
Abstract
Purpose:
To compare all-cause mortality and primary patency with drug-coated balloon angioplasty (DCBA) compared with plain balloon angioplasty (PBA) in people with hemodialysis-related stenosis.
Materials and methods:
PubMed, Embase, and Cochrane Library databases were searched from November 1966 to February 2021 to identify randomized controlled trials (RCTs) that assessed the use of DCBA versus PBA for stenosis in hemodialysis circuits. Data extracted from the articles were integrated to determine all-cause mortality, target lesion primary patency (TLPP), circuit access primary patency (CAPP), 30-day adverse events, and technical success for the two approaches. We performed meta-analysis on these results using a fixed-effects model to evaluate odds ratios (ORs) and 95% confidence intervals (CIs) where I2 < 50% in a test for heterogeneity, or a random-effect model if otherwise. Sensitivity and subgroup analyses were also performed.
Results:
Sixteen RCTs of 1672 individuals were included in our meta-analysis, of which 839 individuals received DCBA and 833 received PBA. The pooled outcome showed no statistical difference between DCBA and PBA in all-cause mortality at 6 months (OR = 1.29, 95% CI = 0.72–2.32, p = 0.39, I2 = 4%), 12 months (OR = 1.02, 95% CI = 0.68–1.53, p = 0.91, I2 = 0%), and 24 months (OR = 1.50, 95% CI = 0.87–2.57, p = 0.15, I2 = 0%), 30-day adverse events (OR = 1.09, 95% CI = 0.30–3.98, p = 0.90, I2 = 66%), and technical success (OR = 0.18, 95% CI = 0.02–1.92, p = 0.16, I2 = 65%). The DCBA had significantly better outcomes versus PBA in TLPP at 6 months (OR = 2.37, 95% CI = 1.84–3.04, p < 0.001, I2 = 44%) and 12 months (OR = 1.77, 95% CI = 1.22–2.56, p = 0.002, I2 = 56%), and CAPP at 6 months (OR = 2.07, 95% CI = 1.21–3.54, p = 0.008, I2 = 67%) and 12 months (OR = 1.66, 95% CI = 1.29–2.15, p < 0.001, I2 = 0%).
Conclusion:
In hemodialysis circuit stenosis, DCBA appears to have similar safety but greater efficacy than PBA.
Introduction
Hemodialysis (HD) is the most well-adopted method of renal replacement therapy globally since the 1960s.1,2 Longevity on dialysis is directly proportional to dialysis quality, and that quality in turn depends on the reliability and integrity of access to the individual’s vascular system. The ideal HD access provides reliable, complication-free access for the delivery of prescribed dialysis and is suited to the individual’s needs. However, it is not possible to avoid stenosis with either arteriovenous fistular (AVF), as recommended by the National Kidney Foundation Kidney Disease Outcomes Quality Initiative guidelines, 3 or arteriovenous graft (AVG) and central venous catheter (CVS). Stenosis is the most common complication of HD, which seriously affects the quality of HD and can be life-threatening, owing to neointimal hyperplasia.4–6
Balloon angioplasty is typically used for the primary treatment of clinically and angiographically significant AVF and AVG stenotic lesions. 3 Unfortunately, the percentage of older individuals who undergo repeat intervention within 6 months is relatively high, at approximately 50%.7–11 Drug-coated balloon angioplasty (DCBA), such as paclitaxel-coated balloon angioplasty, is already widely used in the therapy of peripheral arterial disease (PAD), and has been shown to improve the restenosis rate and freedom of reintervention.12,13 DCBA may decrease the risk of de novo stenosis or restenosis by inhibiting neointimal hyperplasia and decreasing inflammatory responses in the vessel wall.
However, previous studies on the application of DCBA in HD access are controversial compared with plain balloon angioplasty (PBA): some studies show that the DCBA is superior compared with PBA in de novo stenosis or restenosis with AVF, AVG, and CVS,14–17 while some studies do not. 18 One meta-analysis showed that the application of DCBA increases all-cause mortality compared with PBA among people with PAD. 19 This study therefore aimed to investigate long-term mortality and patency with DCBA versus PBA for individuals with HD circuit de novo stenosis or restenosis.
Materials and methods
Literature search and inclusion/exclusion criteria
Based on the standards outlined in the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement, we searched PubMed, Embase, and Cochrane Library databases for randomized controlled trials (RCTs) that evaluated DCBA versus PBA in de novo stenosis or restenosis with AVF/AVG/CVS from November 1966 to February 2021. The last literature search was updated on February 3, 2021. The following search terms were used in combinations with AND/OR: “fistula,” “arteriovenous fistula,” “arteriovenous fistulae,” “arteriovenous fistulas,” “arteriovenous access,” “AV fistulas,” “hemodialysis fistulas,” “dialysis fistulas,” “hemodialysis access,” “dialysis access,” “dialysis fistulae,” “dialysis fistula,” “drug-coated balloon,” “drug-eluting,” “drug-coated,” “plain balloon angioplasty,” “paclitaxel-coated,” “paclitaxel-eluting,” “conventional balloon,” “angioplasty,” “standard balloon,” “de novo stenosis,” “restenosis.”
