
Abstract
Background:
Early cannulation arteriovenous grafts (ecAVG) for dialysis access are limited by reintervention for venous stenosis (VS) despite their good initial patency. Whilst stent-grafts (SG) have shown promise, the optimal sizing is unclear. Therefore, this study aims to determine if outflow vein diameter, SG diameter or these relative to each other (V:Sr) alters outcomes, and if so, which is more important.
Methods:
Retrospective analysis was performed of Gore® Acuseal® ecAVGs with VS treated with Gore® Viabahn® SG over a 7-year period. Primary patency (PP), time to thrombosis and functional patency were analysed by SG length/diameter, vein diameter and V:Sr.
Results:
We identified 114 ecAVGs with median follow-up 492 days (IQR 189–770). SG length and diameter did not correlate with PP, however, there was a significant relationship between vein diameter and PP (RR = 0.901 (0.832–0.975), p = 0.01) and between V:Sr and PP (RR = 0.462 (0.255–0.838), x2 = 5.866, p = 0.0015). The optimal V:Sr was ⩾1.4 (i.e. vein diameter at least 40% greater than the stent-graft; or ‘free-floating’ stent outflow) (RR = 2.759 (1.670–4.558), p < 0.001), translating to a difference in median PP of 252 versus 496 days (IQR: 188–316; 322–670). On multivariate analysis, absolute vein diameter lost significance, whilst V:Sr remained an independently significant predictor of PP (RR = 3.247 (1.560–6.759), p = 0.02).
Conclusions:
Placement of the SG outflow into a relatively larger segment of vein was associated with a significant increase in PP independent of the absolute vein diameter. This suggests that larger calibre SG which are apposed to the vein wall are not required for optimal primary patency, and indeed should be actively avoided. Instead, a ‘free-floating’ stent outflow which is undersized relative to the recipient vein (whilst maintaining a minimum anchoring calibre) is recommended where possible. This should be considered during intervention and may require selection of longer devices, where practical, to bring the stent outflow into a larger vein segment.
Level of Evidence:
Level 3a, Non-randomised controlled cohort/follow-up study
Keywords
Introduction
Vascular access remains a leading cause of morbidity and costs for patients with end-stage renal failure requiring haemodialysis. A major limitation of the wider use of early cannulation arteriovenous grafts (ecAVG) is the rate of re-intervention for venous stenosis (VS), with up to 50% requiring intervention at 1-year. 1 VS itself is the leading cause of thrombosis, which in turn is associated with poorer long-term patency. Thus, effective intervention for VS is a key target for improving patient outcomes and reducing costs of vascular access provision. 1
The number and type of treatments available for VS has increased over the past decade with older treatments such as surgical revision and bare-metal stents largely replaced by newer percutaneous techniques. The two current options involve either pharmacological treatment with drug-eluting balloon angioplasty (DEB) or mechanical methods to prevent recurrent stenosis such as stent-grafts (SG). Whilst the data on DEB in ecAVG is still increasing, there is a reasonable body of observational series and randomised trials to suggest that SG are associated with better outcomes.1–4
The pathophysiological benefits of SG are four-fold 5 : firstly, the stenotic area is enlarged to improve flow volumes using a nitinol stent; secondly, ingrowth of neo-intimal hyperplasia is prevented by an ePTFE re-enforced lining; thirdly, the location of the ‘venous anastomosis’ is moved from the area of VS and neointimal hyperplasia to a larger non-impacted section of arterialised vein; fourthly, the flow dynamics at this level are improved with a laminar flow profile that is less likely to stimulate further stenosis. The optimal sizing of stent-grafts thus relies on effective anchoring in the ecAVG, effective lumen restoration and critically an optimal outflow location. This later aspect allows for user discretion to tailor both the diameter and length to match a perceived optimal diameter of the recipient vein.
Traditional arterial teaching is that a stent-graft should go from ‘normal to normal’ with a 10% oversizing and minimal length, 6 however it is uncertain if this rationale applies to arteriovenous circuitst. Although there is industry advice to anchor the device (at least 6 mm calibre SG) and sufficiently overlap into the ecAVG when treating juxta-anastomotic lesions, there is little objective data on the outcome (incidence of end-of stent stenosis) and how this relates to size matching of the SG to the outflow vein.
The aim of this study is therefore to determine the impact of SG sizing (both relative and absolute device diameter as well as device length) and the recipient vein diameter on outcome.
Materials and methods
A consecutive cohort of patients in whom a single type of SG (WL Gore® Viabahn®) was placed in a single type of ecAVG (WL Gore® Acuseal®) as the primary intervention for venous anastomotic stenosis was identified (January 2015–2022) from which data on demographics, interventions for venous stenosis, complications and outcomes were obtained using a prospective electronic patient record. Follow-up was complete for all patients who received a SG, and complete for all ecAVG other than two patients lost to follow-up 2 and 6- months following ecAVG insertion.
Routine monitoring of ecAVG using haemodialysis adequacy (clearances, pressures and flow) was supplemented with surveillance offered to all patients 3-monthly with urgent interval imaging performed for symptoms. Weekly multi-disciplinary team meetings (MDTM) that included vascular access nurses, radiologists, surgeons and nephrologists reviewed the previous week’s imaging. VS were treated if >75%, recurrent, associated with clinical concerns, or had progressed since previous imaging. The treatment of VS was at the discretion of the interventional radiologist and if of uncertain clinical significance, deferred for MDTM discussion.
