
Abstract
A 38-year-old male patient was diagnosed as acute non-ST-segment elevation myocardial infarction on Apr 21st 2021 and he received percutaneous transluminal coronary angioplasty for RCA via transradial artery access. He sought for second percutaneous coronary intervention in our center for frequently exertional angina on Sep 13th 2021. Proximal right radial artery pulsation can not be touched in physical examination, indicating right radial artery occlusion (RAO). Distal transradial access was applied and RAO was confirmed via angiography. With balloon pre-dilation, the guidewire and guiding catheter crossed the occlusion and coronary intervention was successfully completed. A Reewarm 2.5 × 220 mm paclitaxel drug-coated balloon (Endovastec, China) was released at 12 atm in radial arterial lesion with 90 s. Pulsation of radial artery can be well palpated 24 h after PCI. No oral anticoagulant was added. The right radial artery remained patent after 8-month and 14-month follow-up and there was no abnormal sensation or obstacle of right hand.
Keywords
Introduction
Transradial access (TRA) has become the main pathway of coronary intervention due to its comfort and low incidence of vascular complications. 1 However, the clinicians must confront the complications of TRA, of which radial artery occlusion is a severe one, affecting repeat coronary intervention, arteriovenous fistulation for end-stage kidney disease, application of coronary bypass graft. 2 Retrograde recanalization of RAO with plain balloon via dTRA was feasible, 3 but the high incidence of restenosis and re-occlusion can not be overcome.4–6 In this case, we improved our procedure not only recanalization with plain balloon but also treatment with paclitaxel-coated balloon. Right radial artery remained patent after 14-month follow-up. The patient agreed to be reported anonymously with written consent and the ethics committee of Fuwai hospital has approved its publication.
Case description
A 38-year-old male patient was hospitalized in Fuwai Hospital on Sep 13th 2021. He was diagnosed as acute non-ST-segment elevation myocardial infarction (NSTEMI) on Apr 21st 2021. Percutaneous transluminal coronary angioplasty (PTCA) was completed with drug-coated balloon (DCB) for infarction-related RCA via TRA at local hospital, and he was suggested to treat residual left main artery stenosis in experienced cardiology center. The patient received optimal medications but still felt frequently exertional angina. He sought for second percutaneous coronary intervention (PCI) in our center. He has no history of hypertension, diabetes and other peripheral artery disease before. The patient’s height was 176 cm, and his weight was 76 kg. The blood pressure at admission was 127/89 mmHg (1 mmHg = 0.133 kPa), and the heart rate was 75 bpm. Right radial artery pulsation proximal to styloid process could not be touched, indicating right radial artery occlusion (RAO), while pulsation at snuffbox could be touched from superficial palmar arch, providing a possibility to recanalize the radial artery.
Procedure was conducted on Sep 14th 2021 via distal transradial artery access (dTRA) at location of snuffbox. The puncture site was chosen at the strongest pulse point at snuffbox without assistance of ultrasound. Duration of puncture and sheath insertion was about 5 min. Angiography confirmed RAO at right forearm (Figure 1(a)). Pilot 50 guidewire (Abbott, USA) and guiding catheter (St Jude Medical, USA) crossed occlusion after compliant balloon pre-dilation (8–12 atm). Balloon-assist technique (BAT) was adopted for diagnostic and guiding catheter (St Jude Medical, USA) to pass right radial artery after blood flow restored (Figure 1(b)–(e)). It took 27 min to recanalize the radial artery. Coronary angiography showed significant stenosis in the distal left main artery (LM) and proximal-middle part of left anterior descending artery (LAD). Assisted with intravascular ultrasound (IVUS, 60 MHz, BostonScientific, USA), two Resolute Integrity stents (Medtronic, USA) was implanted at lesions from medium LAD to LM. Duration of coronary intervention was 42 min. Guiding catheter retracting, a Reewarm 2.5 × 220 mm paclitaxel DCB (Endovastec, China) was released at 12 atm in radial arterial lesion for 90 s (Figures 1(f)–(h) and 2(a)). After 0.2 mg nitroglycerin bolus, IVUS was conducted confirming thrombi and limited dissection in right radial artery (Figure 2(b)–(e)). Duration of total procedure was 90 min. Pulsation of radial artery can be well palpated 24 h after PCI. No oral anticoagulant was added.
