, guided by real-time Doppler spectrogram, to obtain laminar flow.
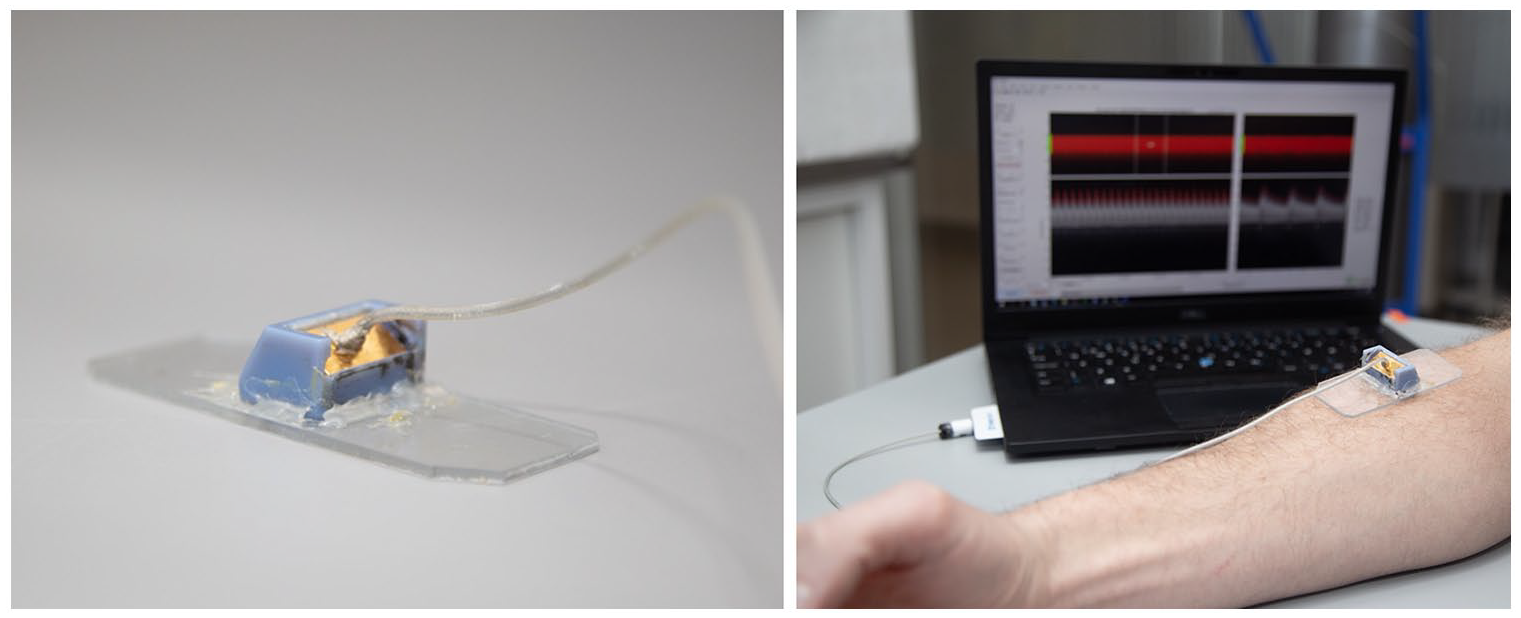
Prototype of earlybird probe attached to a fastening stand. In the background, interface illustrating Doppler flow velocity curves (photo: Karl Jørgen Marthinsen/NTNU).
Duplex ultrasound
For DUS VFR measurements in the experimental setup we used GE Vivid E95 (General Electric (GE) Vingmed Ultrasound, Horten, Norway), equipped with 9L and 11L linear transducers, while for the clinical setup we used GE Logic S8 ultrasound system (GE Healthcare, Milwaukee, Wisconsin, USA), equipped with a ML6-15 transducer. DUS measurements were performed by an experienced ultrasound examiner. The lumen or vessel of interest was precisely visualized. Several repeated measurements were performed. Flow velocity was measured in angle corrected pulse wave Doppler-mode at an insonation angle below 60°. Sample-volume was set between 70% and 99% of the vessel lumen. Inner diameter was measured perpendicular to the vessel wall. VFR was automatically calculated by the ultrasound machine software, based on the intensity-weighted mean frequency (TAMEAN), and diameter.