Patency was based on published European Guidelines: primary patency being either the interval to the first re-intervention (intervention-free survival) for dysfunction or thrombosis, the interval to the time when patency is measured or the interval to abandonment. Functional patency was defined as the interval to abandonment or achievement of a censored event (death, elective change of modality, loss of follow-up). 7
Stent-graft insertion was performed under the care of a Consultant Interventional Radiologist (total of 10 working in our department). Decisions made regarding the calibre, length and position of device were determined on an individual basis by best clinical judgement. Standard percutaneous access and angiography techniques were used including 0.035″ platform devices (Medtronic Admiral Xtreme Balloon Catheter, WL Gore Viabahn Endoprosthesis). Following deployment, the device was post dilated to nominal diameter using an appropriate balloon to ensure adequate apposition to the ecAVG.
Diameter measurements were obtained by retrospective review of digital subtraction angiography (DSA) images (Toshiba Infinix-i & Siemens Artis zee) of both the SG and outflow vein. Device length and diameter were recorded from the implant record. Calibration was achieved using known values including the ecAVG and SG diameters (these were only used when seen to be completely patent or an unrestrained stent in a larger vein). Measurements were performed by a consultant interventional radiologist and verified by sample cohort measurements performed independently by a second consultant interventional radiologist. SG relative sizing (vein:stent graft ratio–V:Sr) was ascertained by comparing the outflow vein measured diameter (defined as the diameter at the point of SG outflow regardless of the presence of any subsequent aneurysmal dilatations or central stenoses) to the measured diameter of the SG used. Thus, a 6 mm SG implanted into a 6 mm vein would have a ratio of 1.0, whereas a 6 mm SG implanted into an 8 mm outflow vein would have a ratio of 1.3 and a 6 mm SG implanted into a 10 mm vein would have a ratio of 1.7; that is, the larger the ratio, the larger the vein relative to the stent at the point of outflow.
Data analysis
Initially the relationship of primary patency from the time of SG implantation was examined for SG diameter, SG length, outflow vein diameter and the V:Sr . Given a significant relationship, the optimal V:Sr was determined by sequential splitting of the data. The outcome on patency and time to first thrombosis was then determined using this optimal V:Sr. A multivariate analysis including both vein diameter and V:Sr was then performed to determine the relative importance of these variables.
Statistical methods
The Kaplan-Meier method was used for categorical variables, and Cox proportional-hazards method for continuous variables.8,9 The validity of the proportional-hazards assumption was ensured by making an interaction of the variable with time, with the significance of the time-dependent variable (T-cov) calculated when included in a Cox model, with all variables showing proportionality. 10
The optimal V:Sr was determined by finding the greatest benefit on sequential splitting of the data and using a Cox proportional hazards model to detect the point at which there was the greatest difference in primary patency (measured as a relative risk (RR)) between the under- and over- sized groups.
There was no evidence of informative censoring as no patients with a SG were lost to follow-up. The log-rank test was used to test for significance. All p-values were derived from two-tailed tests with p < 0.05 considered statistically significant. Data were analysed using SPSS software (IBM SPSS Statistics, Version 27).
The study was registered with the appropriate regional committee – The Renal Services Clinical Effectiveness Group. Formal research ethics approval was not required due to the retrospective, observational study of established practice within accepted guidelines.
Results
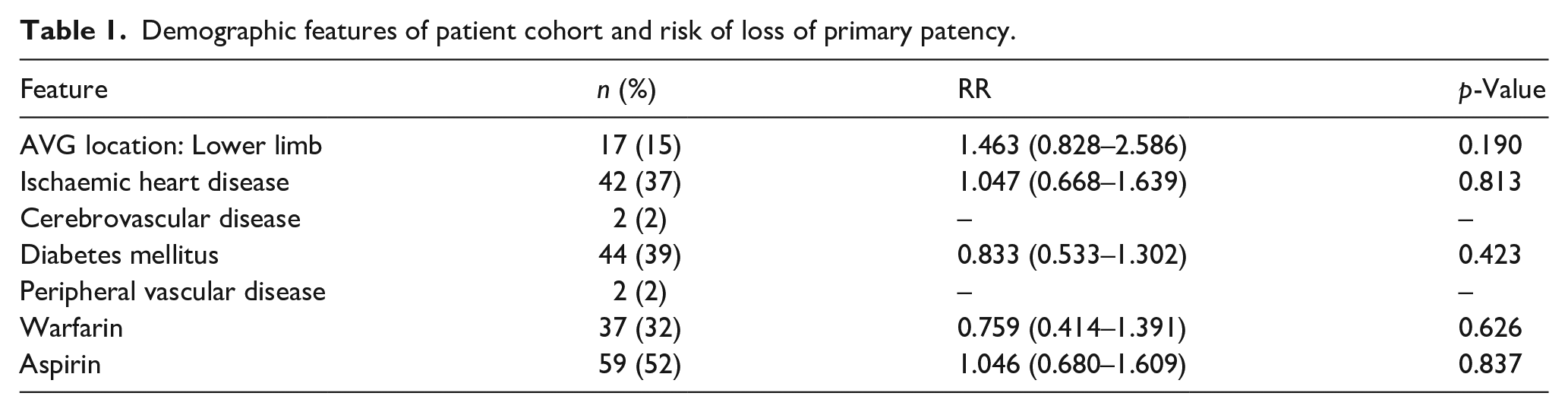
Over the 7-year time-period, 114 consecutive SGs were placed for venous stenosis, with a median follow-up after insertion of 492 days (IQR 189–770 days) and a total of 64,579 days exposure. Re-intervention was required in 86 patients with a median primary patency following SG insertion of 249 days (IQR 115–432 days). At the time of measuring patency, 31 remain in use (27%), 19 had a transplant with a functional ecAVG (16%), 21 patients died with a functioning ecAVG (18%) and 43 (39%) lost the ecAVG for varied reasons (thrombosis, infection, patient preference, change in modality, frailty and other comorbidity). Co-morbidity was common, but neither co-morbidity nor medication (anti-platelet or warfarin) was related to time to re-intervention (Table 1).
