
Abstract
Background:
Arterial lines and central venous catheter (CVC) allow to monitor patients’ acid-base status and gas exchange. Their placement and maintenance may however be burdened by severe complications. Midline Catheters (MC) are peripheral venous accesses that are less invasive and easier to insert compared to CVC and arterial lines.
Methods:
A prospective observational study was performed including stabilized critical patients with clinical indication to midline positioning before intensive care unit (ICU) discharge. The primary aim was to assess if venous sampling from MCs can be a reliable alternative to CVC for pH and CO2 monitoring. The secondary aim was to evaluate the correlation between samplings from MC, CVC and arterial line with regards to pH, carbon dioxide tension (pCO2), lactates and electrolytes. Three samples from CVC, arterial line and MC were collected simultaneously. Agreement and correlation of the studied parameters between different sampling sites were explored.
Results:
40 patients were included in the analysis. A good agreement for pH and pCO2 was recorded between MC and CVC: mean differences were 0.001 (95% CI −0.006 to 0.007) and 0.7 (−0.1 to 1.5), percentage error 0.4% and 11.2%, respectively. Correlation between MC and both central venous and arterial samples for pH, pCO2, lactates and electrolytes was found to be moderate-to-strong (Pearson’s R coefficient range 0.59–0.99, p < 0.001 for all these parameters).
Conclusions:
In stabilized critical patients, midline catheters represent a reliable alternative to CVC and arterial lines to monitor acid-base disturbances, CO2 levels and electrolytes. The present findings add to the known advantages of MC, which might be considered a first-line vascular access for non-critical or stabilized patients who do not require infusion of vesicant or irritant drugs.
Background
Arterial blood gas analysis represent a gold standard to evaluate pH, carbon dioxide and oxygen partial pressure (pCO2 and pO2 respectively) for both diagnostic and treatment purposes.1–3 However, arterial puncture/cannulation is technically difficult, is burdened with important complications, and is more painful and expensive compared with venous cannulation. Venous blood gas analysis (VBG) provides an alternative to arterial blood gas analysis. In hemodynamically stable patients, blood samples from central vascular catheters (CVC) provide pH and pCO2 values that have a good correlation with arterial ones.3–7 This correlation needs to be interpreted considering that the venoarterial difference of pCO2 is normally 4–6 mmHg but is increased to 8–10 mmHg in case of cardiac failure, 8 as it depends on the ratio of metabolic CO2 (VCO2) to cardiac output. 9 Central VBG may be obtained from an indwelling CVC, which is often required in patients admitted in the intensive care units (ICU) for intravenous infusions and hemodynamic monitoring. However, despite ultrasound guided CVC positioning and careful maintenance over time, complications such as arterial puncture and hematoma, pneumothorax, catheter-related blood stream infection (CRBSI) and thrombosis are reported.10–12
Midline catheters (MC), also known as mid-axillary catheters, are 15–25 cm long advanced peripheral catheters inserted in a deep vein of the arm, usually aimed at administering peripheral intravenous therapies for short or medium term.13–15 MCs are placed under ultrasound (US) guidance, both for vein cannulation and for locating the catheter tip in the axillary or subclavian vein. 16 Therefore, they are not considered to dwell in the central circulation, unlike CVC and peripherally inserted central venous catheters (PICCs). 17 MCs may provide some advantages compared to PICCs, as MCs positioning and management is easier in non-intensive hospital wards. 18 Compared to long peripheral catheters, 14 MCs’ tip is located in a larger vein of the thoracic district, proximal or distal to the clavicle.
To the best of our knowledge, no study has ever assessed whether MCs allow to monitor the acid base status and CO2 levels. At our institution, CVC and arterial lines are removed and replaced with a peripheral catheter (midline vs PICC) before ICU discharge, to minimize the risk of complications such as catheter-related infection or arterial ischemia.