Study Selection
Two authors independently assessed the eligibility of all retrieved articles, with a third author resolving any conflicts. Conflicts were settled by agreement among the authors. References from the retrieved articles were also searched. Eligibility for inclusion in our meta-analysis was based on the following criteria: (1) RCTs; (2) focused on DCBA application in de novo or recurrent AVF/AVG/CVS stenosis with PBA as the control; (3) contained data on all-cause mortality, target lesion primary patency (TLPP), circuit access primary patency (CAPP), technical/anatomic success, and 30-day adverse events for both DCBA and PBA; and (4) included a clinical follow-up of at least 6 months.
Data extraction and quality assessment
The following data were extracted from the enrolled studies: first author, year of publication, 6, 12, and 24-month all-cause mortality, 6, 12, 18, and 24-month TLPP, 6, 12, 18, and 24-month CAPP, 30-day adverse events, and technical/anatomic success. The Cochrane Risk of Bias tool was used to evaluate the quality of RCTs, and contained seven main sections: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. Heterogeneity was evaluated using the I2 statistic; I2 < 25% was taken to indicate a low risk of heterogeneity, 25%–50% a moderate risk of heterogeneity, and >50% a high risk of heterogeneity. Heterogeneity with an I2 > 50% and p < 0.05 was considered significant across the enrolled studies. Potential publication bias was determined using the Egger test.
Outcome measures and statistical methods
All-cause mortality, TLPP, CAPP, 30-day adverse events, and technical/anatomic success were evaluated to determine the safety and effectiveness of DCBA compared with PBA. TLPP was defined as freedom from clinically-driven target lesion revascularization or access circuit thrombosis during the follow-up period after the index procedure. CAPP was defined as the interval from the index procedure to the next access intervention anywhere in the hemodialysis circuit. Thirty-day adverse events were categorized according to the Society of Interventional Radiology (SIR) criteria for adverse events. 20 Technical/anatomic success was defined as successful completion of the angioplasty procedure with less than 30% residual stenosis on the final angioplasty.