Demographic features of patient cohort and risk of loss of primary patency.
The most common diameter SG used was 7 mm (n = 67, 59%), followed by 8 mm (n = 26, 23%), 6 mm (n = 20, 18%) and 9 mm (n = 1, 1%) with all ecAVGs having an internal diameter of 6 mm. The length of SG used was predominantly 5 cm (n = 52, 46%) or 10 cm (n = 58, 51%) with 15 cm used in the rest (n = 4, 4%).
39% (n = 44) of SG employed were the same size or larger relative to the outflow vein (a V:Sr of 1.0 or less), with 61% (n = 70) being smaller relative to the outflow vein (V:Sr >1.0). The median V:Sr was 1.2 (IQR: 1–1.5) (Figure 1).
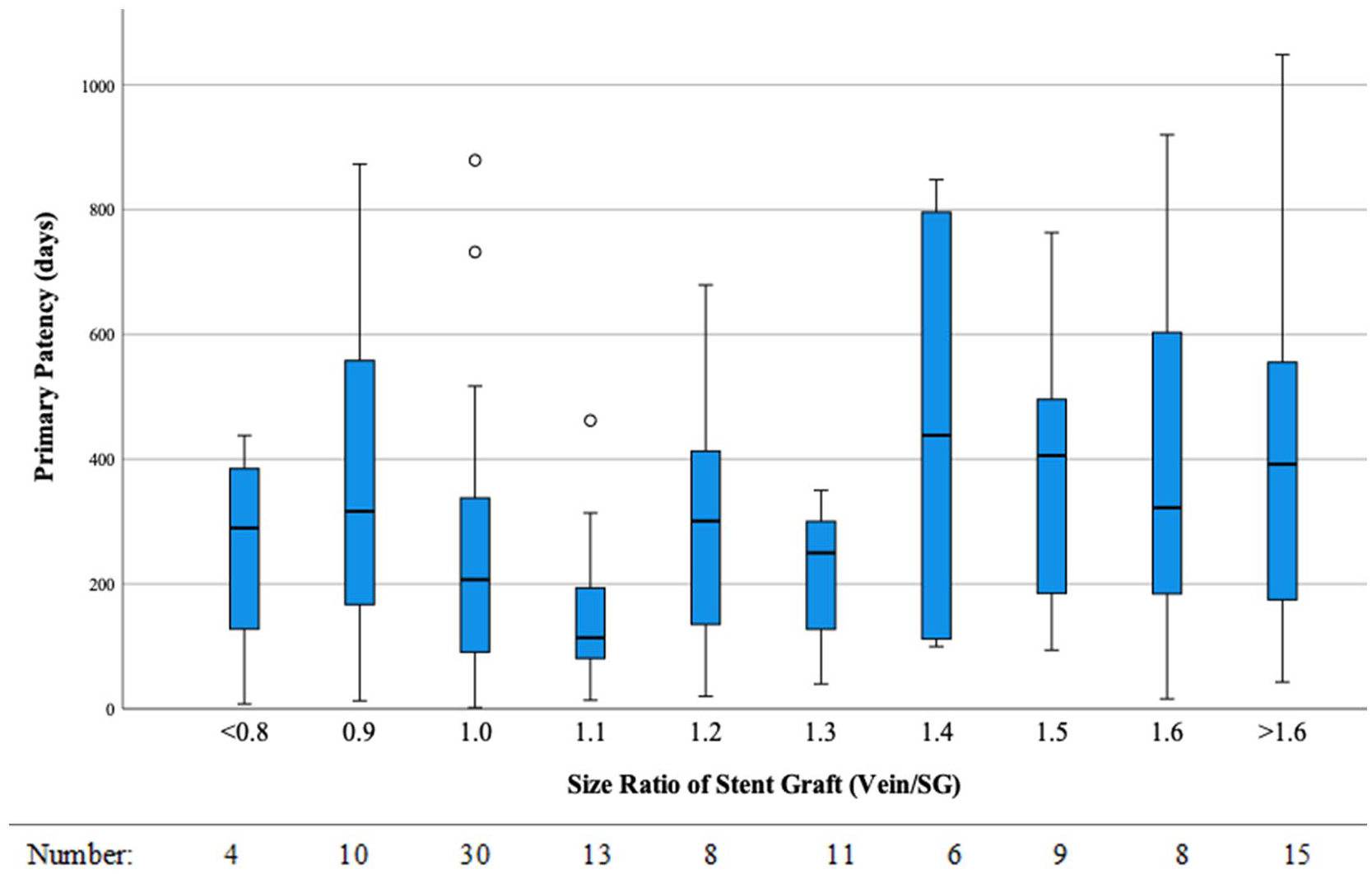
Vein:SG ratio (V:Sr) and primary patency.
