
Abstract
Background:
Catheter implantation techniques for peritoneal dialysis (PD) have advanced significantly in recent years. We aimed to analyze the survival and associated complications of catheters inserted using a new technique that is guided by ultrasound and fluoroscopy and requires minimal tissue dissection. The procedure was performed by nephrologists in the outpatient basis, we compared these results of the minimally invasive insertion with traditional implantation using trocars.
Methods:
A total of 152 PD catheters were placed in 152 patients with stage 5 chronic kidney disease; 62.5% of the patients were men, with a mean age of 56.6 ± 18.5 years. The following two methods were used: minimally invasive insertion (MI group, n = 73) and trocar insertion (T group, n = 79). Patients in both the groups were followed prospectively for 26 months from the date of the first implantation.
Results:
Gender, age, and prevalence of diabetes mellitus were not significantly different between the groups, while the body mass index, presence of obesity, and abdominal scars from previous surgeries were higher in the MI group (p = 0.021). The incidence of catheter dysfunction was lower in the MI group compared to group T (6.8% vs 20.3%; p = 0.019). Exit site infection was also lower with the new technique (4.1% vs. 18.9%; p = 0.005). Further, the cumulative incidence of peritonitis also reduced with MI (p = 0.034). Finally, the overall catheter survival at 1 year was 89%, which has been shown as higher in group MI (95% vs 82% in group T; p = 0.025).
Conclusion:
The MI technique for catheter insertion showed low complication rates and excellent catheter survival as compared to traditional implantation methods; thus, it may be an alternative method for PD catheter placement.
Keywords
Introduction
In peritoneal dialysis (PD), the success in achieving access to the abdominal cavity is crucial. This strengthens the confidence of the patient and assisting team in the modality; however, possible associated complications can make it permanently unachievable. Despite the high prevalence of PD among patients undergoing renal replacement therapy (RRT) in some countries around the world, according to the latest Brazilian census from the Brazilian Society of Nephrology only 6.8% of the patients undergoing renal replacement therapy (RRT) are on PD, which has not changed in the recent decades.1–3 The technical and logistical difficulties for peritoneal catheter implantation contribute to this low prevalence; however, the participation of nephrologists in this process can significantly affect the current scenario.4,5
In 2014, the authors of the present study compared traditional PD catheter implantation techniques and did not find significant differences in complications and catheter survival rates in 129 implantations surgically (minilaparotomy) or by nephrologists using trocar. 6 Notably, laparoscopic implants have the lowest rates of mechanical complications among the existing methods7–9; however, the open surgical technique remains the most used method for catheter insertion despite recent improvements in laparoscopic implants. 10 This is mainly attributable to nephrologists’ inadequate training in performing peritoneal access as well as the unavailability of advanced techniques in many institutions. 11 Moreover, in a recent guideline, the International Society of Peritoneal Dialysis recommended the use of ultrasonography and fluoroscopy as an auxiliary tool to promote the success and safety of these procedures. 12
These considerations encouraged the authors to adopt a peritoneal catheter implantation method performed by nephrologists in an outpatient setting, which was guided by ultrasonography and fluoroscopy and accompanied with low costs and a high level of patient safety and potential reproducibility. This study aimed to analyze the related complication rates and survival of catheters inserted using this new approach, in comparison with those of more traditional catheter insertion techniques.
Methods
The present study was a clinical, comparative, and longitudinal study approved by the local Research Ethics Committee, under No. 3,629,353, issued October 8th, 2019. The data was collected prospectively and recorded in electronic medical records (DialSist®, Pro Renal, Brazil) was retrospectively analyzed.
Study population
From August 2018 to February 2020, the authors implanted peritoneal catheters in 73 patients with stage 5 chronic kidney disease (CKD) undergoing dialysis by using a minimally invasive image-guided percutaneous technique (group MI). These procedures were compared to the database of a study previously published by the authors, 6 which consisted of 79 implantations performed by trocar between June 2006 and June 2008 (group T). Patients older than 14 years of age, with a previous diagnosis of end stage CKD, and referred to this health unit by their nephrologists were included. Further, these patients should have chosen PD as the option to start on RRT to be included in the study. The exclusion criteria were the presence of abdominal wall hernias. For both the groups, all the procedures were performed by the same group of nephrologists. Table 1 shows the patients’ clinical characteristics.
Characteristics of the study population.
