
Abstract
Background:
Peripherally inserted central catheter (PICC) has been widely used. The catheter-related complications might occur and the reports of secondary malposition into azygos veins were rare.
Methods:
This retrospective review summarized the experience in diagnosis and management of secondary malposition of PICC into azygos veins in 25 cases.
Results:
When the catheter dysfunction occurred in the PICC on the left limb, it was necessary to consider whether there would be malposition into azygos veins after other reasons were excluded. The malposition could be diagnosed by chest lateral radiograph or chest computed tomography. The secondary malposition into azygos veins was resolved by repositioning or withdrawing the PICC. After re-inserting the catheter, it should be closely monitored whether the malposition occurred again. Intracavitary electrocardiogram positioning technology was used to confirm the catheter tip position before using corrosive drug. After the catheters withdrawn from the azygos veins, close attention should be paid to the property and concentration of the infusion drug strictly and the complications such as blockage and re-malposition. No serious complications such as infection, thrombosis and extravasation occurred in this group of patients after treatment.
Conclusions:
The results of our study suggested that the right limb is recommended for PICC catheterization in order to avoid secondary malposition into azygos veins and the malposition into azygos veins should be dealt with in time.
Keywords
Introduction
Peripherally inserted central catheter (PICC) has been widely used in clinical practice.1,2 However, the catheter-related complications may occur during indwelling, and secondary malposition is one of the most common complications. The definition of secondary malposition is as follows: during catheter insertion, it is confirmed by chest X-ray, computed tomography (CT), digital subtraction angiography (DSA) and transesophageal echocardiography that the tip of the catheter is located in the vena cava, but the tip of the catheter moved to another position other than the vena cava during indwelling. It was reported that the incidence of secondary malposition of PICC is about 4%–12%. 3 PICC is often ectopic to the internal jugular veins, innominate veins, subclavian veins, axillary veins, etc. But reports of secondary malposition into azygos veins were rare. The azygos veins start from the right ascending lumbar veins, and carry the blood from right posterior intercostal veins, hemiazygos veins, accessory hemiazygos veins, and veins of the thoracic esophagus, pericardium, and main bronchus along the way. At the level of the 4th thoracic vertebra, the azygos veins curves forward to form azygos arches. The blood in azygos veins flows into the superior vena cava above the root of the right lung. The diameter of the azygos veins at the junction of superior vena cava is approximately 0.96 ± 0.18 cm. 4 When the PICC was inserted into the azygos veins through the azygos arches or their branch, it would form a right angle or acute angle. Coupled with long-term mechanical stimulation, there might be catheter blockage, thrombosis, vascular wall damage, etc. If infused with drugs that are irritating to blood vessels when PICC in the azygos veins, it might cause drug extravasation and damage to surrounding tissues. In severe cases, it could be life-threatening. From January 2017 to January 2019, there were 25 patients with secondary malposition of PICC into azygos veins which is found by CT examination in our hospital, and no adverse consequences occurred after timely treatment. The nursing care experience was reported as follows.
Patients and methods
This study is a single-center, observational, retrospective study. Eligible patients were from the Department of IV team, Sir Run Run Shaw Hospital, Zhejiang University. Our requirements to screen patients for our study were as follows: (1) patients aged 18 years and above, (2) confirmed secondary malposition of PICC into azygos veins by CT examination in our hospital, (3) received treatment for secondary malposition in our hospital.
This study was performed with the approval of the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University (20190725-159). All patients were enrolled after signing informed consent.