Experimental setup
The experimental validation setup consisted of a peripheral flow phantom (Model 524, Peripheral Vascular Doppler flow Phantom, ATS Laboratories, Norfolk, USA), a reservoir and a dual head rotator pump (Multiflow Rollerpump, Stöckert Instrumente, Münich, Germany) connected in a closed circuit, Figure 2. The circuit was filled with a blood mimicking fluid, consisting of a solution of distilled water and corn starch. The peripheral flow phantom is made of a tissue-mimicking material of urethane rubber, and consists of several lumens simulating vessels, ranging from 4 to 8 mm in diameter, at 15 mm depth from the surface. The speed of sound in urethane rubber is 1450 m/s + 1.0% at 23°. We assume that the simulated vessel lies parallel to the surface and that flow is laminar and radially symmetric. By adjusting the speed of the rotator pump, different pulsatile VFR (calibrated VFR) could be moved through the phantom. The calibrated VFR was estimated by measuring the variation of the reservoir-weight using a scale and controlled for each separate measurement. We assumed the density of water to be 1 kg/dm3. For each calibrated VFR a paired recording was made with earlybird and DUS VFR, with respectively the 9L and 11L ultrasound transducer.
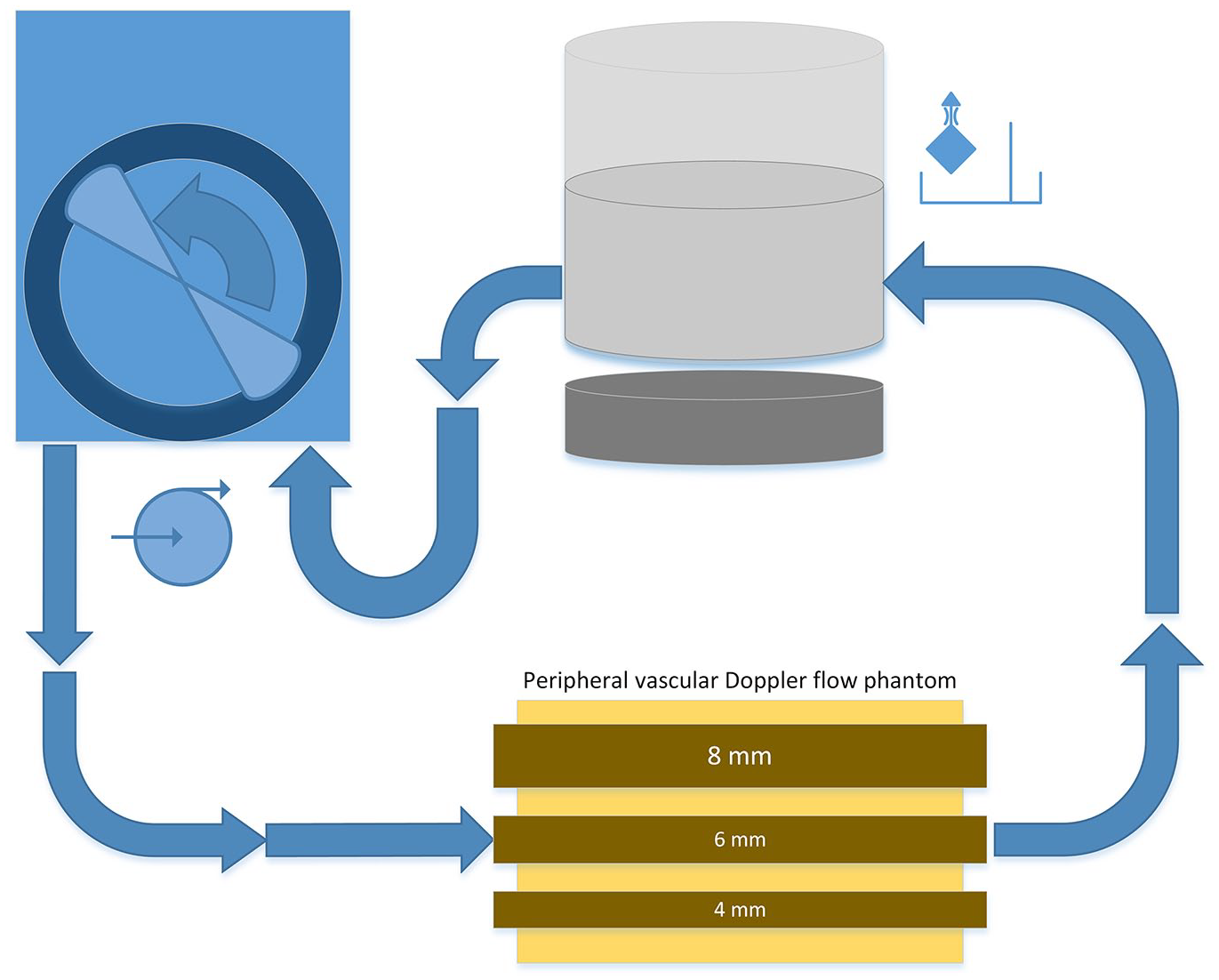
Experimental setup: closed loop-circuit for blood-mimicking-fluid including vented reservoir on top of a magnetic stirrer, dual-headed rotator pump and vascular phantom with three different lumen diameters of 8, 6, and 4 mm.
Clinical setup
In total 16 patients, established with a distal radio-cephalic forearm AVF for hemodialysis access, were recruited from one dialysis unit. The median age was 66 years (range 44–87). The patients were non-fasting, and all measurements were done before cannulation of the fistula vein and connection to the hemodialysis unit.