We performed a prospective observational study including ICU patients with clinical indication of MC positioning. The primary aim was to verify whether venous blood gas analysis from MC is an accurate and precise surrogate for acid-base status and CO2 levels monitoring, as compared with central venous samples. The secondary aim of was to assess whether results of venous blood gas analyses from MC significantly correlated with arterial and central venous samples.
Materials and methods
A prospective observational study was performed including patients admitted to the ICU of Fondazione IRCCS San Gerardo dei Tintori (Monza, Italy) from November 2021 to July 2022. Patients were enrolled if they had a clinical indication19,20 for midline catheter positioning (i.e. estimate requirement of intravenous therapy of 7 days or more). Patients who did not express a written informed consent were excluded from the study.
Technical aspects
MCs were inserted by trained Nurses of the local Vascular Access Team, in adherence with current best practices 18 and with the Safe Insertion of PICCs (SIP) Protocol 21 and with an US guided positioning of the MC tip in the axillary vein, about 3 cm distal to the clavicle shadow. 16
Data collection
Demographic data (sex, age and BMI), diagnosis at ICU admission and time from ICU admission to midline positioning were recorded. Blood samples were drawn and analysed simultaneously (i.e. within a minute) by two operators from the midline catheter, the central venous line and the arterial line. The central venous catheter and/or the arterial line were then removed, if clinically indicated. Point-of-care RAPIDPoint® 500e Blood Gas Systems (Siemens Healthcare GmbH, Erlangen, Germany) were used for blood sample analysis and are normally placed at the bedside. For each sample pH, carbon dioxide (CO2), hemoglobin level, hemoglobin saturation and electrolytes were recorded.
Statistical analysis
Normality of data distribution was assessed by Shapiro–Wilk test. Continuous data were presented as mean ± standard deviation (SD). Categorical data were reported as count and proportion. Differences in continuous variables between parameters sampled from MC versus central venous or arterial line were assessed by paired Student’s t-test or Mann–Whitney U test as appropriate and were reported as mean differences with 95% confidence interval (95% CI). Analysis of agreement between pCO2 and pH in MC versus CVC was performed by using the Bland–Altman analysis. Bias (i.e. accuracy, calculated as the mean difference between values obtained from the two sites) with 95% limits of agreement (LA) (i.e. precision) were reported. The percentage error (PE) was calculated as 95% limit of agreement (1.96 × SD from the bias) divided by the mean pH or pCO2 (calculated as the mean of Midline and CVC measurements) times 100.
Correlation between MC and central venous or arterial samples was explored by linear regression analysis. Pearson correlation coefficient (R) and p-values were reported.
Data were analysed using JMP 15.2 software (SAS Institute, Cary, NC). Statistical significance was set at a two-tailed p-value < 0.05.
Results
During the study period, 40 patients were included. Eight (19.5%) patients were female, mean age was 55 ± 15 years and mean BMI was 28.5 ± 5 kg/m2. Twenty-three (57.5%) patients had a diagnosis of pneumonia, 22 of which were COVID-19 related. Other frequent causes of ICU admission were trauma (n = 5, 12.5%), intracranial hemorrhage (n = 5, 12.5%), and surgical emergencies (n = 3, 7.5%). Hypertension was the most common comorbidity among the study cohort (n = 17, 44%), followed by type II diabetes (n = 5, 13%), psychiatric and neurologic disease (n = 4, 10% and n = 4, 10% respectively). Other less frequent comorbidities reported were asthma (n = 3), chronic heart failure (n = 3), chronic renal disease (n = 3), chronic liver disease (n = 1) and autoimmune disorders (n = 1). One patient was pregnant.
Blood parameters obtained from the three different sampling sites are reported in Table 1.
Acid-base, oxygen levels and electrolytes from the three different sampling sites.