Results
Clinical information
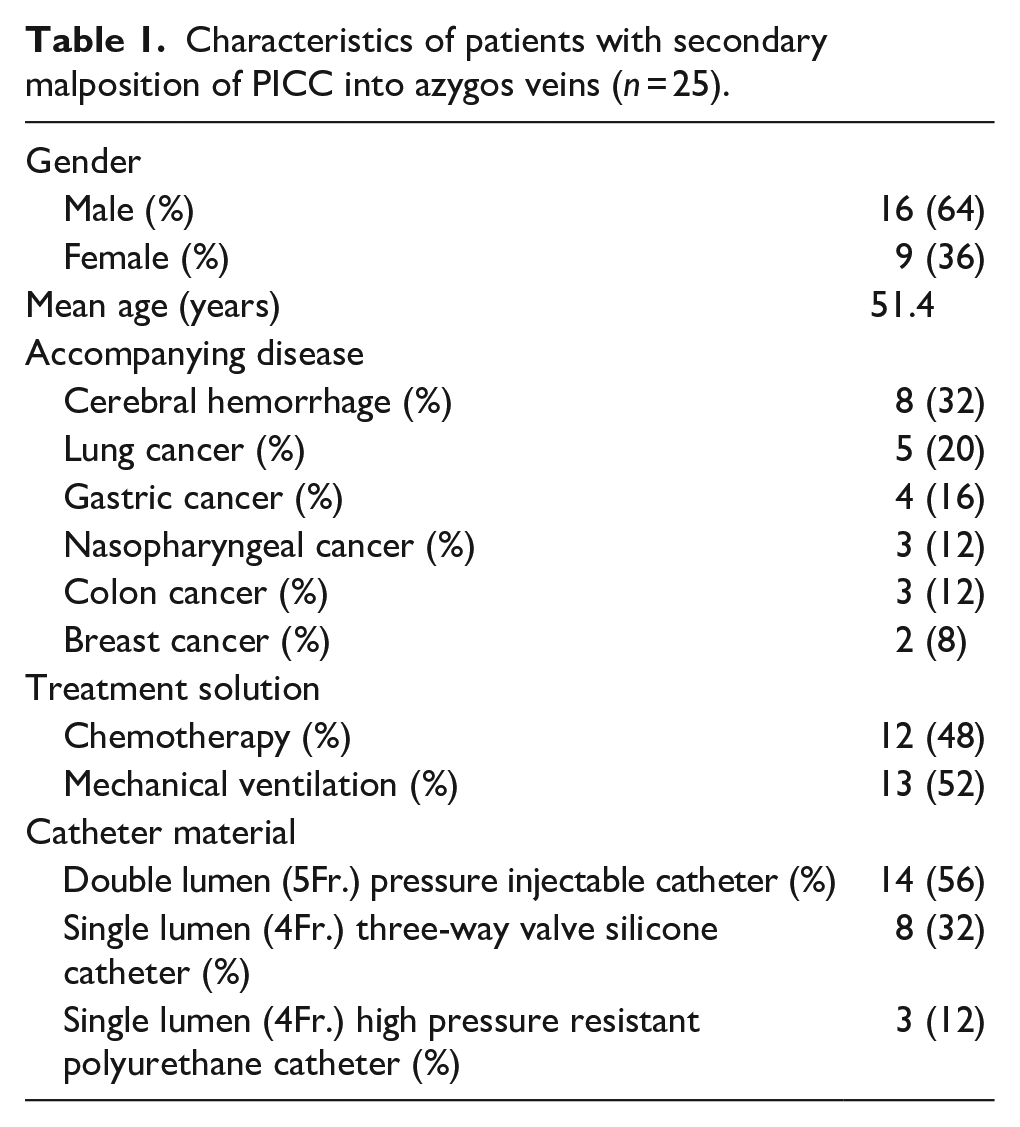
There were 25 cases in our group, 16 patients were male and nine were female. The characteristics of the 25 patients were summarized in Table 1. The mean age was 51.4 years (range 32–66 years). In this group of patients, there were eight cases of cerebral hemorrhage, five cases of lung cancer, four cases of gastric cancer, three cases of nasopharyngeal cancer, three cases of colon cancer and two cases of breast cancer. There were 12 cases of chemotherapy and 13 cases with ventilator assisted breathing. Twenty-five cases were intubated through the left upper limb, of which 18 cases through left vena basilica, five cases through left brachial vein. There were 14 cases with double-lumen 5F high-pressure resistant polyurethane catheter, eight cases with single lumen 4F three-way valve silicone catheter and three cases with single lumen 4F high pressure resistant polyurethane catheter. The discovery time of secondary malposition into azygos veins is between two and 143 days after catheter insertion. The catheters in five cases continued to be used successfully after changing patients’ body position and injecting 0.9% Saline quickly, and the catheters continued to be indwelled (69.4 ± 31.3) days. 14 cases used the PICC as medium-length catheters after the tips were withdrawn from the azygos vein. Two cases of double-lumen catheter had one-lumen blockage, which was recanalized after intraluminal thrombolysis, and the catheters continued to be indwelled (61.3 ± 18.9) days. In six cases, the PICC was removed and a new PICC inserted. None of the patients in our group had serious adverse consequences such as infection, drug extravasation, and thrombosis.
