
Abstract
Introduction:
Tunneled cuffed catheters (TCC) are generally used as a temporary means to provide hemodialysis (HD) until permanent arteriovenous access is established. However, certain complications are associated with use of TCCs such as infections, catheter malfunction/malposition or venous stenosis. Limited data is available on outcomes and long term complications associated with TCCs in our country. The aim of this study was to study the outcomes of TCCs and associated long term complications during the course of its usage.
Methods:
We retrospectively studied case records of patients who had TCCs placed for HD at our institution, from January 2016 to June 2018.
Results:
A total of 116 TCCs were placed during the study period. The mean age of the population was 57.09 years; 58.6% were males. The right internal jugular vein (52.6%) was the most common site of TCC insertion followed by the left internal jugular vein (29.3%). Functioning TCCs were successfully removed in almost two-thirds of cases (65.7%) once their permanent access was mature. Development of catheter related blood stream infection (CRBSI) was seen in 22 patients (19.8%) requiring catheter removal in 14 (12.6%) patients. Mechanical complications leading to catheter removal were seen in seven patients (6.3%). The median catheter duration was 62.5 days ranging from 1 to 343 days.
Conclusion:
TCCs, though associated with complications particularly CRBSI, are a viable option for short- to intermediate-term use for HD till the maturation of permanent arteriovenous access in a limited-resource setting.
Introduction
Tunneled cuffed catheters (TCCs) are a feasible option for hemodialysis (HD) access. They are relatively easy to insert, and are immediately available to use after placement especially in patients with poor vascular anatomy, cardiac dysfunction, poor general condition, history of failed or difficult vascular access surgeries or any other reason hindering their chances of having a functioning permanent vascular access for HD. 1 This is particularly relevant in low and middle income countries like Pakistan where a great majority of patients do not receive regular medical care precluding timely creation of permanent vascular access. 2 They typically present late in the course of disease necessitating initiation of HD via a temporary access in an emergent or semi-emergent setting. However, there are certain long-term complications associated with use of TCCs such as infections of the exit site or tunnel, catheter related blood stream infections (CRBSI), catheter kinking, mal positioning, malfunction or thrombosis and in the long run, central venous stenosis. 1
We studied the outcomes of TCCs in terms of catheter survival and magnitude of potential long term complications that may arise during the course of catheter since there is paucity of data in this area from our region. The information obtained would help develop better strategies to tackle the potential complications as well as would help create awareness among health care professionals regarding proper management of TCCs.
Materials and methods
We conducted a retrospective observational study of the patients who had TCCs placed at the Aga Khan University hospital, from January 2016 to June 2018. The institutional ethics review committee approved the study.
Medical records files of the patients were reviewed and data on age, gender, cause of renal failure, location of catheter insertion, reason for catheter insertion, type of procedure, past history of central line insertion, reason for catheter removal, CRBSI, microbial growth, catheter duration and dialysis vintage was collected on a performa.
Data was analyzed using software SPSS version 21. For descriptive statistics, means with standard deviation were reported for all quantitative variables with normal distribution whereas median with interquartile range was reported for all variables with skewed distribution. For categorical data, frequencies with percentages were reported.