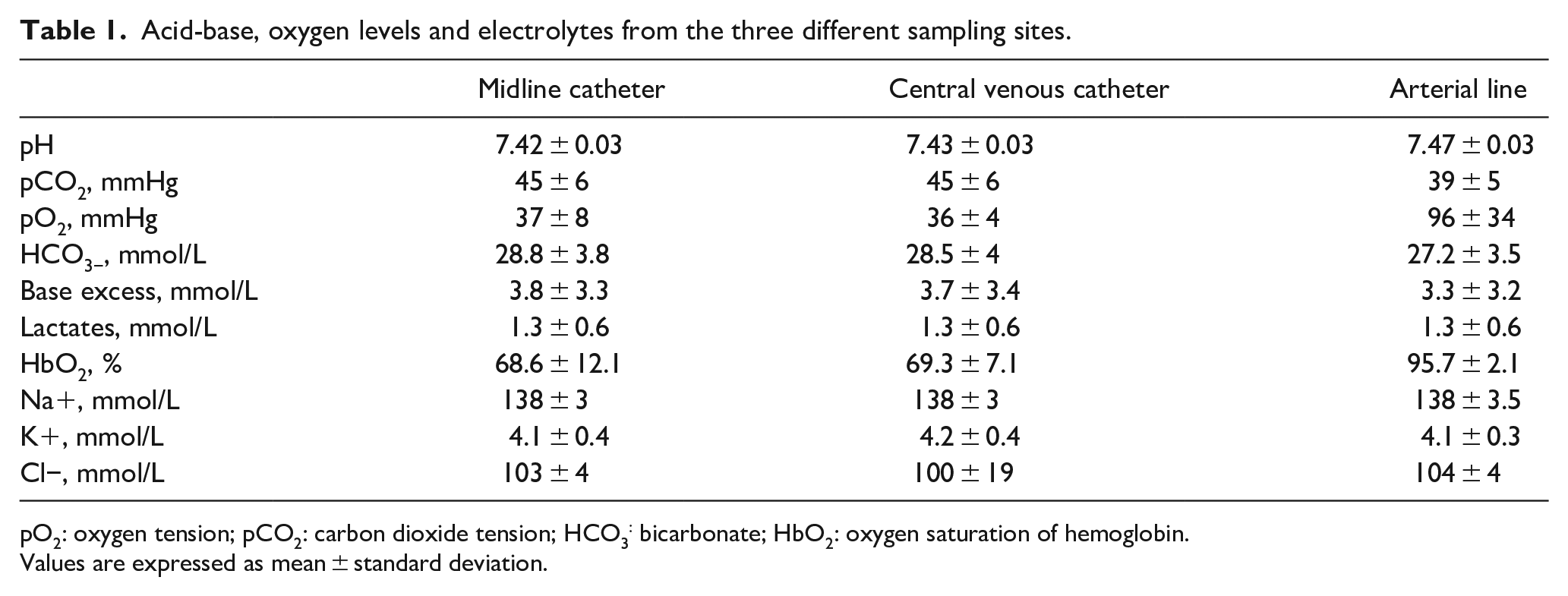
pO2: oxygen tension; pCO2: carbon dioxide tension; HCO3: bicarbonate; HbO2: oxygen saturation of hemoglobin.
Values are expressed as mean ± standard deviation.
The comparison of blood parameters between different samples (i.e. MC vs CVC and MC vs arterial line) is displayed in Table 2.
Comparison of blood parameters between MC, CVC and arterial line.