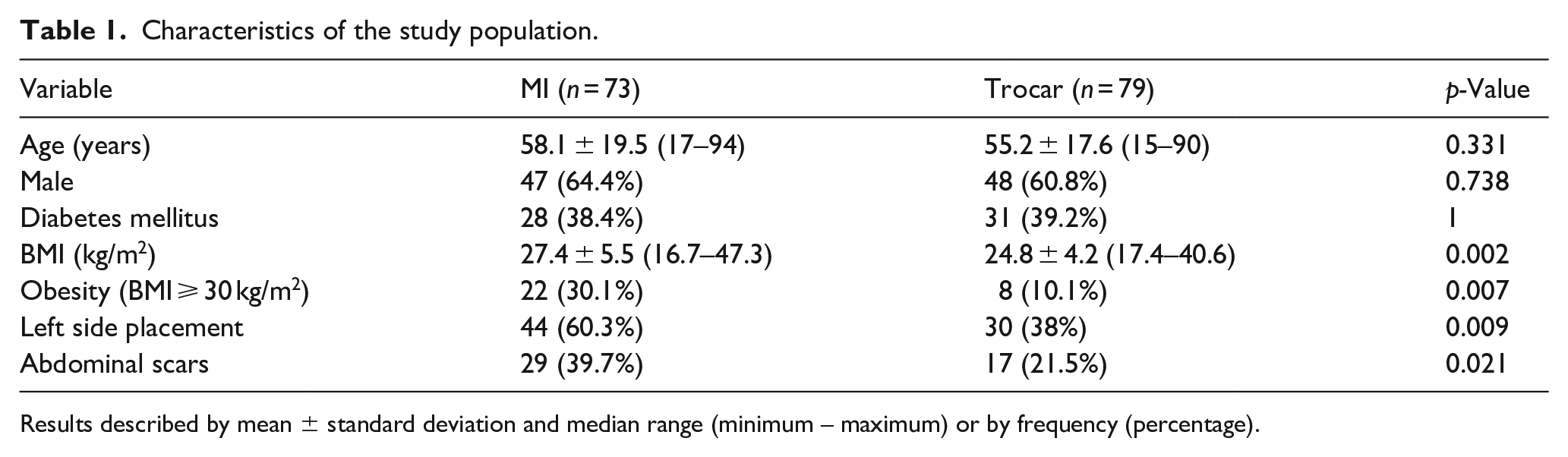
Results described by mean ± standard deviation and median range (minimum – maximum) or by frequency (percentage).
A total of 152 peritoneal catheters were implanted in 152 patients. Eight patients were excluded, three from group MI and five from group T. The main etiologies for CKD were diabetic nephropathy in 55 patients (36.2%), hypertensive nephrosclerosis in 40 (26.3%), chronic glomerulonephritis in 30 (19.7%), polycystic kidney disease in 6 (3.9%), uropathies in 6 (3.9%), ischemic kidney disease in 4 (2.6%), and other causes in 11 (7.2%) patients.
Catheter insertion techniques
In the MI group, the procedures were performed in an outpatient setting, with an observation period of up to 2 h after implantation. In this group, Argyle® installation kits with 42 cm double-cuff straight catheters were used; thus, the subcutaneous tunnel was made in the cranial and lateral directions due to the catheter’s shape. All the procedures were performed using real-time ultrasound and fluoroscopy, with a minimally invasive technique devised by the authors as follows (Figure 1):
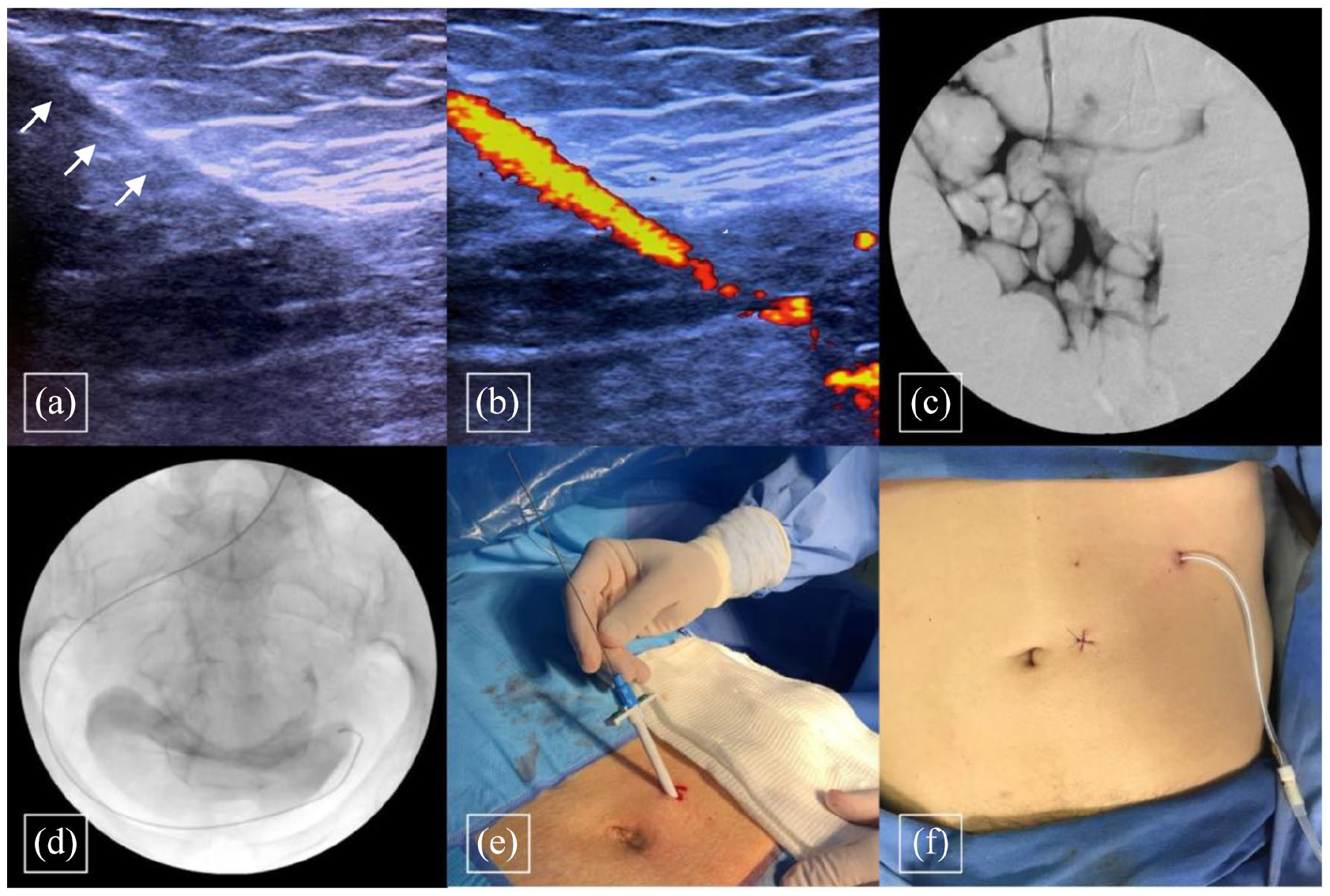
Main steps of the minimally invasive technique: (a) anesthesia of the rectus abdominis muscle and puncture of the peritoneal cavity, (b) use of power Doppler to confirm access to the cavity, (c) injection of 10 ml of iodinated contrast, and (d) passage of Teflon guide wire, and (e) Sheath introduced; (f) Result.
Under sedation and local anesthesia, a small paraumbilical incision of up to 1 cm in length was made, which was followed by the administration of rectus muscle anesthesia under ultrasound and puncture of the peritoneal cavity with a 14G-caliber venous catheter. Subsequently, the needle was removed, and the catheter was kept in the intracavitary position. The needle’s angle during peritoneal puncture varied according to the thickness of the abdominal wall, with larger angles being applied in more obese patients to ensure that the peritoneal cavity would be reached. Then, 0.9% saline solution was infused under visualization with Power Doppler, ensuring free flow into the cavity. The next step was the injection of 10 ml of iodinated contrast through the catheter under fluoroscopy, with free spreading in the peritoneum. After securing access to the peritoneum, the passage of the Teflon guidewire and the introducer sheath were carried out, with subsequent introduction of the catheter, and creation of the exit site and tunneling. Finally, the small incision made for the puncture and passage of the catheter was sutured with a simple stitch using a 3.0 mononylon thread.