The patients underwent a DUS-scanning of bilateral brachial arteries, the ipsilateral radial artery, and the outflow vein of the AVF. DUS VFR were calculated from all anatomic sites. The DUS VFR for the brachial artery was calculated by subtracting the contralateral against the ipsilateral achieved measurements as described in guidelines. 3 Repeated measurements were made for each vessel. At the discretion of the examiner, based on consistency of the recording, undisturbed signal acquisition and laminar flow, the recording with the most consistent measurement was chosen to be used for further analysis. We recorded flow velocities with earlybird at the AVF outflow vein as earlier described.
Earlybird volume flow rate calculation
For earlybird VFR calculations we assumed fully developed laminar parabolic flow. Calculations were made post procedural. VFR (Q) for parabolic flow, where TAV is time-averaged maximum velocity and r the radius, is given by equation (1):

Maximum velocity over the vessel cross-section was automatically calculated from the Doppler spectrogram, and corrected for differences in speed of sound between the rubber-phantom and tissue. An algorithm to automatic calculate vessel diameter (EB D) based on power Doppler M-mode data was developed, compensating for sample volume size and insonation angle. No visual confirmation of the course of the vessel are made with earlybird. We assumed that the vessel of interest lies parallel to the skin. In a clinical setting the vessel may deviate, this will lead to an imprecise estimation of diameter. Angle corrected TAV was based on an insonation angle of 63.3°. VFR expressed as equation (2).

Statistics
Normality was assessed. For the absolute VFR-data, the relative difference between each method and the calibrated reference for experimental data, as well as the relative difference between each method and the mean of the methods for the clinical data, parametric tests were used since the relative differences were approximately normally distributed. Pearson correlation analysis are presented. Intra-rater variability and reliability analysis for agreement between methods were done using intraclass correlation coefficient (ICC) with its 95% confidence intervals, using single measurements for absolute agreement in a two-way mixed model,18,19 and level of agreement reported according to Koo and Li. 20
Bland-Altman plots, 95% limits of agreement, and root-mean-square (RMS) were calculated based on the relative difference of DUS and earlybird from the calibrated VFR for the experimental data and based on the relative difference from the mean of DUS and earlybird VFR at the AV outflow vein for the clinical setup.21,22 Consistent bias expressed as the mean relative difference was assessed using One-Sample t-test. Linear regression was used to assess proportional bias. All statistical analyses were done in in SPSS (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY).
Ethics
The study was approved by the regional ethical committee (REC central Norway, 044/2017) and by the Norwegian Government of Health, June 12th, 2017. All participants provided written informed consent.
Results
Experimental setup
In an experimental setup 36 paired calculations for calibrated, earlybird and DUS VFR were recorded. Of the ultrasound examinations, 18 were taken using the 11L transducer and 18 using the 9L transducer (supplementary material; table 1).
The calibrated VFR correlated against DUS VFR (r = 0.984, p < 0.001) as well as for earlybird VFR (r = 0.991, p < 0.001), Figure 3. No relative difference between DUS and calibrated VFR was seen between the two types of transducers (1.51% (SE 8.22), p = 0.855). For further analysis of DUS VFR, the data of two transducers were combined. The level of agreement between methods for DUS and calibrated VFR is poor to excellent, due to a wide 95 % confident interval, ICC of 0.949 (95% CI, 0.449–0.986), p < 0.001. While for earlybird and calibrated VFR an excellent level of agreement was found with an ICC of 0.970 (95% CI, 0.932–0.985), p < 0.001.