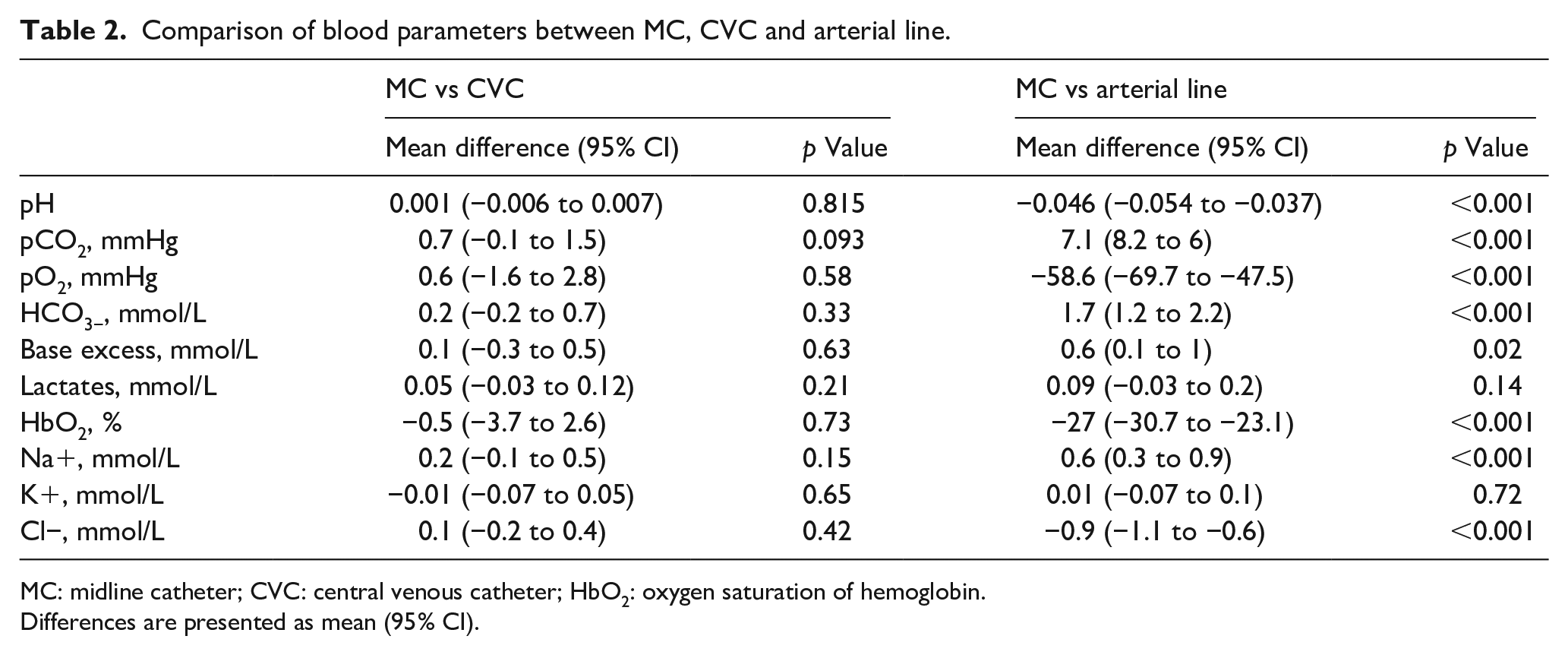
MC: midline catheter; CVC: central venous catheter; HbO2: oxygen saturation of hemoglobin.
Differences are presented as mean (95% CI).
No significant difference between MC and CVC samples was recorded. Differences in all blood parameters between MC and arterial line were statistically significant except for lactate and potassium levels (Table 2).
Analysis of agreements between MC and CVC parameters
Bland–Altman analysis showed good agreement for both pCO2 and pH values between CVC and MC (Figure 1 – Panel A and B respectively). Percentage errors were 11.2% and 0.4%, respectively.