In group T implants, all the procedures were performed in an inpatient setting, with a 24 h stay in hospital after implantation. For these patients, only Kendall® 42-cm double-cuff pre-curved catheters were used; thus, in this group, the subcutaneous tunnel was made in the caudal and lateral directions. These procedures were performed using trocar, according to the technique described by Ash and Daugirdas 13 that is briefly illustrated below (Figure 2):
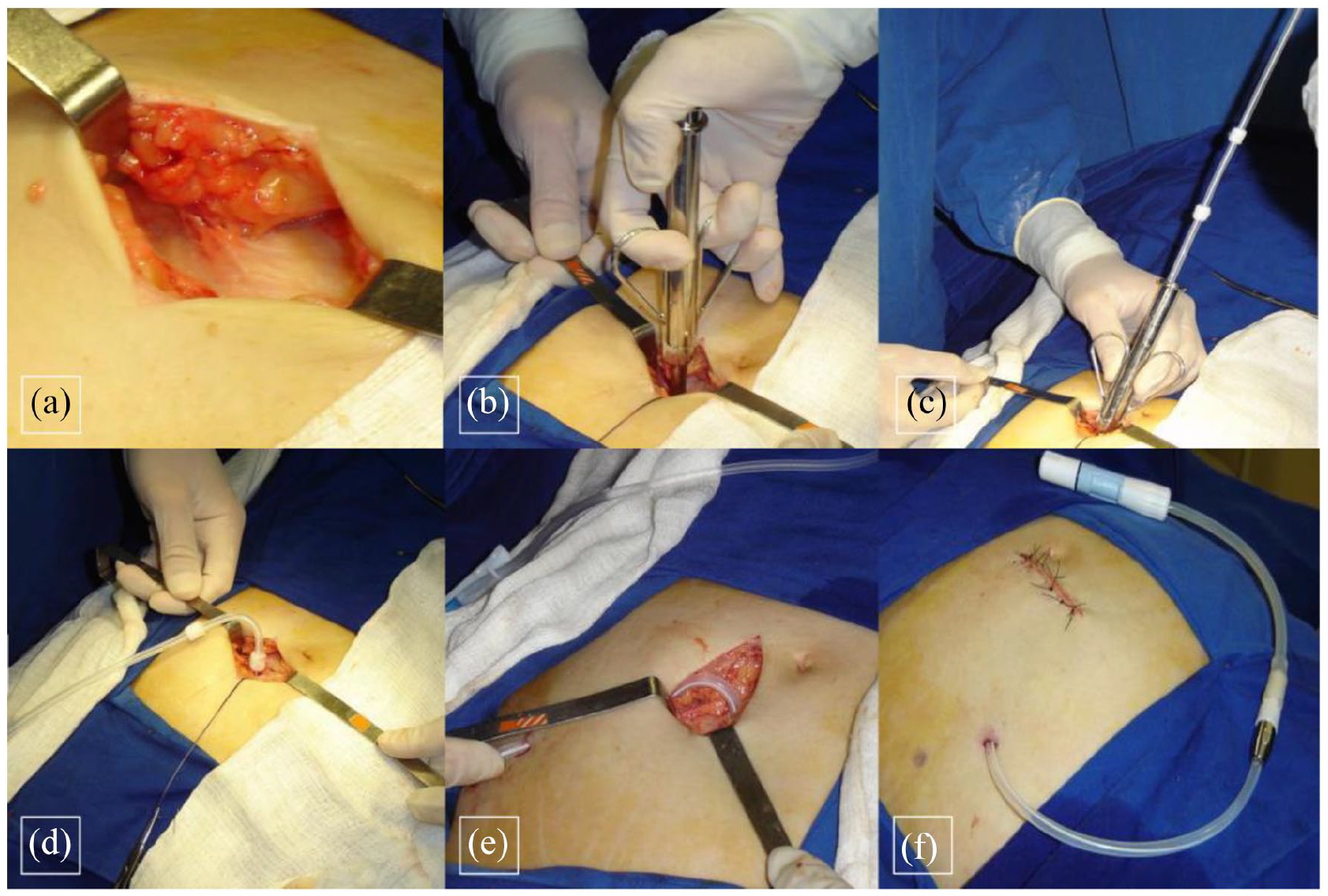
Main steps of the trocar technique: (a) incision and dissection of the subcutaneous tissue until the aponeurosis was reached, (b) puncture of the peritoneal cavity with a trocar, (c) catheter introduction, (d) catheter in the peritoneal cavity, (e) subcutaneous tunneling, and (f) result.
Routinely, in both the groups, the side of the implantation was chosen by the patients. Nonetheless, in cases with abdominal scars, the flank with no previous surgical interventions (or the less manipulated side) was chosen. During the postoperative period, the first dressing was changed 24 h after the catheter insertion. Mupirocin ointment was used at the exit site in all the subsequent dressings. For both the methods, the break-in period was 2 weeks.
Clinical outcomes
The primary outcomes were the presence of mechanical and infectious catheter complications. The mechanical complications analyzed were catheter dysfunction requiring further catheter manipulation in the operating room, peritoneal or surgical wound bleeding, dialysate leakage, cuff extrusion, and viscera perforation. Catheter dysfunction was defined as the occurrence of infusion or drainage of less than 500 ml of dialysis solution within 5 min. 6 All cases of catheter dysfunction were submitted to abdominal radiograph, to verify tip catheter position inside the abdominal cavity. Surgical wound infections, subcutaneous tunnel or exit site infections, and peritonitis were considered as infectious complications. The infectious complications were classified as early, if the complications occurred in the first 30 days after catheter implantation, or late, if they occurred after 30 days. 11