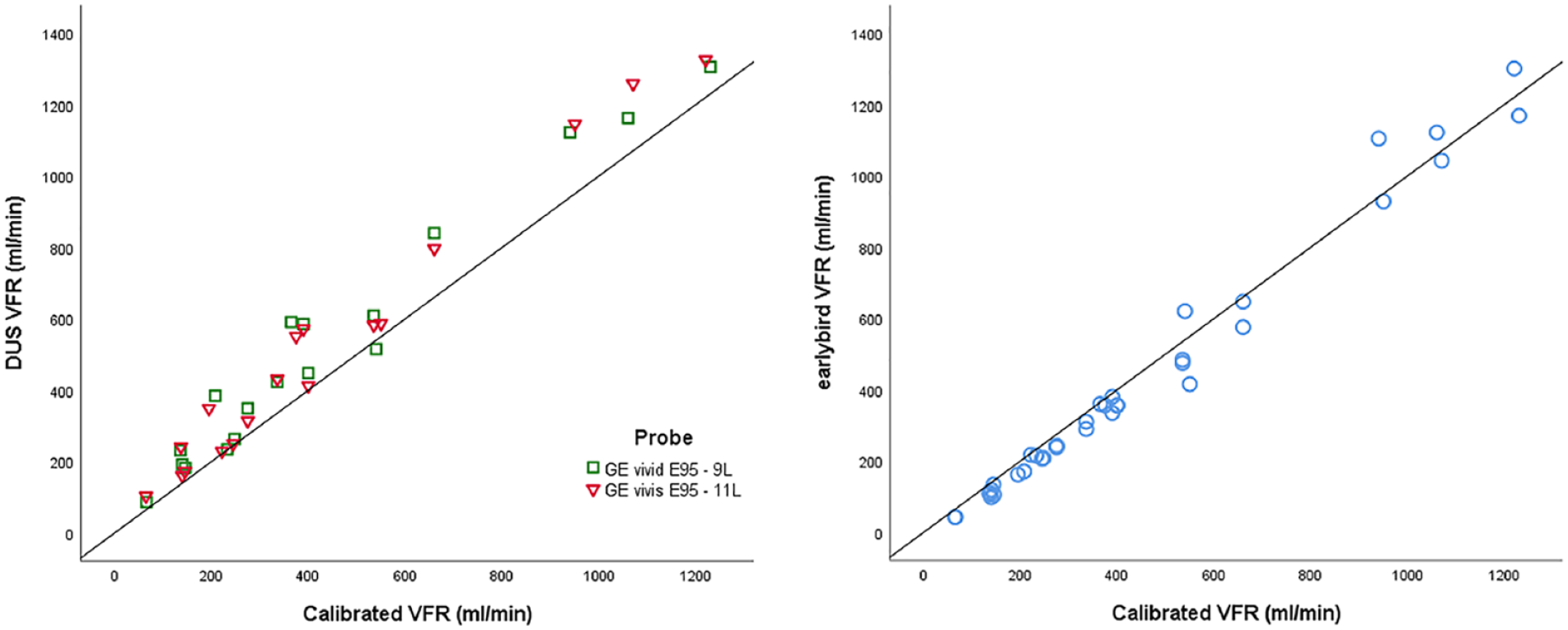
Scatterplot of correlation between calibrated volume flow rate (VFR) and duplex ultrasound (DUS) and earlybird VFR respectively. VFR is reported in ml/min. The 9L and 11L transducers are marked separately. Correlation analysis for DUS includes both transducers. Pearson Correlation for DUS VFR, r = 0.984, p < 0.001, and for earlybird VFR, r = 0.991, p < 0.001.
The relative difference of the calibrated VFR to DUS and earlybird VFR were calculated and plotted in a Bland-Altman-like plot with 95% limits of agreement, Figure 4. There is a consistent bias of the relative difference of DUS from the calibrated VFR of 27.2% (SE 4.06), p < 0.001, 95% limits of agreement −20.5 and 74.9%, and for earlybird VFR of −10.5% (SE 1.96), p < 0.001, 95% limits of agreement −33.5 and 12.6%. There is a proportional bias for both DUS VFR (B = −0.029, SE 0.012, p = 0.017) and earlybird VFR (B = 0.023, SE 0.005, p < 0.001), indicating that the relative difference changes with −0.029 and 0.023, respectively, for one unit in increase of calibrated VFR. Accuracy analysis between calibrated and DUS VFR gives an RMS-error of 36.3%, and for calibrated and earlybird VFR of 15.6%.
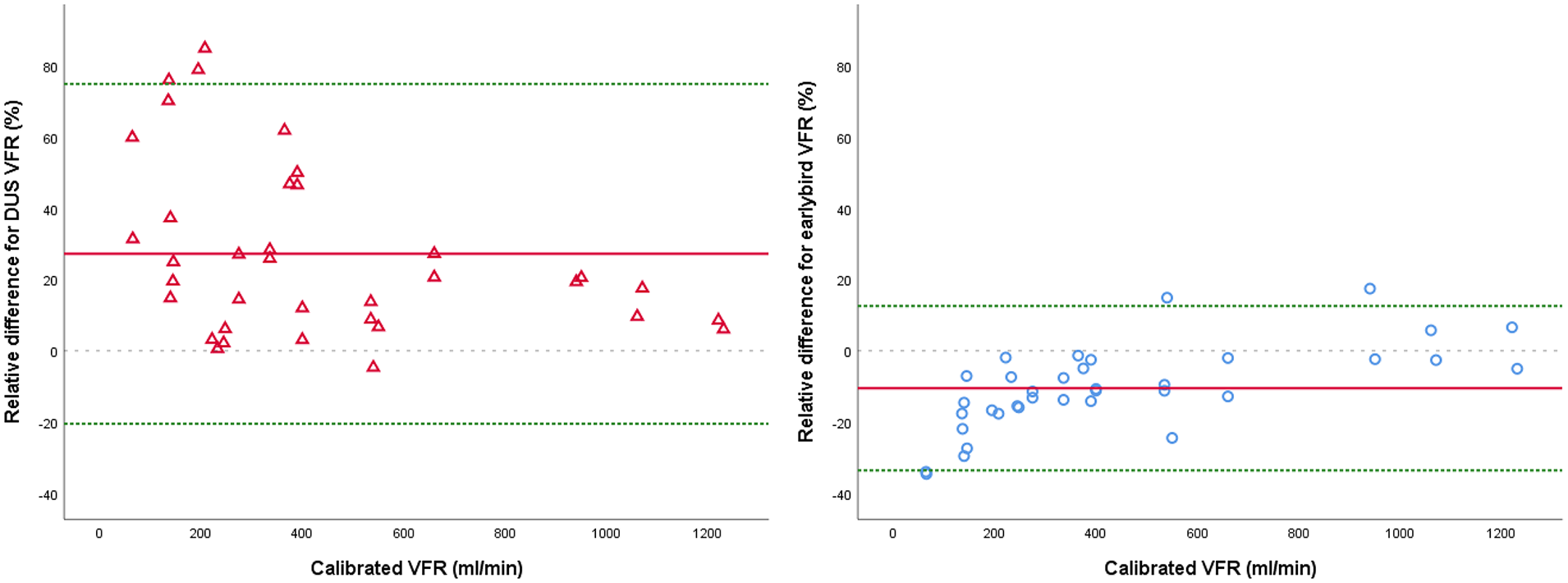
Bland-Altman plots of the relative difference (%) of duplex ultrasound (DUS) or earlybird, and the calibrated volume flow rate (VFR) ((VFR—calibrated VFR)/calibrated VFR). Mean relative difference (red solid line) and 95% limits of agreement (dotted green line) are given.
DUS and earlybird intra-rater reliability was analyzed for experimental data by setting the DUS measurements with the two different transducers, done on the same calibrated VFR, as two separate examinations. An excellent intra-rater reliability was found for both DUS (0.995 (0.986, 0.998), p < 0.001) and earlybird (0.977 (0.940, 0.991), p < 0.001).
Clinical experiment