SG length and SG diameter did not correlate with primary patency (x2 = 0.482, p = 0.786; x2 = 2.895, p = 0.408). However, both vein diameter and V:Sr were significantly associated with primary patency (Cox analysis with vein diameter analysed as a continuous variable: vein diameter – RR = 0.901, 0.832–0.975, p = 0.01; V:Sr – RR = 0.462; 0.255–0.838, x2 = 5.866, p = 0.0015).
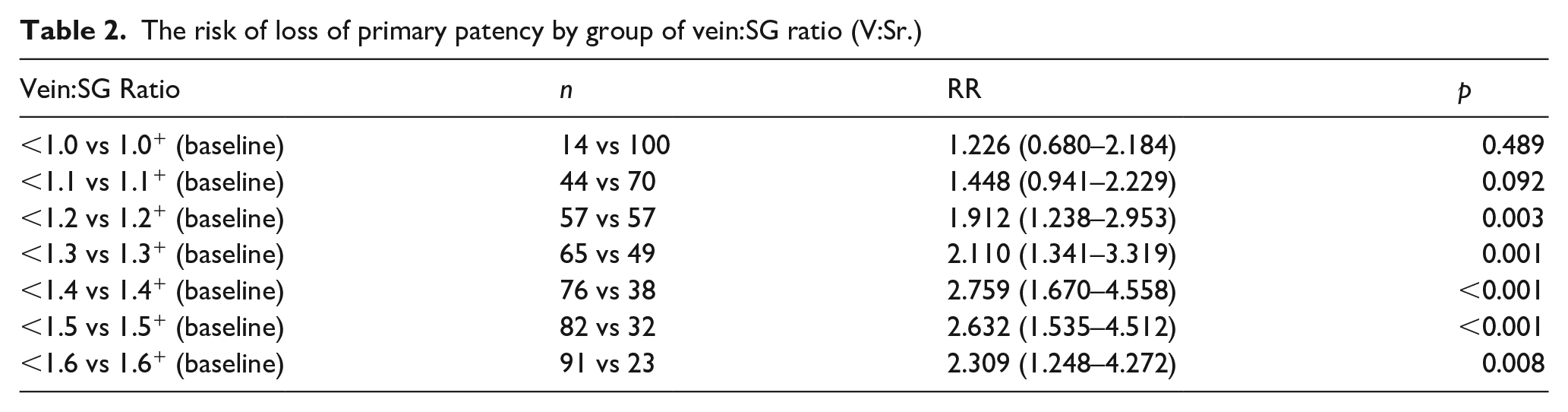
The optimal V:Sr was determined by sequentially splitting the cohort by V:Sr and calculating the impact on loss of primary patency using a Cox analysis (Table 2, Figure 2). The optimal V:Sr was 1.4, with a ratio of ⩾1.4 giving the largest impact on improved primary patency (RR = 2.759 (1.670–4.558), p < 0.001). Interestingly, increasing the V:Sr did not adversely affect the outcome. The median primary patency at V:Sr