According to the Mantel–Haenszel method, the meta-analysis of these results was conducted using a fixed-effects model to evaluate the odds ratios (ORs) and 95% confidence intervals (Cls) when the risk of heterogeneity was low or moderate; otherwise, a random effects model was used. Subgroup analyses were conducted according to the study design. Sensitivity analyses for all-cause mortality, TLPP, CAPP, 30-day adverse events, and technical success rates were also conducted to estimate the sensitivity of the results by omitting one article at a time. A two-sided p < 0.05 indicated statistical significance. Analyses were performed using Stata software (version 14.0; StataCorp, College Station, TX, USA) and Review Manager (version 5.4.1; Cochrane Information Management System; http://ims.cochrane.org/revman).
Results
Characteristics of included studies
In total, 3748 potentially relevant records were identified, of which 3687 articles were removed by abstract and title screening. The remaining 61 articles were submitted for full-text review. Of these, 17 reports14–18,21–32 (16 RCTs) involving 1672 individuals met the selection criteria (Figure 1). Most studies focused on the target lesion of AVF and AVG, and others also included CVS. More than 81% of studies focused on both de novo and restenosis lesion types, and more than 68% of studies used IN.PCT Admiral (Medtronic) as the type of DCBA invention, with a drug dose of 2–3.5 μg/mm2. The DCBA maintenance time ranged from 45 s to 3 min. More than 62% of studies used pre-dilation with a high-pressure balloon (HBP) before DCBA. Characteristics of all enrolled articles are summarized in Table 1. Among the 16 RCTs included in our study, eight were multicenter studies.14–16,25–28,31
Characteristics of included RCTs.
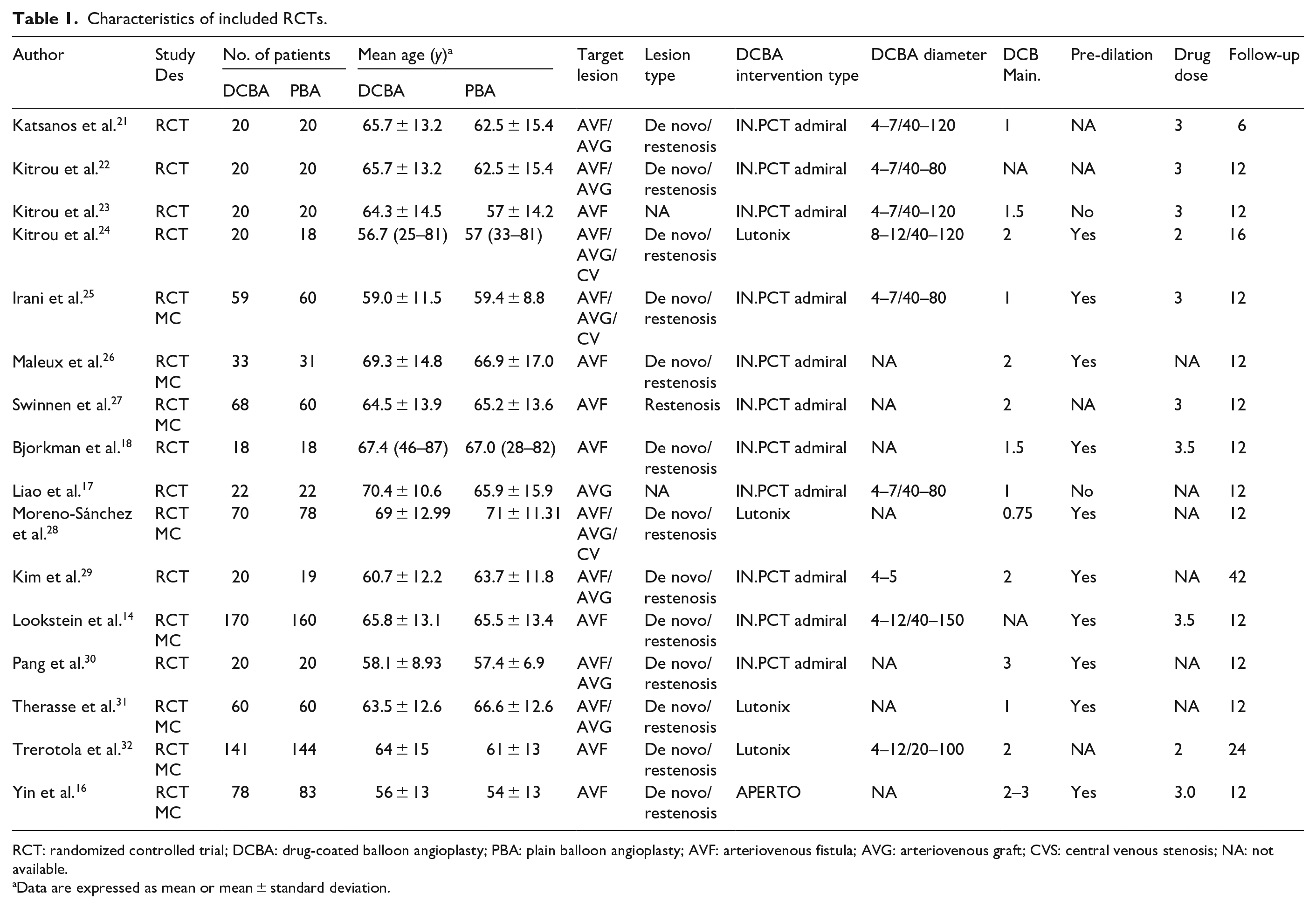
RCT: randomized controlled trial; DCBA: drug-coated balloon angioplasty; PBA: plain balloon angioplasty; AVF: arteriovenous fistula; AVG: arteriovenous graft; CVS: central venous stenosis; NA: not available.
Data are expressed as mean or mean ± standard deviation.
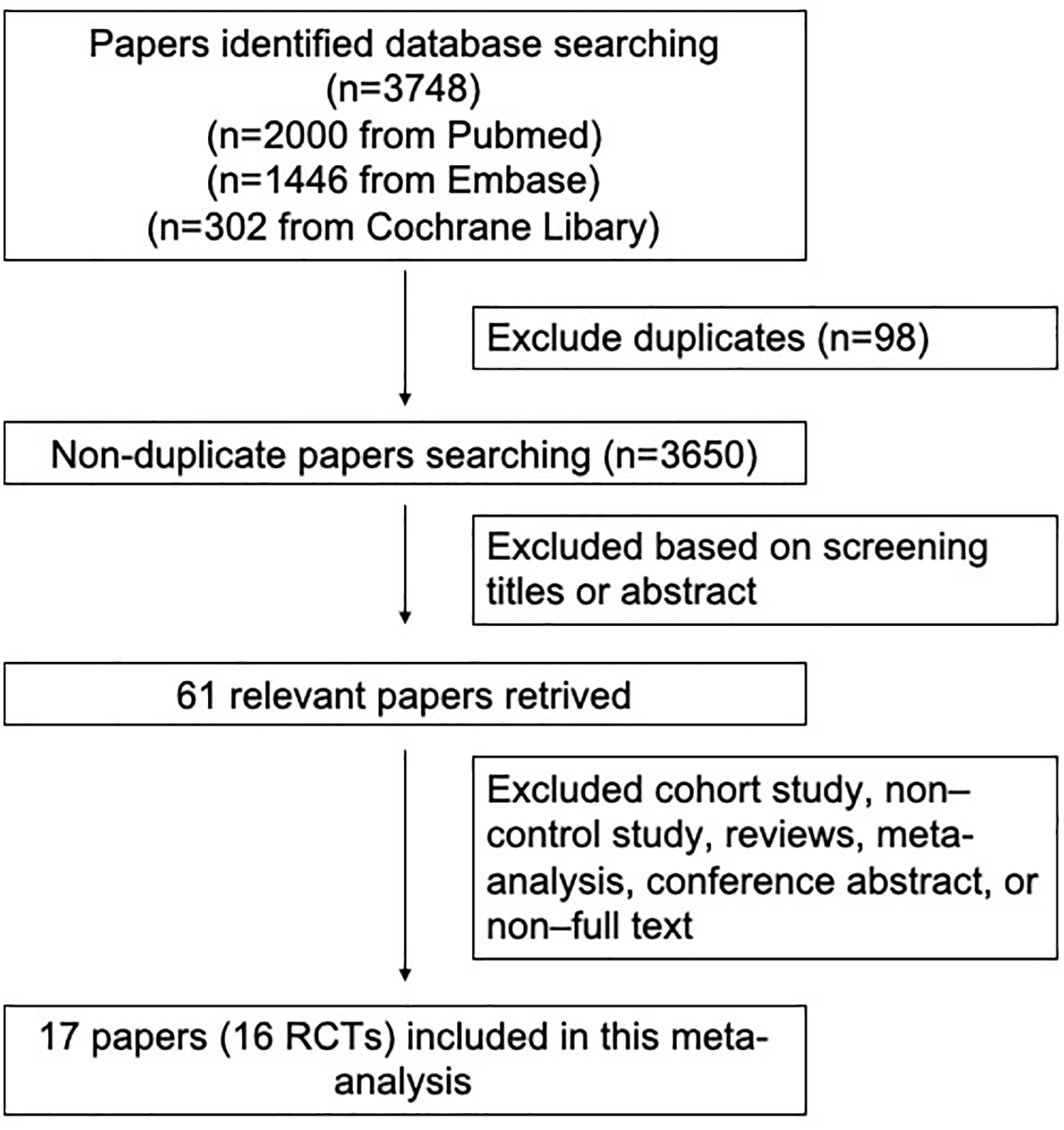
Flowchart of paper screening and selection process.
