
Abstract
Introduction:
Thrombosed arteriovenous fistulas (AVFs) are either treated by thrombectomy or pharmaco-mechanical thrombolysis with or without percutaneous balloon angioplasty. In this study, we have described an effective and economical technique of salvaging these fistulae using a 20–22-gauge spinal needle and urokinase and have named it direct percutaneous thrombolysis (DPT).
Materials and method:
This prospective study comprised of 148 patients out of which 120 patients presented with AVF thrombosis and were divided into two groups; those with no obvious stenosis on ultrasound (n = 38) and second with venous stenosis (n = 82). Remaining 28 patients developed thrombosis post angioplasty for venous stenosis. Percutaneous injection of urokinase into the thrombus was done under ultrasound guidance, followed by balloon angioplasty if there was associated stenosis.
Results:
In 38 patients who didn’t have any stenosis, 32 AVFs were successfully thrombolysed by DPT, with technical success of 84.2%. Remaining six patients required angioplasty because of chronic nature of clot. In 82 patients who had venous stenosis, 80 cases were treated successfully by DPT followed by angioplasty with technical success of 97.5%. In third group (n = 28), who developed thrombosis post angioplasty, 100% success rate was noted. The mean length of thrombus was 31.4 ± 4.6 mm and mean diameter of thrombosed vein was 10.5 ± 1.2 mm. There were no major complications encountered during the procedure. Minor complications were seen in 19 patients which included prolonged oozing from puncture site and local hematoma formation.
Conclusion:
Ultrasound guided DPT with urokinase is a safe and economical option for salvaging thrombosed AVF without vascular stenosis that does not need angioplasty.
Keywords
Introduction
As per Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines, native arteriovenous fistula (AVF) remains the vascular access of choice for providing maintenance hemodialysis in end stage renal disease (ESRD) patients. 1 However, thromboses of these AVFs remain one of the main causes of both early and delayed failure, leading upto 65%–85% of cases of permanent access loss. 2 Such patients require either new AVF creation or placement of chronic central venous catheters for hemodialysis. Thrombosis of AVF can occur due to multitude of causes, most common being stasis due to stenoses, others being systemic factors like hypotension or hypercoagulability (common in ESRD patients) and local factors like prolonged compression on the puncture site post-dialysis or post-percutaneous procedures and improper needling.2,3
Salvaging of these dysfunctional thrombosed AVFs is necessary to ensure improved long-term survival and quality of life for these patients. Surgical thrombectomy which was the mainstay treatment previously, has been increasingly replaced by various endovascular techniques due to their good patency rates and decreased morbidity.4,5 The various endovascular methods currently available can be divided into catheter guided thrombolysis, mechanical thrombectomy or combination of both. Thrombolytic agents like tissue plasminogen activator (tPA) or urokinase are infused either through peripheral veins or via an infusion catheter placed into the thrombosed vein. Systemic complications such as bleeding are less with local catheter guided thrombolysis compared to systemic thrombolysis.5–7 Mechanical aspirational, rheolytic or rotational thrombectomy devices are also used sometimes followed by angioplasty. Most of these treatment methods offer good clinical outcome but are quite expensive, and it becomes very difficult for most of the patients to afford these treatments.
In this study we have described an effective and economical method of thrombolysing and salvaging these thrombosed AVFs by injecting urokinase in clotted AVF percutaneously under USG guidance using a 20–22-gauge spinal needle and have named it direct percutaneous thrombolysis (DPT). This was followed by balloon angioplasty if required. We have also reported our experience of performing DPT in native thrombosed AVFs without stenosis and DPT + balloon angioplasty in thrombosed AVFs with stenosis.
Material and methods
Patients
This was a single-center prospective study conducted after obtaining approval from our institutional review board. All those patients, who were referred to our department for fistula salvage from July 2016 to June 2020 were enrolled in the study. Exclusion criteria included thrombosed vein diameter more than 2 cm and thrombus length more than 10 cm (because of previous experience of high failure rate), local thrombophlebitis and any contraindication for use of thrombolytics. Total of 148 patients were included in our study, out of which 120 patients (74 males, 46 females) presented with AVF thrombosis. Targeted ultrasound was done in these patients and were divided into two groups; those with no obvious stenosis on ultrasound (n = 38) and second with venous stenosis (n = 82). Remaining 28 patients (12 males, 16 females) initially presented with poor flow and were found to have venous stenosis on USG, and developed AVF thrombosis post angioplasty.