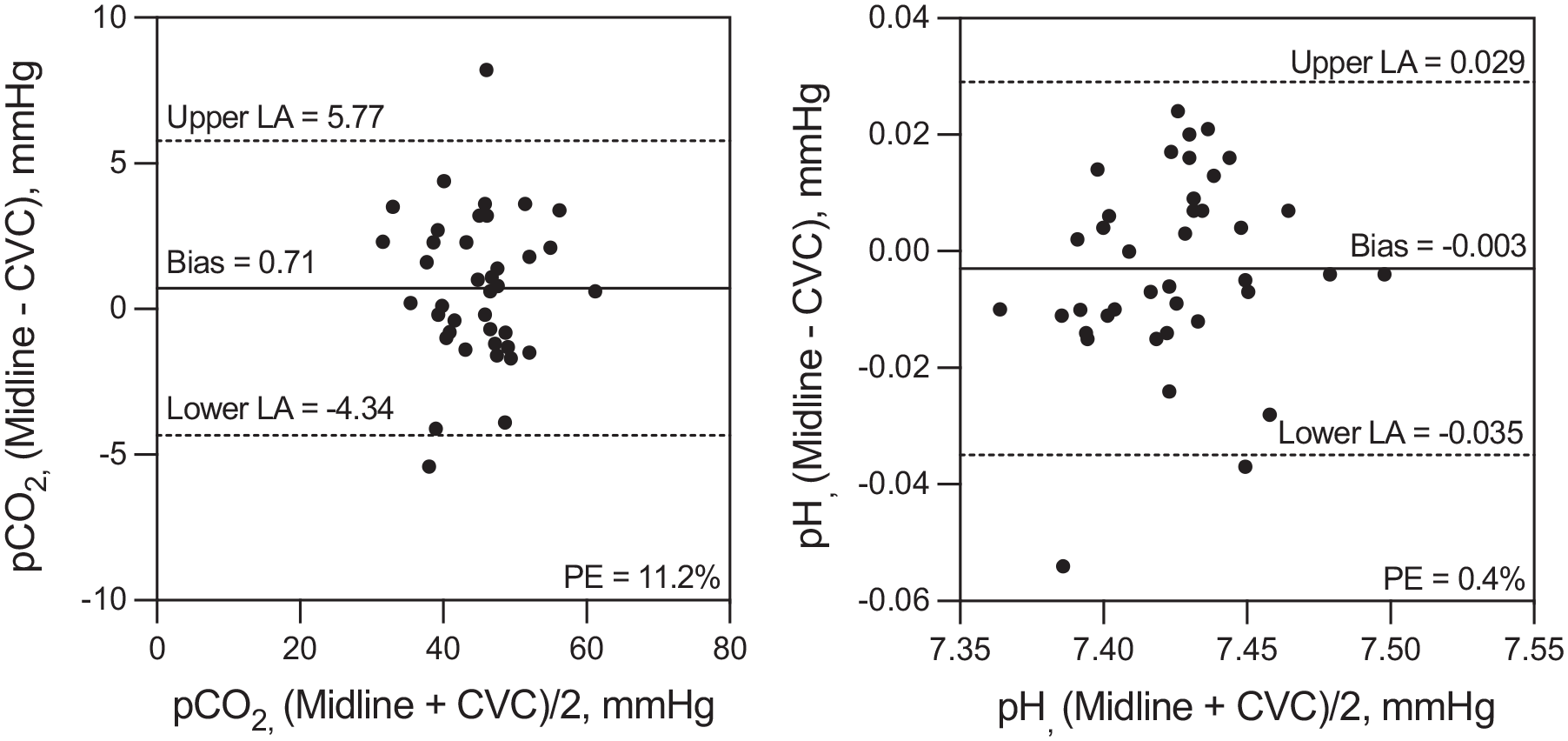
Bland–Altman plots for pCO2 (Panel A), pH (Panel B). Bias represents the mean difference between values of the parameters sampled from MC and CVC.
Correlation between MC and CVC parameters
Correlation analysis showed a significant and moderate-to-strong relationship between pH, pCO2, HCO3-, lactates and electrolytes for both CVC and arterial line samplings compared to MC (see Table 3). As expected, HbO2 and pO2 levels were significantly correlated between MC and CVC but not with between arterial and midline samples. The graphic representation of the correlation analysis between MC and CVC’s pCO2 and pH is reported in Supplemental Material (Figures S1 – panels A and B, respectively).