The secondary outcome was catheter survival and patency. Cumulative catheter survival was defined as the time from insertion until its removal for any reason, or the censoring or end of the follow-up period. The causes for censoring were death, renal transplantation, transfer to hemodialysis or to another center, and partial recovery of renal function with the suspension of dialysis. In both groups, the total follow-up period was 26 months from the date of the first implantation with a median follow-up of 380 days (19–758) in the MI group as compared to 206 days (14–788) in the T group. For the MI group, the follow-up was completed in October 2020, while in the T group it was completed in September 2008.
Statistical analysis
The results obtained in the study were described by means (standard deviations) and medians (range) for quantitative variables, and by frequencies and percentages for categorical variables. A comparison of the two groups in relation to the quantitative variables was performed using the Student’s t test for independent samples. The categorical variables were analyzed using the Fisher’s exact test or the Chi-square test. To assess the factors associated with peritonitis free time and dysfunction free time, Fine and Gray models were adjusted, considering the competitive risks of death with the catheter patency, renal transplantation, therapy change, and a partial recovery of the glomerular filtration rate with a discontinuation of dialysis. The estimated measure of association was the sub-distribution hazard ratio (SHR), with a 95% confidence interval (CI). Logistic regression models were adjusted, and the Wald test was used for the analysis of mechanical and infectious complications. The estimated measure of association was the odds ratio with a 95% CI. The Kaplan–Meier method was used for catheter survival analysis. Statistical significance was indicated by a p-value < 0.05. The data was analyzed using Stata/SE v.14.1 Stata Corp LP, USA.
Results
Figure 3 shows the main complications observed in both the groups. The success rate of the new technique was 98.6%, as, in group MI, one patient did not undergo catheter implantation, with the need for conversion to minilaparotomy.