The Cochrane Risk of Bias Tool showed that most RCTs included in this meta-analysis had insufficient blinding strategies (Supplemental Table 1).
All-cause mortality
Eight studies14–18,25,26,31,32 reported all-cause mortality at 6 months. The pooled 6-month all-cause mortality rate in the DCBA group was 4.48% (26/581) compared with 3.46% (20/578) in the PBA group. There was no significant difference in 6-month all-cause mortality between the two groups (OR = 1.29, 95% CI = 0.72–2.32, Z = 0.86, p = 0.39, Figure 2(a)). The heterogeneity in the pooled results for this variable was low (I2 = 4%). The results of the Egger test showed no significant publication bias (p = 0.103).
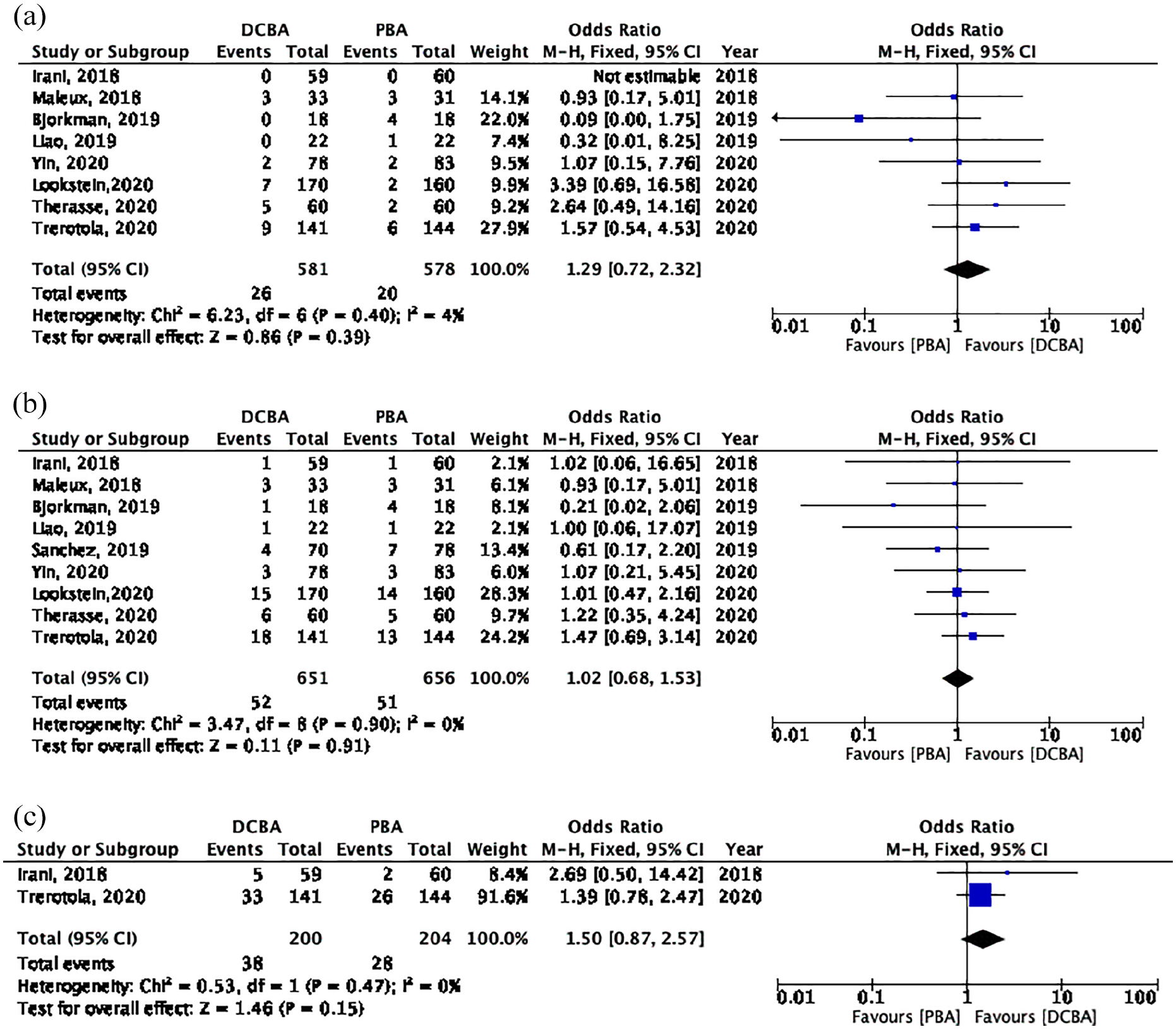
Forest plots of all-cause mortality at (a) 6 months, (b) 12 months, and (c) 24 months between drug-coated balloon angioplasty (DCBA) and plain balloon angioplasty (PBA).