Correlation between arterial line and CVC versus midline samplings.
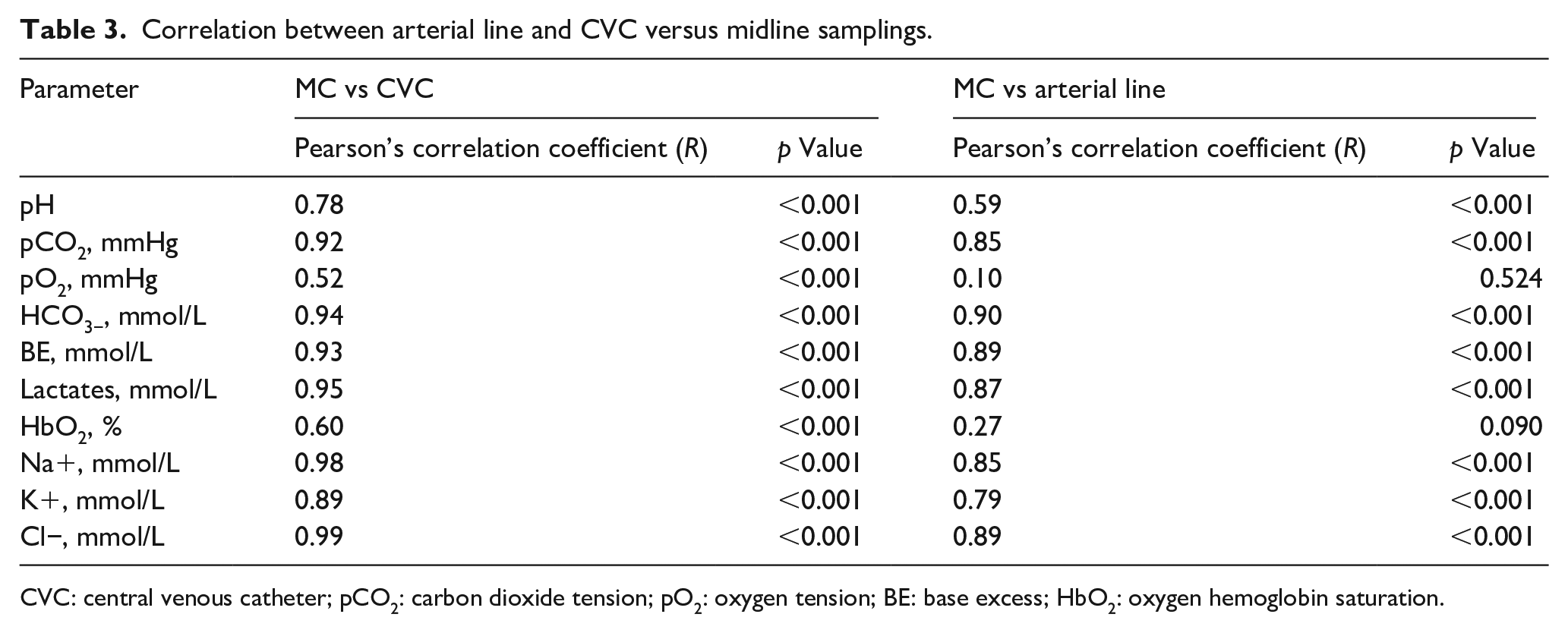
CVC: central venous catheter; pCO2: carbon dioxide tension; pO2: oxygen tension; BE: base excess; HbO2: oxygen hemoglobin saturation.
Discussion
In this prospective observational study, blood samples from midline catheters were compared to central venous and arterial samples to assess the validity of MC to monitor patients’ acid-base status and CO2 levels. A good agreement for pH and pCO2 measurements was found between MC and CVC samplings. Moreover, a very strong correlation between MC, arterial and CVC samples for most of the parameters of blood gas analysis were recorded except for oxygen content, as expected.
