
Abstract
Background:
The role of nurses in peripherally inserted central catheters (PICC) placement has been limited in France. Having a fully trained nurse-led PICC team can positively impact nursing profession and make better use of valuable human and economic healthcare resources. It can also improve the standards of patient’s care, procedural experience, and safety.
Aim:
The aim of this article is to report the successful outcomes of nurse-led PICC team performed over a 6-year period from a single central hospital in France.
Methods:
The authors reviewed all PICCs insertions performed by their trained nurse led team between 2014 and 2019. All quantitative and qualitative variables were considered: the patients admitted, the type of PICC inserted, overall procedural time, the mentor’s help, the insert failures, the number of punctures required, the procedural pain utilizing Visual Analog Scale (VAS), any procedural complications, chest X-rays needed, the follow up to the eighth day (D8).
Results:
From 2014 to 2019, 12,687 PICC were inserted with 128 failed procedures (1%). In 2019, 73% of procedural insertion time was less than 10 min. The request of support rapidly decreased to 2 calls/month. More than 90% of procedures were associated with mild pain (VAS ⩽ 3). After the first month of training, 81% of all procedures were performed with a single insertion puncture. Accidental artery puncture during procedure was 0.5%. The authors found room for improvement, progressing from 97% in the first year to 99% in 2019. Furthermore, the authors found that only 1.85% of all catheters developed local infection within D8, and only 0.83% evolved in vein thrombosis. Total bloodstream infection was at 0.1%.
Conclusion:
The authors report successful outcomes from data collected during the 6-year period demonstrating clear benefits of a nurse-led vascular access team with regard to system wide efficiencies and patient satisfaction.
Keywords
Introduction
Safe and reliable central vascular access is an essential invasive procedure when a variety of treatments such as irritants, vesicants, parenteral nutrition, and long term intravenous therapy must be delivered to patients. Traditionally, inserting central venous catheters has been under the domain of medical practitioners (anesthetists, radiologists, surgeons) due to the potential procedural complications and technical complexities. In recent years the increased demand and medical shortage of practitioners has led to the adoption of trained-nurse insertion teams.1–8,13,14 Since 2009, in France, cooperation protocols between health caregivers allowed trained nurses to perform central venous insertions under a proper medical delegation of duty. The first French hospital to create a nurse-trained service for central venous access was Leon Berard Cancer Center in Lyon, France. 1 Following the example and experience of this facility, a similar service has been opened in our hospital (Lyon Sud Hospital Center, France).
The aim of this article is to analyze the results achieved during our experience of the initial 6-year period (from 2014 to 2019).
Materials and methods
When first established, our vascular access unit was composed of four trained nurses from the department of anesthesia plus two medical practitioners as delegates. The increasing demand for central venous access led to additional training of four more nurses, with a further addition of eight nurses and five physician mentors. The need for central venous access was always confirmed and patient’s clinical history carefully reviewed prior to the procedure. When initially established, the vascular access team performed only peripherally inserted central catheters (PICC) insertion, however more recently, included the insertion midlines, ports, and Broviac catheter. This article focuses only on the insertion of 4–5 French (Fr) PICCs inserted under ultrasound guidance and utilizing an ECG-based guidance system for tip positioning. The procedure was considered as a failure when the catheter could not be correctly placed in superior vena cava. Post procedural chest X-rays were only performed to check left-side insertions or in the presence of patients with heart rhythms without P-wave.15,16,18–21,27,29–31 Prior to commencing the procedure, an ultrasound assessment of the superficial and central veins anatomy was performed, using a Rapid Central Vein Assessment approach (RaCeVa). 22 The three most common indications for PICCs were chemotherapy (32.2%), antibiotic therapy (33.8%), and parenteral nutrition (16.4%).
Theoretical and practical training
The process for nurses to be accredited to insert vascular access devices (VADs) in the facility was divided into two parts: theoretical component and clinical training. The theoretical learning was structured in 30 h and it combined multiple components of device insertion and management: clinical indications, pathophysiological and anatomical review, clinical examination and patient assessment, ultrasounds, and chest X-rays interpretation. The clinical training process involved 30 observations of mentors demonstrating various inserting techniques, 30 mentor-supervised insertions, and 30 unsupervised insertions.