Characteristics of patients with secondary malposition of PICC into azygos veins (n = 25).
Discussion
Diagnosis of secondary malposition into azygos veins
Secondary malposition of PICC into azygos veins is usually asymptomatic or not obvious. It is often found in retrospective study of complications or during imaging examinations, which brings difficulties and challenges to early recognition. It was reported that most of the primary and secondary malposition of the pacemaker leads and PICC into azygos veins were inserted through the left limb.5,6 The patients in our group were all inserted through the left limb. It was reported that increased intrathoracic pressure is an important cause of secondary malposition into azygos veins.7,8 In this group, 13 patients received positive pressure ventilation with ventilator, and two patients frequently coughed and expectorated sputum, all of which would lead to increased intrathoracic pressure. The authors had difficult blood withdrawal in five cases, difficult infusion in four cases and complete lumen occlusion in one case, and two cases showed that the tips of the catheters were thickened or kinked on the chest frontal radiograph, all findings that were not evident on the post-procedural chest x-ray. Therefore, when PICC is used, blood should be withdrawn before infusion to make sure catheter intravenous, which was in strict accordance with the practical standards. When catheter dysfunction occurs, such as difficult blood withdraw or poor venous infusion, the cause should be clarified. After excluding other reasons, patients with malposition predisposing factors with a catheter on the left limb should consider the possibility of malposition of catheter, and chest frontal radiograph and chest lateral radiographs should be taken.