Technique
Under ultrasound guidance, 20–22 G spinal needle (or intravenous cannula) was introduced percutaneously into the clot. After confirming the needle tip position into clot, 50,000–100,000 IU of urokinase diluted in saline (5–10 ml) was injected in the clot by advancing and withdrawing needle under real time ultrasound guidance. Attempt was made to cover maximum possible length of clot in a single skin puncture, so that number of skin punctures can be minimized. Entire clot was laced locally with urokinase and left for 20–30 min (Figure 1). If satisfactory flow was not restored after 20–30 min, repeat thrombolysis was done with maximum of 50,000–100,000 IU urokinase. After waiting another 30–60 min, if there was no satisfactory flow, then patient was taken for angioplasty. Clinical end point was good brisk flow restoration and not complete clot clearance.
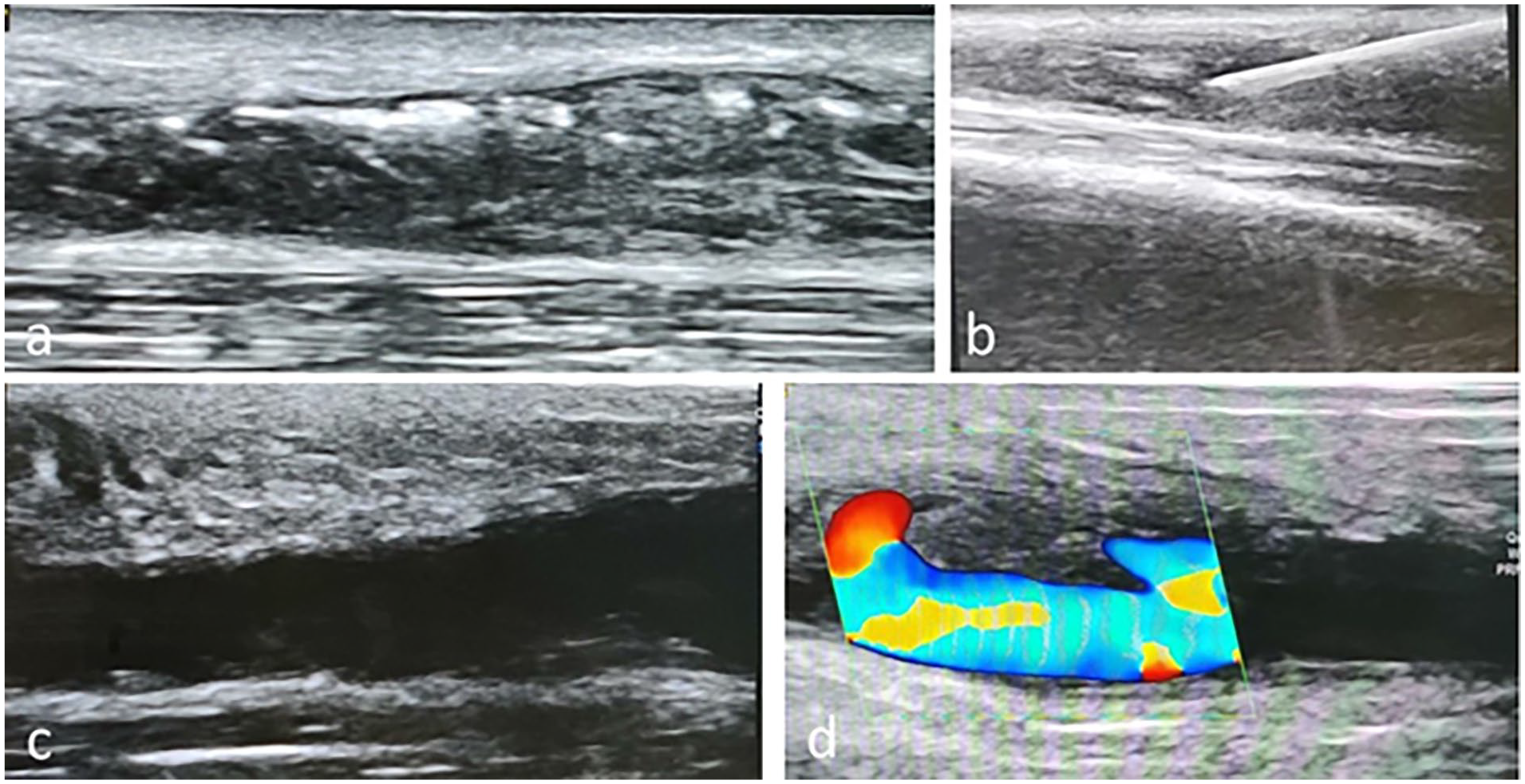
Ultrasound images of direct percutaneous thrombolysis performed for thrombosed radio-cephalic fistula with no stenosis in 43-year-male patient: (a) thrombosed cephalic vein with no flow, (b) under USG guidance, 21 G spinal needle introduced into the thrombus, and 100,000 IU urokinase bolus dose administered, (c) post thrombolysis, complete dissolution of thrombus in B-mode USG, and (d) on color doppler, good flow noted in the cephalic vein.