In total 16 patients were recruited to undergo evaluation of VFR of their underarm AV-fistula. Of these, three patients were examined twice and two patients three times at a three-month interval. Each paired measurement is regarded as one sample, making a total of 23 paired recordings of DUS and earlybird (Supplemental material; table 2). It was not possible to obtain DUS measurements of the contralateral brachial artery for one patient.
There is a strong correlation between DUS and earlybird VFR of the AVF outflow vein (r = 0.781, p < 0.001). DUS VFR of the radial artery moderately correlated with DUS and earlybird VFR for AVF outflow vein (r = 0.506, p = 0.014 and r = 0.578, p = 0.004, respectively). DUS VFR of the subtracted brachial artery did not correlate to the DUS VFR of the radial artery or the AVF outflow vein, as well as earlybird VFR for AVF outflow vein (p = 0.101, p = 0.400, p = 0.421), Figure 5. The level of agreement for DUS and earlybird VFR of the AVF outflow vein is moderate to good, with an ICC of 0.750 (95% CI 0.502, 0.885), p < 0.001.
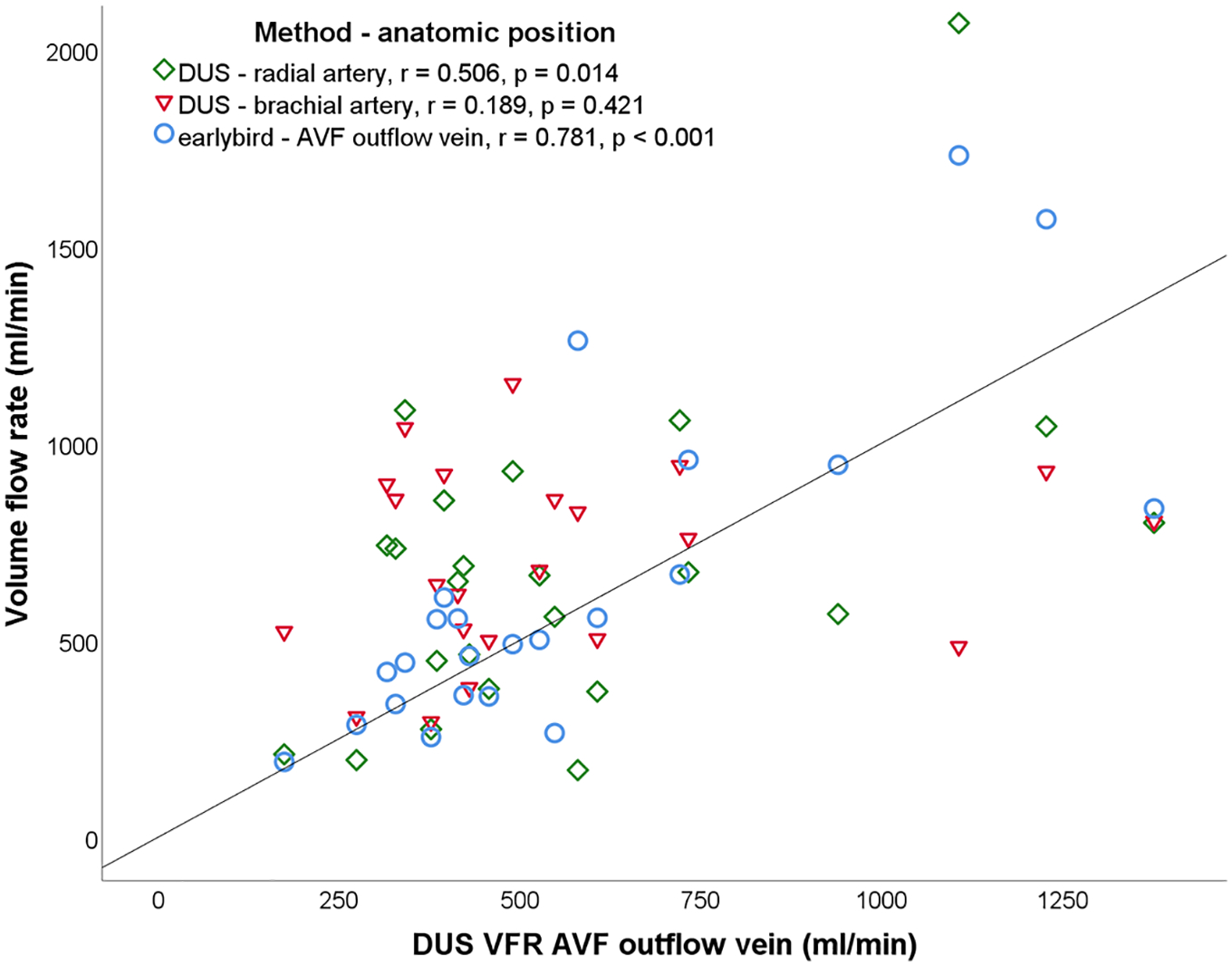
Scatterplot of DUS VFR of the AVF outflow vein against the DUS VFR of the radial artery (a. radialis), subtracted brachial artery (a. brachialis) and earlybird VFR positioned at the AVF outflow vein. Pearson correlation (r) is reported for DUS VFR of the AVF outflow vein and VFR for each method respectively. The identity line is given.
In the clinical setup, we compared two methods of estimating VFR based on the Doppler-technique, both methods are suspected to divert from the “true” VFR. Therefore, mean VFR of the two methods were calculated and used for further analysis, presented in a Bland-Altman plot in Figure 6. There is no significant relative difference from the mean VFR of the two methods, 2.9% (SE 3.39), p = 0.399, indicating no consistent bias. No proportional bias was found (B = 0.012 (SE = 0.010), p = 0.245). The 95% limits of agreement are −29.0 and 34.8%. RMS-deviation for the relative difference from the mean of DUS and earlybird VFR is 16.2%.