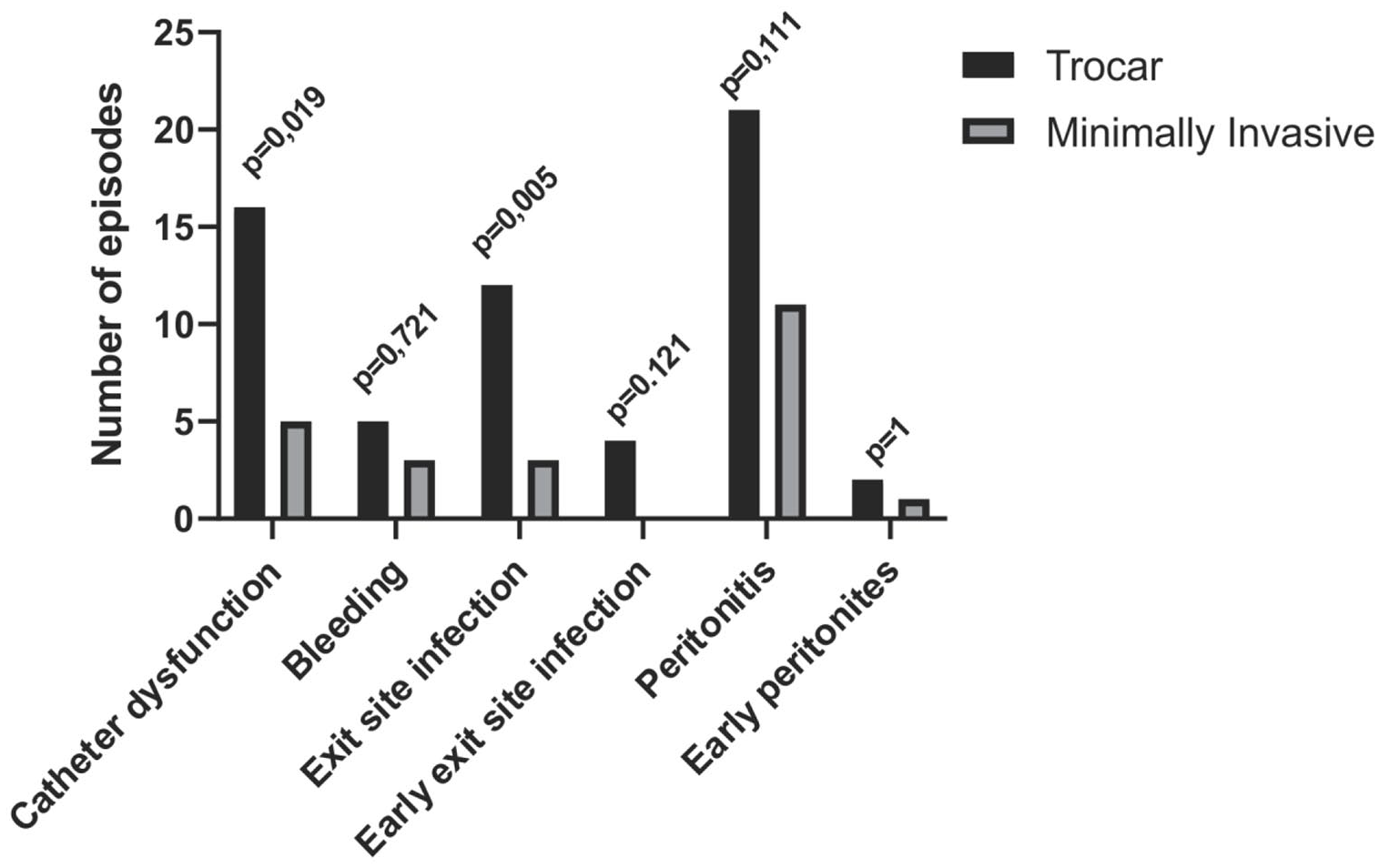
Mechanical and infectious complications.
Mechanical complications
The most common mechanical complication in both the groups was catheter dysfunction, which was observed in five patients in the MI group (6.8%) and 16 (20.3%) in the T group (p = 0019). The cumulative incidence of dysfunction also favored the MI technique (Figure 4(a)). The radiographic images showed that the catheter was displaced in all cases of dysfunction. For catheter repositioning in patients from the MI group, a rigid guide wire was used with no need for a new incision. In group T, all the patients with dysfunction needed a new incision, followed by repositioning using a rigid guide wire in virtue of the subcutaneous tunnel conformation. The cases of catheter dysfunction were successfully corrected in five (100%) patients in the MI group and 13 (81.2%) patients in the T group (p = 0.549). Table 2 shows the potential variables associated with this complication.