First group of patients who just had thrombus without any obvious stenosis on ultrasound, underwent DPT followed by angioplasty if DPT was unsuccessful. In the second group of patients having thrombosis with stenosis, percutaneous transluminal angioplasty (PTA) was performed 30–40 min after DPT in all cases (Figure 2). For angioplasty, retrograde arterial access was usually preferred in distal radial artery and in some cases, antegrade venous access (cephalic or basilic veins) was taken. Care was taken not to access through the same puncture site used for DPT in order to reduce bleeding complications. Post dilatation, venography was done to check the response. If the response was suboptimal, repeat angioplasty was done. Clinical end point again was good distal runoff and not complete clot clearance. Third group of patients who developed thrombosis post-angioplasty were initially treated with DPT followed by angioplasty if required.
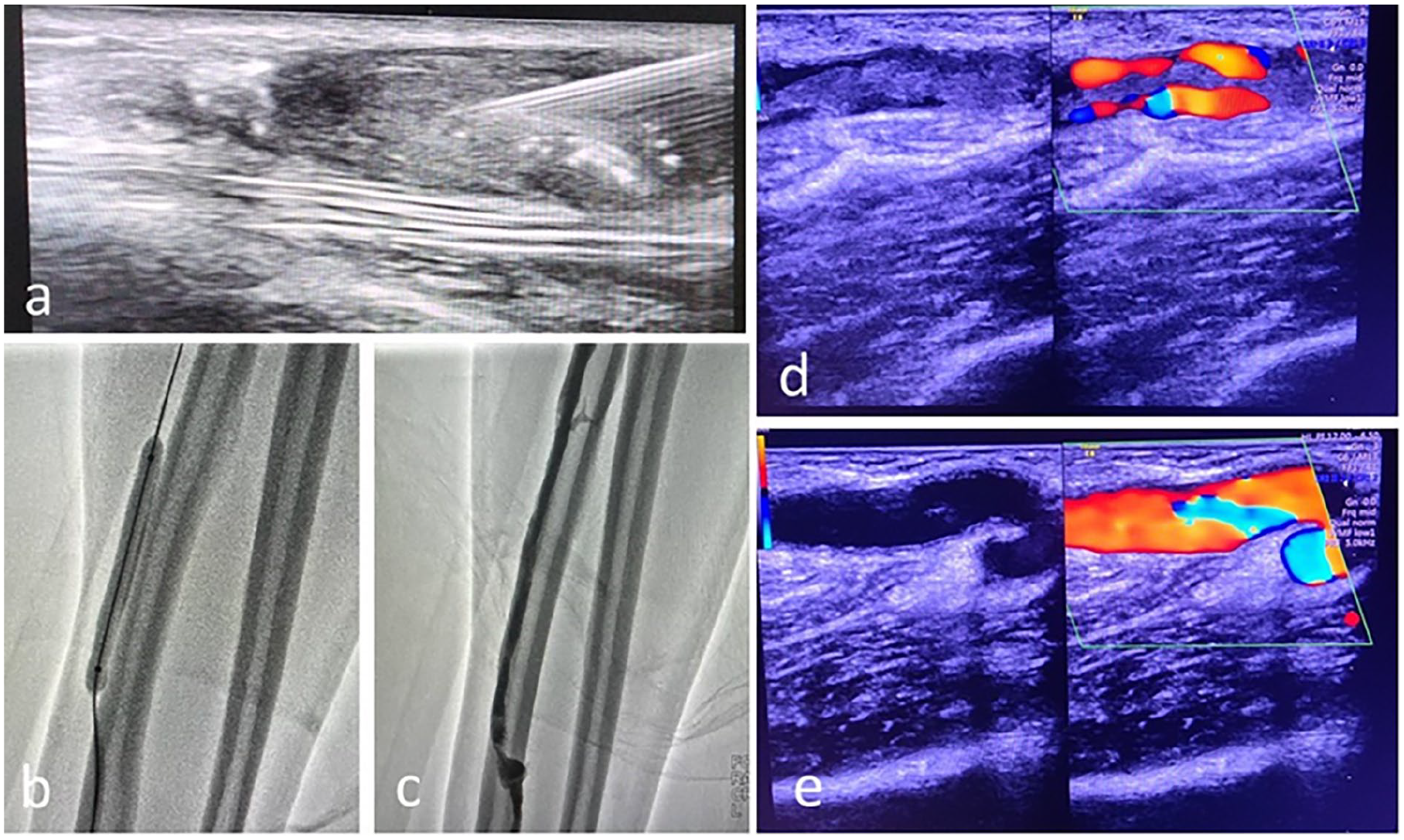
Ultrasound and angiographic images of direct percutaneous thrombolysis followed by angioplasty performed for thrombosed radio-cephalic fistula with stenosis in 39-year-male patient. (a) Under USG guidance, 21 G spinal needle introduced into the thrombosed cephalic, and 100,000 IU urokinase bolus dose administered, (b) percutaneous angioplasty performed for short segment cephalic vein stenosis, (c) post angioplasty, angiography showing good flow across the fistula into the cephalic vein, (d) B-mode and Color doppler image pre-procedure showing thrombus in cephalic vein with partial decreased flow, and (e) B-mode and Color doppler image post-procedure showing complete dissolution of thrombus with good complete flow in lumen.
Once good flow was achieved either post thrombolysis or post angioplasty, these patients were placed on anticoagulation with intravenous heparin 5000IU 6 hourly for 24 h. All of these procedures were done on a day care admission basis.
According to the quality improvement guidelines published by the Society of Interventional Radiology, anatomical or technical success is defined as restoration of flow with less than 30% residual diameter stenosis. Clinical success is defined as resumption of normal dialysis for at least one session or palpation of continuous thrill extending from arterial anastomosis. 4
Results
The study population consisted of 148 patients with 86 males (58.1%) and 62 females (41.9%). The mean age of the patients was 45.72 ± 2.34 years (range: 21–67 years). Among 148 patients, 86 (58.1%) had thrombosed radio-cephalic fistulas (RCF), 49 (33.1%) had thrombosed brachio-cephalic fistulas (BCF) and 13 (8.8%) had thrombosed brachio-basilic fistulas (BBF). The mean length of thrombus was 31.4 ± 4.6 mm (range: 12–100 mm) and mean diameter of thrombosed vein was 10.5 ± 1.2 mm (range: 6–16 mm). The thrombus involved the cannulating segment of veins in 105 cases (71%) and juxta-anastomotic venous segment in 60 cases (40.5%).