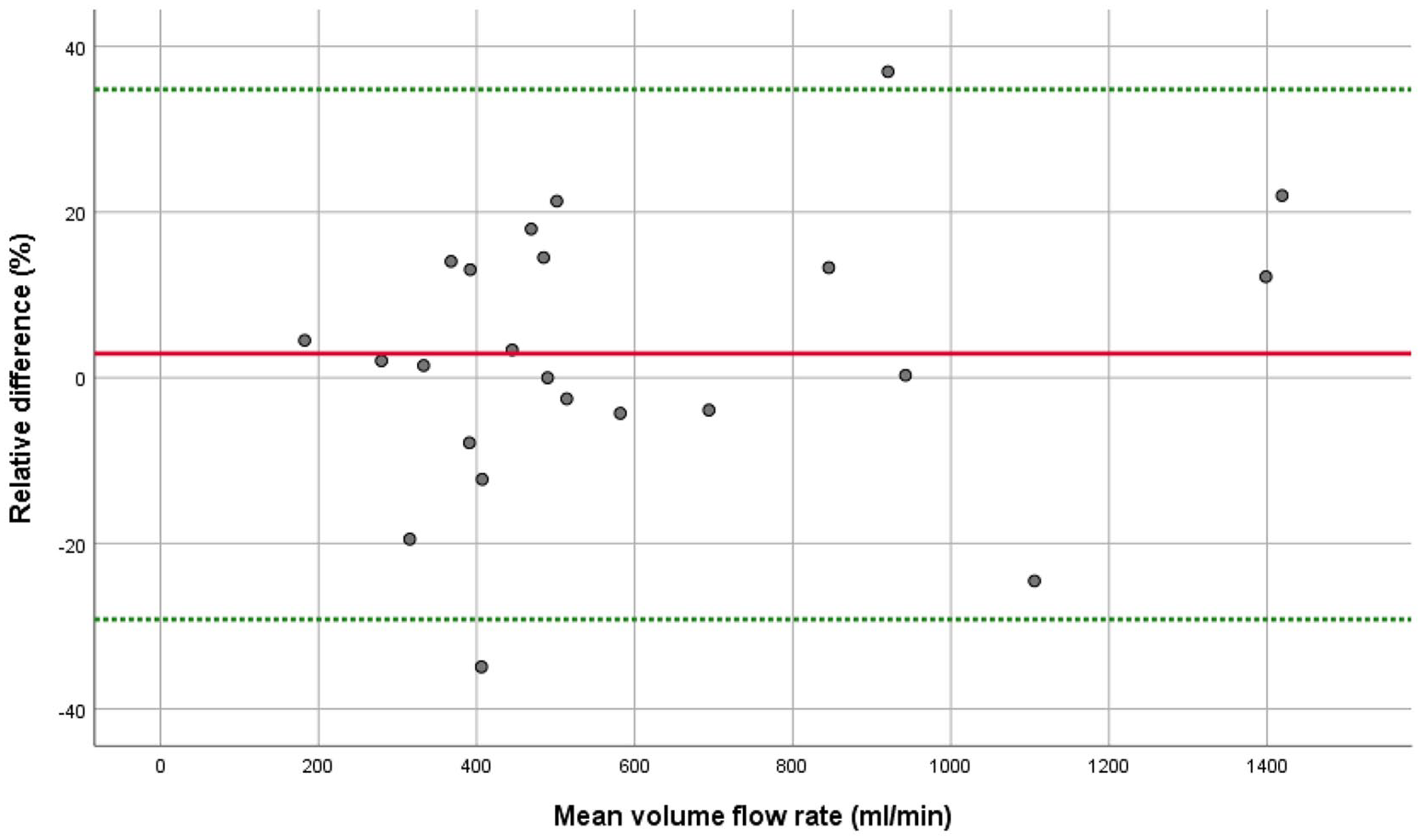
Bland-Altman plot of the relative difference (%) of DUS and earlybird VFR from the mean VFR ((earlybird VFR—mean VFR)/mean VFR), measured at AVF outflow vein. Mean relative difference (red solid line) and 95% limits of agreement (dotted green line) are given.
Discussion
We tested a novel ultrasound Doppler device (earlybird) against ultrasound to determine VFR. In an experimental setting, both earlybird and DUS estimates the calibrated VFR well. We found greater accuracy and less bias for VFR estimated with earlybird than for DUS. Repeated measurements with earlybird were consistent. The findings were confirmed in a clinical setting, where we compared earlybird and DUS VFR at the AVF outflow vein.
Both in the experimental and clinical setup, DUS and earlybird VFR deviates from the calibrated and mean VFR. The “true” VFR in a clinical setting is not known. In a simulator-model analyzing accuracy of DUS VFR measurements of AVF outflow vein, the measured VFR deviated 35 ± 36%. 23 An error of DUS VFR measurements of approximate 30% are reported in clinical settings.3,24 In AVF surveillance programs, a reduction in VFR less than 33% should not be regarded as significant. 3 Trend analysis has been proposed to overcome these well-known obstacles. 3
Indirect VFR measurements by dilution techniques or DUS have been the method-of-choice to evaluate dialysis access functioning. There is good agreement between the methods.25–27 These methods need specialized trained personnel, often require flow reversal during dialysis and can be time consuming. 9 Because of high technical failure-rate and high-cost of dilution techniques, DUS is the recommended method. 