Assessing endpoints
The authors report the outcome of PICC insertions performed by their trained nurse team between 2014 and 2019 and the results archived were evaluated considering quantitative and qualitative variables: the number of patients admitted, the amount of PICC inserted, the insertion time, the number of situations requiring mentor’s help, the amount of insert failures, the quantity of punctures needed, the evaluation of patient’s procedural pain utilizing visual analog scale (VAS), arterial punctures, chest X-rays needed, follow up at D8.
Statistical data analysis
The authors decided to explore each variable of the data series separately, following an univariate time series approach: a sequence of measurements of the same variable collected over month and years. The objective was to determine a model that described our time series. In order to achieve this, the authors used the following time series forecast methods: preliminary graphic analysis (mean, variance, standard deviation); centered moving average for smoothing data (windows width = 12); exponential smoothing; ordinary regressions models. “R2” describes the ratio of the variable Y explained by the variable X, which is an index of the curve's reliability.
Results
From 2014 to 2019, 17,777 patients were admitted for VADs: Table 1 shows the entire yearly activity and the population studied. In 2014, 1316 patients were admitted for PICC insertion with 38 failed insertions (2.9%), and 6 arterial punctures (0.5%). In 2019 increased demand for VADs led to treat 3840 patients, 2204 for PICCs, the remainder for midlines, totally implantable venous access ports (TIVAPs) and Broviac, with 10 failures (0.5%), and 2 arterial punctures (0.1%).
Activity year-on-year and the population studied.
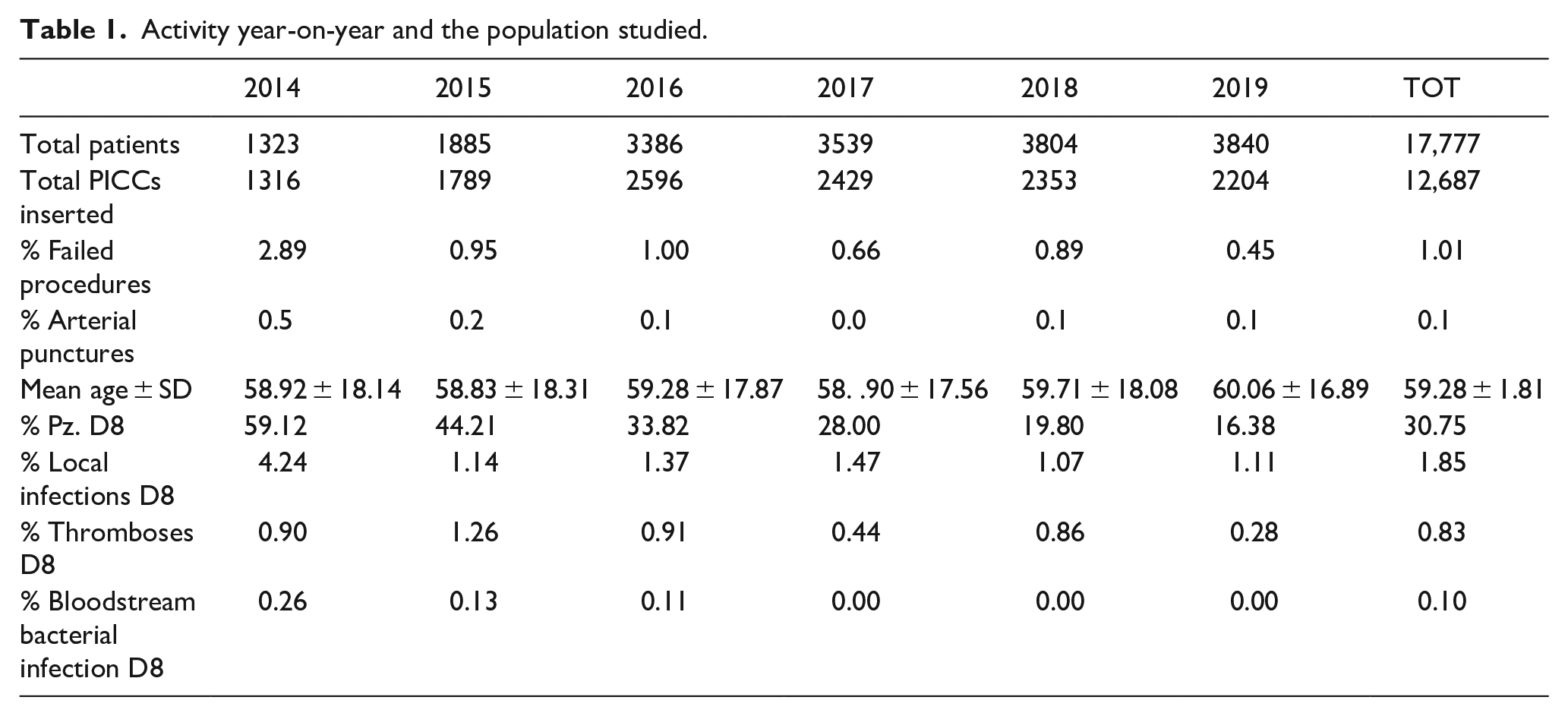
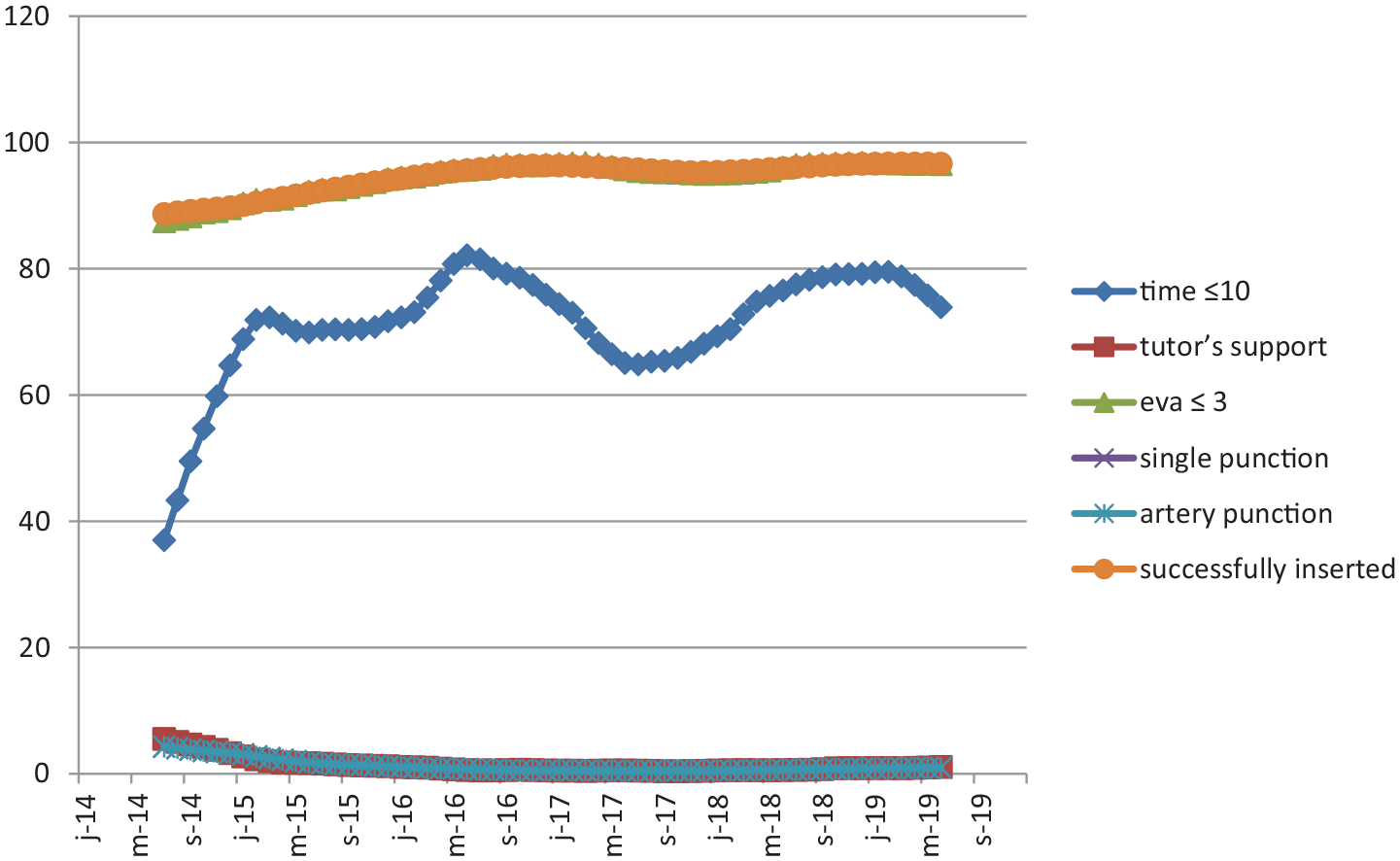
From 2014 to 2019, the authors received 12,687 patients for PICC insertions with only 128 failed procedures (1%). The insertion time rate remarkably decreased starting from the third month. In 2019, 73% of procedures were performed in less than 10 min (R2: 0.8014; Figure 1).