Among the 38 patients from group one, (26 RCF and 12 BCF), who had no obvious detectable stenosis on ultrasound, 21 patients (55.3%) gave history of prolonged compression post dialysis and 11 (28.9%) had history of hypotension during the procedure. Twenty-six patients (68.4%) underwent DPT within 48 h of symptom onset, while remaining 12 patients presented more than 48 h. Technical success was achieved in 32 cases (84.2%), with average of 100,000–200,000 IU urokinase per patient. Clinical success was achieved in 31 cases (81.6%). One patient developed re-thrombosis after successful DPT and later on required angioplasty. Six patients in whom DPT failed to restore flow, underwent angioplasty and post angioplasty all these six fistulas were salvaged. All these six patients who did not respond to DPT presented later than 48 h of their symptom onset.
In second group (n = 82), who were detected to have stenosis, (42 RCF, 28 BCF and 12 BBF), 46 patients (56%) had stenosis in the cannulating segment and remaining 36 patients (44%) had juxta-anastomotic site stenosis. All these patients underwent DPT + angioplasty and technical success was achieved in 80 cases (97.5%). In two patients because of heavy clot load, flow could not be established and procedure was abandoned. Fourteen patients developed re-thrombosis after 24 h bringing down clinical success to 80%.
Twenty-eight patients from group 3 (18 RCF, 9 BCF, 1 BBF) who developed thrombosis post-angioplasty, were treated with DPT followed by repeat balloon angioplasty if required and in all cases, flow was restored with 100% technical and clinical success.
No major complications were noted in any of the patients. Minor complications were seen in 19 patients (12.8%), which included prolonged oozing from puncture site in 15 cases (10%), local hematoma formation in five patients (3.4%), and post procedure edema and local blister formation in two patients (1.3%). In two patients of thrombosed BCF with dilated juxta-anastomotic venous segment and cephalic vein stenosis in mid arm, post DPT there was migration of clots into brachial artery distal to anastomosis, which were later on aspirated using 6 F guide catheter.
Discussion
This study showed that DPT is an effective method for salvaging acutely thrombosed native AV fistulas in selective group of patients, and can be used as first line option especially in patients with thromboses without any underlying anatomical stenoses.
Thromboses with or without stenosis constitute a leading cause of failure of native AV fistulas, and early treatment is necessary to prevent the access loss. 1 Dialysis access thrombosis can be attributed to Virchow’s triad of stasis, hypercoagulability and endothelial injury/dysfunction. 2 Stasis may be due to reduced inflow as can occur with systemic hypotension or decreased outflow as seen with venous stenosis. The stenosis may occur due to turbulent flow across the fistula causing microendothelial injury and neointimal hyperplasia, molecular factors or injury due to repeated needling during dialysis.2,8 In general, the most common underlying cause for thromboses remain the venous stenoses, as was seen in 68% of our cases. Intradialytic hypotension occurring in ~5%–30% of the patients undergoing hemodialysis, constitute another important cause of vascular access thrombosis, even in patients without any stenosis. 9 In our series, 29% of our patients with no venous stenosis had history of intradialytic hypotension.
Treatment of thrombosed AV fistulas has two main objectives—removing the thrombus per se and removing underlying causes if any. The former can be achieved by surgical thrombectomy or by endovascular means using various declotting methods like—pharmacological thrombolysis, mechanical thrombectomy or pharmaco-mechanical methods. The endovascular approach offers advantage in addressing the thrombus and vascular stenosis by doing adjunct balloon angioplasty. Mechanical clot dissolution can be performed using compliant balloons, percutaneous thrombolytic devices, hydrodynamic rheolytic devices or percutaneous thrombo-aspiration.5,10 Even though the procedure time is reduced with use of such devices, damage to the vascular endothelium is of major concern. The high cost and availability of these devices preclude their usage in all situations.
Pharmacological thrombolysis involves usage of thrombolytic agents such as streptokinase, urokinase or recombinant tissue plasminogen activator (rt-PA; alteplase & reteplase). 11 Catheter-directed thrombolysis is well described in literature, with thrombolytic agents infused either continuously or in forceful pulsed manner at least 30–120 min prior to the procedure.6,7,12,13 Once clot gets macerated adequately, mechanical aspiration, thrombectomy or balloon angioplasty can be attempted. The requirement of infusion catheter again adds to the cost of the procedure. If all the side holes of the catheter are not within the thrombus, systemic dose of thrombolytics might increase.