Results
A total of 116 TCCs were placed during the study period. 98.3% procedures were performed electively by vascular surgeons using the percutaneous Seldinger technique in the operating room. Table 1 shows the baseline characteristics of the study population. The mean age was 57.09 years (range 18 to 86 years) with 58.6% males. Figure 1 shows age groups of the study population. More than half of the subjects (53%) were above 60 years of age
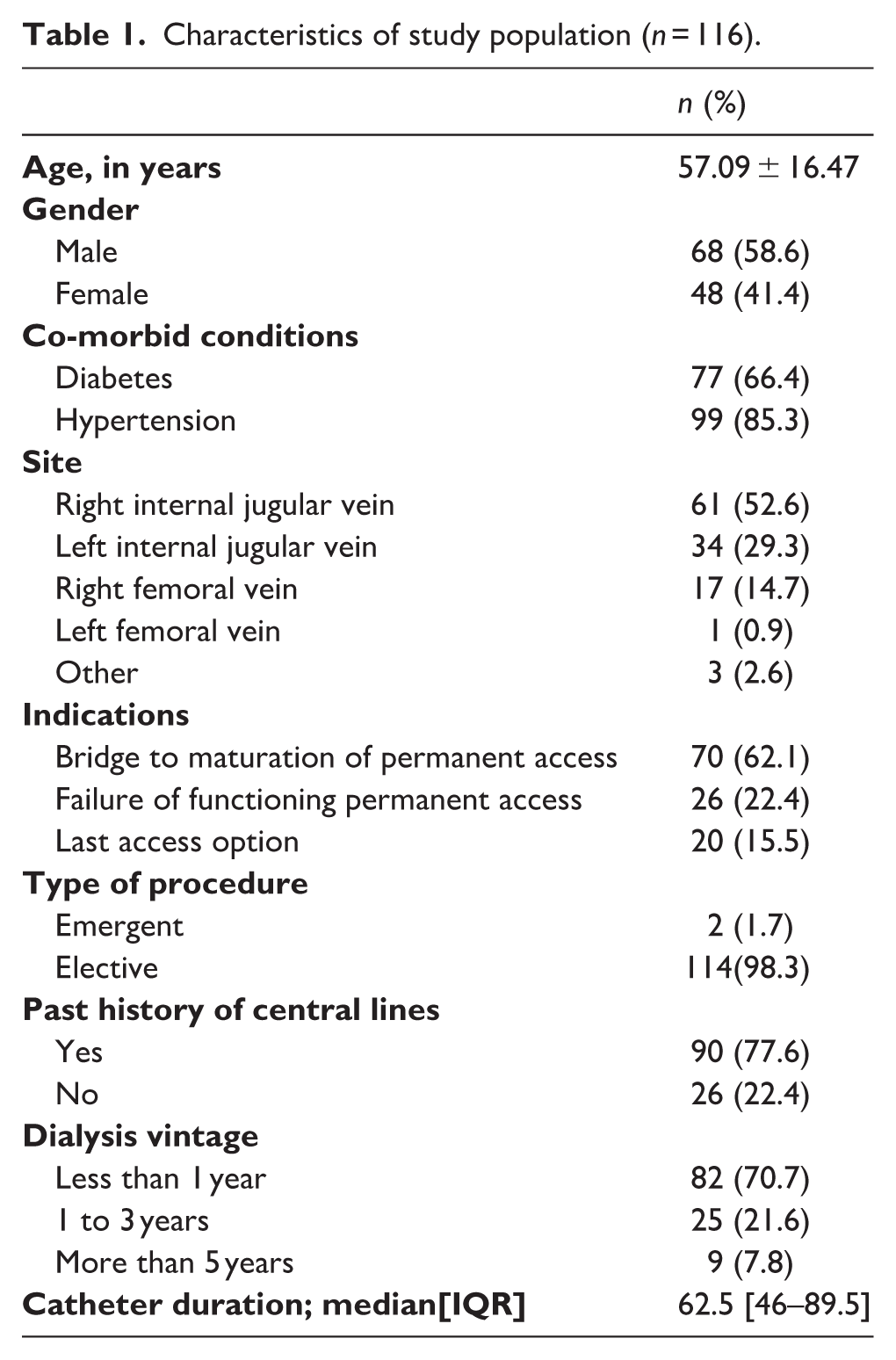
Characteristics of study population (n = 116).