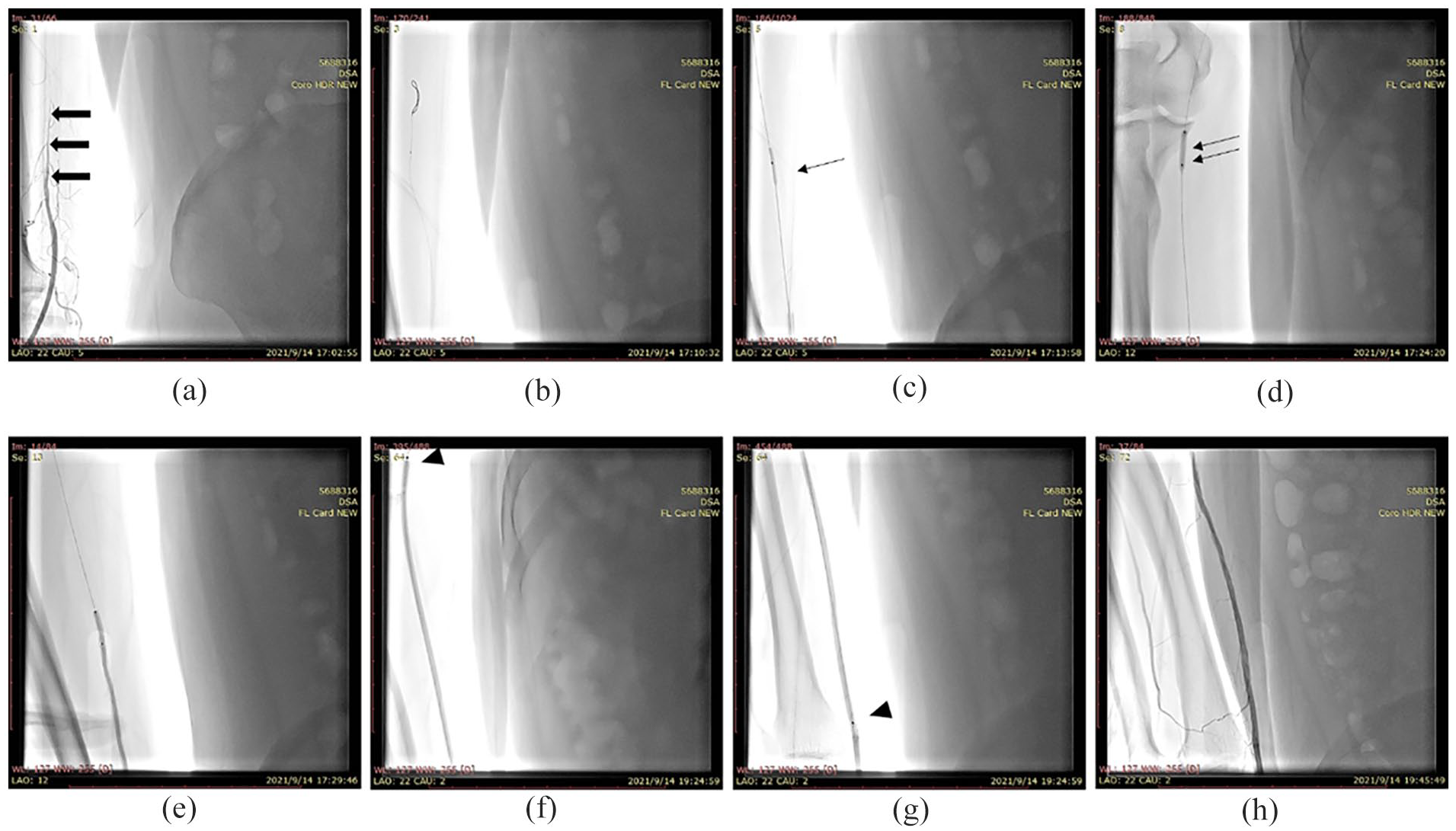
Angiography and intervention of right radial artery: (a) gradual interrupted blood flow of right radial artery (Coarse arrow), (b) a Pilot 50 guidewire crossed the lesion site with Knuckle technique, (c) the 1.5 × 15 mm balloon dilated the occlusion site (Single fine arrow), (d) the 2.5 × 15 mm balloon dilated the lesion (Double fine arrow), (e) catheter passed the radial artery lesion with balloon assisted technique, (f and g) the Reewarm 2.5 × 220 mm paclitaxel drug-coated balloon were released at the lesion (Triangles show the upper and lower marker points), and (h) angiography of radial artery after treatment.