of <1.4 was 252 days (IQR: 188–316) versus 496 days (322–670) for V:Sr ⩾1.4 (x2 = 17.034, p < 0.001) (Figure 3). On multivariate analysis, the V:Sr remained significant (RR = 3.247 (1.560–6.759), p = 0.02) after allowing for absolute vein diameter as an independent variable, which lost significance (RR = 1.031 (0.937–1.134), p = 0.535).
The risk of loss of primary patency by group of vein:SG ratio (V:Sr.)
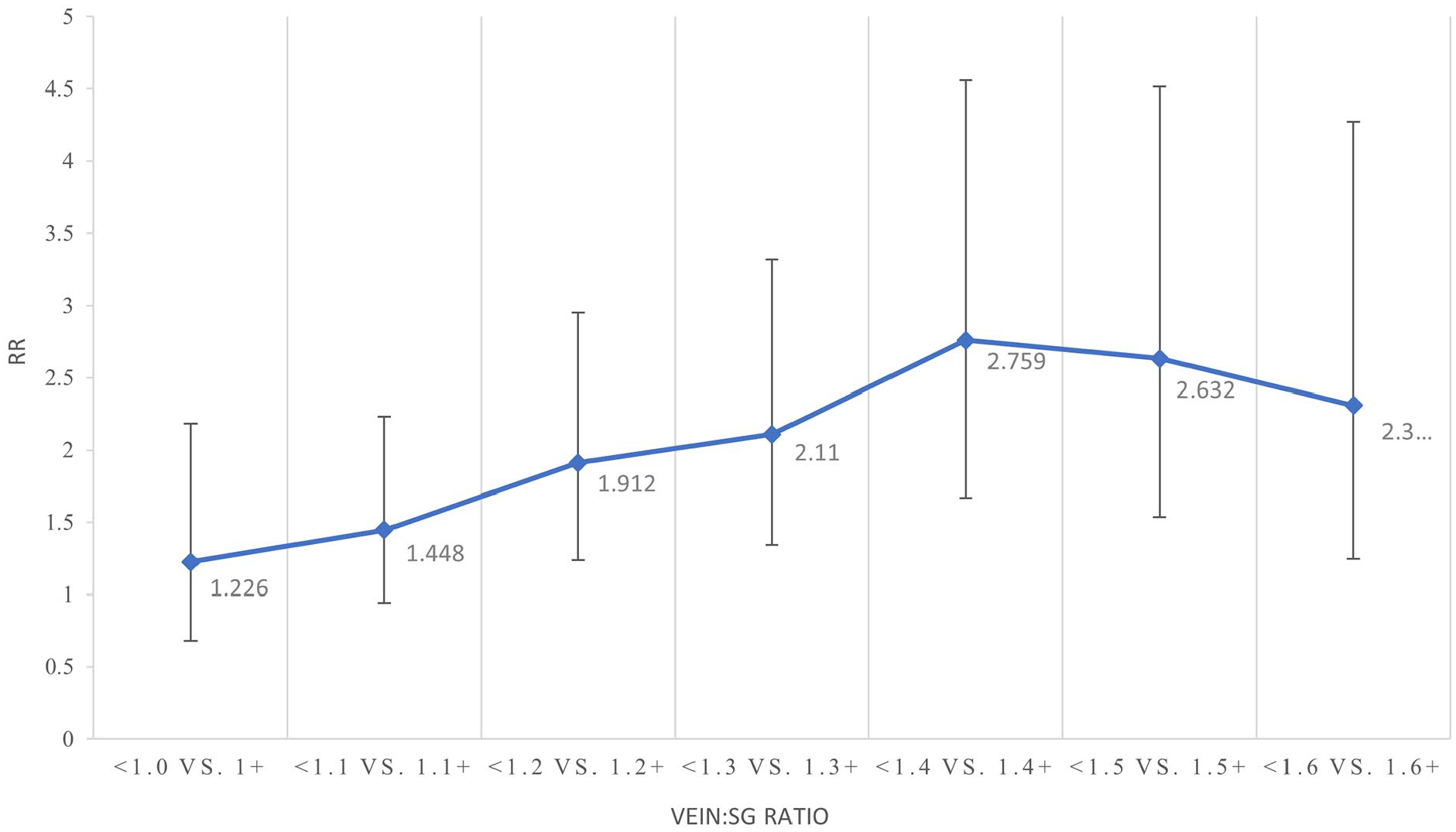
The risk of loss of primary patency by group of vein:SG ratio (V:Sr).
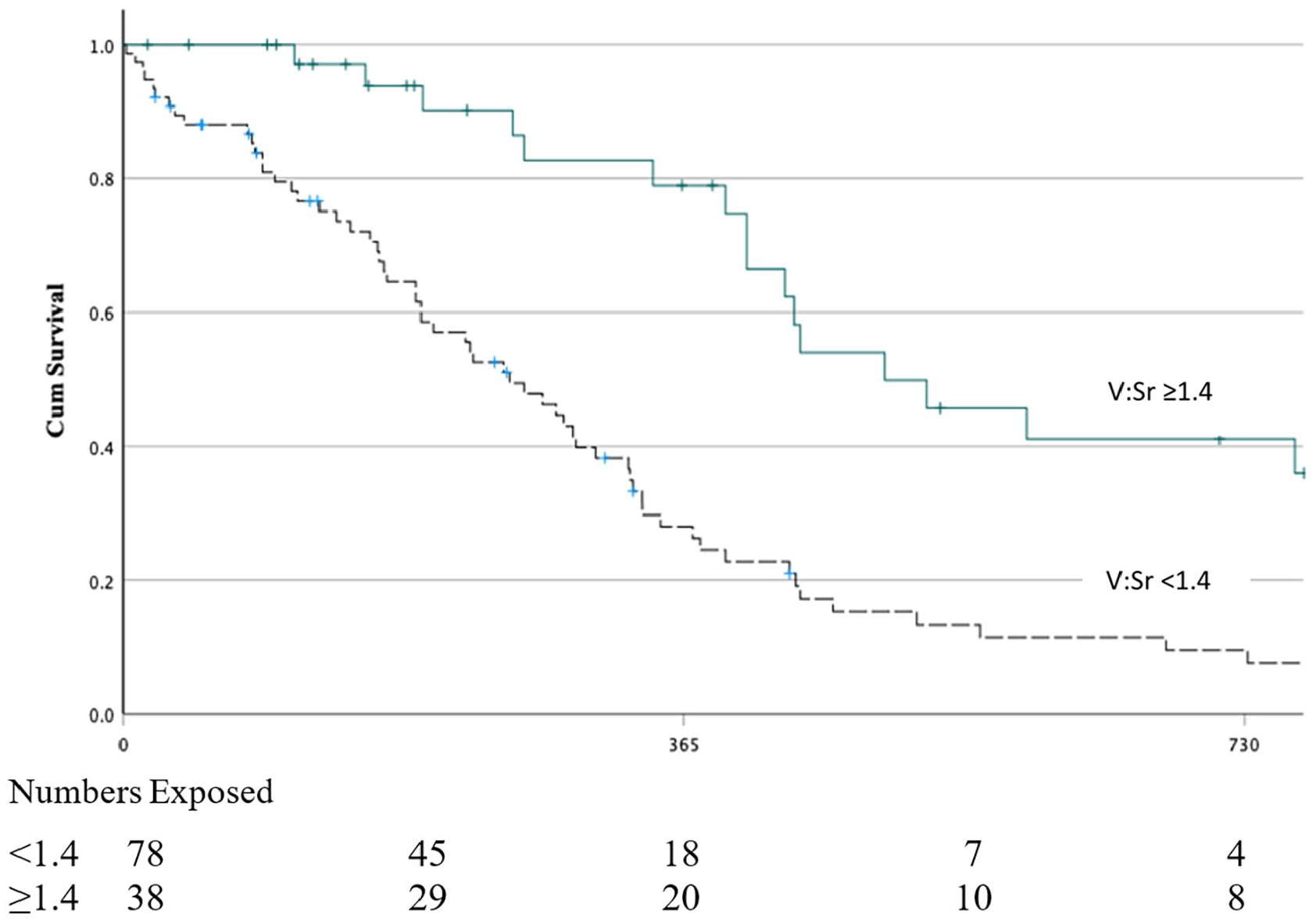
Primary patency comparing vein:SG ratio (V:Sr) of <1.4 vs ⩾1.4-Median: 252 (IQR:188–316) vs 496 (322–670) days, x2 = 17.034, p < 0.001; RR of loss of primary patency = 3.247 (1.560–6.759), p = 0.02 (adjusted for vein diameter as an independent variable on multivariate analysis).