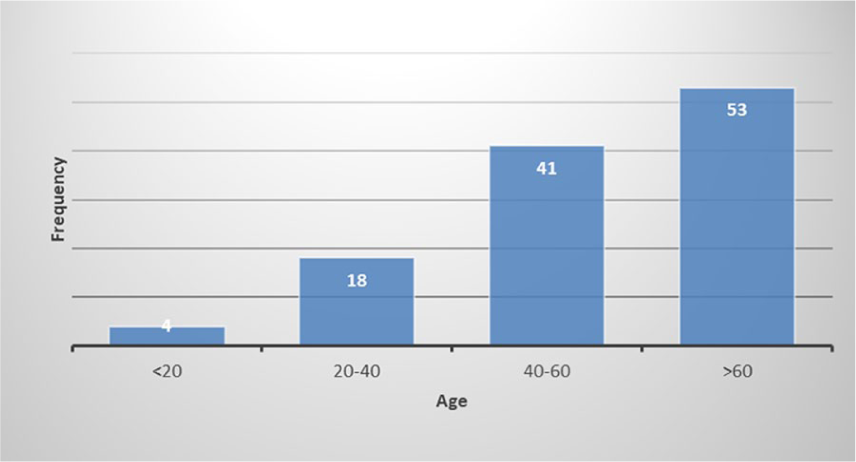
Age (years) groups of study population.
Hypertension was the most common co-morbid condition (85.3%) followed by diabetes (66.4%). Almost half of the patients (43.97%) had both diabetes as well as hypertension. Most of the patients had a dialysis vintage of 1 year (70.7%) while 21.6% of the patients were within their second or third year of dialysis treatment. The median catheter duration was 62.5 days ranging from 1 to 343 days.
The right internal jugular vein (IJV) was the most preferred site for catheter placement. The distribution of data according to site of catheter insertion is shown in Figure 2.
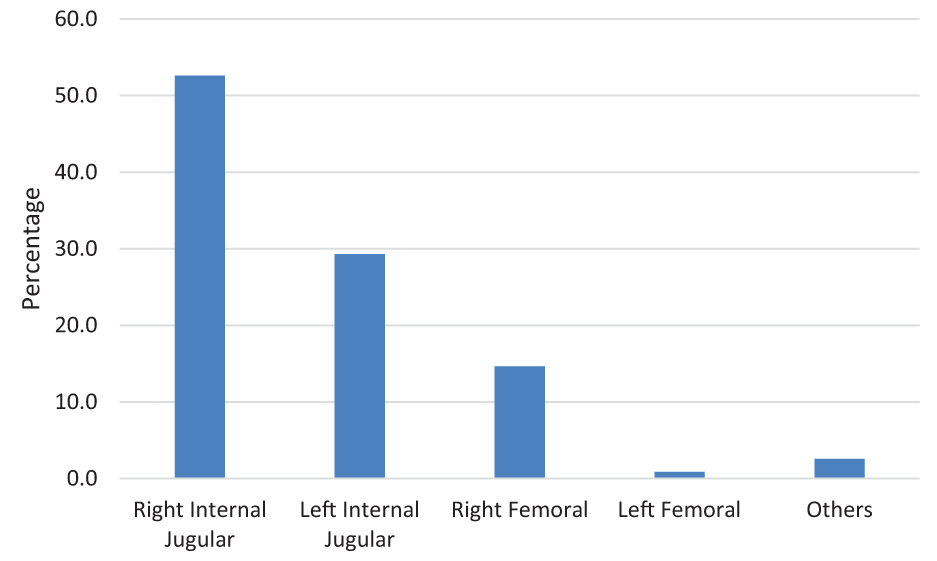
Sites used for tunneled cuffed catheters (TCCs) insertion.
Among the indications for TCCs, most of the patients (62.1%) required the procedure as a bridge to maturation of their permanent vascular access, either arterio-venous fistula (AVF) arteriovenous bridge graft (AVBG). 22.4% of the patients had a history of AVF/AVBG failure and hence required TCCs and in 15.5% cases, TCCs were placed as the only option for HD access.
Almost half of the TCCs were inserted after patients had initiated HD via a temporary non-tunneled catheter (44%).
Most of the patients had previous history of central lines placement for various indications (77.5%). Only 22.5% of patients were catheter naïve. Among those who had a history of previous central line insertion, there was a strong preference toward right IJV (48 patients); 12 patients had a history of left internal jugular central access; 21 patients had central lines in their right femoral vein and seven had left femoral catheterization. One patient each had a prior history of subclavian cannulation and a prior peripherally inserted central line insertion.