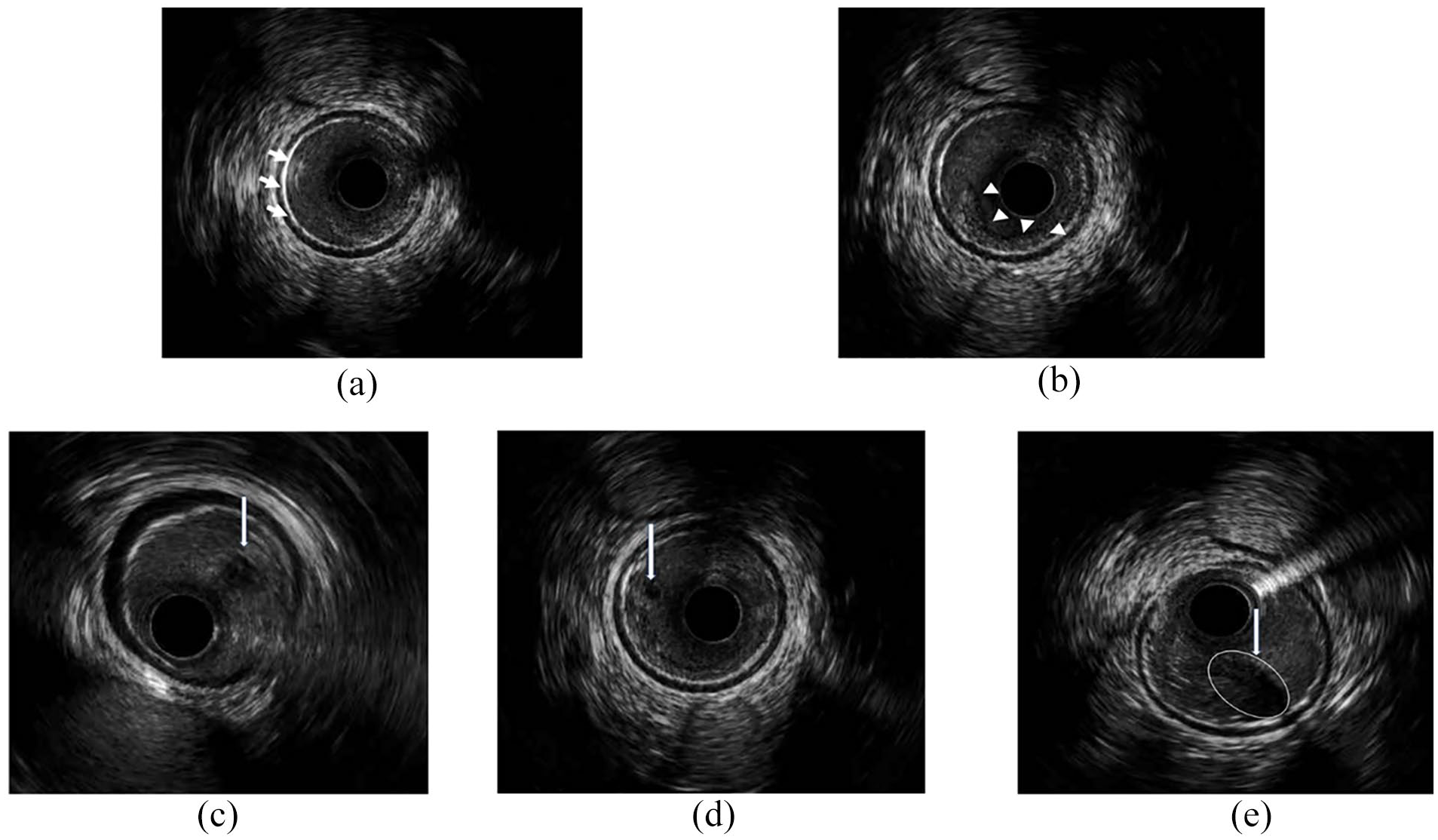
Intravascular ultrasound (IVUS) examination of right radial artery after dilation: (a) echography after drug-coated balloon (DCB) dilation (The high echogenic layer marked with white short arrows is the drug adhering the intima), (b) limited radial arterial dissection (marked with white triangles), and (c–e) thrombus in right radial artery (marked with long white arrows and circles).
Ultrasound examination of right radial artery at 8-month and 14-month follow-up was showed in Figure 3(a) to (j). The right radial artery remained patent after treatment. With intimal hyperplasia, the diameter of right radial artery was narrower than the other side at proximal 5 cm to radial styloid process at 8-month follow-up (Figure 3(c)) and recovered at 14-month follow-up (Figure 3(h)). There is no abnormal sensation or obstacle of right hand.