There was no significant difference in the risk of thrombosis with V:Sr (x2 = 1.551, p = 0.213), nor in functional patency (x2 = 0.2, p = 0.886), although interestingly the risk of loss of functional patency due to thrombosis tended to significance (x2 = 2.817, p = 0.093).
Discussion
Venous stenosis is recognised as a key limitation of ecAVG, occurring in half during the first year despite surgical strategies to reduce this. 11 SG have shown great promise in reducing the impact of VS on outcome, but there is little information on technical aspects of deployment. This study demonstrates that, whilst the calibre or length of SG is not critical, the relative size of the SG to the outflow vein is significant. We can define the group who had V:Sr ⩾1.4 as having a free-floating stent outflow (Figure 4) and our data show that this is associated with a doubling in the time before further intervention is required.
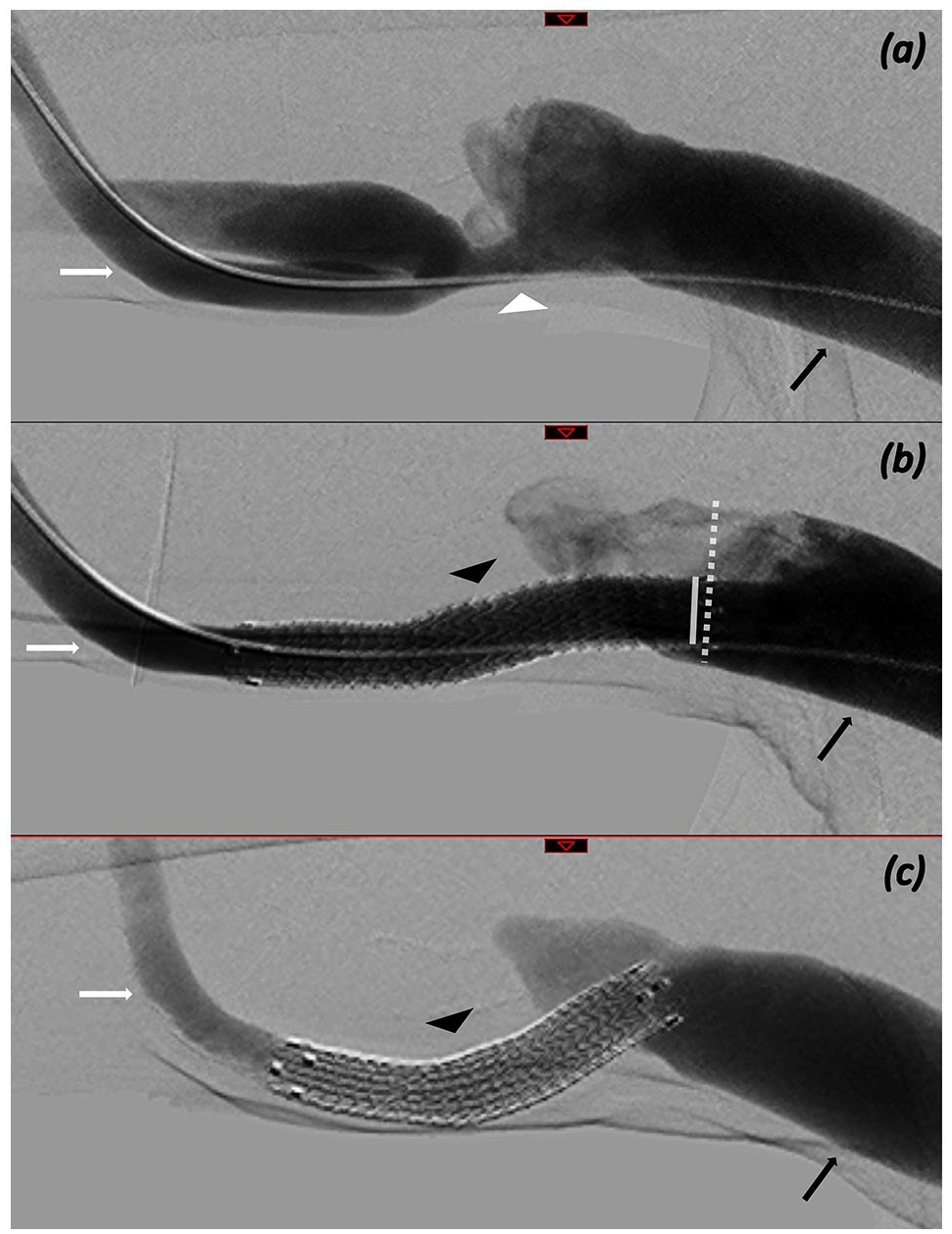
Multiple DSA images demonstrating ecAVG-venous anastomosis, before stent insertion (a), immediately after stent insertion and post dilation (b) and at 18 month follow up (c). ecAVG (white arrow) communicates with the outflow vein (black arrow) via stenotic venous anastomosis (white arrowhead). Newly inserted stent-graft demonstrated (black arrowhead) across the anastomosis. Angiographic measurements obtained included the stent-graft diameter (solid white line) and outflow vein diameter (dashed white line) at the point of stent outflow. Here the V:Sr is calculated to be >1.4 and there is maintained primary patency at 18 months.