Figure 3 summarizes the outcomes of TCCs in study population. Of the total 116 cases, five patients were lost to follow-up and hence not included in analysis. Functioning TCCs were successfully removed in almost two-thirds of cases (65.7%) once their permanent access was mature and therefore catheters were no longer needed. Development of CRBSI was seen in 22 patients (19.8%) and necessitated catheter removal in 14 (12.6%) patients. Mechanical complications namely catheter malfunction, malposition, thrombosis, bleeding from catheter site and central venous stenosis (alone or in combination) leading to catheter failure and subsequent removal were noted in seven patients (6.3%). There were 16 deaths recorded (14.4%) with functioning catheters in place; out of those four patients died due to sepsis suspected to be CRBSI; rest of them had other co-morbid conditions as a cause/s of death namely acute myocardial infarction, pneumonia, congestive cardiac failure, stroke, and liver cirrhosis.
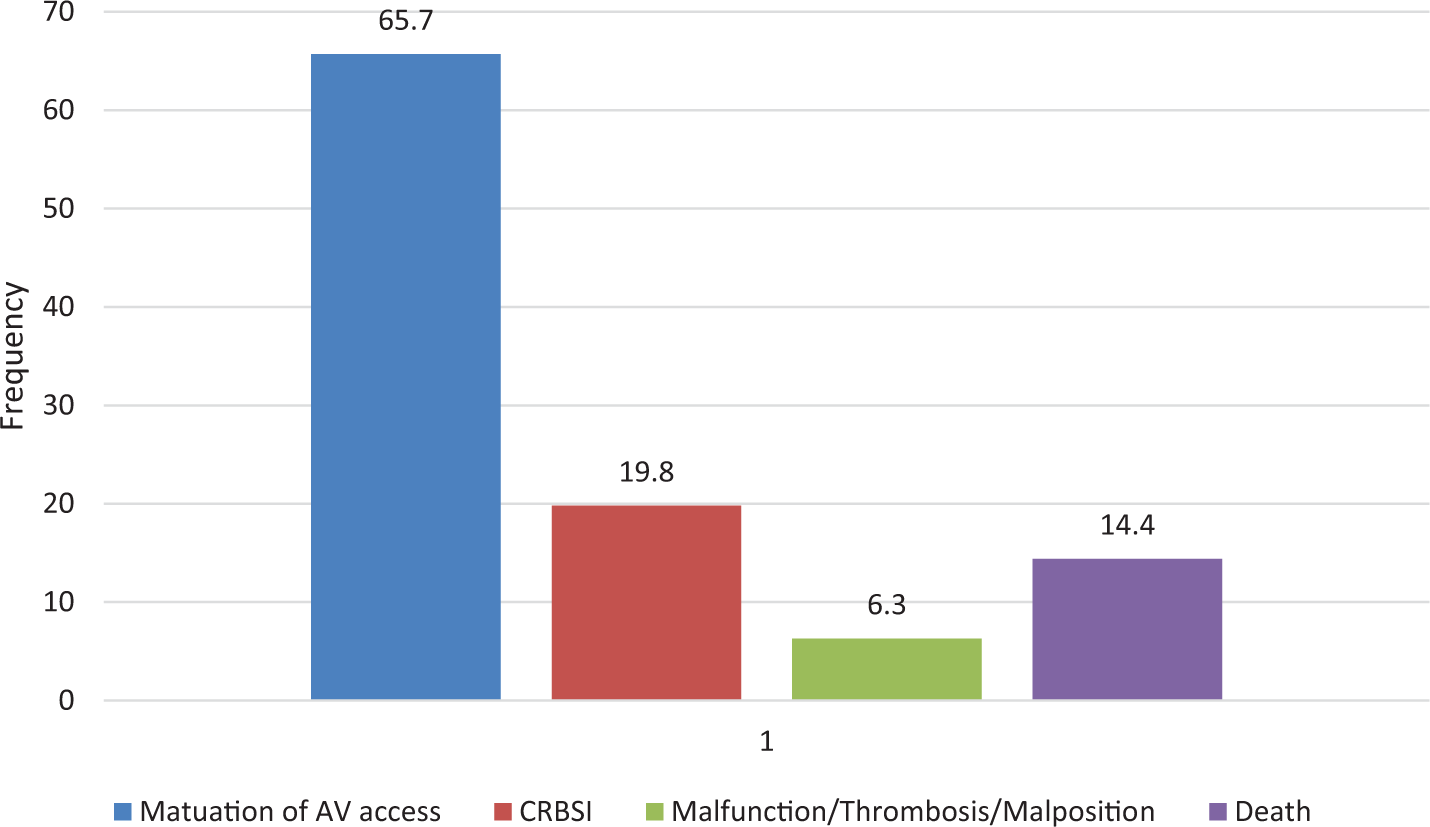
Outcomes of tunneled cuffed catheters (TCCs).