Nine studies14–18,25,26,28,31,32 reported all-cause mortality at 12 months. The pooled 12-month all-cause mortality rate in the DCBA group was 7.9% (52/651), compared with 7.8% (51/656) in the PBA group. There was no significant difference in 12-month all-cause mortality between the two groups (OR = 1.02, 95% CI = 0.68–1.53, p = 0.91, Z = 0.11, Figure 2(b)). The heterogeneity in the pooled results for this variable was low (I2 = 0%). The results of the Egger test showed no publication bias (p = 0.163).
Only two studies25,32 reported all-cause mortality at 24-months. The pooled 24-month all-cause mortality rate in the DCBA group was 19% (38/200) compared with 13.7% (28/204) in the PBA group. There was no significant difference in 24-month all-cause mortality between the two groups (OR = 1.50, 95% CI = 0.87–2.57, p = 0.15, Z = 1.46, Figure 2(c)). The heterogeneity in the pooled results for this variable was low (I2 = 0%).
Target lesion primary patency
Eleven studies reported TLPP at 6 months.14–17,21,23–25,28,30,32,33 The TLPP at 6 months in the DCBA group was 75.2% (468/622), compared with 57.8% (365/632) in the PBA group. The pooled results showed a significant statistical difference between the two groups, with a moderate risk of heterogeneity (OR: 2.37, 95% CI: 1.84–3.04, p < 0.00001, Z = 6.73, I2 = 44%, Figure 3(a)). A significant publication bias was observed in the Egger test (p = 0.049). However, the p value of the Egger test was 0.250 if one study 32 was omitted.
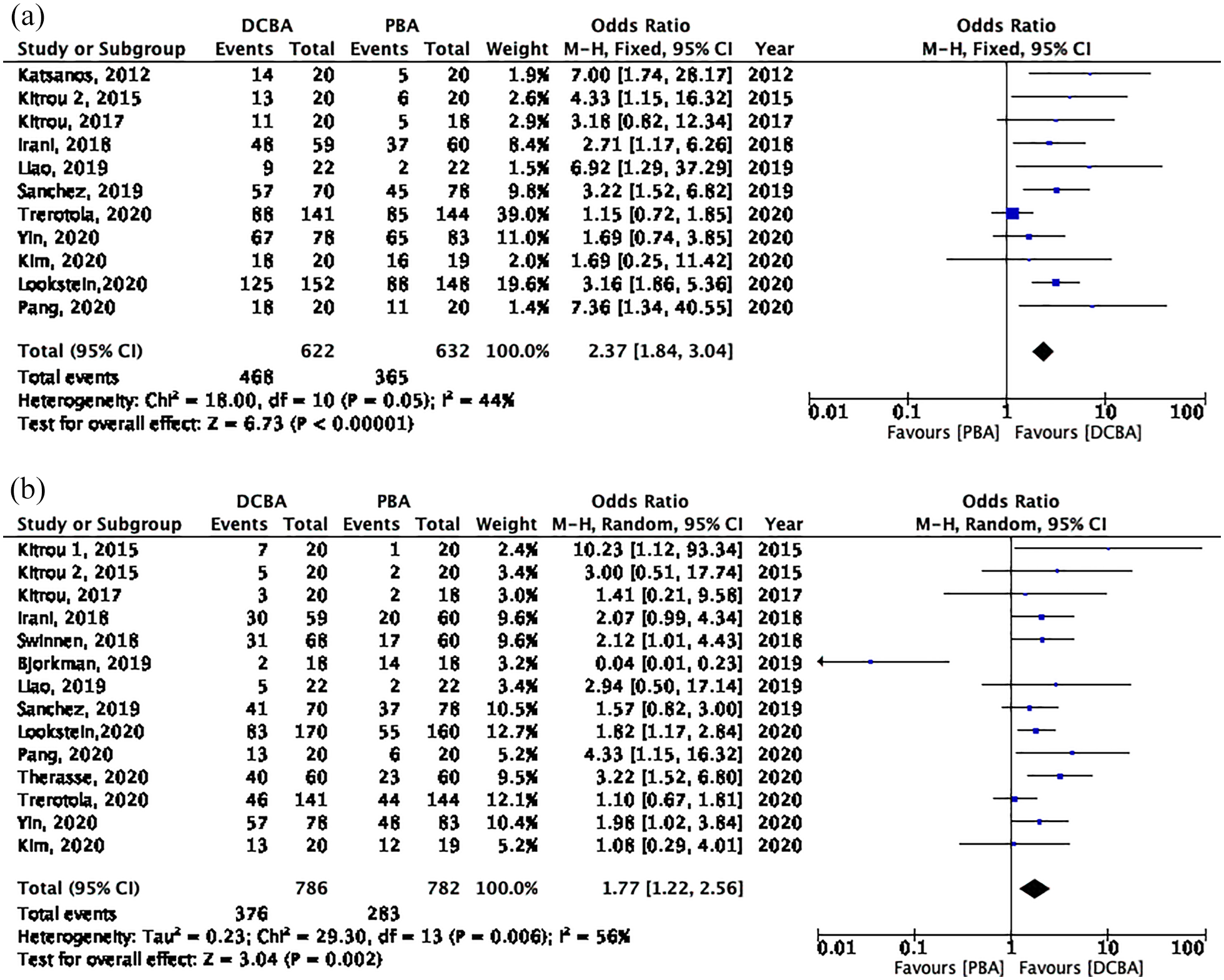
Forest plots of target lesion primary patency (TLPP) at (a) 6 months and (b) 12 months between drug-coated balloon angioplasty (DCBA) and plain balloon angioplasty (PBA).