Patients admitted to acute care usually require intravascular accesses for monitoring and medication administration. Selection of the most appropriate vascular catheter should first consider the potentially severe associated complications. For this reason, it is crucial to find a balance between the clinical needs and the potential complications of each vascular cannulation.
Venous sampling might represent a valuable alternative to the arterial one for patient monitoring. Previous works have analysed the correlation between ABG and VBG in specific clinical situations, such as diabetic ketoacidosis,22,23 chronic obstructive pulmonary disease2,24,25 and trauma.26,27In these clinical contexts, a possible role for VBG at the time of initial assessment has emerged. More recently, the agreement between pH and pCO2 from VBG and ABG was confirmed by Chong and colleagues, 4 who considered for their work venous samples from central lines, and by Zeserson et al. 3 who evaluated peripheral venous samples. The possibility of replacing ABG with VBG is clinically relevant because of the complications that burden arterial line placement and maintenance, such as pain, infection, nerve injury, bleeding/hematoma, arterial aneurysm/pseudoaneurysm, dissection, thrombosis, and limb ischemia. 28
The need of advanced intravenous catheters should be reassessed routinely, 18 in particular before patients’ discharge from the ICU. At our institution, whenever possible, we are used to remove CVC and arterial lines to position a peripheral catheter, to minimize the risk of complications such as CRBSI or arterial ischemia, respectively. Of note, MCs placement is recommended for infusion solutions with <600 mOsm, pH 5–9 and blood products and if the duration of therapy is likely to last > 6 days. 17 Some authors propose MC as a safe alternative to CVCs for administration of vasopressors. 29 The latest standard of practice do not recommend the use of MCs for infusions of irritant or vesicant therapies, even with intermittent regimen and under strict surveillance of the infusion site. 18 So, it is important to carefully assess patient’s actual further need for such intravenous therapies when a catheter ‘de-escalation’ (from multi-lumen CICC to midline) is planned.
To the best of our knowledge, the present study was the first which explored the role of MC in this setting. A significant correlation for pH and pCO2 values between MC and arterial line was recorded. Mean differences between these two parameters were respectively −0.04 (95% CI −0.053 to −0.035) and 7 mmHg (95% CI 5.8–8.1) and were expected because of the physiological arterial-venous CO2 differences. The narrow confidence interval allows the clinician to effectively estimate arterial pH and CO2. For instance, in a patient with a VBG from the midline showing a pCO2 of 48 and a pH of 7.35, respiratory and metabolic acidosis can be excluded, and an arterial pCO2 of 40–42 and a pH of 7.38–7.41 can be roughly estimated.
As expected, the only parameter which cannot be estimated from the MC is the systemic oxygenation (arterial pO2 and HbO2). However, patients in the ICU undergo continuous monitoring of peripheral arterial saturation (SpO2) via pulse oximeter, and except for the case of low-quality signal or specific (and rare) conditions such as carboxyhemoglobinemia or methemoglobinemia, SpO2 can provide a good estimate of arterial oxygen hemoglobin saturation.30,31 Moreover, when arterial blood sampling is not available, such as in resource-limited settings (e.g. the recent COVID-19 pandemic), 30 the SpO2/FiO2 ratio can be effectively used as a surrogate of the pO2/FiO2 ratio for assessment of hypoxia in patients with acute respiratory failure.32,33
Only a rough estimate of mixed venous saturation (SvO2) can be performed by MC sampling. Despite a low average difference (−0.9%, 95% CI −4.2–2.5), the correlation of midline HbO2 with CVC samples was weak (r2 = 0.357). Blood drawn from MC shows the peripheral extraction of a single district of the body (the arm), and therefore the authors recommend against its use to estimate the mixed venous hemoglobin saturation in critically ill patients.