In patients who developed CRBSI, gram positive organisms were the most common isolates (60.4%) and Methicillin Resistant Staphylococcus aureus (MRSA) was the most prevalent organism (30.4%) followed by fungal infection, predominantly candida species (26%) (Figure 4).
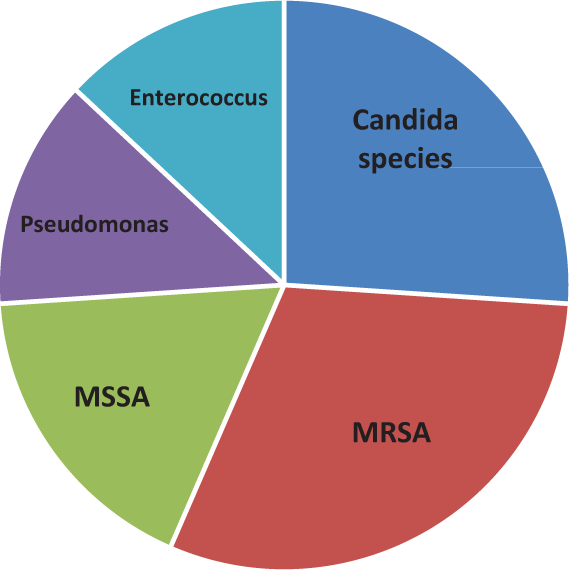
Microbial growth in patients with catheter related blood stream infection.
Discussion
TCCs are reserved for patients with unavailable permanent vascular access either as a bridge to maturation of AVF/AVBG or and in those with poor vasculature rendering a permanent access creation difficult. As a more elderly population with multiple comorbid conditions has been requiring HD in recent years, TCCs are now being widely used for access. 3
The leading reason for TCCs placement in our study was lack of a permanent HD access at the time of initiation of HD, followed by sudden failure of a functioning access in patients already on maintenance HD. Similar observations have been reported in earlier studies from the region as well as from the rest of the world.4–8 Pakistan has a huge burden of chronic kidney disease. 9 Owing to lack of resources and access to healthcare, a great majority of patients do not have a functioning permanent HD access at the time of commencement of HD. Most of these patients end up initiating HD via non-tunneled non-cuffed catheters. These catheters provide ease of placement at patients’ bed-side in an emergency setting without a need for an interventionist or a vascular surgeon; however, they are short-lived and have two- to three-fold higher incidence of CRBSI compared to TCCs. In our study, we found that around 44% of patients had already started HD via non-tunneled catheters at the time of TCCs placement.
IJV is the preferred site for TCCs placement due to its relatively straighter course anatomically, easy handling, lower infection rates and lesser chance of central venous stenosis compared to subclavian and femoral sites. Chung Ho et al stated that catheters inserted in IJV had better patency rates and lesser infections. 10 Our patient population had TCCs placed in right IJV in more than half of the cases and the practice is consistent with the findings from the region as well as other parts of the world.4–6,8,11 Femoral site could be an alternative choice in patients where conventional sites are not available or exhausted, in bed bound patients or those with severe orthopnea. 12 Maya et al. evaluated the outcomes and complication of femoral TCCs, and compared them to a group of matched control patients receiving an IJV dialysis catheter. They observed that femoral TCCs had a significantly shorter primary patency, but risk of CRBSI was similar to that from IJV catheters. 11 Sepas et al. from Iran in their case-control study found no significant difference between femoral and IJV TCCs in terms of the mean patency, complications (e.g. infection and thrombosis), and mortality rate. 13 In the present study, no significant difference in mean catheter duration and patency with respect to various insertion sites for TCCs were observed.