Fourteen studies reported TLPP at 12 months.14–18,22–25,27–31 The pooled TLPP at 12 months in DCBA group was 47.8% (376/786), compared with 36.2% (283/782) in the PBA group. The pooled results showed a significant statistical difference between the two groups, with a high risk of heterogeneity (OR = 1.77, 95% CI = 1.22–2.56, Z = 3.04, p = 0.002, I2 = 56%, Figure 3(b)). Heterogeneity was reduced to low (I2 = 0%) if one study was omitted. 18 As the sensitivity analysis showed no change in the pooled results after omitting each study, these results were considered relatively reliable. No significant publication bias was observed in the Egger test (p = 0.954).
Three studies reported TLPP at 18-months and 24-months.22,23,29,32 The pooled results showed no significant difference between the DCBA and PBA groups at 18 months (OR = 1.46, 95% CI = 0.89–2.39, p = 0.13, Z = 1.51, I2 = 33%), or 24 months (OR = 2.06, 95% CI = 0.14–29.62, p = 0.60, Z = 0.53, I2 = 65%).
Circuit access primary patency
Eight studies reported CAPP at 6 months.14,15,17,21,22,24–26 The pooled CAPP at 6 months in the DCBA group was 64.1% (300/468), compared with 49.2% (228/463) in the PBA group. The pooled results showed a significant increase in this variable with DCBA versus PBA, with a high risk of heterogeneity (OR = 2.07, 95% CI = 1.21–3.54, Z = 2.66, p = 0.008, I2 = 67%), Figure 4(a)). The sensitivity analysis showed no change in the pooled results after omitting each study, indicating reliability. The results of the Egger test showed no significant publication bias (p = 0.453).
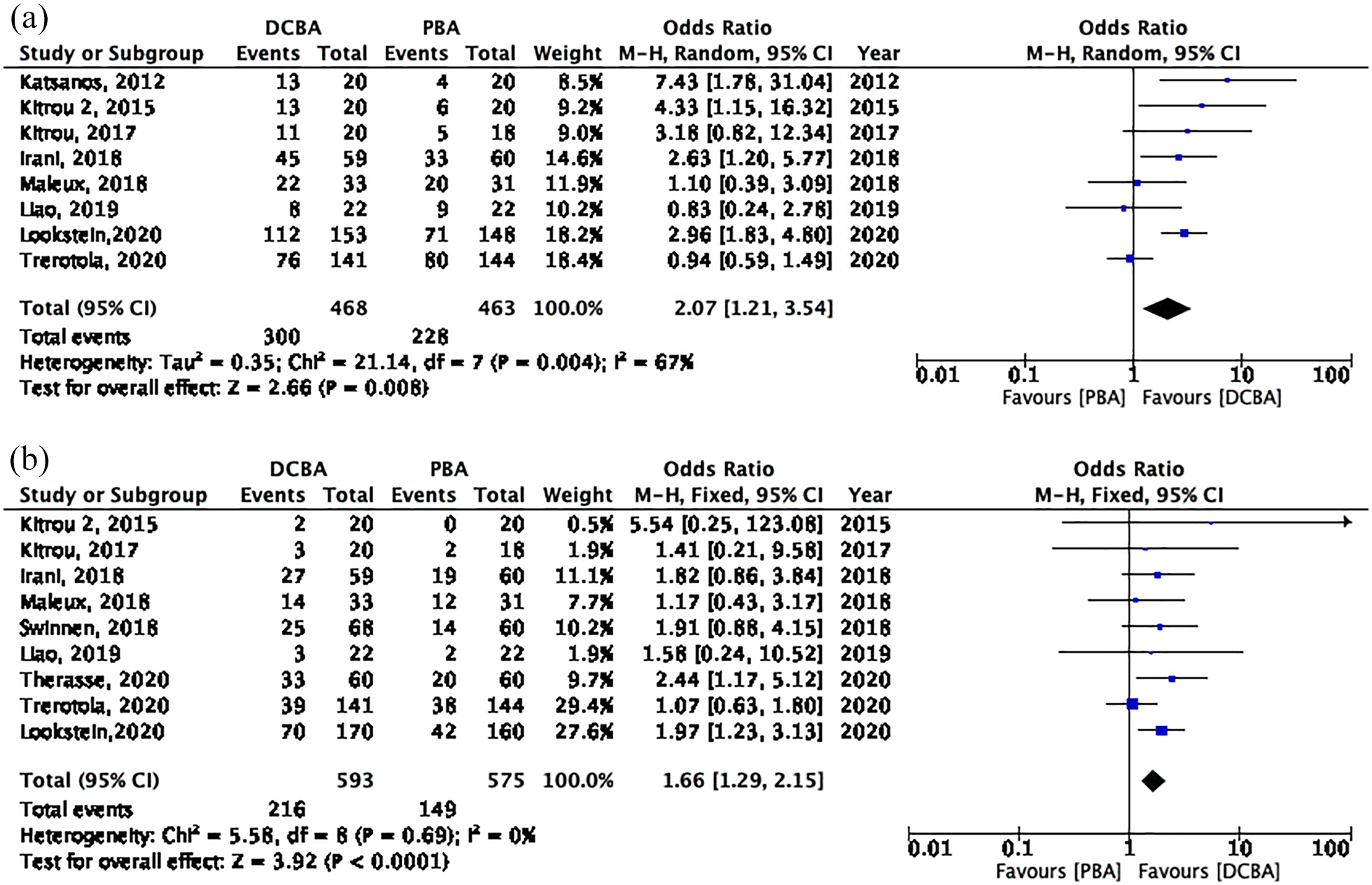
Forest plots of circuit access primary patency (CAPP) at (a) 6 months and (b) 12 months between drug-coated balloon angioplasty (DCBA) and plain balloon angioplasty (PBA). CI, confidence interval; M-H, Mantel-Haenszel.
Nine studies reported CAPP 12 months.14,15,17,23–27,31 The pooled CAPP at 12 months in the DCBA group was 36.4% (216/593) compared with 25.9% (149/575) in the PBA group. The pooled results showed a significant increase in this variable with DCBA versus PBA, with a low risk of heterogeneity (OR = 1.66, 95% CI = 1.29–2.15, p < 0.001, Z = 3.92, I2 = 0%, Figure 4(b)). The results of the Egger test showed no significant publication bias (p = 0.660).