In addition, if there is the chest radiograph showing that the tip of the catheter is located near the bronchial bifurcation and is thickened, kinked or hooked, additional chest lateral radiographs could be taken to confirm the diagnosis (Figures 1 and 2). If the catheter is ectopic to the azygos veins, it can be seen on the image that the catheter goes posterior at the level of the 4th to 5th thoracic vertebrae. Chest CT examination can observe the direction of the catheter tip more clearly. It was reported that the PICC is ectopic to azygos veins during CT examination.9,10 In this group, four cases with high-pressure resistant PICC showed that the catheter was ectopic to the azygos vein after high-pressure injection of contrast agent. The mechanism obeys Newton’s third law of motion, that is, the force and reaction force are always equal in magnitude, opposite in direction, acting on the same straight line. 6 When the contrast agent injected rapidly, the tip of the catheter moves in the direction of least resistance, then might shift upward to the azygos vein. It is recommended to evaluate the position of the catheter tip after enhanced CT and MRI examinations, so as to find out in time that the catheter tip is ectopic due to the high pressure injection of the contrast agent in the catheter.6,9,11
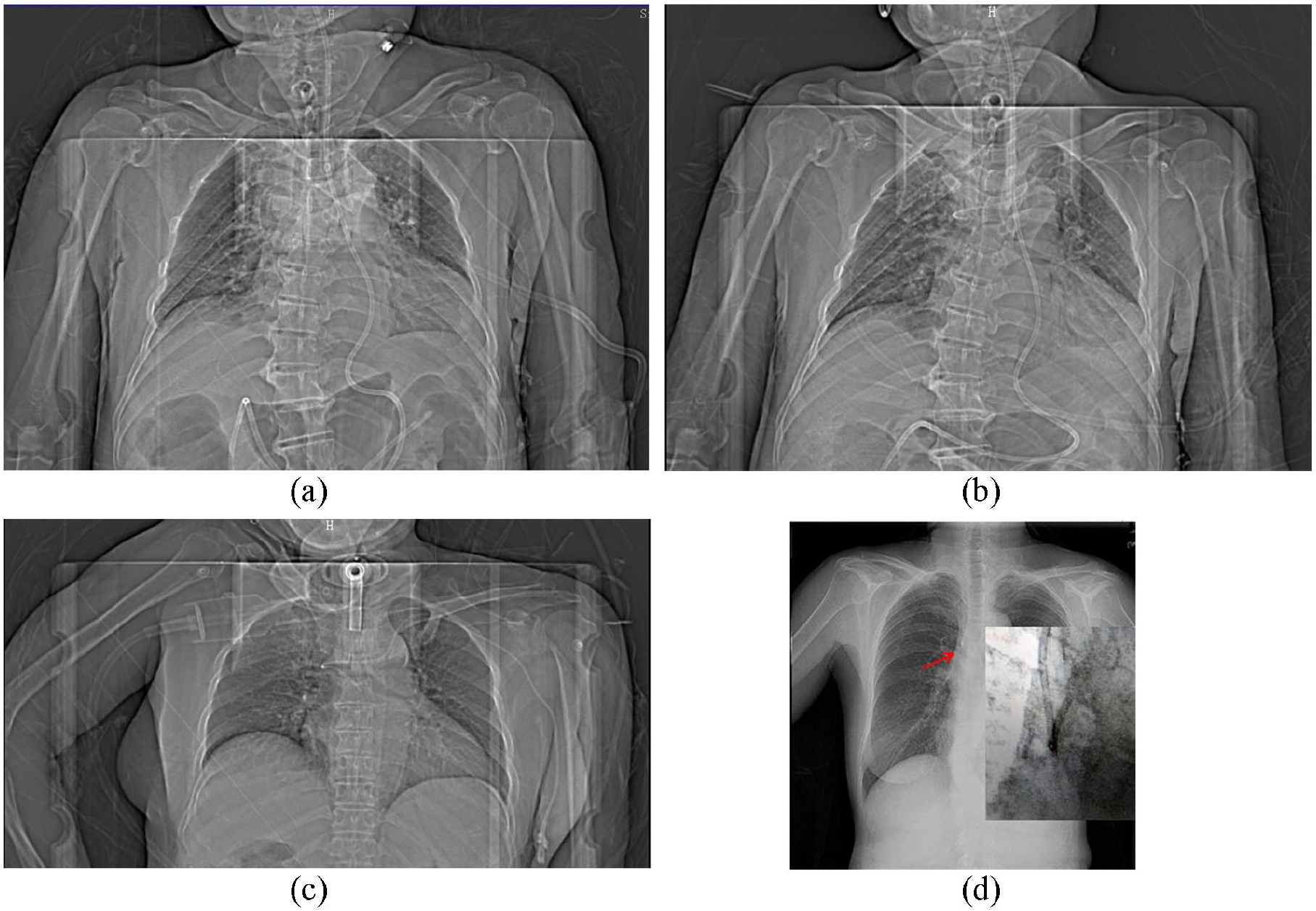
Chest frontal radiograph showed the catheter tip is normal (a), hooked (b), thickened (c), or kinked (d).