Among all complications associated with TCCs, infection especially CRBSI is the most feared one as it is associated with significant morbidity and mortality. Besides, CRBSI is a major cause of hospitalization and catheter removal hence substantially increasing healthcare costs.14,15 The infection rate of TCCs varies from center to center due to difference in practicing standards. Various risk factors for CRBSI have been identified such as co-morbid conditions especially diabetes, site of TCC placement, total number of catheter days, higher total intravenous iron dose, local infection, nasal carrier status for Staphylococcal aureus etc. Recently Martin et al from Melbourne, Australia published their findings that presence of diabetes and left internal jugular vein insertion site were independent risk factors for CRBSI. 16 Seventeen percent of the TCCs in their study were associated with CRBSI leading to removal of catheter in 16% cases. Castro et all reported a higher infection rate associated with TCCs (29.6%), with the mean catheter duration of 333 days explaining the higher frequency of infection. 7 In our study, around one-fifth (19.8%) of TCCs had resulted in CRBSI despite a median catheter duration of 62.5 days only. A similar rate of CRBSI has been described by an earlier study from our institution. 4 A of a higher rate of CRBSI could be partly accounted for by sub optimal living conditions of the patients coupled with the hot and humid climate in our part of the world that might have been a predisposing factor toward catheter colonization from skin flora. Furthermore, in almost a quarter of the patients, TCCs were placed via a guide-wire exchange over the non-tunneled lines already in place. Kumar et al from India, a country with similar prevailing circumstances, described a very low rate of CRBSI which they attributed to routine use of antibiotic lock. At our institution, however, use of antibiotic locks is not standard of care. 8 We believe that development of interventional nephrology programs, by making it possible to place TCCs at the time of emergency presentation, can play a vital role in reducing the burden of non-tunneled lines and CRBSI in developing countries.
Gram positive organisms are responsible for most CRBSI episodes associated with TCCs (40–84% cases). 16 Our CRBSI microbiology results are consistent with the international literature since gram-positive organisms were the most prevalent isolates (60.4%) (Figure 4). However, Candidemia was found in a significant proportion of patients (26%). A recent report on rates of central-line associated blood stream infections in acute care hospitals across the United States found that fungi, especially Candida species, account for up to 27% of infections. 17 None of the studies have reported such a high frequency of fungemia as CRBSI in patients with TCCs. A plausible explanation could be that advanced age, late presentation and initiation of HD and possibly a poorer nutritional status at the time of HD initiation rendered them immunocompromised and hence they were relatively more vulnerable to fungemia.
Our study has certain limitations. It is a retrospective analysis, and therefore some of the information especially follow-up may not be available. Although most of the patients receive their care in our hospital, there may have been external hospital admissions and complications that we may not have included. The median duration of catheter placement was not long enough to have captured patients with central venous stenosis. Lastly, it was a single-center study conducted at a tertiary care hospital hence the results might not be generalizable. The way forward would be larger prospective cohort studies comparing different aspects of catheter survival and complication especially CRBSI in relation to catheter duration, site, total number of catheters and need for additional procedures.
Conclusion
We conclude that TCCs are associated with certain complications, in particular CRBSI, yet are a viable and practical option especially in patients awaiting maturation of permanent HD access. Education of patients and HD staff on appropriate catheter care and infection control procedures are of utmost importance in reducing the burden of CRBSI. Moreover, efforts should be made to minimize the days and duration of TCCs by taking all measures to ensure timely availability of a permanent vascular access for HD. With this being said, some patients may still require long-term TCC use because of difficulty in establishing a permanent access, limited access options, a shorter life expectancy and patient preference.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Aga Khan University Hospital’s Ethics Review Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research involving human participants and/or animals
This article does not contain any studies with human participants or animals performed by any of the authors.