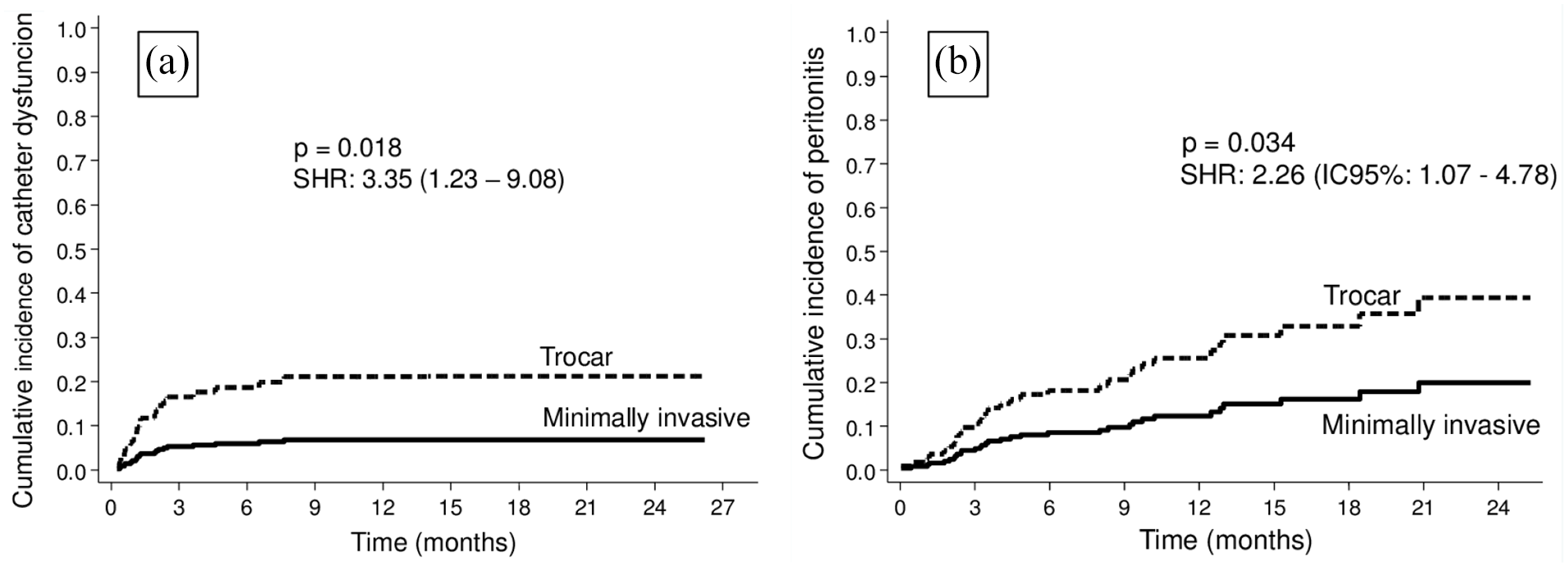
The cumulative incidence of catheter dysfunction (a) and peritonitis (b).
Analysis of catheter dysfunction.
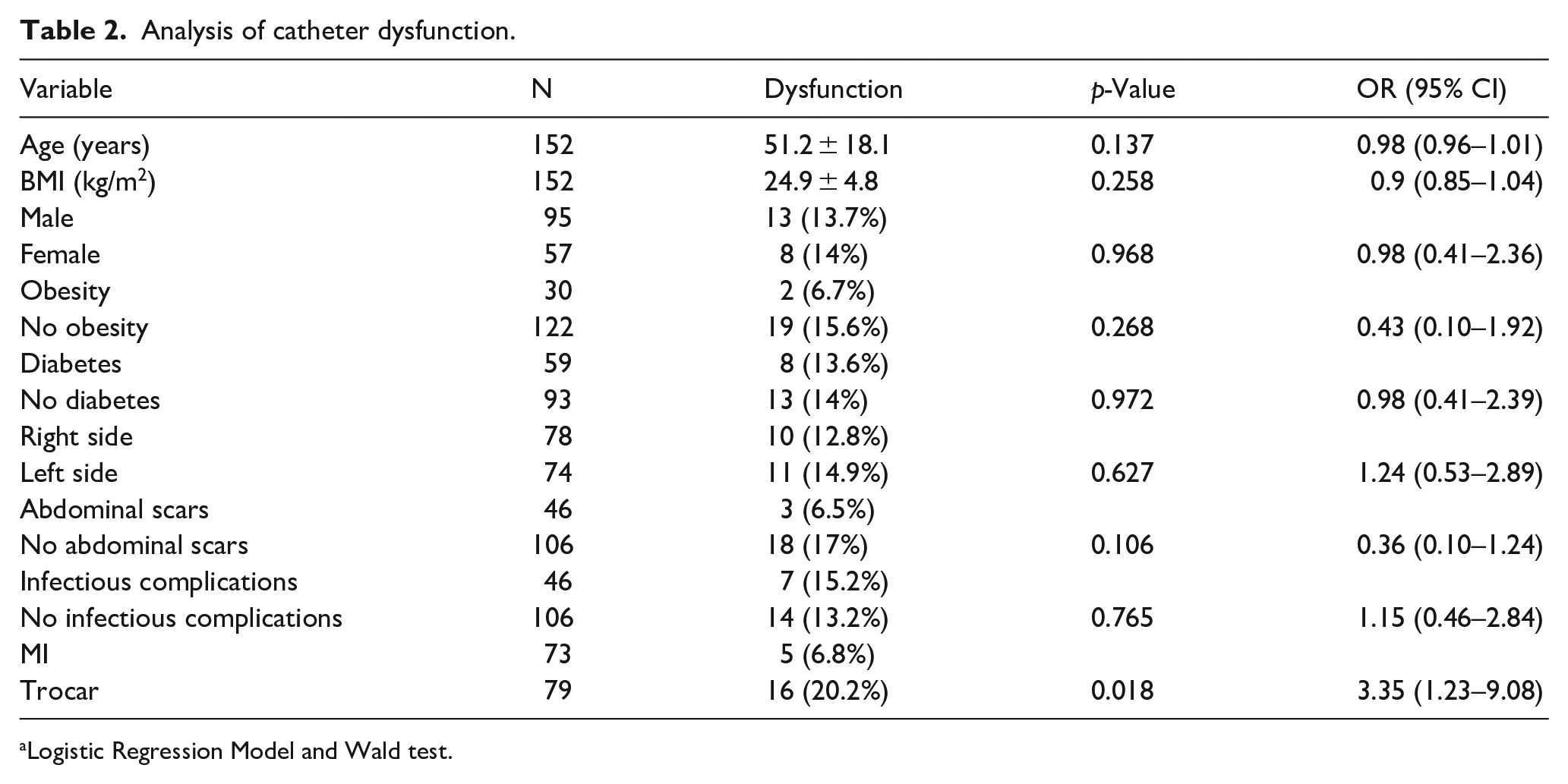
Logistic Regression Model and Wald test.