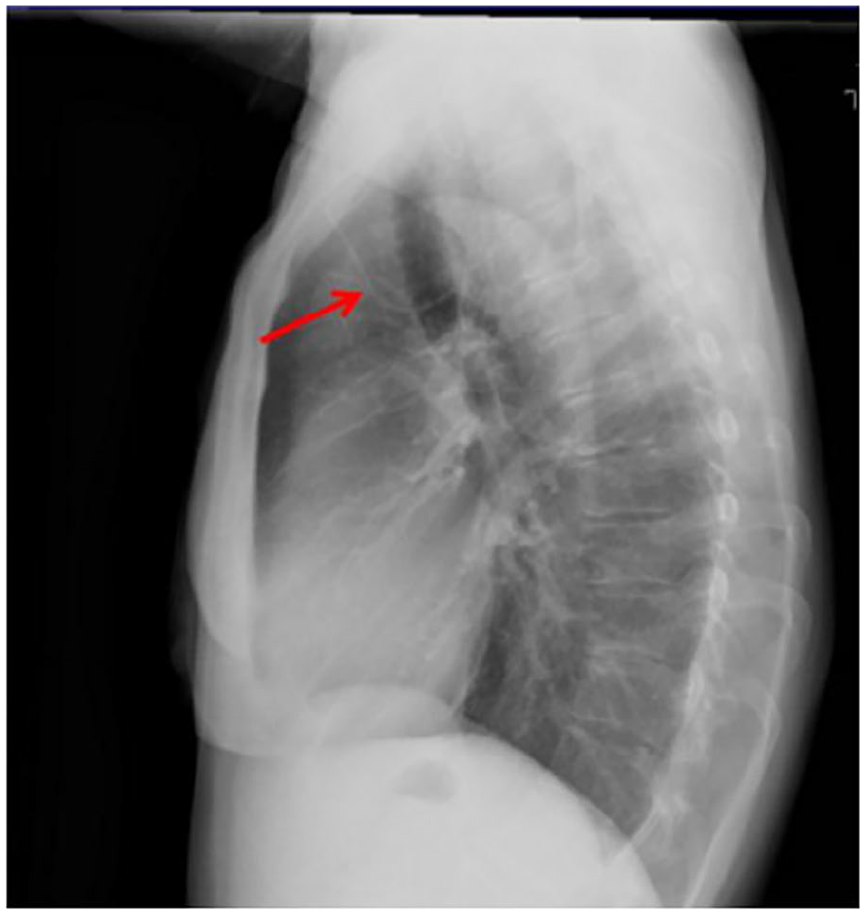
Chest lateral radiograph showed the catheter tip was located in the azygos vein.
Management of secondary malposition of PICC into azygos veins
Once the secondary malposition of PICC into azygos veins is found, it should be dealt with in time. In the cases of secondary malposition into azygos veins, it is necessary to determine whether to allow the change of patient’s position or drug properties according to the patient’s condition.
In this group of patients, 12 patients were allowed to change their positions. They took a sitting position, leaned their body forward 45° and extended their shoulder joint to the maximum angle in order to move the tip of the catheter up.12,13 The authors performed a jet injection of 0.9% Saline and checked the result using the intracavitary electrocardiography method of tip location.14–18 After the appearance of high-amplitude P waves, chest radiograph showed that the PICC was re-positioned into the vena cava in five cases. Considering the possibility of re-malposition, the intracavitary electrocardiogram positioning technology was used to confirm the position of the catheter tip before using of vesicant drugs. If using non-vesicant drugs, there is less risk of tip malposition than vesicant drugs. The catheter was used until the end of treatment in the five cases, and the catheters were kept indwelled (69.4 ± 31.3) days.