The instructions for use for the SG when used at the venous anastomosis recommend sizing relative to the ecAVG diameter (at least 6 mm device calibre) and overlapping by at least 1cm into the ecAVG to provide effective anchoring however do not pre-specify sizing in the outflow vein. This is very different to the traditional arterial approach of oversizing stents by 10% both proximal and distal to the lesion. There may however be a fundamental difference in disease pathology between the arterial and venous outflows: whilst the arterial luminal compromise relates to relatively acellular atherosclerotic plaque, venous outflow stenosis is due to increased wall-shear stress promoting neointimal hyperplasia. 5 Therefore, deploying the end of the SG to lie in a vein larger in diameter than the SG may allow a better, more laminar flow pattern. This may in turn necessitate selecting longer SG devices than are typically accepted.
Our data demonstrate that veins with larger calibre are associated with increased primary patency but that this loses significance when assessed as an independent variable in multivariate analysis with V:Sr. This is of critical importance as it can be said anecdotally that bigger veins perform better whereas our data clarifies that whilst this is true to a certain extent, it is the relative sizing of the SG to the vein which is a more important factor. It is also worth noting that our measurements were only obtained at the point of stent outflow into the native vein and that vein outflow tracts generally tend to enlarge as they head centrally. There will therefore be many patients who were observed to have a SG with wall apposition to the outflow vein who could have had a longer and/or smaller calibre device inserted to facilitate a free-floating stent outflow (Figure 5).
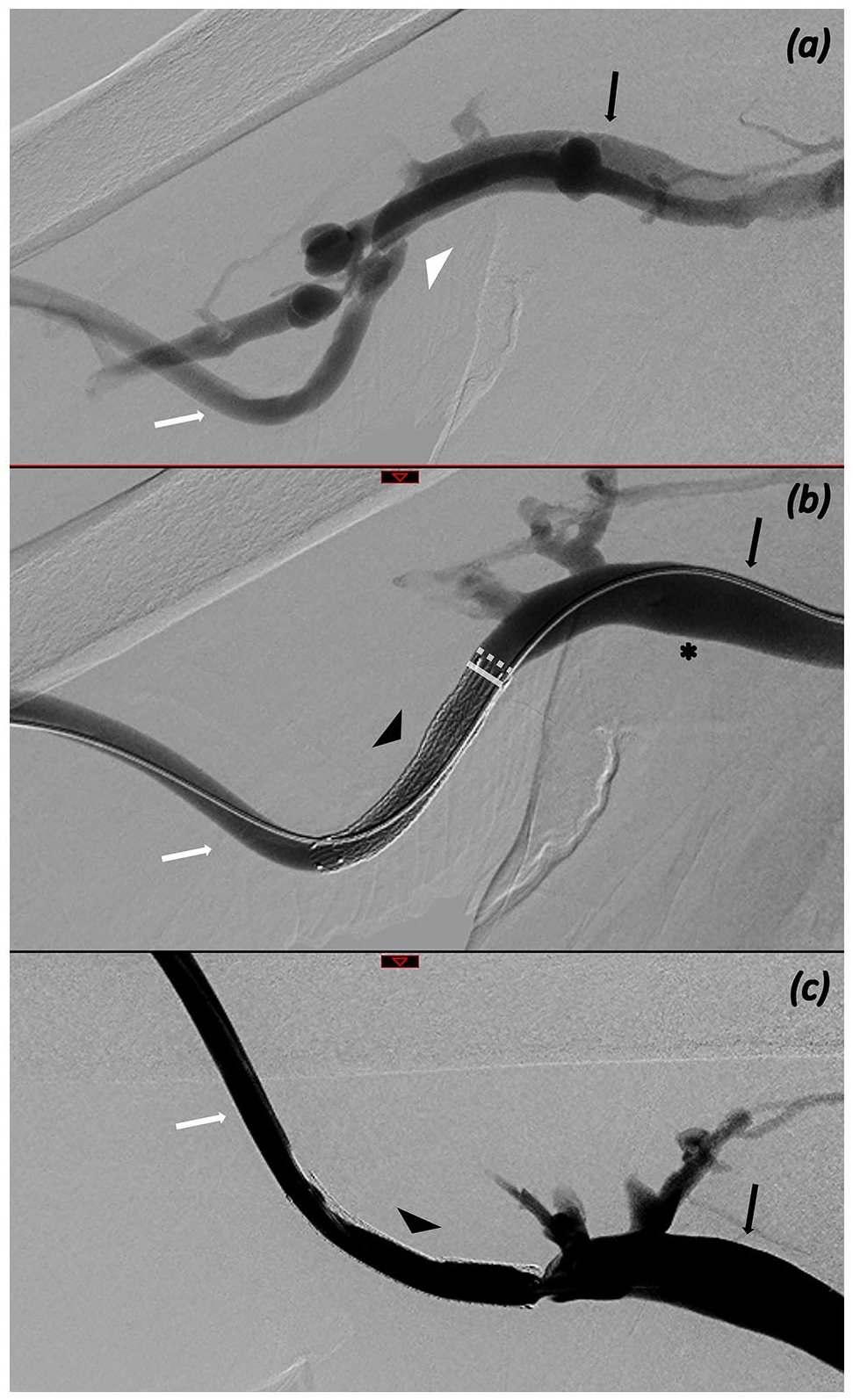
Multiple DSA images demonstrating ecAVG-venous anastomosis, before stent insertion (a), immediately after stent insertion and post dilation (b) and at 3 month follow up (c). ecAVG (white arrow) communicates with the outflow vein (black arrow) via stenotic venous anastomosis (white arrowhead). Newly inserted stent-graft demonstrated (black arrowhead) across the anastomosis. Angiographic measurements obtained included the stent-graft diameter (solid white line) and outflow vein diameter (dashed white line) at the point of stent outflow. Here the V:Sr is calculated to be <1.4 and there is early restenosis. More centrally, the outflow vein is of larger calibre (asterisk) and placement of the stent-graft outflow here would give a V:Sr of >1.4 and possibly facilitate improved primary patency.