25 In the early development of ultrasound, noninvasive blood flow measurements of AVF and grafts for hemodialysis were explored. Rittgers et al. 28 used a 5 MHz flat-head probe with a fixed angle of 60° to the surface to evaluate access grafts with a known diameter. The method was found to be useful, safe and repeatable. Bouthier et al. 29 described a series of 32 patients where AV-fistula blood flow was non-invasive evaluated using a double transducer probe, which made it possible to correct for angle and calculate diameter. Easy-to-use and low-cost devices could allow patients and non-specialized healthcare workers to perform VFR trend surveillance of AV-fistulas daily or at every dialysis visit. This would allow for frequent VFR-data collection, and could be combined with that is, weight and blood pressure, further research is needed to evaluate whether this could change the surveillance practice.
Measurements of flow velocities by the Doppler method is user dependent, needs accurate angle correction and is highly dependent of the insonation angle.30–32 The error of the selected angle should be less than two degrees to achieve a measurement error of 10%. For calculation of earlybird VFR we have assumed that the vessel lies parallel to the surface. In the clinical setup it is not given that the AVF outflow vein is accurately parallel, especially when the vessels enter the antecubital fossa where it lies in more subcutaneous fat and deflects downwards. We have not corrected for this, and this can result in inaccurate earlybird VFR, due to imprecise calculation of both Doppler velocity and diameter. The AVF outflow vein may have considerably tortuosity, diameter alterations and be close to the anastomotic area, which all contribute to less developed parabolic flow. 33 This lowers the accuracy of VFR calculations. These concerns are great limitations of earlybird.