In seven patients, non-invasive repositioning was not successful or not applicable because they could not cooperate. After evaluating the properties of the drugs, the catheter was withdrawn from the azygos vein and left in place. The length of the catheter which was withdrawn from the azygos vein was measured by the measuring ruler in image browsing software. First, perform a sectional straight line measurement from the puncture point to the entrance of the azygos vein, then calculate the length after adding sections, and then calculate the difference between the result with the actual length. This is a relatively fuzzy measurement and the length inside the body cannot be completely accurately measured. In order to reduce error in the measurement, we would add 1-2cm. After the catheter was withdrawn, the chest radiograph showed that the tip of the catheter was at the level of 3rd or 4th thoracic vertebra. The tip of the catheter was above the entrance of the azygos vein, at the junction between the innominate vein and the superior vena cava, or in the superior segment of the superior vena cava. These venous catheters were classified as non-central and therefore not appropriate for infusion of vesicant drugs or other solutions requiring a central route. The authors would mark the non-central venous catheter with a clear mark on the bedside of the patients. And the authors would mark the position of the catheter tip on the maintenance manual and medical records. Non-central venous catheters would be used as medium-length catheters. The authors also inform patients or family members of the results. After the catheter was withdrawn, the exposed length of the catheter was 5–9 cm, which increased the difficulty of catheter fixation and maintenance. The operator should strictly abide by the principle of aseptic operation during maintenance and sterilize catheter. Avoid sharp angles and folding when fixing the catheter. The exposed catheters should be fixed in the wound dressing. The three-way valve catheter could be trimmed in vitro, and trimmed catheters were given in two patients, which solved the problem of excessively exposed catheters.
In addition, if the tip of the catheter wasn’t at the suitable position, the incidence of re- malposition and blockage would increase. Two double-lumen catheters in our group were blocked at the 31th day and 48th day after treatment. The catheters were used normally after intraluminal thrombolysis by urokinase.
In 19 cases, the catheter was left in place without any severe complication such as infection or thrombosis for (61.3 ± 18.9) days. There were also six patients whose catheters were removed and were re-inserted due to central venous pressure measurement or infusion of chemotherapeutic drugs. Among six patients, four cases were successfully catheterized in the right limb, and two cases were still catheterized in the left limb due to poor venous conditions in the right limb. By reviewing the chest radiographs of the 25 patients, we found that the tips of the catheters in 16 patients did not reach the junction of the lower 1/3 of the superior vena cava and the right atrium. The catheters were not static in the blood vessel and would move 2–3 cm with blood flow and body position changes.19,20 When the tip of the catheter is near the bronchial bifurcation, which is the entrance of azygos vein, it is easier to be ectopic to the azygos veins. Therefore, it is recommended to use intracavitary electrocardiogram technology for real-time positioning during intubating catheter to ensure that the tip of the catheter reaches the suitable position. The catheter should be secured properly during PICC catheter indwelling period to avoid malposition.
Conclusion
In this group of patients, the secondary malposition of PICC into azygos veins all occurred at left upper limb and were all related to the anatomical characteristics of the azygos veins. For patients with increased intrathoracic pressure, more attention should be paid to the selection of the limb during catheter intubation and the right limb is recommended for catheterization.
Malposition into azygos veins is typically secondary to the inappropriate method of tip location. When the tips of the catheters reach the junction of the lower 1/3 of the superior vena cava and the right atrium, the occurrence of secondary malposition into azygos veins is extremely rare. So it is recommended to use intracavitary electrocardiogram technology for real-time positioning during catheter intubation to make sure the catheter tip in place accurately. When the catheter dysfunction occurs in patients with catheter on the left upper arm, the possibility of malposition into azygos veins should be considered after other complications have been excluded. Malposition into azygos veins could be confirmed through chest frontal radiograph, chest lateral radiograph or chest CT. After high-pressure injection of contrast agent, it is necessary to pay attention to whether the tip of the catheter is ectopic to azygos veins. Once it is confirmed that the secondary malposition of PICC into azygos veins, it needs to be dealt with in time. The tip of the catheter could be kept away from the entrance of the azygos veins by repositioning or withdrawing the catheter. In some cases, intravenous injection of 0.9% Saline can also be used to correct the position of the catheter tip. 21 If necessary, the catheter should be removed and re-inserted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Zhejiang Natural Science Foundation Committee (LGF19H160030), Sir RunRun Shaw Hospital Nursing Fund Committee (201902HL) and Zhejiang University School of Medicine (419000-11111/027/006).