Only one paper reported CAPP at 18- and 24-months. 32 The CAPP at 18-months in the DCBA group was 21.2% (24/113) compared with 18.4% (24/130) in the PBA group. The CAPP at 24-months was 0 in both DCBA and PBA groups.
Subgroup analysis based on study design
The pooled CAPP at 6 months (OR = 2.55, 95% CI = 1.77–3.68, p < 0.001, Z = 5.03, I2 = 1%) and 12 months (OR: 1.89, 95% CI = 1.37–2.62, p = 0.0001, Z = 3.87, I2 = 0%) indicated that DCBA was more effective compared with PBA in the prevention of stenosis where pre-dilation was used (Supplemental Figure 1A and 1B). However, the pooled CAPP with no pre-dilation at 6 months (OR = 3.17, 95% CI = 0.93–10.82, p = 0.06, Z = 1.85, I2 = 78%) and CAPP at 12 months (OR = 1.34, 95% CI = 0.89–2.03, p = 0.16, Z = 1.40, I2 = 0%) indicated no significant differences between DCBA and PBA (Supplemental Figure 2A and 2B).
The pooled TLPP at 6 months showed significant differences between DCBA and PBA group with both pre-dilation (OR = 2.86, 95% CI = 2.07–3.95, p < 0.001, Z = 6.34, I2 = 0%) and no pre-dilation (OR = 3.39, 95% CI = 1.12–10.24, p = 0.03, Z = 2.17, I2 = 73%) (Supplemental Figures 1C and 2C). The pooled TLPP at 12 months with no pre-dilation also demonstrated a significant difference between the groups (OR = 1.61, 95% CI = 1.10–2.34, p = 0.01, Z = 2.46, I2 = 37%, Supplemental Figure 2D). However, the 12 months TLPP with pre-dilation showed no significant difference between the two groups (OR: 1.64, 95% CI = 1.00–2.67, p = 0.05, Z = 1.98, I2 = 65%), owing to the influence of the study by Bjorkman et al. 18 (Supplemental Figure 1D).
30-day adverse events
Seven studies14,15,26–29,31 reported 30-day adverse events. Overall, 3.9% (22/558) individuals had adverse events in the 30 days after the index procedure in the DBCA group, compared with 3.5% (19/550) in the PBA group. Four studies26,27,29,31 reported 0 adverse events in this time period. The pooled 30-day adverse events indicated no significant difference between the DCBA and PBA groups, with a high risk of heterogeneity (OR = 1.09, 95% CI = 0.30–3.98, p = 0.90, Z = 0.12, I2 = 66%, Supplemental Figure 3). One study 14 accounted for most of the heterogeneity, with I2 = 0% following its omission. The results of the Egger test showed no significant publication bias (p = 0.051).