Rate of quantitative and qualitative variable studied.
Initially important, the request of mentor’s help rapidly decreased from an average of six (5.5%) calls per month in 2014 to two (1.2%) calls in 2019 (R2: 0.9922; Figure 2). To assess patient pain related to PICC insertion a visual analog scale was used (VAS). The authors found more than 90% of procedures being associated with mild pain (VAS ⩽ 3; R2: 0.9648; Figure 1).
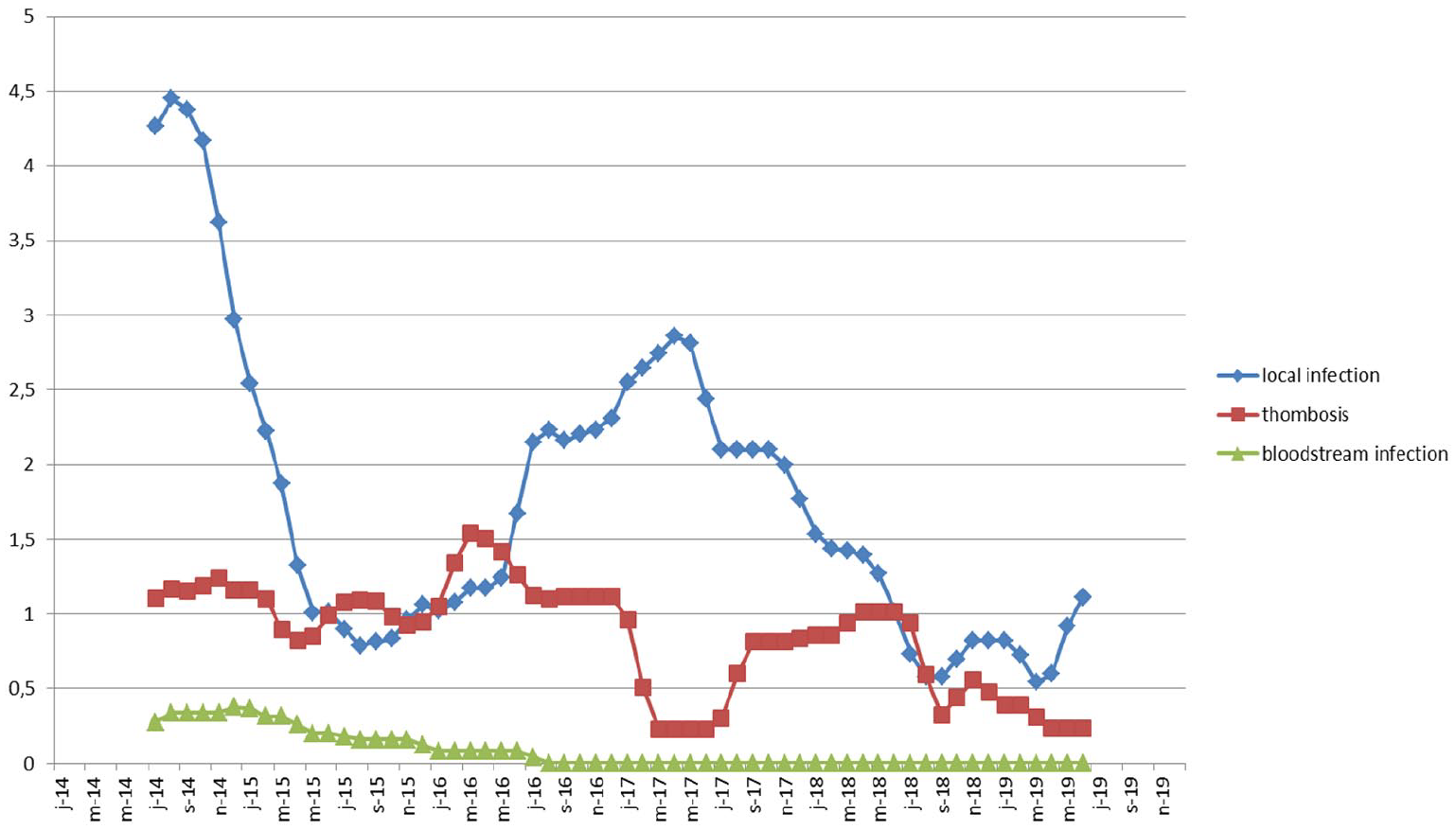
Rate of complications associated with PICC insertion.
With regard to the amount of puncture needed to insert successfully the PICC, the past first month, one puncture was necessary in 81% of cases, with an ongoing improvement of 89% during 2019 (R2: 0.8268 ; Figure 1). From the beginning, the authors found the number of incidental artery puncture rate during procedure was very low (0.5%) due to ultrasound needle guide usage (R2: 0.7631; Figure 1). However they found margin for improvement, progressing from 97% in the first year to 99% in 2019 (R2: 0.9706; Figure 1).
During our 6-year period of activity, 4061 chest X-rays were performed, 2434 to control right inserted PICC, and 1618 to check on left side catheter. From September 2015 and following international guidelines,1,15 the authors maintained a post procedural chest X-ray only to check on left side insertions or in presence of patients with heart rhythm problems. In that way 8797 chest X-rays were economized over 12,858 PICCs inserted. A post procedural follow up strategy was designed to evaluate any possible complication in accordance with regional health agency guidelines. A complications report form was collected at D8 (Table 1).