Different anatomic sites for DUS examination of AVF-functioning are described. DUS measurements of VFR at the brachial and radial artery, as well as AVF outflow vein are commonly used.8,13,34,35 Existing guidelines have not described the optimal anatomic site,3,4,36 although the brachial artery is often preferred.14,15,35 Its anatomic position and easy access facilitate an insonation angle < 60°, as well as it more often presents with laminar and radial symmetric flow. Other studies have found a strong correlation between VFR at the AVF outflow vein and the brachial artery. 35 In our small clinical sample, we did not find the same correlation. This may be due to anatomic variations, that is, side-branches to the fistula which divert blood flow away from the vessel used to measure VFR, and difference in flow through the ulnar artery and palmar-arcade. Of the included paired clinical measurements, one sample deviates from the expected values with a relative low VFR (484 ml/min) in the brachial artery and a fourfold VFR (2067 ml/min) of the radial artery (No. 21; Supplemental material). This may be due to erroneous measurements or under- or over-estimating VFR in the brachial or radial artery, respectively. We chose not to exclude this sample, since this may represent real-life challenges in VFR estimation. In our study, AVF outflow vein was chosen for earlybird VFR measurements because of its easy access and visibility.
The Bland-Altman plots reveal an increasing relative difference in the DUS VFR-measurements for low calibrated VFR in an experimental setting. This may be due to the wall-filter which remove low-velocity signals and increase the calculated DUS VFR, especially at low velocities. Spectral broadening due to transit time, can cause overestimated velocity. The effect will be less in a unfocused single element probe than in a linear probe, mainly due to wider beamwidth. 37 For earlybird the overestimation is less than 5%. To minimize user-dependent error of earlybird measurements, an automatic algorithm-based calculation of diameter and velocity were performed. The algorithm is based on known instrument settings and transducer geometry and is not built on or adapted by the results of this study. Errors in diameter assumptions will greatly influence VFR-calculations. The experimental VFR-measurements confirms an adequate algorithm for calculation of diameter and velocity.
Intra or inter-observatory changes are well-known sources for errors in the DUS measurement 31 and was already described when Gill 38 for the first time described VFR as a possible technique for blood flow evaluation. In the experimental part of this study, we found an excellent intra-observer reliability. We did not perform an inter-rater analysis. Exploration of these sources of error are outside the scope of this proof-of-concept study, but to further assess intra- and inter-observatory reliability would be interesting to validate earlybird as a device for AVF surveillance.
Conclusion
Our study indicates that earlybird is a feasible tool for VFR measurements. Technical development may increase user-friendliness and its clinical applicability and earlybird may be a future promising device for easy assessment and surveillance of hemodialytic vascular access.
Supplemental Material
sj-docx-1-JVA-10.1177_11297298211060960 – Supplemental material for Validation of a novel ultrasound Doppler monitoring device (earlybird) for measurements of volume flow rate in arteriovenous fistulas for hemodialysis
Supplemental material, sj-docx-1-JVA-10.1177_11297298211060960 for Validation of a novel ultrasound Doppler monitoring device (earlybird) for measurements of volume flow rate in arteriovenous fistulas for hemodialysis by Erik Mulder Pettersen, Jørgen Avdal, Stefano Fiorentini, Øyvind Salvesen, Jonny Hisdal, Hans Torp and Arne Seternes in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors would like to thank the dialysis unit at Sørlandet Hospital Kristiansand, especially the efforts of Anne Margrethe Myhrmoen and Marianne Klausen, for their facilitation of this study.
Author contributions
Conception and design: EMP, SF, HT, AS. Data collection: EMP. Analysis and interpretation: EMP, JA, ØS, HT, AS. Statistical analysis: EMP, JA, ØS. Writing the article: EMP. Final approval and critical revision of the article: EMP, JA, SF, ØS, JH, HT, AS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article, except Hans Torp who is the inventor of earlybird and shareholder of CIMON Medical AS. CIMON Medical AS was not involved in the study design; collection, analysis, or interpretation of data; manuscript writing; or the decision to submit the manuscript for publication.
Ethical approval
The study was approved by the regional ethical committee (REC central Norway, 044/2017) and by the Norwegian Government of Health, June 12th, 2017. All participants provided written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Erik Mulder Pettersen has received funding from The Central Norway Regional Health Authority, allocated via The Liaison Committee for Education, Research and Innovation in Central Norway (Samarbeidsorganet).
Guarantor
Section of Vascular Surgery, Department of Surgery, Trondheim University Hospital, St. Olavs Hospital, PB 3250 Torgarden, 7006 Trondheim, Norway
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.