This study has the benefit of assessing a uniform procedure (single type of ecAVG, single type of stent-graft). However, all AVG may be impacted by venous stenosis despite modifications in graft design and technique aimed to influence the rate of occurrence. 1 The findings may be particularly important to operators who attempt to achieve better wall apposition at the outflow, either with larger calibre or ‘flared’ devices. Our data suggest that this is not required to achieve satisfactory outcomes for the AVG and may in fact be counterproductive by contributing to neo-intimal hyperplasia as has been suggested in the literature. 12 This also applies to the location of the AVG, in that whilst the lower limb generally has larger outflow veins, the importance of relative sizing of the stent-graft remains the key to reducing re-intervention rates. The aetiology of recurrent stenosis at the vein-stent interface may relate to several factors including turbulent flow or mechanical forces of the stent. 12 Further work on the distribution of turbulence across the vein-stent interface may clarify if this or the mechanical irritation of the vein is responsible for recurrent stenosis. It is worth noting however, more novel stent-grafts that incorporate a softer end may not induce the same response and therefore potentially limit this phenomenon.
The V:Sr did not impact on functional patency or time to first thrombosis but approached significance for functional patency due to thrombosis. This is unsurprising as the impact on future events will be mitigated by treatment designed to optimise outcomes such as repeated angioplasty especially in this cohort undergoing routine surveillance. Similarly, thrombosis is not exclusively related to venous stenosis and will also be lessened by the high rate of inter-current events in this population such as death and renal transplantation.1,13
Whilst this study has several advantages (long-term follow-up with minimal loss to follow-up, single SG and ecAVG device use, angiographic follow-up, negligible lead time bias due to uniform surveillance procedure) it may be limited by being retrospective and thus susceptible to selection bias in the allocation to treatment. We believe this in turn is mitigated by the multiple operating interventional radiologists who independently chose the length and diameter of SG for insertion which may have led to a natural random distribution.
The outcomes from this data can be implemented in most instances of stent graft placement at the AVG venous anastomosis. The findings of this study are clear that a free-floating stent outflow is the aim and can often be achieved even with a minimum calibre stent graft of 6 mm (determined by the ecAVG). Operators should avoid placing the outflow stent end too close to the stenosis or in a smaller calibre vein where there will be wall apposition. Instead, if there is a segment of vein which is significantly larger in calibre within reasonable distance of the anastomosis then selection of a longer stent (which we have demonstrated in isolation does not correlate with outcome) should be made to bring the outflow to this point and in turn reduce the sequelae of wall shear stress and restenosis. Clearly this may not be achievable in all cases given anatomical factors. Intraprocedural measurement of outflow vein diameter is one potential consideration to facilitate optimal sizing and placement. Ideally, placing an undersized stent (with respect to the outflow vein) is the priority even if a longer stent graft is required.
This principle can also be applied if restenosis develops at the stent outflow and a significantly larger segment of vein is not within reasonable range. Our data suggests that extension of the stent-graft is unlikely to provide robust secondary patency if the new outlfow point still has V:Sr <1.4 and as such other intervention (e.g. DEB) should be considered.
The implications of this study have significance not only for current treatment paradigms but also future studies. Currently, there is a wider recognition that SG have several benefits, and if their use can be further optimised, then the criticisms of cost-efficacy may be reduced. In addition, future RCT of SG use should be based on their optimal deployment with a priority placed on the location of the outflow in the most appropriate location rather than minimising the length of SG used. This study adds necessary increased scrutiny on interventional radiology techniques and methods to optimise outcomes.
Our data show that despite the constant size of the ecAVG, there is variability of the stent-graft diameter and length chosen to treat the venous anastomotic stenosis. We suggest whilst outflow vein calibre is important, it is the vein to stent-graft ratio that is of critical importance and that the choice of device inserted could lead to poorer outcomes. We advocate SG selection that facilitates a free-floating stent outflow in ratio of at least 1.4 to maximise primary patency.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of the Vascular Access Coordinators at the Glasgow Renal and Transplant Unit.
Author contributions
D.B.K., C.S., R.K. and K.S.S. designed the study; D.B.K. and C.S. collected the data; D.B.K. and C.S. analysed the data; C.S. and D.B.K. drafted the paper; all authors revised the paper; all authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.B.K., K.S.S., P.C.T. and R.K. have received honoraria for speaking from W.L. Gore & Associates. D.B.K. has received an investigator research grant from Proteon Therapeutics and W.L. Gore & Associates.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
For this type of study formal consent is not required. Study registered with The Renal Services Clinical Effectiveness Group.