Technical Success
Thirteen studies14,16–18,21–26,28–30 reported technical success rates (Supplemental Figure 4). Only three studies reported technical success rates of less than 100%. Overall, technical success was observed for 96.7% (551/570) in the DCBA group, compared with 99.1% (564/569) in the PBA group. There was no significant difference in technical success between the two groups, with high heterogeneity (OR = 0.18, 95% CI = 0.02–1.92, p = 0.16, Z = 1.41, I2 = 66%, Supplemental Figure 4). There was no significant difference in the results when each of the included studies were omitted. The results of the Egger test showed no significant publication bias (p = 0.325).
Discussion
Maintaining the effectiveness of HD access is a challenge that frequently requires remedial treatment owing to complications associated with arteriovenous (AV) access. Stenosis is the most common complication, which may be life-threatening and seriously affects the quality of HD. 5 Venous stenosis is often the result of neointimal hyperplasia, 6 which leads to AV access non-maturation or dysfunction. 34
PTA is the first-line treatment recommended by the KDOQI guidelines for stenosis in HD access. 3 Previous research has suggested that DCBA could reduce the times of intervention and prolong the access lifespan compared with PBA,35–38 despite no significant difference in the primary patency at 200 days compared with PBA. 23 However, an RCT conducted by Bjorkman and colleagues 18 with a one year follow-up period suggested that target lesion revascularization-free survival was worse after DCBA. This study contributed to a high risk of heterogeneity in past meta-analyses. Compared with previous systematic and meta-analyses, we included 16 RCTs, 8 of which were multicenter, which included 1672 individuals, most of whom received AVF. We evaluated the effectiveness of paclitaxel drug-coated balloon angioplasty, and found the TLPP and CAPP at 6 and 12 months was superior with DCBA compared with PBA. The TLPP in the DCBA group was 75.2% and 64.1% and the CAPP was 47.8%, and 36.4% at 6 and 12 months, respectively; this is similar to the values reported in previous studies.8,10 However, the TLPP and CAPP at 18 or 24 months were not significantly different between the groups. These findings are clinically useful, describing the short and long-term benefits of DCBA.
A meta-analysis in 2018 found that paclitaxel-coated stents and balloons used in individuals with PAD for claudication were associated with an increase in 5-year all-cause mortality. 19 As the relevance of this in people who receive hemodialysis was unclear, the 2019 KDOQI guidelines did not make a recommendation regarding the use of drug-coated balloons. 3 Our analyses showed no significant difference in all-cause mortality between DCBA and PBA at 6, 12, and 24 months; these values were 4.48%, 7.9%, and 19%, respectively (Figure 2). This result corresponds with the annual mortality of the population of people receiving HD in general. 39 Factors affecting mortality in this group include cardiovascular events, infection, nutrition, age at dialysis, and others.39–42 Paclitaxel had been used for almost 30 years as a chemotherapeutic agent in cancer, and can prolong lifespan. 43 Although the dosage used in chemotherapy is greater than in DCBA, no studies demonstrating increased mortality with paclitaxel in a proper application. Thirty-day adverse events also need to be considered, as an indicator of safety; our analysis found no significant difference in 30-day adverse events between DCBA and PBA. Based on the results, paclitaxel-coated balloons do not appear to increase all-cause mortality among people who receive HD.
The pooled technical success results also showed no significant difference between the DCBA and PBA groups. Interestingly, in the subgroup analysis, DCBA with pre-dilation was associated with a longer CAPP with significant differences at both 6 and 12 months compared with the group with no pre-dilation. The technical success rate with pre-dilation was also slightly higher than with no pre-dilation (99.6% vs 96.7%). This indicates that pre-dilation before DCBA should be used.
Limitations
There were several limitations to this study. First, Although the number of RCTs and patients enrolled in our meta-analysis was greater than in previous comparable studies, some articles did not distinguish between types of HD access, or list outcomes based on the type of HD access, and some did not distinguish between types of stenosis. Secondly, the follow-up time in most studies was 12 months, and the longest follow-up among the studies was 24 months. Compared with other diseases such as PAD, individuals with end-stage renal disease receiving HD are vulnerable to complications that were not easy for longer follow-up periods. Only a few articles reported on 24-month data, so our analysis has limited value in assessing this outcome. Thirdly, this meta-analysis was not registered in PROSPERO. Finally, sample sizes of enrolled articles were different, and the presence of heterogeneity and bias also affected outcomes.
Conclusions
In hemodialysis circuit stenosis, DCBA appears to result in similar all-cause mortality but better TLPP and CAPP compared with PBA. However, heterogeneity and risk of bias in the enrolled studies mean that these results should be interpreted with caution. Further studies that extend the follow-up period to 2–5 years are needed to provide more extensive safety and efficacy data for the use of DCBA.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298211070125 – Supplemental material for Long-term mortality and patency after drug-coated balloon angioplasty in the hemodialysis circuit: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-1-jva-10.1177_11297298211070125 for Long-term mortality and patency after drug-coated balloon angioplasty in the hemodialysis circuit: A systematic review and meta-analysis of randomized controlled trials by Yunfeng Li, Zhenwei Shi, Yunyun Zhao, Zhanjiang Cao and Zhengli Tan in The Journal of Vascular Access
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
All analyses were based on previous published studies, thus no ethical approval and patient consent were required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.