No bleeding event was severe, with no need of a new surgical intervention, hospitalization, or blood transfusion. Moreover, extrusion of the external cuff occurred in only one patient in the MI group. In the present study, no cases of viscera perforation, suture dehiscence, incisional hernia, or dialysate leakage were observed.
Infectious complications
All the 152 included patients did not present any cases of surgical wound or subcutaneous tunnel infection. The overall incidence of exit site infection was significantly lower in minimally invasive procedures (group MI: 4.1% vs group T: 18.9%), as seen in Figure 3. The comparison of the cumulative incidence of peritonitis demonstrated a significantly lower value in the minimally invasive implants, as shown in Figure 4(b). Regarding the time interval between implantation and the first episode of peritonitis, in group MI, the mean interval was 5.3 ± 5.1 months (median 2.3 months; 0–13 months), while in group T, it was 6.8 ± 5.7 months (median 4.4 months; 0.4–20.8 months) [p = 0.034; SHR 2.26; 95% CI 1.07–4.78].
No other variable showed a significant correlation with the occurrence of peritonitis, besides the catheter implantation technique (Table 3).
Analysis of peritonitis episodes.

Logistic Regression Model and Wald test.
Catheter follow-up
At the end of the follow-up period of 26 months, 46 (63%) patients in group MI and 49 (62%) patients in group T remained on PD (p = 1). The main causes for the discontinuation of dialysis were death (40.7% vs 43.3%; p = 1), peritonitis (18.5% vs 16.7%; p = 1), and renal transplantation (25.5% vs 6.7%; p = 0.070). The other causes were transference to hemodialysis for non-catheter-related causes (4.3% vs 13.3%; p = 0.673), partial recovery of the renal function with the suspension of dialysis (one case in group MI and two cases in group T), and a change of dialysis center with a loss of follow-up (only one case, in group MI). Of the 152 patients included, only four patients stopped PD due to catheter dysfunction, and all of them belonged to group T (p = 0.114). The overall catheter survival rate at 1 year was 89%. For minimally invasive implantation, the survival rate was 95% and 82% with trocar implantation (p = 0.025).
Discussion
This study demonstrated the results of PD catheter insertions performed by nephrologists in an outpatient setting. Herein, we introduced a minimally invasive technique guided by ultrasonography and fluoroscopy, with a success rate of 98.6%. The cumulative incidences of mechanical and infectious complications were low, and excellent survival of the catheters was verified, suggesting that this intervention might be a highly feasible alternative in PD catheter implantations. Furthermore, the higher rate of success observed in obese patients and those who had undergone abdominal surgeries in the past increased the robustness of our results. In a very recent publication, Swinnen et al. also demonstrated satisfactory results using a technique similar to the one presented in the current study. 14
The use of ultrasonography in the planning and execution of peritoneal access allows the identification of vessels in the puncture trajectory and offers the possibility of determining the depth of the abdominal cavity and identification of signs that are suggestive of intracavitary adhesions. 15 In the present study, obesity and peritoneal depth were not limiting factors for using a minimally invasive technique. In addition to assisting in the preoperative evaluation, real-time ultrasonography allowed anesthesia induction in the rectus muscle and securely guided the puncture of the peritoneal cavity. Moreover, fluoroscopy is an important tool for peritoneal access. Essentially, two studies published in the last decade have demonstrated high success rates and reported a lower incidence of mechanical complications in cohorts that used fluoroscopy during catheter placement.16,17 Nonetheless, in these studies, the procedures were not performed exclusively in an outpatient setting or by nephrologists. Further, they were different from the technique presented here. In a recent study by Swinnen et al., 14 the authors outline the important clinical details that are essential for the success of the implantation and functionality of the catheter. Care with peritoneal puncture angulation and catheter entry into the abdominal cavity, among other essential steps, can be reproduced easily and guarantee excellent results, even in patients with an urgent onset of PD. However, this that was not tested in the present study, but the authors believes that is perfectly feasible.