The authors considered the three most common complications associated with PICC insertion: local infection defined as a positive culture of the PICC segment (⩾103 CFU/ml) with pus emerging from the exit site, without general signs of sepsis and negative blood cultures, thrombosis defined as a thrombus diagnosed with ultrasonography and bloodstream bacterial infections defined as a positive blood culture; although only 31% of all inserted PICC had an appropriate follow-up at D8 linked to the lack of human resources (Table 1). In 2014 they established that only 4% of all placed catheters developed local infection within D8: that percentage, furthermore, decreased at 1% over the years (2019) (R2: 0.9694 ; Figure 2). At the beginning (2014) the catheter thrombosis percentage was at 0.9%, reducing to 0.3% in 2019 (R2: 0.5878; Figure 2). Finally, bloodstream infection as a result of PICC insertion was at 0.3% in 2014 and no cases were reported in 2019 (R2: 0.9813; Figure 2).
Discussion
Increasing demand for PICC placement and shortage of medical staff availability led to create a trained nurse-led team. The specific goal of the dedicated vascular team was to improve hospital efficiency and patients safety, to decrease patients waiting list, to harmonize guidelines and protocols, and finally to promote the appropriate venous access for the right patient, according to his clinical situation. After the training period, once all skills had been acquired, nurses were generally satisfied with their role. 14 Since 2016, the total number of inserted PICCs began to decrease. This descending trend was justified by the introduction of new vascular equipment (TIVAPs, Midline, Broviac) that was meant to replace PICCs, following specific and precise clinical indications. According to the authors’ experience a well-trained nurse was able to perform a PICC insertion within 10 min, with a successful one puncture rate up to 89%. Procedural pain was evaluated mild in 96% of patients, using visual analog scale (VAS ⩽ 3): this is a valid instrument in measuring the procedural pain and an index of successful patient management.