It should be clarified that midline catheters cannot ‘replace’ arterial lines and central catheters when caring for critical patients, as they do not provide any invasive hemodynamic monitoring ability, which is frequently required in the critical care setting to accurately monitor blood pressure and hemodynamic status. The first consideration that should be kept in mind is that this population was made of already stabilized patients ready to be discharged from the ICU. Thus, the conclusions of the present study apply to patients with non-critical hemodynamics. However, it could be interesting to speculate about a reliable way to monitor patients who are still critical, but more stable with regards to hemodynamics and so not peremptorily in need for an invasive monitoring. An expert report by Teboul and colleagues explored several non-invasive techniques for hemodynamic monitoring, such as volume clamp method, continuous radial artery applanation tonometry technique, electrical bioimpedance and bioreactance systems and pulse wave transit time method. The reliability of these non-invasive systems is affected by conditions such as peripheral edema, severe vasoconstriction, cold extremities, arrythmias and vasopressors administration, which are very common if not always present in the critical patient. Their conclusion is that, at the present time, non-invasive monitoring is not recommended in hemodynamically unstable patients, but continual technological refinements probably give some hope for the future. 34
The present study also provided very high correlation coefficients between CVC and MC samples for sodium, potassium and chloride ions (r2 respectively 0.954, 0.792 and 0.983, p < 0.001 for all the three correlations), confirming the role of MC for the assessment of electrolyte alterations.
In the light of these findings, the effective advantages of MCs compared to CVCs should be considered: midline catheters are less invasive, safer and faster to position, and associated with fewer CRBSI,20,35–37 representing a cost-effective alternative vascular access. 38 Moreover, they are an unvaluable alternative when the access to central veins is difficult, such as in patients who suffered from head and neck trauma or those on noninvasive respiratory support (e.g. helmet CPAP). Of note, when MC are used in patients undergoing helmet CPAP ventilation, we suggest the use of counterweight systems instead of armpit straps, in order to minimize the risk of upper extremity deep vein thrombosis due to axillary veins compression 39 a complication that would affect MC’s integrity and performance.
This study has some limitations. First, the study population was relatively small. Formal sample size calculation was not performed, as no data were available to estimate the agreement of MC samples with other sampling sites. Second, the population was largely made of patients who suffered from respiratory failure, so it may not be possible to generalize the results to patients affected by clinical conditions such as acute cardiac failure, seizures, shock, congenital heart disease, in which VBG and ABG do not show significant agreement. 40 Third, only one timepoint was explored. For this reason, it was not possible to estimate the trending ability of MC sampling compared to central venous lines.
Conclusion
In clinically stable patients, midline catheters represent a reliable and valid alternative to CVC and arterial lines to monitor alterations of acid-base status, CO2 levels and electrolytes.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298231163352 – Supplemental material for Midline catheters for blood gas and acid/base monitoring in critical patients: A prospective observational study
Supplemental material, sj-pdf-1-jva-10.1177_11297298231163352 for Midline catheters for blood gas and acid/base monitoring in critical patients: A prospective observational study by Marco Giani, Benedetta Fumagalli, Emanuele Rezoagli, Luigi Cannizzo, Luciano Giannini, Dario D’Amata, Alberto Lucchini, Roberto Rona, Stefano Elli and Giuseppe Foti in The Journal of Vascular Access
Footnotes
Contributorship
Giani and Elli had full access to all the data in the study and take responsibility for their integrity and the accuracy of the data analysis.
Giani and Elli were responsible for the decision to submit the manuscript.
Conceptualization and design: Giani, Elli, Foti.
Data collection: Cannizzo, D’Amata, Giannini
Data curation and investigation, Formal Analysis: Giani and Rezoagli.
Methodology: Giani, Rezoagli, Elli
Writing – original draft: Fumagalli, Giani, Elli
Writing – review and editing: Giani, Rezoagli, Elli, Foti
Supervision: Lucchini, Rona, Foti.
All authors had full access to all the data and accept responsibility to submit for publication.
All authors have read and approved the final text.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local Ethics Committee in November 2021 (Comitato Etico Brianza – ref. n. 317–2021).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.