The incidence of mechanical complications in peritoneal access varies substantially in the extant literature. Catheter dysfunction is a mechanical complication that should be highlighted, as it can cause early failure in the dialysis method. The incidence of mechanical complications is significantly heterogeneous in the current literature, ranging from 1.5% to 34.7%.18–21 In the present study, the satisfactory dysfunction rate was 6.8% in patients who underwent minimally invasive implantations. Similarly, the 100% success rate of catheter function recovery obtained by repositioning suggests that the described technique is even more promising. The authors believe that the use of fluoroscopy may significantly lower the rate of cases with dysfunction, thus providing an effective tool for solving this complication simply and safely without the need for new surgical interventions.
Nevertheless, other mechanical complications, such as significant bleeding episodes (not observed in the present study) have been reported by other authors, with incidence rates ranging from 0.7% to 9%.22–24 We could hypothesize that minor trauma of the rectus muscle and the consequent reduction of tissue damage may explain these positive results. On the contrary, the dialysate leakage has been directly related to the implantation technique and the interval between catheter insertion and beginning of PD.25,26 Considering the equal break-in period in the entire cohort and the technique used in group MI, with maintenance of both the cuffs in the subcutaneous tissue, the insertion of the internal cuff within the rectus muscle does not seem necessary, despite being recommended previously.27–29 Furthermore, no case of perforation was observed with the 152 catheters inserted. The authors believe that the use of ultrasonography to guide the percutaneous puncture of the cavity might reduce this complication to negligible levels.
With regards to infectious complications, early infections related to peritoneal access may occur in up to 5% of the patients. 30 Although obesity is considered a risk factor, 31 our results could not confirm this finding. As expected, peritonitis was the main infectious complication in both the groups, with an overall incidence of 0.32 cases per year of risk (0.22 cases in group MI and 0.47 in group T). These results are in accordance with the current recommendations.32–35 A meta-analysis published in 2015 showed no differences in the catheter survival after 1 year of implantation or in the mechanical complication rates among 2681 percutaneous and surgical implants, as reported by the author. Nonetheless, lower incidences of peritonitis in patients with percutaneous implants were also reported. 36 Thus, reducing the tissue dissection area could contribute to a significantly lower incidence of infectious complications. Interestingly, in the present study, the time interval between catheter implantation and the first episode of peritonitis was significantly shorter in minimally invasive implantations. The low incidence of peritonitis in these patients (11 cases in total) could have contributed to this result, which requires further analysis.
According to several reports, the expected goal for survival of peritoneal catheters 1 year after their insertion is >80% for conventional methods and >95% for advanced laparoscopic procedures. 12 Compared to conventional methods, we obtained better and more significant results in our cohort, which reinforced our confidence in the present technique, and, in this context, the authors consider that the experience of the assistant team is essential to guarantee satisfactory results not only in the short but also in the long term. Although obese patients with a BMI of up to 47.3 kg/m2 and those with abdominal scars were included, they did not present significant differences in catheter survival rates, which demonstrated that these conditions were not contraindications of inclusion in PD programs. Similar data was reported by other authors.37,38
Finally, the MI technique is cost-effective, which provides an added advantage. Procedures performed in an outpatient setting can help reduce over 50% of the related costs, 39 whereas percutaneous methods can reduce the expenses with PD catheter implantation up to 4.8 times. 40 Moreover, despite the need for the operator to have basic knowledge of the handling tools, such as ultrasound and fluoroscopy, the authors believe that the technique described can be used in most of the patients. It is also relevant to highlight that the establishment of interventional nephrology centers can provide opportunities for training new nephrologists in performing the MI technique, considering its easy reproducibility, or even conventional techniques, such as open surgical techniques, which are the most used worldwide. Nevertheless, it is important to note that the ideal implantation method may not exist, and the method used must be customized according to the characteristics of each patient.
This study has some limitations. First, it is a retrospective comparative study with a historical cohort, with a significant time interval between the procedures performed in each group. Nevertheless, all the procedures were performed by the same team of nephrologists, with a prospective recording of the outcomes, and the use of a consolidated database eliminated the risk of information loss. Second, ethical issues regarding the use of techniques that the authors recognize as inferior in randomized studies must be observed. Third, at the time of trocar implants, the authors had extensive experience with this procedure, whereas the first 73 cases performed with the new technique were included in the minimally invasive implant group; this further corroborates the importance of the superior results obtained with this technique. Finally, although the groups used different catheter models; consequently, the direction of the exit site in relation to the insertion point in the cavity was also different. However, the authors observed that the evidence demonstrated no superiority between the catheter models used in the two groups studied, 12 corroborating the relevance of the results obtained.
Conclusion
The presented technique highlighted lower complication rates and excellent catheter survival and may be a highly effective and safe alternative for PD catheter implantation by nephrologists. Likewise, the possibility of performing these procedures in an outpatient setting, accompanies with substantial cost reduction as compared to advanced surgical methods makes the method even more attractive and a very feasible alternative to the traditional techniques of PD catheter placement.
Footnotes
Acknowledgements
The authors would like to thank Pro Renal Brazil for all the support for this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.