This satisfactory performance was achieved using ultrasound and needle guide to minimize multiple punctures, which proved to correlate to more post procedural complications such as arterial punctures (0.1%; 18/12,687). As previously mentioned, these skills were rapidly acquired but in order to be maintained they needed the continuous practice that only a large, dedicated center with more than 1000 central catheters per year could provide.1,23,24 There have been a number of small studies supporting the role of nursing staff inserting VADs as an organizational solution, resulting in increased efficiency, reduction of cost, and improved clinical care.9,10
In addition to the obvious improvement of patients procedural experience, another important aspect correlated to the excellent performance of well trained nurses which resulted, therefore, in a significant decrease in the intervention of mentors. Although initially solicited (with an average of 6 calls/month), by the end of their training, and after a few months of practice, the mentor received an average of only to two monthly calls, a clear expression of total autonomy on behalf of a trained nurse, and consequently, the opportunity to free up valuable medical time.
The creation of a dedicated catheter insertion service run by both medical and nursing staff, improved overall patient care and satisfaction1–8,13,14,25,26 without exposing them to increased risk of complications. 12 In addition, to further minimize the risk of procedural problems each prescription was re-evaluated by both trained nurse and mentor. They assessed: the nature and duration of the treatment, any thrombosis or venous stenosis documented by a previous ultrasound scan or CT scan, and the presence of altered blood values (neutropenia, platelets, coagulopathies). If a contraindication was found, the prescription was discussed again with the prescribing doctor and possibly changed. Normally the waiting list never exceeded 24–48 h, as each day either one or two time slots were dedicated to emergency cases. Yacopetti et al., 3 Alexandrou et al.,4,11 Sainathan et al., 28 and Krein et al. 12 demonstrated that all PICC inserted by well trained nurses had the same or even less amount of complications than the catheters placed by medical staff. In any case the number of complications lowered considerably by using ultrasound and ECG-based guidance for tip position. Current evidence suggested that the ECG based method (intracavitary ECG with or without electromagnetic guidance) was a safe and simple procedure with high success rates to track the catheter insertion, to assess, and correct tip position15,16,18–21,29,30 This equipment minimized the need of radiological post procedural chest X-rays: finally they were still only performed for left-side insertions and to patients without P-wave. This conduct helped economize the use and cost of radiological procedures and most of all it minimized patient X-rays exposure.15–21,27,29–31
Another important and expected result was to successfully reduce the risk of procedural complications such as local infections, thrombosis, and bloodstream bacterial infections.
Limits
The principal limits of our study consisted in the underestimation of the resources needed to follow up patients. In fact, due to staff shortages, patient monitoring at D8 was actually very difficult to perform. This problem could, however, be solved with a more active collaboration of the prescribing team or the use of dedicated software or both. The lost patients rate at D8 was important (41% 2014, 56% 2015, 66% 2016, 72% 2017, 80% 2019), Table 1. The year 2020 was not considered as consequence of the COVID-19 pandemic crisis and therefore the necessity of turning most of the competences of hospital nursing staff to other more critical tasks.
Conclusion
Considering 6 years of experience, the benefits from a dedicated vascular access unit were multiple and relevant both in terms of efficiency and productivity. These concepts improved new forms of collaboration between professionals of the healthcare delivery system. The creation of protocols and guidelines helped to standardize and secure procedures, equipment support, and intense training being helpful for the improvement of patient outcome and satisfaction. Entrusting patients to trained nurses represented a gainful strategy in reducing patients waiting lists in a completely safe way, to cut financial costs, and to improve the efficiency of the vascular access service (more than 1000 requests of VADs a year). In France delegation of duty from doctors to nurses is still a possible process, although submitted to strict laws, in order to optimize hospital resources. In light of these findings, the authors encourage and promote the creation of vascular access units all over France.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
According to the French laws about retrospective study, the local Ethical Committee was not solicited.