In DPT, the thrombosed vessel is directly punctured under ultrasound guidance using 20–22 G spinal needle (or intravenous cannula), eliminating the need for additional device. Insertion of the needle is usually avoided at the anastomotic stie and it is introduced from the distal end of thrombus, traversing the entire length of thrombus. The entire dosage of thrombolytics is administered within the clot under real time, concentrating the drug within the thrombus, and effectively decreasing the requirement of higher doses and systemic toxicity. As the half-life of urokinase is 15–20 min, thrombolysis with urokinase can be repeated after 30 min if satisfactory flow is not established. Our study showed that DPT has procedural success of around 84% for thrombosed AVFs with no stenoses. This is comparable to pharmaco-mechanical methods employed in other studies which ranged from 75% to 93%.7,14–18
The studies by Mangiarotti et al. 14 and Zaleski et al. 15 were one of the initial reports on use of urokinase for thrombosed AVFs, with procedural success of 65%–82%. The maximum dosage of urokinase used in various studies ranged from 250,000 to 1,000,000 IU.6,13–19 The maximum dosage of urokinase used in our study was 400,000 IU. The studies by Boonsrirat and Hongsakul 7 and Cho et al., 16 using pulse-spray technique of urokinase for thrombosed AVFs followed by balloon angioplasty reported technical success of 85.7% and 75% respectively. Liang et al. performed infusion of thrombolytics post angioplasty with urokinase (60,000 IU/h) and reported 93% success rate. 18 Apart from urokinase, the other drug which has been effectively used for thrombolysis is rt-PA (alteplase), with dosages ranging from 1 to 7 mg.6,7,12,20
The patients in whom DPT was not effective presented more than 48 h. As the clot ages, it gets adhered to the wall of the vessel and becomes more resistant to any form of treatment.7,13,21 Hence it is necessary to identify the thrombus early and initiate timely thrombolytic treatment. Our main goal with thrombolytic therapy is to dissolve the clot to promote the blood flow across the occluded site. Entire thrombus need not be removed, since with restoration of blood flow across fistula site, the residual thrombus gets dissolved by inherent fibrinolysis. Vorwerk et al. in their study stated that despite residual thrombus (~10%–50% in their series), blood flow across the fistula site was completely established in 81% of their cases. 22
Minor bleeding complications have been reported with use of urokinase upto 10%.12,13,23 Clinically significant pulmonary embolism resulting in the respiratory distress or even cardiac arrest is rare complication with incidence of 0%–1% reported in literature.24,25 The most common complication encountered in our study was prolonged bleeding and local hematoma formation. These complications were managed conservatively post procedure and did not translate to increased morbidity for patients. There was no major complication resulting in prolonged hospitalization or death in our patients.
The main limitation with this study was inherent selection bias, as we did not enroll patients with very long thrombosed segment and grossly dilated thrombosed venous segment. There was also lack of comparison between the various groups enrolled. A large prospective study comparing the effects of urokinase monotherapy with other pharmaco-mechanical techniques in patients without underlying stenosis is needed to establish the most appropriate method. Another limitation was the lack of adequate follow up regarding the long-term patency with this technique.
Conclusion
Direct percutaneous thrombolysis with urokinase is minimally invasive, effective and economical option for salvaging thrombosed native AVF without vascular stenosis that does not need angioplasty and can be used as first line option replacing catheter directed thrombolysis. It is as effective and safe as other techniques available to treat such fistulas. The main reason for failure with this technique happens to be chronicity of thrombus. Any underlying stenosis should be identified before DPT and adequately treated thereafter with percutaneous angioplasty.
Footnotes
Acknowledgements
NA
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted after obtaining approval form our Institutional Review Board (IRB).
Informed consent
Informed consent was obtained from all individual participants included in the study.