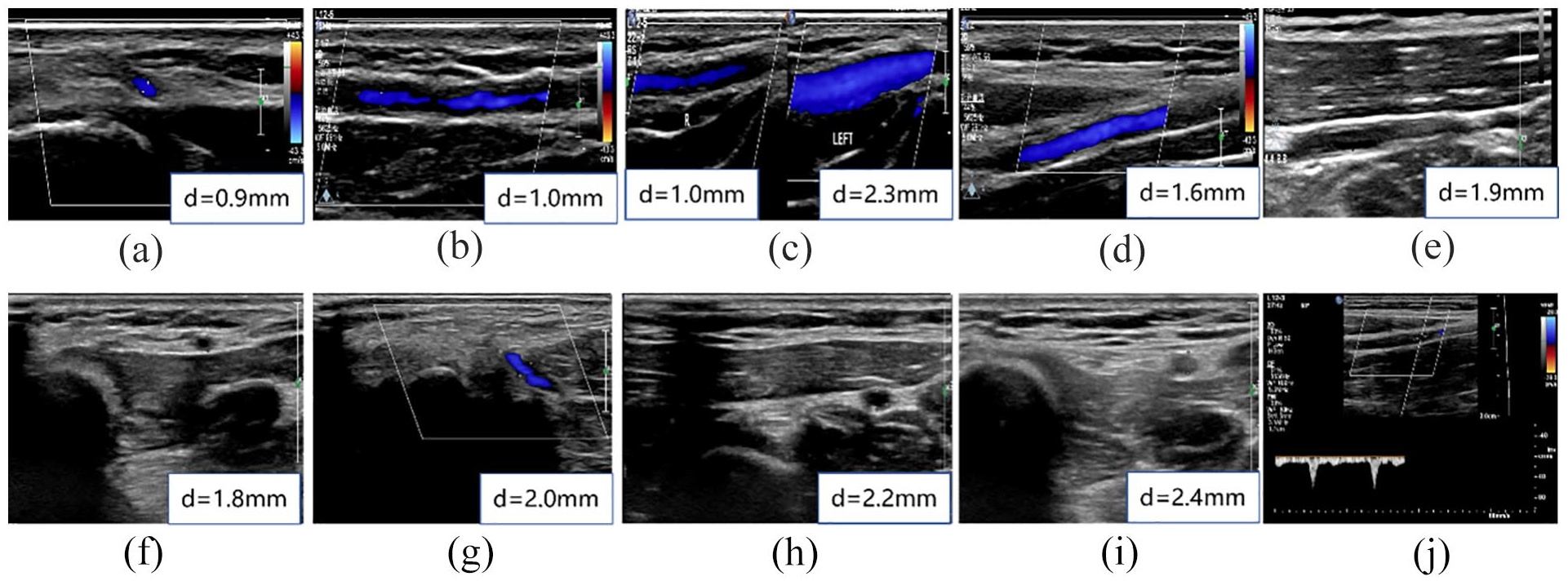
Ultrasound of radial artery at 8-month (a–e) and 14-month (f–j) follow-up. (a) Diameter of right radial artery at snuffbox (8-month), (b) diameter at 5 cm proximal to styloid process of radius (8-month), (c) comparison of right and left radial artery at 5 cm proximal to styloid process of radius (8-month), (d) diameter at 10 cm proximal to styloid process of radius (8-month), (e) diameter at 15 cm proximal to styloid process of radius (8-month), (f) diameter of right radial artery at snuffbox (14-month), (g) diameter at 5 cm proximal to styloid process of radius (14-month), (h) diameter at 10 cm proximal to styloid process of radius (14-month), (i) diameter at 15 cm proximal to styloid process of radius (14-month), and (j) the blood flow velocity of right radial artery (14-month).
Discussion and conclusion
dTRA is a novel arterial pathway applying snuffbox as the puncture site. 7 Retrograde recanalization of radial artery from dTRA is proved to be an effective method to resolve RAO since 2011.4,8 However, high incidence of radial artery restenosis or re-occlusion can not be overcome with plain balloon.4–6 Previous studies showed intimal hyperplasia was critical mechanism of chronic radial artery stenosis.9,10 Therefore, we improved the protocol applying paclitaxel DCB after RAO recanalization to suppress intimal hyperplasia and achieved stable patent radial artery. Dual antiplatelet therapy also assisted to inhibit thrombus formation. To our knowledge, this is the first report to intervene chronic RAO with DCB via dTRA. Although limited dissection after dilation, the blood flow was not affected and the right radial artery remained patent till now. We hope this technique could be verified in larger samples in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CAMS Innovation Fund for Medical Sciences (CIFMS) : 2022-I2M-C&T-B-048